
Co-Infection and Ventilator-Associated Pneumonia in Critically Ill COVID-19 Patients Requiring Mechanical Ventilation: A Retrospective Cohort Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Design
2.3. Diagnosis of Ventilator-Associated Pneumonia
2.4. Definitions
2.5. Data Collection
2.6. Statistical Analysis
3. Results
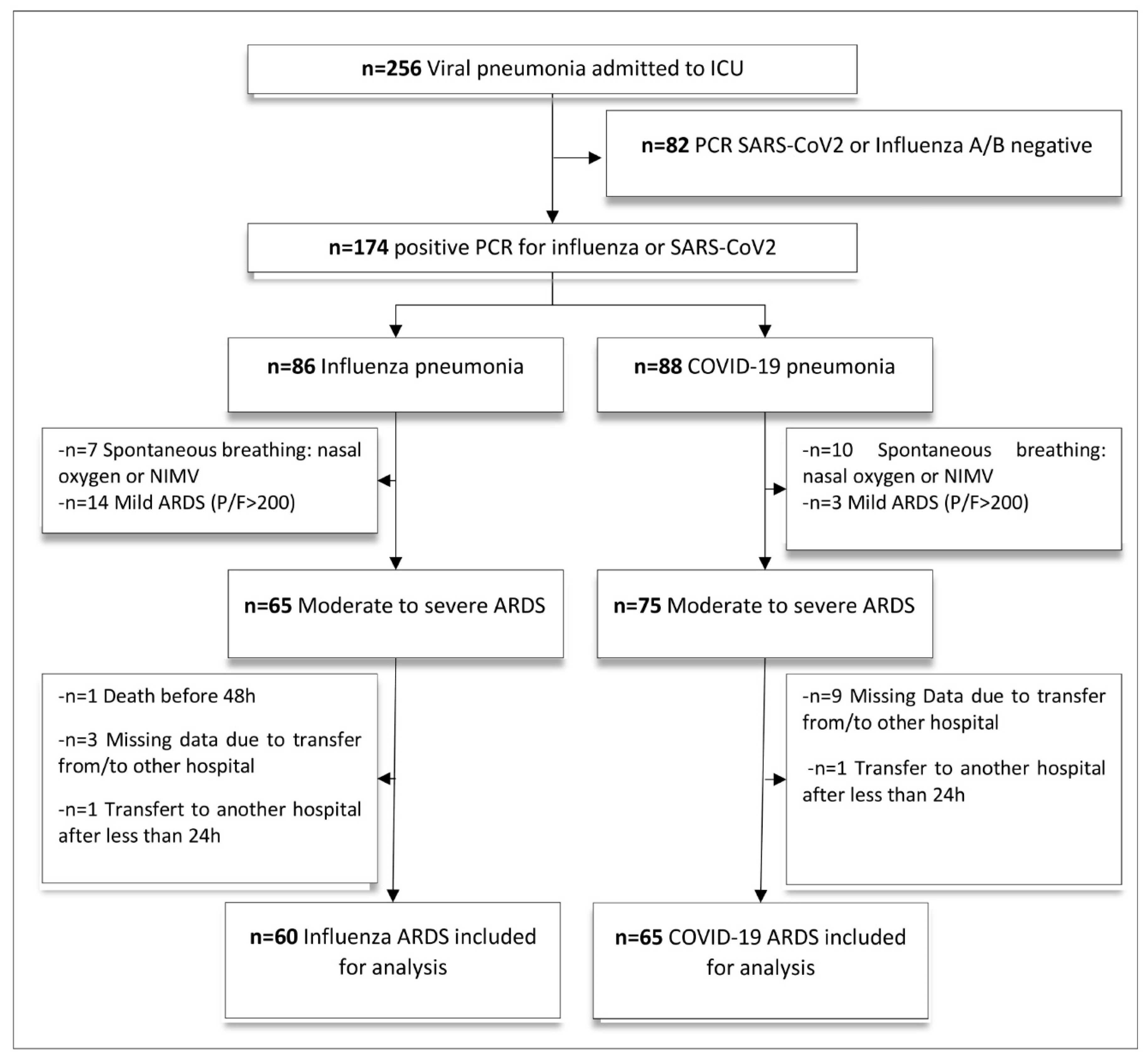
3.1. Study Population
3.2. Incidence of Ventilator-Associated Pneumonia
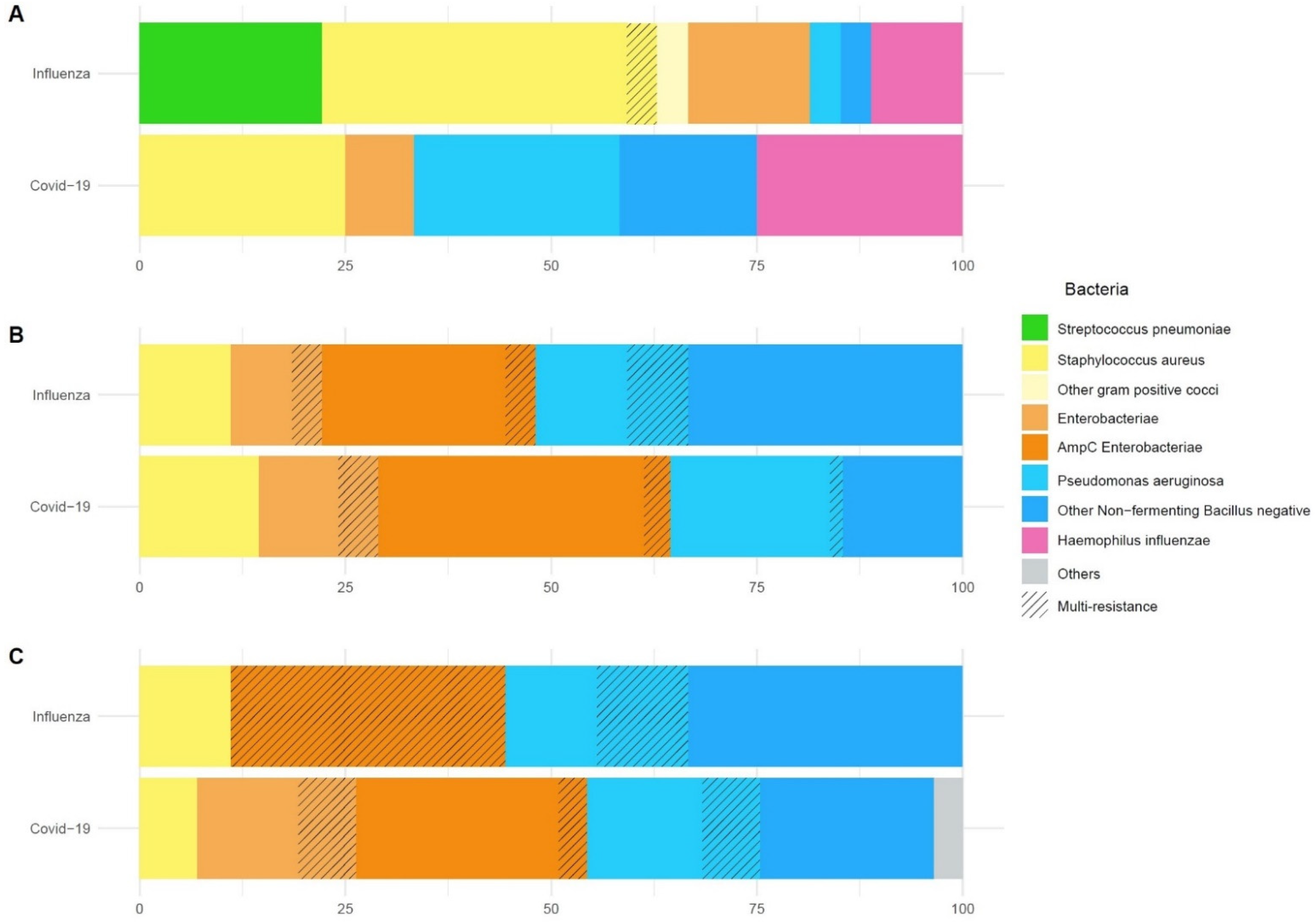
3.3. Microbiological Findings
3.4. Clinical Outcomes
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chertow, D.S.; Memoli, M.J. Bacterial coinfection in influenza: A grand rounds review. JAMA 2013, 309, 275–282. [Google Scholar] [CrossRef] [PubMed]
- Morris, D.E.; Cleary, D.W.; Clarke, S.C. Secondary Bacterial Infections Associated with Influenza Pandemics. Front. Microbiol. 2017, 8, 1041. [Google Scholar] [CrossRef] [PubMed]
- Clancy, C.J.; Nguyen, M.H. COVID-19, superinfections and antimicrobial development: What can we expect? Clin. Infect. Dis. 2020, 71, 2736–2743. [Google Scholar] [CrossRef] [PubMed]
- Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. Acute respiratory distress syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar] [CrossRef]
- Donnelly, J.P.; Chen, S.C.; Kauffman, C.A.; Steinbach, W.J.; Baddley, J.W.; Verweij, P.E.; Clancy, C.J.; Wingard, J.R.; Lockhart, S.R.; Groll, A.H.; et al. Revision and Update of the Consensus Definitions of Invasive Fungal Disease from the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin. Infect. Dis. 2020, 71, 1367–1376. [Google Scholar] [CrossRef]
- Knaus, W.A.; Zimmerman, J.E.; Wagner, D.P.; Draper, E.A.; Lawrence, D.E. APACHE-acute physiology and chronic health evaluation: A physiologically based classification system. Crit. Care Med. 1981, 9, 591–597. [Google Scholar] [CrossRef] [PubMed]
- Bal, A.; Casalegno, J.S.; Melenotte, C.; Daviet, F.; Ninove, L.; Edouard, S.; Morfin, F.; Valette, M.; De Lamballerie, X.; Lina, B.; et al. Influenza-induced acute respiratory distress syndrome during the 2010–2016 seasons: Bacterial co-infections and outcomes by virus type and subtype. Clin. Microbiol. Infect. 2020, 26, 947.e941–947.e944. [Google Scholar] [CrossRef]
