
Impact of R-Carvedilol on β2-Adrenergic Receptor-Mediated Spontaneous Calcium Release in Human Atrial Myocytes

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Study Protocol
2.3. In Vitro Drug Testing
2.4. Immunofluorescent Labeling
2.5. Confocal Calcium Imaging
2.6. Data Analysis
2.7. Statistical Analysis
3. Results
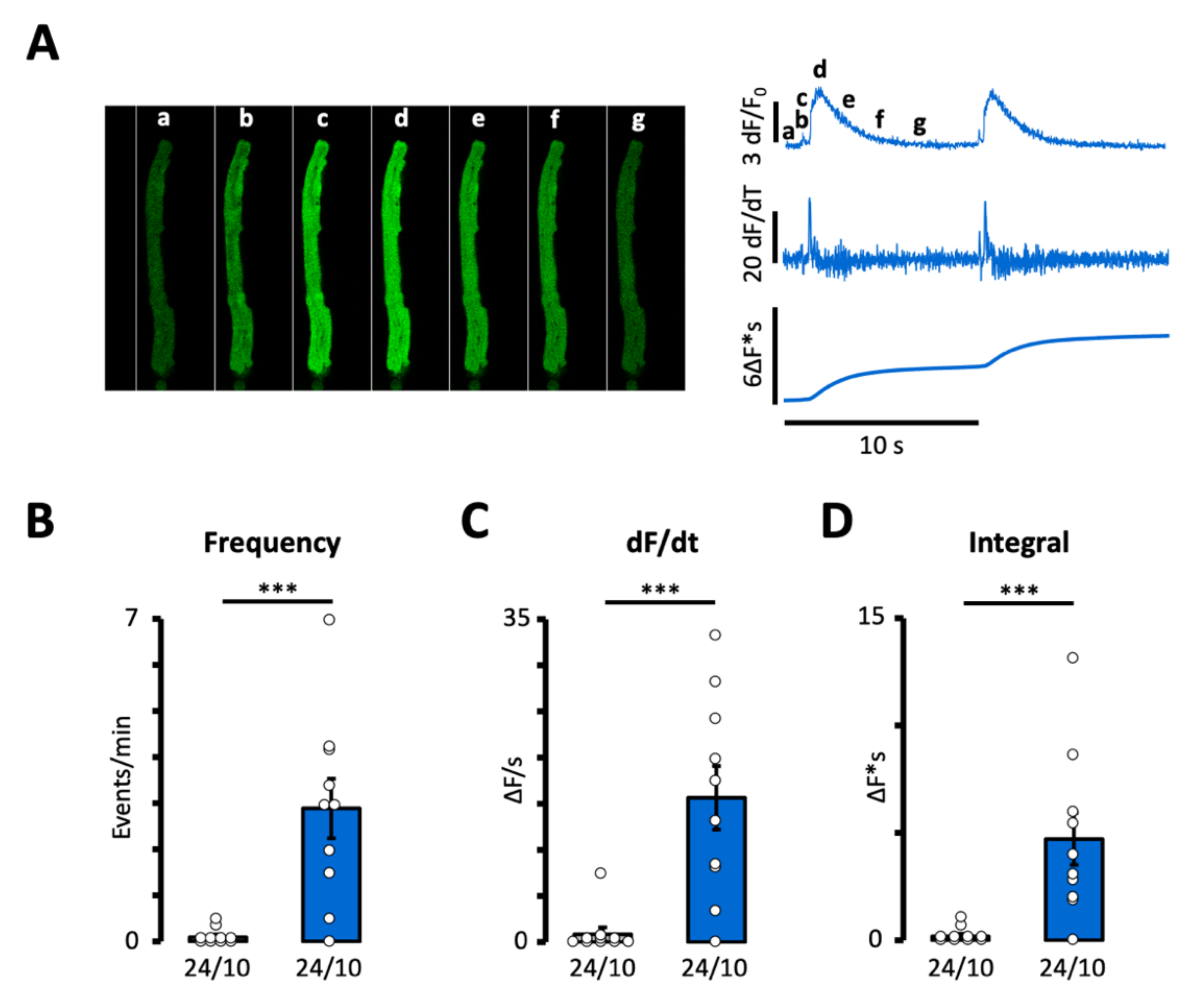
3.1. Impact of β2-Adrenergic Stimulation on Intracellular Calcium Homeostasis in Human Atrial Myocytes
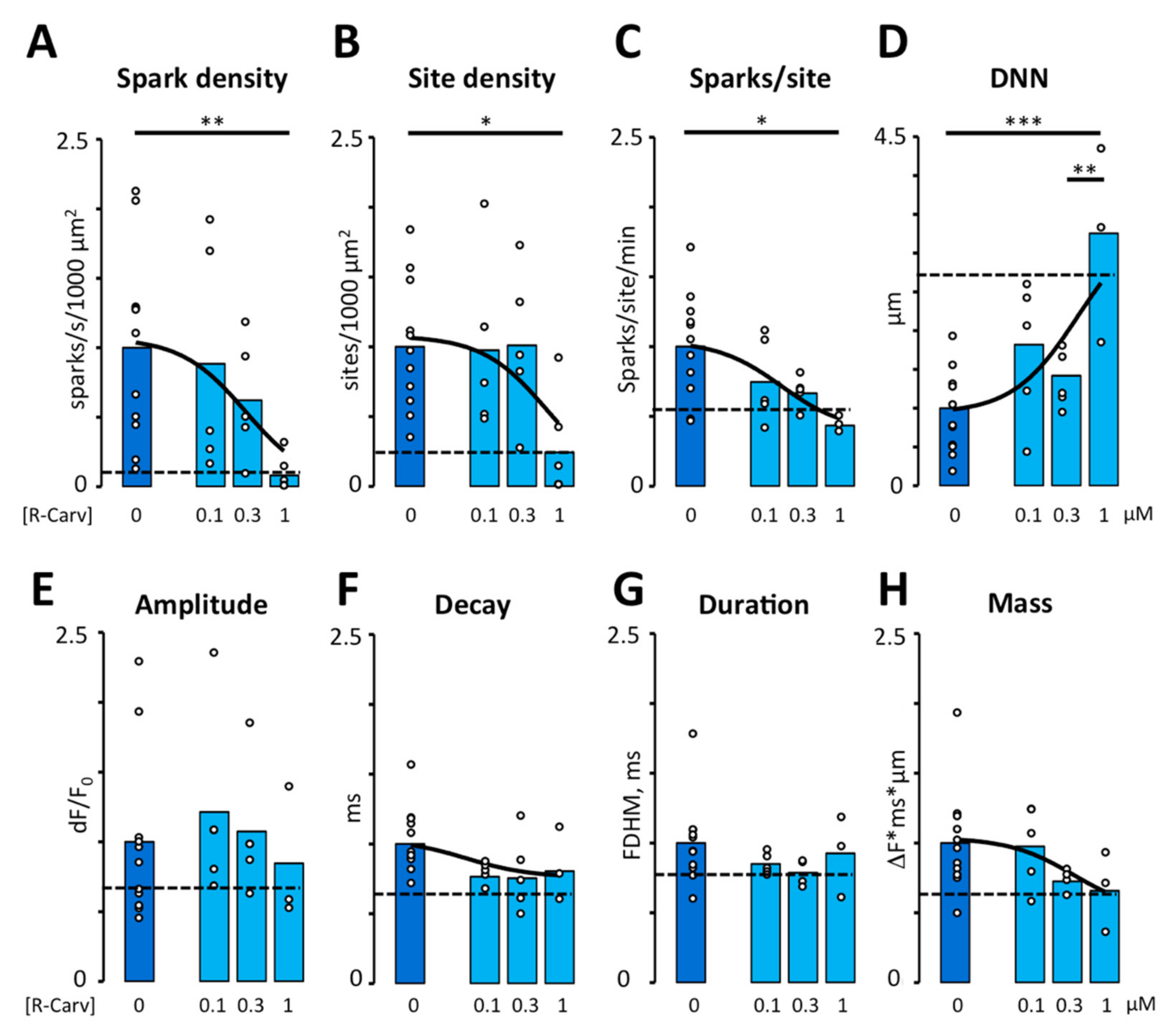
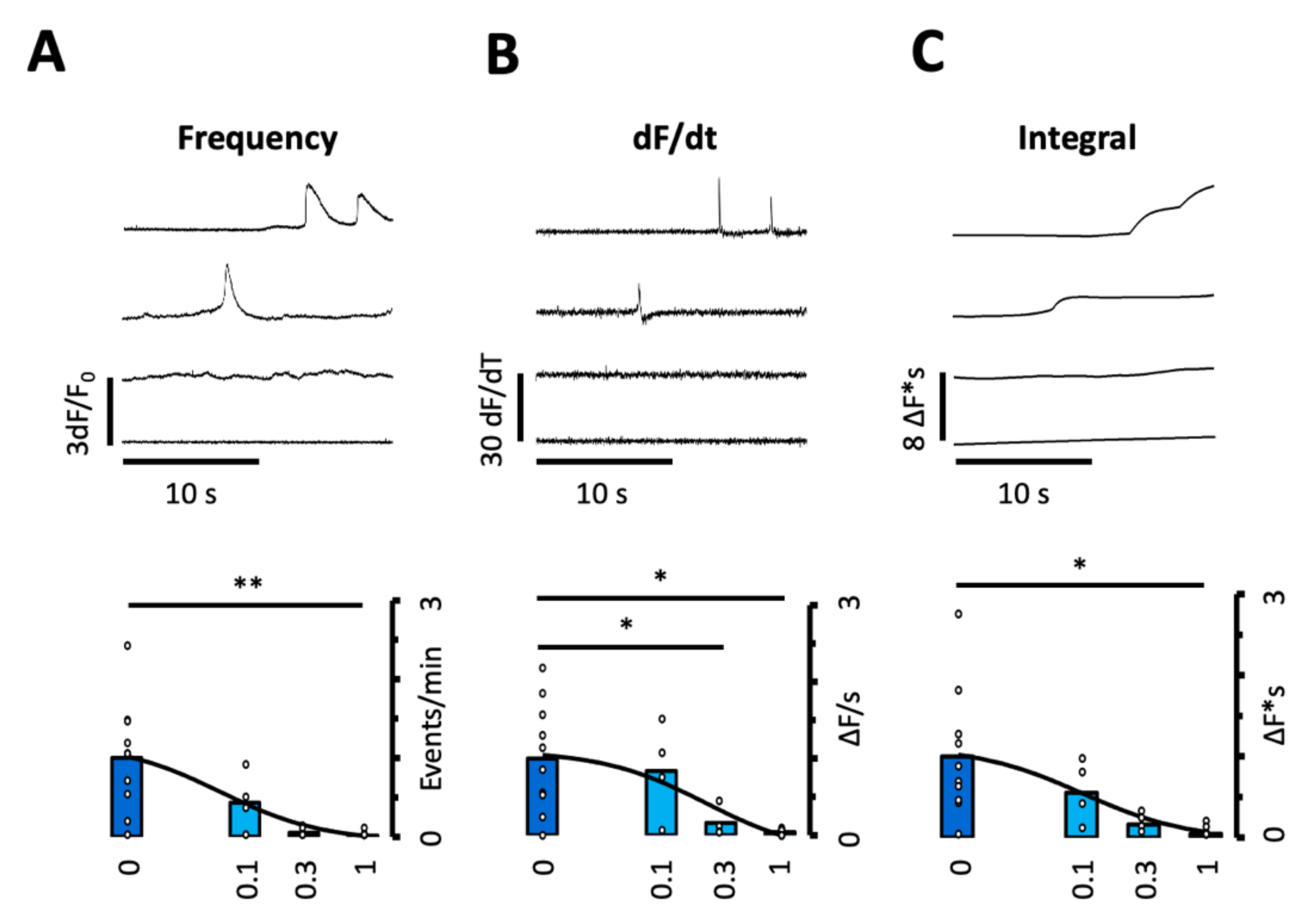
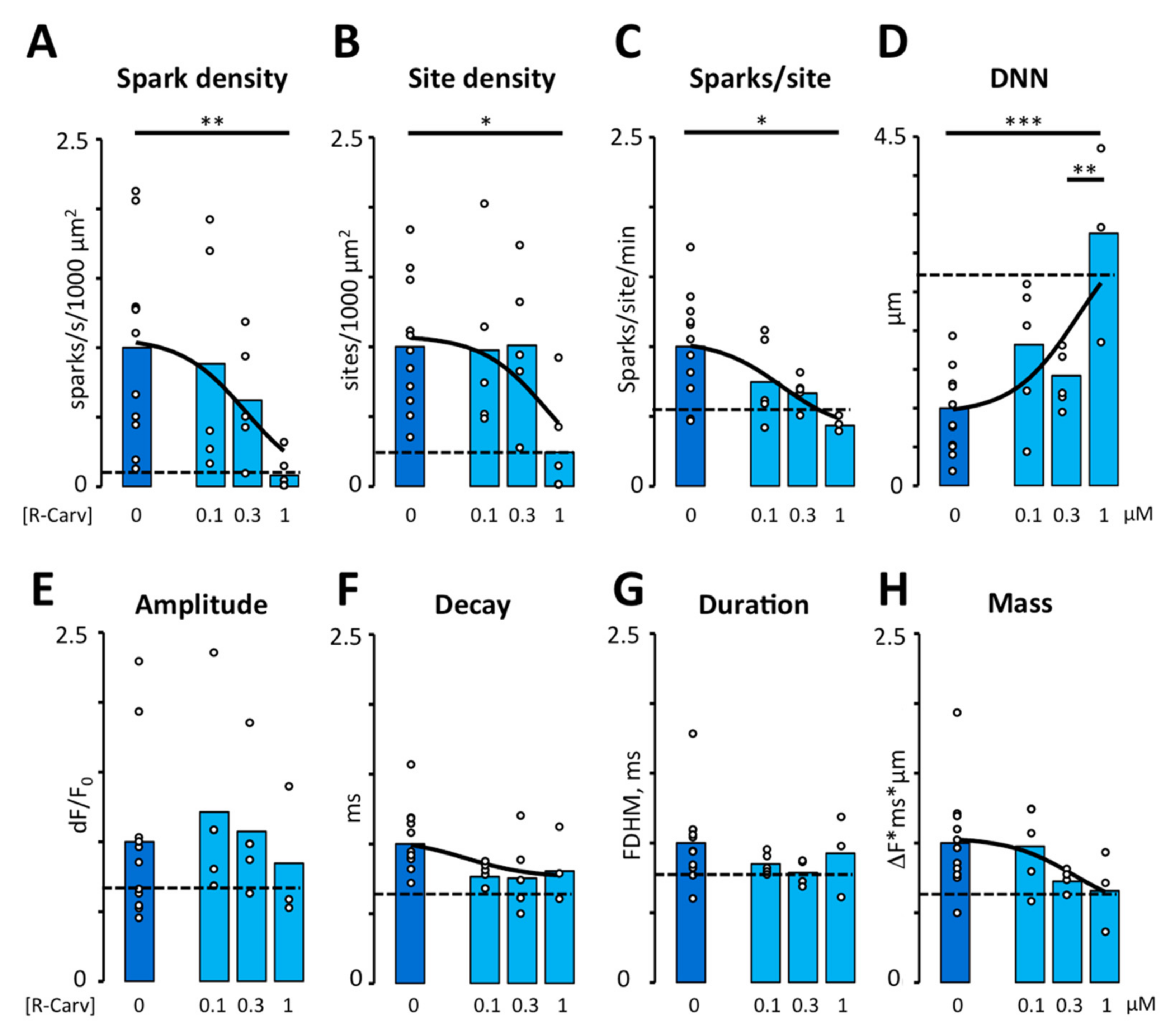
3.2. R-Carvedilol Dose-Dependently Reverses β2-Adrenergic Stimulation of Spontaneous Ca2+ Release
3.3. Impact of R- and S-Carvedilol Enantiomers on β2-Adrenergic Stimulation of RyR Phosphorylation at Ser-2808
4. Discussion
4.1. Impact of β2-Adrenergic Stimulation on Intracellular Calcium Homeostasis in Human Atrial Myocytes
4.2. Ability of R- and S-Carvedilol Enantiomers to Reverse the Effects of β2-Adrenergic Stimulation on Ca2+ Homeostasis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gould, P.A.; Yii, M.; Mclean, C.; Finch, S.; Marshall, T.; Lambert, G.W.; Kaye, D.M. Evidence for Increased Atrial Sympathetic Innervation in Persistent Human Atrial Fibrillation. Pacing Clin. Electrophysiol. 2006, 29, 821–829. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, B.L.; Fishbein, M.C.; Chen, L.S.; Chen, P.S.; Masroor, S. Histopathological Substrate for Chronic Atrial Fibrillation in Humans. Hear. Rhythm 2009, 6, 454–460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, P.S.; Chen, L.S.; Fishbein, M.C.; Lin, S.F.; Nattel, S. Role of the Autonomic Nervous System in Atrial Fibrillation: Pathophysiology and Therapy. Circ. Res. 2014, 114, 1500–1515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pfenniger, A.; Arora, R. Beyond Beta-Blockers: Targeting the Sympathetic Nervous System for the Prevention and Treatment of Atrial Fibrillation. Cardiovasc. Res. 2019, 115, 1940–1942. [Google Scholar] [CrossRef] [PubMed]
