
Combinations of Cannabidiol and Δ9-Tetrahydrocannabinol in Reducing Chemotherapeutic Induced Neuropathic Pain


Abstract
1. Introduction
2. Materials and Methods
2.1. Animals
2.2. Drugs
2.3. Supercritical CO2 Extraction
2.4. Cisplatin-Induced Neuropathy
2.5. Von Frey Testing
2.6. Statistical Analysis
3. Results
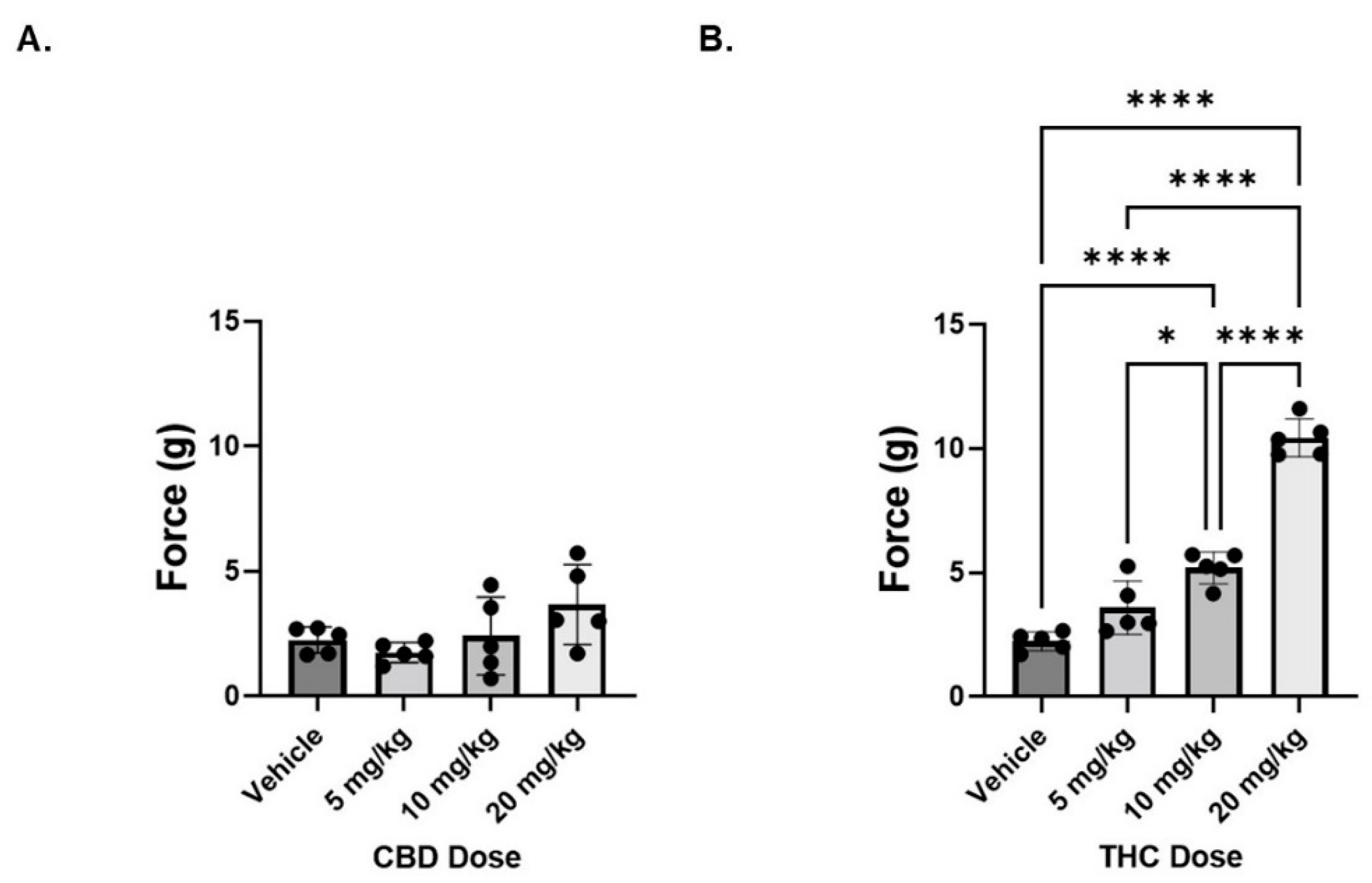
3.1. THC, but Not CBD, Reverses Mechanical Hypersensitivity in Neuropathic Male Mice
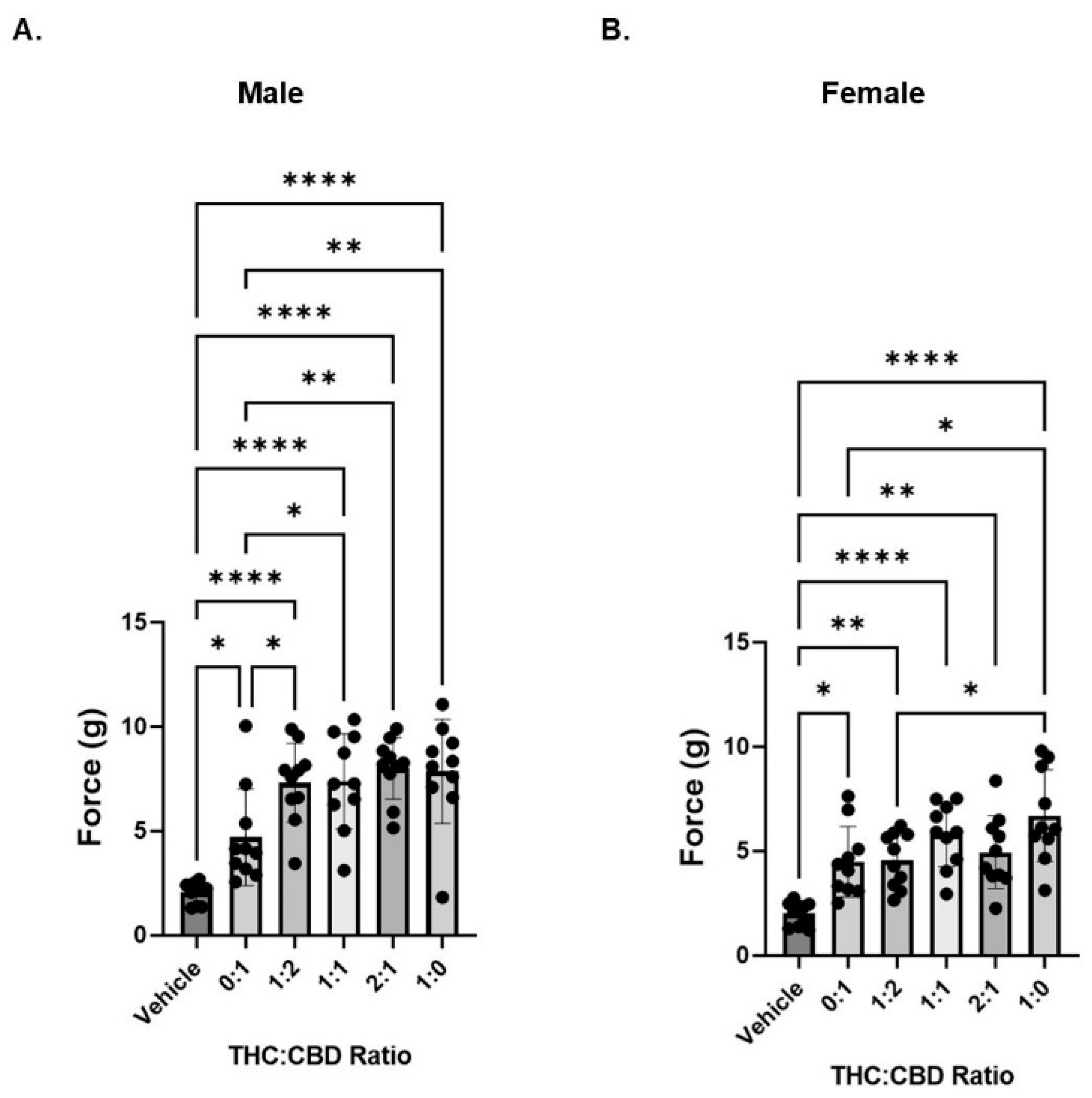
3.2. CBD Does Influence THC-Induced Decreases in Mechanical Hypersensitivity
3.3. CBD and THC Extracts Are Effective at Attenuating Mechanical Hypersensitivity in Neuropathic Mice
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lee, G.; Grovey, B.; Furnish, T.; Wallace, M. Medical cannabis for neuropathic pain. Curr. Pain Headache Rep. 2018, 22, 8. [Google Scholar] [CrossRef]
- Mitchell, V.A.; Harley, J.; Casey, S.L.; Vaughan, A.C.; Winters, B.L.; Vaughan, C.W. Oral efficacy of Δ(9)-tetrahydrocannabinol and cannabidiol in a mouse neuropathic pain model. Neuropharmacology 2021, 189, 108529. [Google Scholar] [CrossRef]
- Jensen, T.S.; Baron, R.; Haanpää, M.; Kalso, E.; Loeser, J.D.; Rice, A.S.; Treede, R.D. A new definition of neuropathic pain. Pain 2011, 152, 2204–2205. [Google Scholar] [CrossRef]