- Klein, E.Y.; Monteforte, B.; Gupta, A.; Jiang, W.; May, L.; Hsieh, Y.H.; Dugas, A. The frequency of influenza and bacterial coinfection: A systematic review and meta-analysis. Influenza Other Respir. Viruses 2016, 10, 394–403. [Google Scholar] [CrossRef]
- Rice, T.W.; Rubinson, L.; Uyeki, T.M.; Vaughn, F.L.; John, B.B.; Miller, R.R., 3rd; Higgs, E.; Randolph, A.G.; Smoot, B.E.; Thompson, B.T.; et al. Critical illness from 2009 pandemic influenza A virus and bacterial coinfection in the United States. Crit. Care Med. 2012, 40, 1487–1498. [Google Scholar] [CrossRef]
- Martin-Loeches, I.; Schultz, M.J.; Vincent, J.L.; Alvarez-Lerma, F.; Bos, L.D.; Sole-Violan, J.; Torres, A.; Rodriguez, A. Increased incidence of co-infection in critically ill patients with influenza. Intensive Care Med. 2017, 43, 48–58. [Google Scholar] [CrossRef]
- Dudoignon, E.; Camelena, F.; Deniau, B.; Habay, A.; Coutrot, M.; Ressaire, Q.; Plaud, B.; Bercot, B.; Depret, F. Bacterial Pneumonia in COVID-19 critically ill patients: A case series. Clin. Infect. Dis. 2020, 72, 905–906. [Google Scholar] [CrossRef] [PubMed]
- Kreitmann, L.; Monard, C.; Dauwalder, O.; Simon, M.; Argaud, L. Early bacterial co-infection in ARDS related to COVID-19. Intensive Care Med. 2020, 46, 1787–1789. [Google Scholar] [CrossRef] [PubMed]
- Contou, D.; Claudinon, A.; Pajot, O.; Micaelo, M.; Longuet Flandre, P.; Dubert, M.; Cally, R.; Logre, E.; Fraisse, M.; Mentec, H.; et al. Bacterial and viral co-infections in patients with severe SARS-CoV-2 pneumonia admitted to a French ICU. Ann. Intensive Care 2020, 10, 119. [Google Scholar] [CrossRef] [PubMed]
- Tay, M.Z.; Poh, C.M.; Rénia, L.; MacAry, P.A.; Ng, L.F.P. The trinity of COVID-19: Immunity, inflammation and intervention. Nat. Rev. Immunol. 2020, 20, 363–374. [Google Scholar] [CrossRef] [PubMed]
- Cao, X. COVID-19: Immunopathology and its implications for therapy. Nat. Rev. Immunol. 2020, 20, 269–270. [Google Scholar] [CrossRef]