- Reiken, S.; Wehrens, X.H.T.; Vest, J.A.; Barbone, A.; Klotz, S.; Mancini, D.; Burkhoff, D.; Marks, A.R. Β-Blockers Restore Calcium Release Channel Function and Improve Cardiac Muscle Performance in Human Heart Failure. Circulation 2003, 107, 2459–2466. [Google Scholar] [CrossRef]
- Nattel, S.; Dobrev, D. The Multidimensional Role of Calcium in Atrial Fibrillation Pathophysiology: Mechanistic Insights and Therapeutic Opportunities. Eur. Heart J. 2012, 33, 1870–1877. [Google Scholar] [CrossRef] [Green Version]
- Wakili, R.; Voigt, N.; Kääb, S.; Dobrev, D.; Nattel, S. Recent Advances in the Molecular Pathophysiology of Atrial Fibrillation. J. Clin. Investig. 2011, 121, 2955–2968. [Google Scholar] [CrossRef] [Green Version]
- Dobrev, D.; Voigt, N.; Wehrens, X.H.T. The Ryanodine Receptor Channel as a Molecular Motif in Atrial Fibrillation: Pathophysiological and Therapeutic Implications. Cardiovasc. Res. 2011, 89, 734–743. [Google Scholar] [CrossRef] [Green Version]
- Neef, S.; Dybkova, N.; Sossalla, S.; Ort, K.R.; Fluschnik, N.; Neumann, K.; Seipelt, R.; Schöndube, F.A.; Hasenfuss, G.; Maier, L.S. CaMKII-Dependent Diastolic SR Ca2+ Leak and Elevated Diastolic Ca2+ Levels in Right Atrial Myocardium of Patients with Atrial Fibrillation. Circ. Res. 2010, 106, 1134–1144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vest, J.A.; Wehrens, X.H.T.; Reiken, S.R.; Lehnart, S.E.; Dobrev, D.; Chandra, P.; Danilo, P.; Ravens, U.; Rosen, M.R.; Marks, A.R. Defective Cardiac Ryanodine Receptor Regulation during Atrial Fibrillation. Circulation 2005, 111, 2025–2032. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Llach, A.; Molina, C.E.; Prat-Vidal, C.; Fernandes, J.; Casadó, V.; Ciruela, F.; Lluís, C.; Franco, R.; Cinca, J.; Hove-Madsen, L. Abnormal Calcium Handling in Atrial Fibrillation Is Linked to Up-Regulation of Adenosine A 2A Receptors. Eur. Heart J. 2011, 32, 721–729. [Google Scholar] [CrossRef] [Green Version]
- Nolla-Colomer, C.; Casabella-Ramon, S.; Jimenez-Sabado, V.; Vallmitjana, A.; Tarifa, C.; Herraiz-Martínez, A.; Llach, A.; Tauron, M.; Montiel, J.; Cinca, J.; et al. Β2-Adrenergic Stimulation Potentiates Spontaneous Calcium Release By Increasing Signal Mass and Co-Activation of Ryanodine Receptor Clusters. Acta Physiol. 2022, 234, e13736. [Google Scholar] [CrossRef]
- Yoshikawa, T.; Port, J.D.; Asano, K.; Chidiak, P.; Bouvier, M.; Dutcher, D.; Roden, R.L.; Minobe, W.; Tremmel, K.D.; Bristow, M.R. Cardiac Adrenergic Receptor Effects of Carvedilol. Eur. Heart J. 1996, 17, 8–16. [Google Scholar] [CrossRef]
- Zhou, Q.; Xiao, J.; Jiang, D.; Wang, R.; Vembaiyan, K.; Wang, A.; Smith, C.D.; Xie, C.; Chen, W.; Zhang, J.; et al. Carvedilol and Its New Analogs Suppress Arrhythmogenic Store Overload-Induced Ca 2+ Release. Nat. Med. 2011, 17, 1003–1009. [Google Scholar] [CrossRef] [Green Version]
- Smith, C.D.; Wang, A.; Vembaiyan, K.; Zhang, J.; Xie, C.; Zhou, Q.; Wu, G.; Chen, S.R.W.; Back, T.G. Novel Carvedilol Analogs That Suppress Store Overload Induced Ca2+ Release. J. Med. Chem. 2013, 56, 8626–8655. [Google Scholar] [CrossRef] [Green Version]
- Bristow, M.R.; Gilbert, E.M.; Abraham, W.T.; Adams, K.F.; Fowler, M.B.; Hershberger, R.E.; Kubo, S.H.; Narahara, K.A.; Ingersoll, H.; Krueger, S.; et al. Carvedilol Produces Dose-Related Improvements in Left Ventricular Function and Survival in Subjects with Chronic Heart Failure. Circulation 1996, 94, 2807–2816. [Google Scholar] [CrossRef]
