2. Materials and Methods
2.1. Systematic Literature Search
A retrospective post-hoc analysis using Individual Patients’ Data (IPD) from previously published clinical trials was conducted. Thus, the study consisted of two steps: in the first one, a systematic search of the literature was performed; in the second step, data derived from the clinical trials identified were analysed.
During the first step, a comprehensive systematic literature search for English-language articles in MEDLINE (PubMed) and EMBASE was conducted. The literature search was performed using the following keywords: male infertility, couple infertility, FSH, FSH administration, sperm DNA fragmentation index, sDF and testosterone. The Boolean functions AND and OR were used to combine keywords.
The following inclusion criteria were established before the literature search: (i) clinical trials (ii) in which the male partner of infertile couples was treated with FSH and both (iii) sDF index and (iv) testosterone serum levels were reported. Considering the rich literature on FSH application in male idiopathic infertility, keywords and inclusion criteria were set to detect only those studies in which both testosterone and sDF after treatment were reported.
Men enrolled showed idiopathic infertility, with one or more sperm parameters altered, in whom no specific causes of male infertility were detected. Retrospective studies were not included. No other inclusion/exclusion criteria were provided.
The corresponding author of each eligible trial was contacted to obtain raw data. When the author accepted, IPD were collected, considering the following specific endpoints: sDF index; testosterone serum levels (measured both before and after FSH administration); patient’s age; body mass index (BMI); FSH dosages; treatment duration; conventional semen analysis parameters (such as sperm concentration, total sperm count, progressive sperm motility, total sperm motility and sperm morphology); hormonal evaluations (such as FSH, luteinizing hormone (LH), inhibin B, sex hormone binding globulin (SHBG) and anti-Mullerian hormone (AMH)); couple infertility duration; number of pregnancies obtained, both spontaneous and after assisted reproduction (if available).
IPD obtained by each study were combined in a single dataset and descriptive analyses were conducted.
2.2. Identification of FSH Administration Efficacy in Men with Idiopathic Infertility
The final dataset generated on IPD extracted following the systematic literature search was evaluated to reach primary and secondary endpoints. In detail, the primary endpoint was the potential correlation between testosterone serum levels and sDF change after FSH treatment. Secondary endpoints were (i) sDF decrease after FSH administration and (ii) to determine whether testosterone serum levels could predict the sDF decrease after FSH administration.
2.2.1. Endpoints’ Definitions
As previously reported, the efficacy of FSH administration is associated with sDF index decrease. This improvement was recorded in each study considered alone (or “as a unit”). Here, we analysed IPD to quantify the comprehensive sDF decrease after FSH administration, comparing pre- and post-treatment values.
Similarly, the pre- and post-FSH treatment change in secondary endpoints was evaluated.
In order to better define a successful treatment, the entire cohort was divided into responders and non-responders to FSH. Responders were empirically defined as men in whom the sDF index decreased by at least 20% (relative decrease) of baseline levels after treatment. This threshold was empirically adopted to highlight a clinically significant sDF reduction.
2.2.2. Statistical Analysis
Statistical procedures were applied to the dataset to reach the secondary objectives of the study.
In order to determine the correlation between testosterone serum levels and sDF change after FSH treatment, correlation analyses were performed, combining testosterone serum levels and sDF at baseline and after FSH administration. Data were first analysed for distribution with Kolmogorov–Smirnov test and correlations were assessed using Pearson’s or Spearman’s methods for normally or not-normally distributed data, respectively. Correlation analyses were performed by considering anthropometric variables, hormones, semen parameters and sDF index, and by applying Bonferroni adjustment. Since 14 variables were considered,
p < 0.003 was considered for statistical significance in correlation analyses. Moreover, multivariate stepwise linear regression analyses were performed, using sDF index as the dependent variable and testosterone, FSH, LH, SHBG, inhibin B, AMH, FSH treatment duration, patient’s age and BMI as independent parameters. In order to correct potential confounders, multiple models were used to yield total-effect estimates for covariates [
20].