- Remy, K.E.; Mazer, M.; Striker, D.A.; Ellebedy, A.H.; Walton, A.H.; Unsinger, J.; Blood, T.M.; Mudd, P.A.; Yi, D.J.; Mannion, D.A.; et al. Severe immunosuppression and not a cytokine storm characterizes COVID-19 infections. JCI Insight 2020, 5, e140329. [Google Scholar] [CrossRef]
- Mudd, P.A.; Crawford, J.C.; Turner, J.S.; Souquette, A.; Reynolds, D.; Bender, D.; Bosanquet, J.P.; Anand, N.J.; Striker, D.A.; Martin, R.S.; et al. Targeted Immunosuppression Distinguishes COVID-19 from Influenza in Moderate and Severe Disease. medRxiv 2020. [Google Scholar] [CrossRef]
- Giamarellos-Bourboulis, E.J.; Netea, M.G.; Rovina, N.; Akinosoglou, K.; Antoniadou, A.; Antonakos, N.; Damoraki, G.; Gkavogianni, T.; Adami, M.-E.; Katsaounou, P.; et al. Complex Immune Dysregulation in COVID-19 Patients with Severe Respiratory Failure. Cell Host Microbe 2020, 27, 992–1000. [Google Scholar] [CrossRef]
- Abelenda-Alonso, G.; Rombauts, A.; Gudiol, C.; Meije, Y.; Ortega, L.; Clemente, M.; Ardanuy, C.; Niubo, J.; Carratala, J. Influenza and Bacterial Coinfection in Adults with Community-Acquired Pneumonia Admitted to Conventional Wards: Risk Factors, Clinical Features, and Outcomes. Open Forum Infect. Dis. 2020, 7, ofaa066. [Google Scholar] [CrossRef]
- Shah, N.S.; Greenberg, J.A.; McNulty, M.C.; Gregg, K.S.; Riddell, J.t.; Mangino, J.E.; Weber, D.M.; Hebert, C.L.; Marzec, N.S.; Barron, M.A.; et al. Bacterial and viral co-infections complicating severe influenza: Incidence and impact among 507 U.S. patients, 2013–2014. J. Clin. Virol. 2016, 80, 12–19. [Google Scholar] [CrossRef]
- Hughes, S.; Troise, O.; Donaldson, H.; Mughal, N.; Moore, L.S.P. Bacterial and fungal coinfection among hospitalized patients with COVID-19: A retrospective cohort study in a UK secondary-care setting. Clin. Microbiol. Infect. 2020, 26, 1395–1399. [Google Scholar] [CrossRef] [PubMed]
- Langford, B.J.; So, M.; Raybardhan, S.; Leung, V.; Westwood, D.; MacFadden, D.R.; Soucy, J.R.; Daneman, N. Bacterial co-infection and secondary infection in patients with COVID-19: A living rapid review and meta-analysis. Clin. Microbiol. Infect. 2020, 26, 1622–1629. [Google Scholar] [CrossRef] [PubMed]