- Ko, D.T.; Herbert, P.R.; Coffey, C.S.; Curtis, J.P.; Foody, J.M.; Sedrakyan, A.; Krumholz, H.M. Adverse Effects of Beta-Blocker Therapy for Patients with Heart Failure. A Quantitative Overview of Randomized Trials. Arch. Intern. Med. 2004, 164, 1389–1394. [Google Scholar] [CrossRef] [Green Version]
- Bartsch, W.; Sponer, G.; Strein, K.; Müller-Beckmann, B.; Kling, L.; Böhm, E.; Martin, U.; Borbe, H.O. Pharmacological Characteristics of the Stereoisomers of Carvedilol. Eur. J. Clin. Pharmacol. 1990, 38, 104–107. [Google Scholar] [CrossRef]
- Frishman, W.H. Carvedilol. N. Engl. J. Med. 1998, 339, 1759–1765. [Google Scholar] [CrossRef]
- Stoschitzky, K.; Koshucharova, G.; Lercher, P.; Maier, R.; Sakotnik, A.; Klein, W.; Liebmann, P.M.; Lindner, W. Stereoselective Effects of (R)- and (S)-Carvedilol in Humans. Chirality 2001, 13, 342–346. [Google Scholar] [CrossRef]
- Zhang, J.; Zhou, Q.; Smith, C.D.; Chen, H.; Tan, Z.; Chen, B.; Nani, A.; Wu, G.; Song, L.-S.; Fill, M.; et al. Non-β-Blocking R -Carvedilol Enantiomer Suppresses Ca2+ Waves and Stress-Induced Ventricular Tachyarrhythmia without Lowering Heart Rate or Blood Pressure. Biochem. J. 2015, 470, 233–242. [Google Scholar] [CrossRef] [Green Version]
- Herraiz-Martínez, A.; Llach, A.; Tarifa, C.; Gandía, J.; Jiménez-Sabado, V.; Lozano-Velasco, E.; Serra, S.A.; Vallmitjana, A.; Vázquez Ruiz De Castroviejo, E.; Benítez, R.; et al. The 4q25 Variant Rs13143308T Links Risk of Atrial Fibrillation to Defective Calcium Homoeostasis. Cardiovasc. Res. 2019, 115, 578–589. [Google Scholar] [CrossRef] [Green Version]