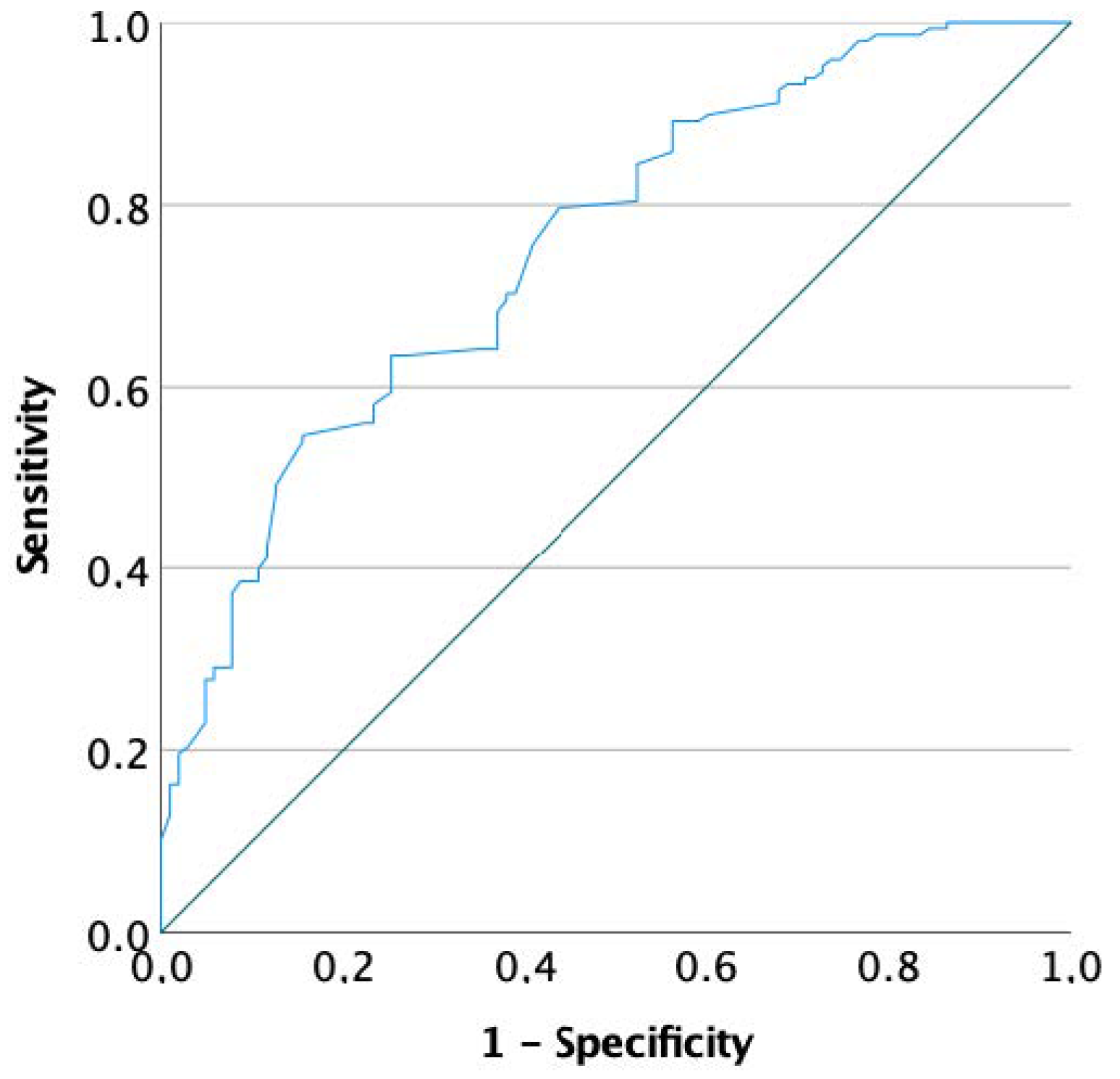
Moreover, to determine the change in hormone levels to classify a man with and without significant sDF decrease, the entire cohort was considered by dividing patients into responders and non-responders, according to sDF change after FSH administration. Then, logistic regression analyses were performed using the responders/non-responders classification as the dependent variable. Conventional semen parameters, patients’ age, BMI, FSH dosage, treatment duration and hormones collected after FSH administration were included among co-variates. Logistic regression analyses were repeated considering baseline parameters to identify potential predictors of FSH effectiveness. In this setting, to graphically show the connection/trade-off between clinical sensitivity and specificity for every possible cut-off for a predictor of FSH effectiveness, receiver operating characteristic (ROC) curves were generated.