- Oliva, A.; Siccardi, G.; Migliarini, A.; Cancelli, F.; Carnevalini, M.; D’Andria, M.; Attilia, I.; Danese, V.C.; Cecchetti, V.; Romiti, R.; et al. Co-infection of SARS-CoV-2 with Chlamydia or Mycoplasma pneumoniae: A case series and review of the literature. Infection 2020, 48, 871–877. [Google Scholar] [CrossRef] [PubMed]
- HCSP. Coronavirus SARS-CoV-2: Recommandations Sur L’usage des Anti Infectieux. Available online: https://www.hcsp.fr/explore.cgi/avisrapportsdomaine?clefr=849 (accessed on 12 December 2020).
- Chastre, J.; Wolff, M.; Fagon, J.Y.; Chevret, S.; Thomas, F.; Wermert, D.; Clementi, E.; Gonzalez, J.; Jusserand, D.; Asfar, P.; et al. Comparison of 8 vs. 15 days of antibiotic therapy for ventilator-associated pneumonia in adults: A randomized trial. JAMA 2003, 290, 2588–2598. [Google Scholar] [CrossRef]
- Clinical characteristics and day-90 outcomes of 4244 critically ill adults with COVID-19: A prospective cohort study. Intensive Care Med. 2021, 47, 60–73. [CrossRef]
- Nseir, S.; Martin-Loeches, I.; Povoa, P.; Metzelard, M.; Du Cheyron, D.; Lambiotte, F.; Tamion, F.; Labruyere, M.; Makris, D.; Boulle Geronimi, C.; et al. Relationship between ventilator-associated pneumonia and mortality in COVID-19 patients: A planned ancillary analysis of the coVAPid cohort. Crit. Care 2021, 25, 177. [Google Scholar] [CrossRef]
- Luyt, C.E.; Sahnoun, T.; Gautier, M.; Vidal, P.; Burrel, S.; Pineton de Chambrun, M.; Chommeloux, J.; Desnos, C.; Arzoine, J.; Nieszkowska, A.; et al. Ventilator-associated pneumonia in patients with SARS-CoV-2-associated acute respiratory distress syndrome requiring ECMO: A retrospective cohort study. Ann. Intensive Care 2020, 10, 158. [Google Scholar] [CrossRef]
- Rouze, A.; Martin-Loeches, I.; Povoa, P.; Makris, D.; Artigas, A.; Bouchereau, M.; Lambiotte, F.; Metzelard, M.; Cuchet, P.; Boulle Geronimi, C.; et al. Relationship between SARS-CoV-2 infection and the incidence of ventilator-associated lower respiratory tract infections: A European multicenter cohort study. Intensive Care Med. 2021, 47, 188–198. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Total (n = 125) | Influenza (n = 60) | COVID-19 (n = 65) | p | |