- Herraiz-Martínez, A.; Tarifa, C.; Jiménez-Sábado, V.; Llach, A.; Godoy-Marín, H.; Colino, H.; Nolla-Colomer, C.; Casabella, S.; Izquierdo-Castro, P.; Benítez, I.; et al. Influence of Sex on Intracellular Calcium Homeostasis in Patients with Atrial Fibrillation. Cardiovasc. Res. 2021, 118, 1033–1045. [Google Scholar] [CrossRef]
- Beasley, R.; Pearce, N.; Crane, J.; Burgess, C. β -Agonists: What Is the Evidence That Their Use Increases the Risk of Asthma Morbidity and Mortality? J. Allergy Clin. Immunol. 1999, 104, 18–30. [Google Scholar] [CrossRef]
- Beasley, R.; Nishima, S.; Pearce, N.; Crane, J. Beta-Agonist Therapy and Asthma Mortality in Japan. Lancet 1998, 351, 1406–1407. [Google Scholar] [CrossRef]
- Workman, A.J.; Pau, D.; Redpath, C.J.; Marshall, G.E.; Russell, J.A.; Kane, K.A.; Norrie, J.; Rankin, A.C. Post-Operative Atrial Fibrillation Is Influenced by Beta-Blocker Therapy but Not by Pre-Operative Atrial Cellular Electrophysiology. J. Cardiovasc. Electrophysiol. 2006, 17, 1230–1238. [Google Scholar] [CrossRef] [Green Version]
- Baltogiannis, G.G.; Lysitsas, D.N.; di Giovanni, G.; Ciconte, G.; Sieira, J.; Conte, G.; Kolettis, T.M.; Chierchia, G.; De Asmundis, C.; Brugada, P. CPVT: Arrhythmogenesis, Therapeutic Management, and Future Perspectives. A Brief Review of the Literature. Front. Cardiovasc. Med. 2019, 6, 92. [Google Scholar] [CrossRef]
- Triposkiadis, F.; Karayannis, G.; Giamouzis, G.; Skoularigis, J.; Louridas, G.; Butler, J. The Sympathetic Nervous System in Heart Failure. Physiology, Pathophysiology, and Clinical Implications. J. Am. Coll. Cardiol. 2009, 54, 1747–1762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bylund, D.B.; Eikenberg, D.C.; Hieble, J.P.; Langer, S.Z.; Lefkowitz, R.J.; Minneman, K.P.; Molinoff, P.B.; Ruffolo, R.R.; Trendelenburg, U. International Union of Pharmacology Nomenclature of Adrenoceptors. Pharmacol. Rev. 1994, 46, 121–136. [Google Scholar] [CrossRef] [PubMed]
