
SAR296968, a Novel Selective Na+/Ca2+ Exchanger Inhibitor, Improves Ca2+ Handling and Contractile Function in Human Atrial Cardiomyocytes

 ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Human Myocyte Isolation
2.2. Preparation of SAR296968 Solutions and Storage Conditions
2.3. Measurement of Ca2+ Sparks
2.4. Patch-Clamp Experiments
2.5. Measurements of Contractility in Human Atrial Trabeculae
2.6. Statistical Analysis
3. Results
3.1. Patient Data
3.2. SAR296968 Decreases Pro-Arrhythmic Activity in Human Atrial Cardiomyocytes
3.3. SAR296968 Improves Contractility in Human Atrial Trabeculae
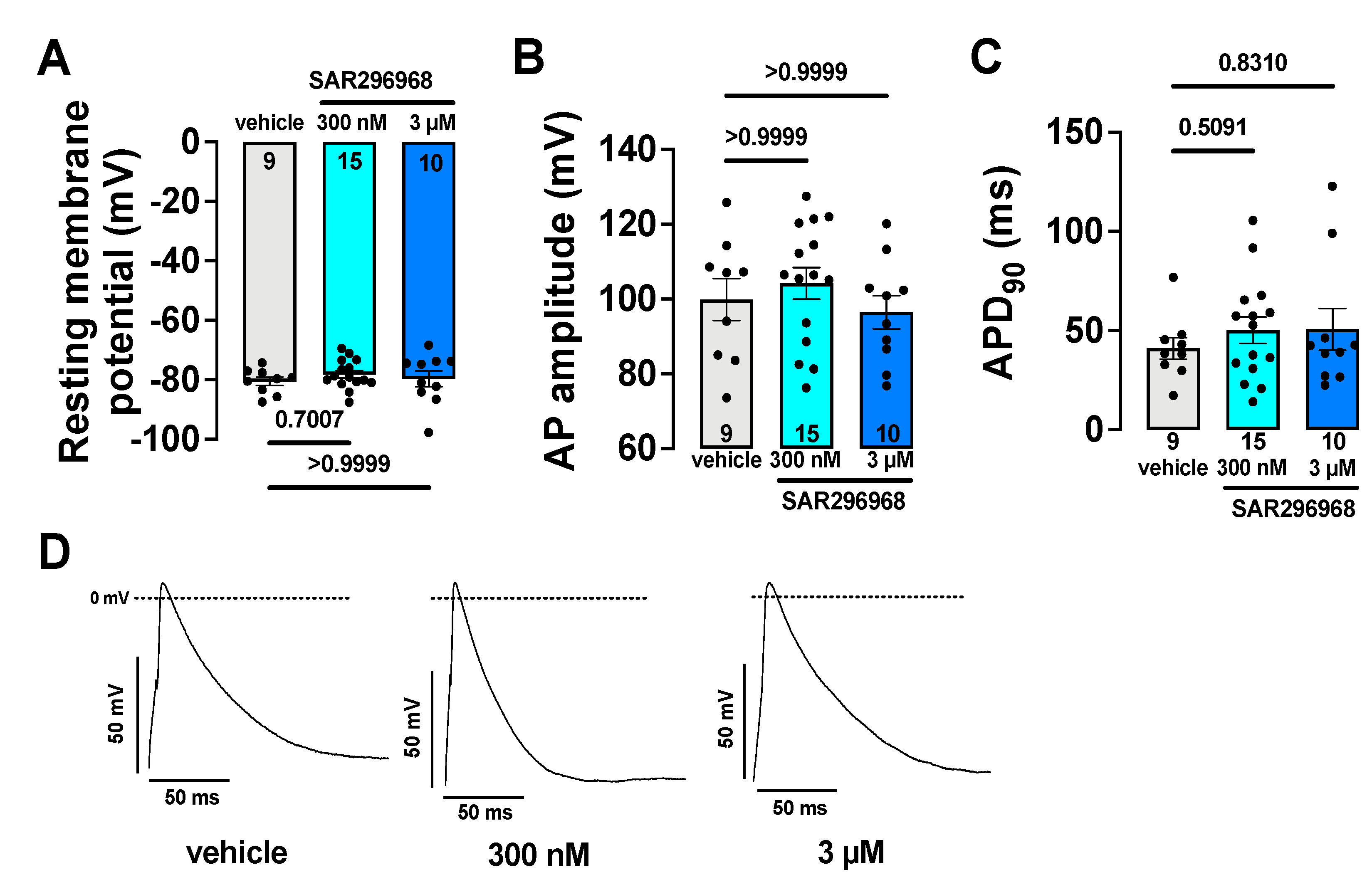
3.4. Electrophysiological Safety Parameters Remain Unaltered by SAR296968
4. Discussion
4.1. Pharmacological Profile and Safety
4.2. SAR296968 Reduces Triggered Activity in Atrial Myocytes
4.3. SAR296968 Increases SR Ca2+ Content and Improves Contractility in Human Atrium
4.4. SAR296968 Improves Diastolic Function
4.5. Translational Implications
4.6. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E., Jr.; Drazner, M.H.; Fonarow, G.C.; Geraci, S.A.; Horwich, T.; Januzzi, J.L.; et al. 2013 ACCF/AHA guideline for the management of heart failure: Executive summary: A report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation 2013, 128, 1810–1852. [Google Scholar] [CrossRef] [PubMed]
- Arnold, J.M.O.; Liu, P.; Howlett, J.; Ignaszewski, A.; Leblanc, M.-H.; Kaan, A.; Pearce, C.; Sinclair, L.; Pearce, S.; Prentice, C. Ten year survival by NYHA functional class in heart failure outpatients referred to specialized multidisciplinary heart failure clinics 1999 to 2011. Eur. Heart J. 2013, 34, P1505. [Google Scholar] [CrossRef]
- Gevaert, A.B.; Boen, J.R.A.; Segers, V.F.; Van Craenenbroeck, E.M. Heart Failure With Preserved Ejection Fraction: A Review of Cardiac and Noncardiac Pathophysiology. Front. Physiol. 2019, 10, 638. [Google Scholar] [CrossRef]
- Hasenfuss, G.; Reinecke, H.; Studer, R.; Meyer, M.; Pieske, B.; Holtz, J.; Holubarsch, C.; Posival, H.; Just, H.; Drexler, H. Relation between myocardial function and expression of sarcoplasmic reticulum Ca(2+)-ATPase in failing and nonfailing human myocardium. Circ. Res. 1994, 75, 434–442. [Google Scholar] [CrossRef]
- Schwinger, R.H.; Bohm, M.; Schmidt, U.; Karczewski, P.; Bavendiek, U.; Flesch, M.; Krause, E.G.; Erdmann, E. Unchanged protein levels of SERCA II and phospholamban but reduced Ca2+ uptake and Ca(2+)-ATPase activity of cardiac sarcoplasmic reticulum from dilated cardiomyopathy patients compared with patients with nonfailing hearts. Circulation 1995, 92, 3220–3228. [Google Scholar] [CrossRef]