|---|---|---|---|---|
| General characteristics | ||||
| Age (years) | 62 (55–69) | 60 (52–65) | 65 (56–72) | 0.022 |
| Male gender | 92 (74) | 39 (65) | 53 (82) | 0.058 |
| BMI (kg/m2) | 27 (24–31) | 27 (23–32) | 27 (25–31) | 0.663 |
| Heath status | ||||
| Good | 70 (56) | 37 (61) | 33 (50) | 0.015 |
| Mild to moderate | 22 (17) | 9 (15) | 13 (20) | |
| Serious | 25 (20) | 6 (10) | 19 (29) | |
| Severe | 3 (2) | 3 (5) | 0 (0) | |
| Blood group | ||||
| A/B/AB | 52/81 (64) | 21/41 (51) | 31/40 (77) | 0.025 |
| O | 38/81 (46) | 20/41 (49) | 9/40 (22) | |
| Underlying medical condition | ||||
| Diabetes | 21 (16) | 6 (9) | 15 (25) | 0.034 |
| Dyslipidaemia | 25 (20) | 13 (20) | 12 (20) | 1.000 |
| Hypertension | 45 (31) | 14(21) | 31 (51) | 0.893 |
| Myocardial infarction | 16 (12) | 9 (15) | 7 (10) | 0.660 |
| Heart failure | 3 (2) | 3 (4) | 0 (0) | 0.104 |
| COPD | 15 (12) | 10 (15) | 5 (7) | 0.192 |
| Asthma | 6 (4) | 2 (3) | 4 (6) | 0.681 |
| Smoker | 34 (27) | 18 (30) | 16 (24) | 0.398 |
| Chronic kidney disease | 10 (8) | 2 (3) | 8 (12) | 0.098 |
| Immunocompromised | 11 (8) | 7 (11) | 4 (6) | 0.440 |
| Solid tumour | 15 (12) | 7 (11) | 8 (12) | 1.000 |
| Non-steroidal anti inflammatory | 12 (9) | 6 (10) | 6 (9) | 1.000 |
| Steroid use | 10 (8) | 8 (13) | 2 (3) | 0.041 |
| ACE inhibitors or ARB treatment | 38 (30) | 17 (28) | 21 (32) | 0.820 |
| Characteristics at ICU admission | ||||
| SAPS II | 37 (31–43) | 36 (31–46) | 37 (32–42) | 0.748 |
| SOFA | 7 (6–9) | 8 (6–9) | 7 (5–8) | 0.003 |
| Glasgow coma scale | 15 (15–15) | 15 (15–15) | 15 (15–15) | 0.330 |
| Mean blood pressure (mmHg) | 64 (60–69) | 65 (58–71) | 63 (60–66) | 0.475 |
| Norepinephrine administration | 67 (53) | 51 (85) | 16 (65) | <0.001 |
| Acute renal failure | ||||
| K-DIGO 0–1 | 94 (75) | 42 (69) | 52 (79) | 0.023 |
| K-DIGO 2–3 | 31(25) | 18 (30) | 13 (21) | |
| PaO2/FiO2 (mmHg) | 137 (107–168) | 138 (103–158) | 136 (109–175) | 0.168 |