Statistical analysis was performed using the “Statistical Package for the Social Sciences” software for Windows (version 27.0; SPSS Inc., Chicago, IL, USA). For all comparisons, p < 0.05 was considered statistically significant.
4. Discussion
This re-analysis of published clinical trials data investigating FSH administration in male idiopathic infertility highlights a novel aspect of male infertility management. Alongside the expected amelioration of conventional semen quality and an overall 20% decrease of sDF baseline index, exogenous FSH stimulation induces an increase in testosterone, inhibin B and AMH serum levels. Both inhibin B and AMH are Sertoli cell products, reflecting the proliferative status of the testicular germinative epithelium [
25,
26]. Thus, their increase after FSH administration is not unexpected. On the contrary, the testosterone rise after FSH administration is unexpected and detected here for the first time, suggesting an action of FSH on testicular function more complex than thought so far. Indeed, we could speculate that FSH boosts spermatogenesis throughout a direct action on Sertoli cells and also an indirect effect involving the testis interstitial compartment. This finding is in line with previous demonstrations of the capability of the supraphysiological FSH stimulation to sustain spermatogenesis even in the absence of LH action [
27]. Indeed, a quali-quantitative normal spermatogenesis was reported in a hypophysectomised man presenting an activating FSH receptor mutation, suggesting that a strong FSH action alone could support the LH/testosterone function [
27].
Our new analysis showed for the first time the global testicular action (not limited to the spermatogenic compartment) of FSH chronically administered to infertile men. As confirmed, after three months of FSH administration, sperm quality (in terms of sDF index) correlated with testosterone serum levels, highlighting the association between the FSH-related sDF improvement and the increase in testosterone serum levels. Accordingly, both multivariate linear and logistic regression analyses identified a strong correlation between testosterone increase and sDF decrease after FSH treatment. This finding is totally novel since the literature on this topic is entirely silent. This innovative result could open new perspectives in the way of evaluating responses to FSH treatment in male idiopathic infertility. This new correlation, although interesting, is far from being directly transposed to clinical practice. Specific, properly designed prospective trials must be designed to understand the real clinical application of the finding. From a physiological point of view, the strict connection between seminiferous and interstitial testicular compounds is expected, since effective spermatogenesis requires both FSH action and adequate intratesticular testosterone levels [
28]. However, this link has been generally underestimated in clinical practice, since intratesticular testosterone assessment is very complex, requiring testicular biopsy or sampling [
29]. In addition, testosterone measured in the peripheral blood correlates poorly to its intratesticular levels, which are estimated to be at least 100 times higher [
30]. For these reasons, several attempts have been made to identify surrogate markers of intratesticular testosterone levels [
29]. Among these, serum 17-hydroxyprogesterone (17-OHP) and Insulin-like factor 3 (INSL3) have been proposed [
30,
31]. These hormones were demonstrated as able to predict intratesticular testosterone levels after human chorionic gonadotropin (hCG) stimulation [
32,
33]. However, both 17-OHP and INSL3 did not correlate with testosterone intratesticular levels at baseline, only after hCG treatment. This result mirrors the sDF–testosterone correlation detected only after FSH administration in this study. Thus, the connection of sDF–testosterone is novel in the field of human reproduction, although some suggestion of such a correlation is provided in other fields. For example, Wood et al. described improvements in both testosterone serum levels and sDF index six months after bariatric surgery [
34]. In our analysis, we speculate that both testicular compartments, seminiferous and interstitial, tend to realign only after overstimulation induced by exogenous gonadotropins. However, as neither intratesticular testosterone levels nor their surrogate markers are available in our analysis, we cannot provide conclusive explanations of the FSH action at intratesticular level.