- Studer, R.; Reinecke, H.; Bilger, J.; Eschenhagen, T.; Bohm, M.; Hasenfuss, G.; Just, H.; Holtz, J.; Drexler, H. Gene expression of the cardiac Na(+)-Ca2+ exchanger in end-stage human heart failure. Circ. Res. 1994, 75, 443–453. [Google Scholar] [CrossRef] [PubMed]
- Hasenfuss, G.; Pieske, B. Calcium cycling in congestive heart failure. J. Mol. Cell Cardiol. 2002, 34, 951–969. [Google Scholar] [CrossRef] [PubMed]
- Lenaerts, I.; Bito, V.; Heinzel, F.R.; Driesen, R.B.; Holemans, P.; D’Hooge, J.; Heidbuchel, H.; Sipido, K.R.; Willems, R. Ultrastructural and functional remodeling of the coupling between Ca2+ influx and sarcoplasmic reticulum Ca2+ release in right atrial myocytes from experimental persistent atrial fibrillation. Circ. Res. 2009, 105, 876–885. [Google Scholar] [CrossRef]
- Flesch, M.; Schwinger, R.H.; Schiffer, F.; Frank, K.; Sudkamp, M.; Kuhn-Regnier, F.; Arnold, G.; Bohm, M. Evidence for functional relevance of an enhanced expression of the Na(+)-Ca2+ exchanger in failing human myocardium. Circulation 1996, 94, 992–1002. [Google Scholar] [CrossRef]
- Schotten, U.; Greiser, M.; Benke, D.; Buerkel, K.; Ehrenteidt, B.; Stellbrink, C.; Vazquez-Jimenez, J.F.; Schoendube, F.; Hanrath, P.; Allessie, M. Atrial fibrillation-induced atrial contractile dysfunction: A tachycardiomyopathy of a different sort. Cardiovasc. Res. 2002, 53, 192–201. [Google Scholar] [CrossRef]
- Schillinger, W.; Janssen, P.M.; Emami, S.; Henderson, S.A.; Ross, R.S.; Teucher, N.; Zeitz, O.; Philipson, K.D.; Prestle, J.; Hasenfuss, G. Impaired contractile performance of cultured rabbit ventricular myocytes after adenoviral gene transfer of Na(+)-Ca(2+) exchanger. Circ. Res. 2000, 87, 581–587. [Google Scholar] [CrossRef] [PubMed]
- Beuckelmann, D.J.; Nabauer, M.; Erdmann, E. Intracellular calcium handling in isolated ventricular myocytes from patients with terminal heart failure. Circulation 1992, 85, 1046–1055. [Google Scholar] [CrossRef] [PubMed]
- Dunlay, S.M.; Roger, V.L.; Redfield, M.M. Epidemiology of heart failure with preserved ejection fraction. Nat. Rev. Cardiol. 2017, 14, 591–602. [Google Scholar] [CrossRef]
- Primessnig, U.; Bracic, T.; Levijoki, J.; Otsomaa, L.; Pollesello, P.; Falcke, M.; Pieske, B.; Heinzel, F.R. Long-term effects of Na(+)/Ca(2+) exchanger inhibition with ORM-11035 improves cardiac function and remodelling without lowering blood pressure in a model of heart failure with preserved ejection fraction. Eur. J. Heart Fail. 2019, 21, 1543–1552. [Google Scholar] [CrossRef] [PubMed]