- Smith, C.; Teitler, M. Beta-Blocker Selectivity at Cloned Human Beta 1- and Beta 2- Adrenergic Receptors. Cardiovasc. Drugs Ther. 1999, 13, 123–126. [Google Scholar] [CrossRef] [PubMed]
- Baker, J.G. The Selectivity of b -Adrenoceptor Agonists at Human b 1-, b 2- and b 3- Adrenoceptors. Br. J. Pharmacol. 2010, 160, 1048–1061. [Google Scholar] [CrossRef] [Green Version]
- Agarwal, S.R.; Sherpa, R.T.; Moshal, K.S.; Harvey, R.D. Compartmentalized CAMP Signaling in Cardiac Ventricular Myocytes. Cell. Signal. 2022, 89, 110172. [Google Scholar] [CrossRef]
- Wang, Y.; Shi, Q.; Li, M.; Zhao, M.; Reddy Gopireddy, R.; Teoh, J.P.; Xu, B.; Zhu, C.; Ireton, K.E.; Srinivasan, S.; et al. Intracellular Β1-Adrenergic Receptors and Organic Cation Transporter 3 Mediate Phospholamban Phosphorylation to Enhance Cardiac Contractility. Circ. Res. 2021, 128, 246–261. [Google Scholar] [CrossRef]
- Maruyama, M.; Xiao, J.; Zhou, Q.; Vembaiyan, K.; Chua, S.-K.; Rubart-von der Lohe, M.; Lin, S.-F.; Back, T.G.; Wayne Chen, S.; Chen, P.-S. Carvedilol Analogue Inhibits Triggered Activities Evoked by Both Early and Delayed Afterdepolarizations. Hear. Rhythm 2013, 10, 101–107. [Google Scholar] [CrossRef] [Green Version]
- Peltenburg, P.J.; Kallas, D.; Bos, J.M.; Lieve, K.V.V.; Franciosi, S.; Roston, T.M.; Denjoy, I.; Sorensen, K.B.; Ohno, S.; Roses-Noguer, F.; et al. An International Multicenter Cohort Study on β -Blockers for the Treatment of Symptomatic Children With Catecholaminergic Polymorphic. Circulation 2022, 145, 333–344. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| (37 Patients) | ||
|---|---|---|
| Age, Years | 67.0 [65.0; 69.0] | |
| Sex (Female/Male) | 16/21 (43.2%/56.8%) | |