- Finnerup, N.B.; Attal, N.; Haroutounian, S.; McNicol, E.; Baron, R.; Dworkin, R.H.; Gilron, I.; Haanpää, M.; Hansson, P.; Jensen, T.S.; et al. Pharmacotherapy for neuropathic pain in adults: A systematic review and meta-analysis. Lancet Neurol. 2015, 14, 162–173. [Google Scholar] [CrossRef]
- Nicholson, B.; Verma, S. Comorbidities in chronic neuropathic pain. Pain Med. 2004, 5 (Suppl. S1), S9–S27. [Google Scholar] [CrossRef]
- van Hecke, O.A.S.K.R.; Austin, S.K.; Khan, R.A.; Smith, B.H.; Torrance, N. Neuropathic pain in the general population: A systematic review of epidemiological studies. Pain 2014, 155, 654–662. [Google Scholar] [CrossRef]
- Russo, E.B. Cannabinoids in the management of difficult to treat pain. Ther. Clin. Risk Manag. 2008, ume 4, 245–259. [Google Scholar] [CrossRef]
- Legare, C.A.; Raup-Konsavage, W.M.; Vrana, K.E. Therapeutic potential of cannabis, cannabidiol, and cannabinoid-based pharmaceuticals. Pharmacology 2022, 107, 131–149. [Google Scholar] [CrossRef] [PubMed]
- Ward, S.J.; Ramirez, M.D.; Neelakantan, H.; Walker, E.A. Cannabidiol prevents the development of cold and mechanical allodynia in paclitaxel-treated female C57Bl6 mice. Anesthesia Analg. 2011, 113, 947–950. [Google Scholar] [CrossRef]