- Primessnig, U.; Schonleitner, P.; Holl, A.; Pfeiffer, S.; Bracic, T.; Rau, T.; Kapl, M.; Stojakovic, T.; Glasnov, T.; Leineweber, K.; et al. Novel pathomechanisms of cardiomyocyte dysfunction in a model of heart failure with preserved ejection fraction. Eur. J. Heart Fail. 2016, 18, 987–997. [Google Scholar] [CrossRef] [PubMed]
- Kamimura, D.; Ohtani, T.; Sakata, Y.; Mano, T.; Takeda, Y.; Tamaki, S.; Omori, Y.; Tsukamoto, Y.; Furutani, K.; Komiyama, Y.; et al. Ca2+ entry mode of Na+/Ca2+ exchanger as a new therapeutic target for heart failure with preserved ejection fraction. Eur. Heart J. 2011, 33, 1408–1416. [Google Scholar] [CrossRef]
- Pott, C.; Eckardt, L.; Goldhaber, J.I. Triple threat: The Na+/Ca2+ exchanger in the pathophysiology of cardiac arrhythmia, ischemia and heart failure. Curr. Drug Targets 2011, 12, 737–747. [Google Scholar] [CrossRef]
- Sossalla, S.; Kallmeyer, B.; Wagner, S.; Mazur, M.; Maurer, U.; Toischer, K.; Schmitto, J.D.; Seipelt, R.; Schondube, F.A.; Hasenfuss, G.; et al. Altered Na(+) currents in atrial fibrillation effects of ranolazine on arrhythmias and contractility in human atrial myocardium. J. Am. Coll. Cardiol. 2010, 55, 2330–2342. [Google Scholar] [CrossRef] [PubMed]
- Nagy, Z.A.; Virag, L.; Toth, A.; Biliczki, P.; Acsai, K.; Banyasz, T.; Nanasi, P.; Papp, J.G.; Varro, A. Selective inhibition of sodium-calcium exchanger by SEA-0400 decreases early and delayed after depolarization in canine heart. Br. J. Pharmacol. 2004, 143, 827–831. [Google Scholar] [CrossRef]
- Pelat, M.; Barbe, F.; Daveu, C.; Ly-Nguyen, L.; Lartigue, T.; Marque, S.; Tavares, G.; Ballet, V.; Guillon, J.M.; Steinmeyer, K.; et al. SAR340835, a Novel Selective Na(+)/Ca(2+) Exchanger Inhibitor, Improves Cardiac Function and Restores Sympathovagal Balance in Heart Failure. J. Pharmacol. Exp. Ther. 2021, 377, 293–304. [Google Scholar] [CrossRef]
- Kohajda, Z.; Farkas-Morvay, N.; Jost, N.; Nagy, N.; Geramipour, A.; Horvath, A.; Varga, R.S.; Hornyik, T.; Corici, C.; Acsai, K.; et al. The Effect of a Novel Highly Selective Inhibitor of the Sodium/Calcium Exchanger (NCX) on Cardiac Arrhythmias in In Vitro and In Vivo Experiments. PLoS ONE 2016, 11, e0166041. [Google Scholar] [CrossRef] [PubMed]
- Cheng, H.; Lederer, W.J.; Cannell, M.B. Calcium sparks: Elementary events underlying excitation-contraction coupling in heart muscle. Science 1993, 262, 740–744. [Google Scholar] [CrossRef] [PubMed]