| Echocardiography | LAD index | 2.35 [2.27; 2.43] |
| LVEF, % | 55.0 [53.0; 57.0] | |
| Cardiovascular Risk Factors | No Smoking | 16 (43.2%) |
| Smoking | 9 (24.3%) | |
| Ex smoking | 11 (29.7%) | |
| Hypertension | 21 (56.8%) | |
| Diabetes | 8 (21.6%) | |
| Dyslipidemia | 24 (64.9%) | |
| Surgical Treatment | AVR | 16 (43.2%) |
| MVR | 3 (8.1%) | |
| CABG | 26 (70.3%) | |
| Pharmacological Treatment | ACE inhibitor | 14 (37.8%) |
| ARB | 6 (16.2%) | |
| Calcium antagonists | 9 (24.3%) | |
| β-blockers | 19 (51.4%) | |
| Acetylsalicylic acid | 21 (56.8%) | |
| Statins | 26 (70.3%) | |
| More than one treatment | 27 (73.0%) |
| Properties | Fenoterol | Isoproterenol |
|---|---|---|
| CALCIUM SPARKS (cells/patients) | (45/11) | (30/9) |
| Density (events/s/1000 µm2) | 0.52 ± 0.11 | 0.53 ± 0.12 |
| Site density (sites/1000 µm2) | 9.55 ± 1.36 | 11.5 ± 1.1 |
| Sparks/site (events/s) | 0.042 ± 0.005 | 0.039 ± 0.011 |
| Distance to nearest neighbor (µm) | 2.39 ± 0.39 | 3.66 ± 0.64 |
| Amplitude (ΔF/F0) | 1.48 ± 0.21 | 1.23 ± 0.16 |
| Rate of Rise (ΔF/F0/s) | 0.025 ± 0.004 | 0.028 ± 0.003 |
| Tau (ms) | 55.4 ± 3.8 | 43.3 ± 3.6 * |
| FDHM (ms) 1 | 65.7 ± 5.4 | 56.9 ± 2.8 |
| FWHM (µm) 2 | 3.06 ± 0.16 | 2.44 ± 0.19 * |
| Mass (∆F × ms × µm) | 289 ± 43 | 182 ± 27 * |
| CALCIUM WAVES 3 | ||
| Frequency (events/min) | 2.89 ± 0.65 | 1.98 ± 0.94 |
| Properties | Maximum | Minimum | IC-50 1 |
|---|---|---|---|
| Spark density | 1.06 ± 0.21 | 0 ± 0.67 | 0.30 ± 0.60 |
| Site density | 1.07 ± 0.16 | 0 ± 1.35 | 0.70 ± 1.95 |
| Sparks/site (events/s) | 1.03 ± 0.12 | 0.38 ± 0.29 | 0.17 ± 0.25 |
| Distance to nearest neighbor (µm) | 3.5 ± 1.62 | 0.99 ± 0.26 | 0.48 ± 0.71 |
| Tau (ms) | 1.0 ± 0.18 | 0.73 ± 0.14 | 0.06 ± 0.17 |
| Mass (∆F × ms × µm) | 1.03 ± 0.11 | 0.49 ± 0.52 | 0.37 ± 0.91 |