Putting together three different cohorts of patients treated with the same regimen of recombinant FSH for three months, we highlight an overall 20% decrease of sDF baseline index with the current therapeutic approach. In particular, we detect a FSH efficacy rate of about 59.2%, considering the sDF index decrease. This relevant result could be directly translated into clinical practice. Hitherto, many direct tests have been suggested to predict sperm capability to penetrate the oocyte, such as sperm–zona binding ratios and zona pellucida-induced acrosome reaction tests [
35,
36]. Similarly, indirect variables could be measured in seminal plasma with the same objective, such as phospholipase, sperm acrosin, fructose and neural alfa-glucosidase [
37,
38,
39]. In this setting, the sDF index provides an informative and reliable measure of the real fertilization capability [
40,
41,
42,
43]. SDF is the end result of the action of multiple factors that induce single- or double-strand DNA breaks in the sperm genome [
44], due to oxidative stress [
45], apoptosis [
46,
47], impaired chromatin remodelling [
48] and environmental agents, such as toxicants, drugs and radiation [
49,
50,
51]. As a result, high levels of sDF index reflect an impaired semen quality [
17] and a reduced fertility [
16]. Sperm DNA integrity is crucial for embryo development and successful pregnancy outcome, and sDF values are inversely related to the chances of achieving natural pregnancy [
52,
53]. Accordingly, increased sDF index was comprehensively detected in infertile compared with fertile men in a recent meta-analysis, which proposed an sDF threshold of 20% to discriminate between fertile and infertile men (AUC: 0.84,
p < 0.001, sensitivity 79%, specificity 86%) [
16]. The proven relevance of sDF assessment in human fertility justified the insertion of its measurement within the latest edition of the World Health Organization (WHO) laboratory manual for the examination and processing of human semen [
54]. In the current re-analysis, sDF index significantly decreased after FSH treatment concomitantly with the increase in conventional semen parameters, demonstrating an overall FSH-induced improvement in sperm quality, which could be measured through this relatively new tool. However, the correlation between sDF and conventional semen parameters is still controversial [
55,
56,
57]. Here, sDF is correlated to sperm progressive motility after FSH administration, in line with previous studies depicting the highest sDF index in men presenting the lowest percentage of motile sperms [
58,
59]. A connection between sDF and sperm motility could be hypothesized since these two parameters share a marked detrimental susceptibility to reactive oxygen species (ROS). Indeed, oxidative stress is assumed to be the most relevant causative factor contributing to sDF [
17], while sperm motility is acquired during the long sperm transit through the epididymis, resulting more likely vulnerable to ROS damage [
47].
Subgrouping our cohort in responders and non-responders to FSH treatment considering an sDF decrease threshold of 20% of its basal level could be useful to identify markers and predictors of FSH efficacy. With this approach, only two markers of FSH efficacy are identified, testosterone serum levels and male age, although ROC analyses were not able to identify useful thresholds for clinical practice. On the contrary, sDF amelioration after FSH therapy is predicted only by sDF basal levels, with a significant threshold of 16.75%. Since no differences between responders and non-responders were demonstrated by conventional semen parameters, we could speculate that semen analysis is not really accurate to evaluate male fertility status.
Our results should be carefully considered due to several limitations. First, we combined raw data of three clinical studies, putting together a large cohort of patients for this research topic, yet still limited to elaborate definitive conclusions. Second, a relatively high heterogeneity among trials should be expected. Although all three trials used recombinant FSH at the same dosage (150 IU every other day) for the same treatment period (three months), inclusion criteria of each trial may have differed. Indeed, Simoni et al. enrolled only men with sDF >15% at baseline, while Colacurci et al. did not consider sDF index as an inclusion criterion. Thus, enrolled populations were not completely homogeneous. In addition, in all studies, testosterone serum levels were measured by immunometric assays and not by liquid chromatography-mass spectrometry, which is the gold standard for steroid measurement [
60].

 ,
, 



{kind=link}