- Lebek, S.; Pichler, K.; Reuthner, K.; Trum, M.; Tafelmeier, M.; Mustroph, J.; Camboni, D.; Rupprecht, L.; Schmid, C.; Maier, L.S.; et al. Enhanced CaMKII-Dependent Late INa Induces Atrial Proarrhythmic Activity in Patients With Sleep-Disordered Breathing. Circ. Res. 2020, 126, 603–615. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Bohm, M.; Burri, H.; Butler, J.; Celutkiene, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Berecki, G.; Wilders, R.; de Jonge, B.; van Ginneken, A.C.; Verkerk, A.O. Re-evaluation of the action potential upstroke velocity as a measure of the Na+ current in cardiac myocytes at physiological conditions. PLoS ONE 2010, 5, e15772. [Google Scholar] [CrossRef] [PubMed]
- Bengel, P.; Dybkova, N.; Tirilomis, P.; Ahmad, S.; Hartmann, N.; Mohamed, B.A.; Krekeler, M.C.; Maurer, W.; Pabel, S.; Trum, M.; et al. Detrimental proarrhythmogenic interaction of Ca(2+)/calmodulin-dependent protein kinase II and NaV1.8 in heart failure. Nat. Commun. 2021, 12, 6586. [Google Scholar] [CrossRef]
- Pabel, S.; Ahmad, S.; Tirilomis, P.; Stehle, T.; Mustroph, J.; Knierim, M.; Dybkova, N.; Bengel, P.; Holzamer, A.; Hilker, M.; et al. Inhibition of NaV1.8 prevents atrial arrhythmogenesis in human and mice. Basic Res. Cardiol. 2020, 115, 20. [Google Scholar] [CrossRef]
- Blaustein, M.P.; Lederer, W.J. Sodium/calcium exchange: Its physiological implications. Physiol. Rev. 1999, 79, 763–854. [Google Scholar] [CrossRef]
- Baartscheer, A.; Schumacher, C.A.; Belterman, C.N.W.; Coronel, R.; Fiolet, J.W.T. [Na+]i and the driving force of the Na+/Ca2+-exchanger in heart failure. Cardiovasc. Res. 2003, 57, 986–995. [Google Scholar] [CrossRef]
- Zahradníková, A.; Valent, I.; Zahradník, I. Frequency and release flux of calcium sparks in rat cardiac myocytes: A relation to RYR gating. J. Gen. Physiol. 2010, 136, 101–116. [Google Scholar] [CrossRef]
- Neco, P.; Rose, B.; Huynh, N.; Zhang, R.; Bridge, J.H.; Philipson, K.D.; Goldhaber, J.I. Sodium-calcium exchange is essential for effective triggering of calcium release in mouse heart. Biophys. J. 2010, 99, 755–764. [Google Scholar] [CrossRef] [PubMed]
- Ottolia, M.; Torres, N.; Bridge, J.H.; Philipson, K.D.; Goldhaber, J.I. Na/Ca exchange and contraction of the heart. J. Mol. Cell Cardiol 2013, 61, 28–33. [Google Scholar] [CrossRef] [PubMed]