| Wave frequency 2 | 1.18 ± 0.31 | −0.09 ± 0.26 | 0.06 ± 0.08 |
| dF/dt | 1.08 ± 0.20 | −0.25 ± 0.49 | 0.23 ± 0.31 |
| Wave area | 1.11 ± 0.27 | −0.08 ± 0.34 | 0.10 ± 0.15 |
| Ser-2808/RyR total | 1.03 ± 0.06 | 0.54 ± 0.15 | 0.36 ± 0.41 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Casabella-Ramón, S.; Jiménez-Sábado, V.; Tarifa, C.; Casellas, S.; Lu, T.T.; Izquierdo-Castro, P.; Gich, I.; Jiménez, M.; Ginel, A.; Guerra, J.M.; et al. Impact of R-Carvedilol on β2-Adrenergic Receptor-Mediated Spontaneous Calcium Release in Human Atrial Myocytes. Biomedicines 2022, 10, 1759. https://doi.org/10.3390/biomedicines10071759
Casabella-Ramón S, Jiménez-Sábado V, Tarifa C, Casellas S, Lu TT, Izquierdo-Castro P, Gich I, Jiménez M, Ginel A, Guerra JM, et al. Impact of R-Carvedilol on β2-Adrenergic Receptor-Mediated Spontaneous Calcium Release in Human Atrial Myocytes. Biomedicines. 2022; 10(7):1759. https://doi.org/10.3390/biomedicines10071759
Chicago/Turabian StyleCasabella-Ramón, Sergi, Verónica Jiménez-Sábado, Carmen Tarifa, Sandra Casellas, Tien Tina Lu, Paloma Izquierdo-Castro, Ignasi Gich, Marcel Jiménez, Antonino Ginel, José M. Guerra, and et al. 2022. "Impact of R-Carvedilol on β2-Adrenergic Receptor-Mediated Spontaneous Calcium Release in Human Atrial Myocytes" Biomedicines 10, no. 7: 1759. https://doi.org/10.3390/biomedicines10071759
APA StyleCasabella-Ramón, S., Jiménez-Sábado, V., Tarifa, C., Casellas, S., Lu, T. T., Izquierdo-Castro, P., Gich, I., Jiménez, M., Ginel, A., Guerra, J. M., Chen, S. R. W., Benítez, R., & Hove-Madsen, L. (2022). Impact of R-Carvedilol on β2-Adrenergic Receptor-Mediated Spontaneous Calcium Release in Human Atrial Myocytes. Biomedicines, 10(7), 1759. https://doi.org/10.3390/biomedicines10071759