| PEEP applied (cm H2O) | 10 (8–12) | 10 (8–12) | 10 (8–12) | 0.286 |
| Tidal volume (mL/kg predicted body weight) | 6.5 (6.2–7.0) | 6.4 (6.0–7.0) | 6.7 (6.3–7.0) | 0.069 |
| Respiratory system compliance (mL/cm H2O) | 40 (31–49) | 34 (26–41) | 46 (38–54) | <0.001 |
| Total (n = 125) | Influenza (n = 60) | COVID-19 (n = 65) | p | |
|---|---|---|---|---|
| Primary outcome | ||||
| VAP incidence/100 IMV days (IC 95%) | 5.2 (4.1–6.6) | 3.4 (2.2–5.2) | 7.2 (5.3–9.6) | 0.004 |
| Secondary outcomes | ||||
| Bacterial co-infection at baseline | ||||
| Prevalence | 31/125 (24) | 20/60 (33) | 11/65 (16) | 0.055 |
| Empiric antibiotic therapy | 125/125 (100) | 60/60 (100) | 65/65 (100) | 1.000 |
| Duration of antibiotic therapy (days) | 6 (4–7) | 7 (5–8.5) | 5 (4–6) | <0.001 |
| Appropriateness of empiric antibiotic therapy | ||||
| Appropriate | 12/31 (38) | 15/20 (75) | 4/11 (36) | 0.056 |
| Inappropriate | 19/31 (61) | 5/20 (25) | 7/11 (63) | |
| First VAP | ||||
| Prevalence | 66/125 (52) | 23/60 (38) | 43/65 (66) | 0.003 |
| Delay (days from intubation) | 8 (4–13) | 7 (4–14) | 8 (5–13) | 0.626 |
| Early VAP (≤6 days) | 24/66 (36) | 11/23 (47) | 13/43 (30) | 0.251 |
| Late VAP (>7 days) | 42/66 (63) | 12/23 (52) | 30/43 (69) | |
| Appropriateness of empiric antibiotic therapy | ||||
| Appropriate | 24/66 (36) | 4/23 (17) | 20/43 (46) | 0.035 |
| Inappropriate | 8/66 (12) | 2/23 (8) | 6/43 (13) | |
| None | 33/66 (50) | 16/23 (69) | 17/43 (39) | |
| Appropriate final antibiotic therapy | 66/66 (100) | 23/23 (100) | 43/43 (100) | 1.000 |
| Second and third VAP | ||||
| Prevalence of 2nd VAP | 26/125 (20) | 6/60 (10) | 20/65 (30) | 0.013 |
| Prevalence of 3rd VAP | 9/125 (7) | 1/60 (1) | 8/65 (12) | 0.050 |
| Recurrence | 0.005 | |||
| Persistence | 11/35 (31) | 0/7 (0) | 11/28 (39) | |
| Relapse | 15/35 (42) | 2/7 (28) | 13/28 (46) | |
| Superinfection | 9/35 (25) | 5/7 (71) | 4/28 (14) | |
| Appropriateness of empiric antibiotic therapy | ||||
| Appropriate | 11/35 (31) | 2/7 (28) | 9/28 (32) | 0.393 |
| Inappropriate | 7/35 (20) | 0/7 (0) | 7/28 (25) | |