- Chu, L.; Greenstein, J.L.; Winslow, R.L. Modeling Na(+)-Ca(2+) exchange in the heart: Allosteric activation, spatial localization, sparks and excitation-contraction coupling. J. Mol. Cell Cardiol. 2016, 99, 174–187. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Armoundas, A.A.; Hobai, I.A.; Tomaselli, G.F.; Winslow, R.L.; O’Rourke, B. Role of sodium-calcium exchanger in modulating the action potential of ventricular myocytes from normal and failing hearts. Circ. Res. 2003, 93, 46–53. [Google Scholar] [CrossRef]
- Respress, J.L.; van Oort, R.J.; Li, N.; Rolim, N.; Dixit, S.S.; de Almeida, A.; Voigt, N.; Lawrence, W.S.; Skapura, D.G.; Skardal, K.; et al. Role of RyR2 phosphorylation at S2814 during heart failure progression. Circ. Res. 2012, 110, 1474–1483. [Google Scholar] [CrossRef]
- Sikkel, M.B.; Collins, T.P.; Rowlands, C.; Shah, M.; O’Gara, P.; Williams, A.J.; Harding, S.E.; Lyon, A.R.; MacLeod, K.T. Flecainide reduces Ca(2+) spark and wave frequency via inhibition of the sarcolemmal sodium current. Cardiovasc. Res. 2013, 98, 286–296. [Google Scholar] [CrossRef]
- Hove-Madsen, L.; Llach, A.; Bayes-Genis, A.; Roura, S.; Rodriguez Font, E.; Aris, A.; Cinca, J. Atrial fibrillation is associated with increased spontaneous calcium release from the sarcoplasmic reticulum in human atrial myocytes. Circulation 2004, 110, 1358–1363. [Google Scholar] [CrossRef]
- Bers, D.M. Cardiac sarcoplasmic reticulum calcium leak: Basis and roles in cardiac dysfunction. Annu. Rev. Physiol. 2014, 76, 107–127. [Google Scholar] [CrossRef]
- Williams, G.S.; Chikando, A.C.; Tuan, H.T.; Sobie, E.A.; Lederer, W.J.; Jafri, M.S. Dynamics of calcium sparks and calcium leak in the heart. Biophys. J. 2011, 101, 1287–1296. [Google Scholar] [CrossRef]
- Eisner, D.A.; Caldwell, J.L.; Trafford, A.W.; Hutchings, D.C. The Control of Diastolic Calcium in the Heart: Basic Mechanisms and Functional Implications. Circ. Res. 2020, 126, 395–412. [Google Scholar] [CrossRef]
- Ozdemir, S.; Bito, V.; Holemans, P.; Vinet, L.; Mercadier, J.J.; Varro, A.; Sipido, K.R. Pharmacological inhibition of na/ca exchange results in increased cellular Ca2+ load attributable to the predominance of forward mode block. Circ. Res. 2008, 102, 1398–1405. [Google Scholar] [CrossRef] [PubMed]
- Kubalova, Z.; Terentyev, D.; Viatchenko-Karpinski, S.; Nishijima, Y.; Gyorke, I.; Terentyeva, R.; da Cunha, D.N.; Sridhar, A.; Feldman, D.S.; Hamlin, R.L.; et al. Abnormal intrastore calcium signaling in chronic heart failure. Proc. Nat. Acad. Sci. USA 2005, 102, 14104–14109. [Google Scholar] [CrossRef] [PubMed]
- Antoons, G.; Willems, R.; Sipido, K.R. Alternative strategies in arrhythmia therapy: Evaluation of Na/Ca exchange as an anti-arrhythmic target. Pharmacol. Ther. 2012, 134, 26–42. [Google Scholar] [CrossRef] [PubMed]
- Melenovsky, V.; Hwang, S.J.; Redfield, M.M.; Zakeri, R.; Lin, G.; Borlaug, B.A. Left atrial remodeling and function in advanced heart failure with preserved or reduced ejection fraction. Circ. Heart Fail. 2015, 8, 295–303. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| n = 46 | |
| Male gender, n (%) | 40 (87) |
| Age (years), mean ± SD | 68.8 ± 7.7 |
| Body mass index (kg/m2), median [IQR] | 28.6 [6.6] n = 35 |
| Coronary heart disease, n (%) | 44 (95.7) |
| LVEF (%), median (IQR) | 60 [14.5] n = 40 |
| HFpEF, n (%) | 24 (52.2) |
| Atrial fibrillation, n (%) | 3 (6.5) |
| GFR (mL/min), mean ± SD | 70.6 ± 21.5 n = 44 |
| Type of surgery | |
| CABG, n (%) | 44 (95.7) |
| Aortic valve replacement, n (%) | 6 (13) |
| Mitral valve replacement, n (%) | 1 (2.2) |
| Cardiovascular risk factors | |
| Arterial hypertension, n (%) | 37 (88.1) |
| Hypercholesterolaemia, n (%) | 19 (41.3) |
| Diabetes mellitus, n (%) | 3 (7.7) n = 39 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hegner, P.; Drzymalski, M.; Biedermann, A.; Memmel, B.; Durczok, M.; Wester, M.; Floerchinger, B.; Provaznik, Z.; Schmid, C.; Zausig, Y.; et al. SAR296968, a Novel Selective Na+/Ca2+ Exchanger Inhibitor, Improves Ca2+ Handling and Contractile Function in Human Atrial Cardiomyocytes. Biomedicines 2022, 10, 1932. https://doi.org/10.3390/biomedicines10081932
Hegner P, Drzymalski M, Biedermann A, Memmel B, Durczok M, Wester M, Floerchinger B, Provaznik Z, Schmid C, Zausig Y, et al. SAR296968, a Novel Selective Na+/Ca2+ Exchanger Inhibitor, Improves Ca2+ Handling and Contractile Function in Human Atrial Cardiomyocytes. Biomedicines. 2022; 10(8):1932. https://doi.org/10.3390/biomedicines10081932
Chicago/Turabian StyleHegner, Philipp, Marzena Drzymalski, Alexander Biedermann, Bernadette Memmel, Melanie Durczok, Michael Wester, Bernhard Floerchinger, Zdenek Provaznik, Christof Schmid, York Zausig, and et al. 2022. "SAR296968, a Novel Selective Na+/Ca2+ Exchanger Inhibitor, Improves Ca2+ Handling and Contractile Function in Human Atrial Cardiomyocytes" Biomedicines 10, no. 8: 1932. https://doi.org/10.3390/biomedicines10081932
APA StyleHegner, P., Drzymalski, M., Biedermann, A., Memmel, B., Durczok, M., Wester, M., Floerchinger, B., Provaznik, Z., Schmid, C., Zausig, Y., Maier, L. S., & Wagner, S. (2022). SAR296968, a Novel Selective Na+/Ca2+ Exchanger Inhibitor, Improves Ca2+ Handling and Contractile Function in Human Atrial Cardiomyocytes. Biomedicines, 10(8), 1932. https://doi.org/10.3390/biomedicines10081932