| None | 17/35 (48) | 5/7 (71) | 12/28 (42) | |
| Appropriate final antibiotic therapy | 35/35 (100) | 7/7 (100) | 28/28 (100) | 1.000 |
| ICU Stay | ||||
| Invasive ventilation, days | 14 (8–21) | 13 (8–21) | 14 (8–22) | 0.397 |
| Death at D28 | 18 (14) | 11 (18) | 7 (10) | 0.342 |
| ICU mortality | 23 (18) | 13 (21) | 10 (15) | 0.500 |
| ICU stay, days | 20 (13–30) | 18 (13–25) | 21 (12–31) | 0.335 |
| Antibiotic therapy, days | 13 (7–19) | 10 (7–17) | 16 (7–21) | 0.051 |
| Influenza (n = 60) | COVID-19 (n = 65) | |
|---|---|---|
| Bacterial co-infection at baseline | n = 20 | n = 11 |
| Species identified in respiratory samples (total number) | 27 | 12 |
| Staphylococcus aureus | 11 (40) | 3 (25) |
| Streptococcus pneumoniae | 6 (22) | 0 (0) |
| Hemophilus influenzae | 3 (11) | 3 (25) |
| Enterobacteriaceae | 4 (14) | 1 (8) |
| AmpC Producing β-lactamase Enterobacteriaceae | 0 (0) | 0 (0) |
| Non fermenting gram-negative bacilli | 2 (7) | 5 (41) |
| Pseudomonas aeruginosa | 1 (3) | 3 (25) |
| Others | 1 (3) | 0 (0) |
| Multi-drug resistant species | 1 (5) | 0 (0) |
| Methicillin-resistant Staphylococcus Aureus | 1 | 0 |
| First VAP | n = 22 | n = 43 |
| Species identified in respiratory samples (total number) | 26 | 62 |
| Staphylococcus aureus | 3 (11) | 9 (14) |
| Enterobacteriaceae | 10 (36) | 31 (50) |
| AmpC producing β-lactamase Enterobacteriaceae | 7 (26) | 22 (35) |
| Non fermenting gram-negative bacilli | 13 (50) | 22 (35) |
| Pseudomonas aeruginosa | 5 (19) | 13 (20) |
| Acinetobacter baumannii | 1 (3) | 7 (11) |
| Stenotrophomonas maltophilia | 7 (53) | 2 (3) |
| Others | 0 (0) | 0 (0) |
| Multi-drug resistant species | 4 (14) | 6 (9) |
| Extended spectrum β-lactamase | 1 | 3 |
| Enterobacteriaceae cephalosporinase | 1 | 2 |
| Pseudomonas aeruginosa Ceftazidime-R or Carbapenem-R | 2 | 1 |
| Second and third VAP | n = 8 | n = 28 |
| Species identified in respiratory samples (total number) | 9 | 57 |
| Staphylococcus aureus | 1 (11) | 4 (7) |
| Enterobacteriaceae | 3 (33) | 27 (47) |
| AmpC producing β-lactamase Enterobacteriaceae | 3 (33) | 16 (28) |
| Non fermenting gram-negative bacilli | 5 (55) | 25 (43) |
| Pseudomonas aeruginosa | 2 (22) | 12 (21) |
| Acinetobacter baumannii | 2 (22) | 5 (8) |
| Stenotrophomonas maltophilia | 1 (11) | 8 (14) |
| Others | 0 (0) | 1 (1) |
| Multi-drug resistant species | 4 (36) | 10 (17) |
| Extended spectrum β-lactamase | 0 | 4 |
| Enterobacteriaceae cephalosporinase | 3 | 2 |
| Pseudomonas aeruginosa Ceftazidime-R or Carbapenem-R | 1 | 4 |
| Fungal pneumonia | ||
| Probable pulmonary aspergillosis | 8 (13) | 6 (9) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sarton, B.; Grare, M.; Vardon-Bounes, F.; Gaubert, A.; Silva, S.; Crognier, L.; Riu, B.; Seguin, T.; Georges, B.; Minville, V.; et al. Co-Infection and Ventilator-Associated Pneumonia in Critically Ill COVID-19 Patients Requiring Mechanical Ventilation: A Retrospective Cohort Study. Biomedicines 2022, 10, 1952. https://doi.org/10.3390/biomedicines10081952
Sarton B, Grare M, Vardon-Bounes F, Gaubert A, Silva S, Crognier L, Riu B, Seguin T, Georges B, Minville V, et al. Co-Infection and Ventilator-Associated Pneumonia in Critically Ill COVID-19 Patients Requiring Mechanical Ventilation: A Retrospective Cohort Study. Biomedicines. 2022; 10(8):1952. https://doi.org/10.3390/biomedicines10081952
Chicago/Turabian StyleSarton, Benjamine, Marion Grare, Fanny Vardon-Bounes, Anna Gaubert, Stein Silva, Laure Crognier, Béatrice Riu, Thierry Seguin, Bernard Georges, Vincent Minville, and et al. 2022. "Co-Infection and Ventilator-Associated Pneumonia in Critically Ill COVID-19 Patients Requiring Mechanical Ventilation: A Retrospective Cohort Study" Biomedicines 10, no. 8: 1952. https://doi.org/10.3390/biomedicines10081952
APA StyleSarton, B., Grare, M., Vardon-Bounes, F., Gaubert, A., Silva, S., Crognier, L., Riu, B., Seguin, T., Georges, B., Minville, V., & Ruiz, S. (2022). Co-Infection and Ventilator-Associated Pneumonia in Critically Ill COVID-19 Patients Requiring Mechanical Ventilation: A Retrospective Cohort Study. Biomedicines, 10(8), 1952. https://doi.org/10.3390/biomedicines10081952