- Ward, S.J.; McAllister, S.D.; Kawamura, R.; Murase, R.; Neelakantan, H.; Walker, E.A. Cannabidiol inhibits paclitaxel-induced neuropathic pain through 5-HT(1A) receptors without diminishing nervous system function or chemotherapy efficacy. Br. J. Pharmacol. 2014, 171, 636–645. [Google Scholar] [CrossRef] [PubMed]
- Casey, S.L.; Atwal, N.; Vaughan, C.W. Cannabis constituent synergy in a mouse neuropathic pain model. Pain 2017, 158, 2452–2460. [Google Scholar] [CrossRef]
- King, K.M.; Myers, A.M.; Soroka-Monzo, A.J.; Tuma, R.F.; Tallarida, R.J.; Walker, E.A.; Ward, S.J. Single and combined effects of Δ9 -tetrahydrocannabinol and cannabidiol in a mouse model of chemotherapy-induced neuropathic pain. J. Cereb. Blood Flow Metab. 2017, 174, 2832–2841. [Google Scholar] [CrossRef]
- Henderson-Redmond, A.N.; Crawford, L.C.; Sepulveda, D.E.; Hale, D.E.; Lesperance, J.J.; Morgan, D.J. Sex differences in tolerance to delta-9-tetrahydrocannabinol in mice with cisplatin-evoked chronic neuropathic pain. Front. Mol. Biosci. 2021, 8, 684115. [Google Scholar] [CrossRef]
- Überall, M.A. A review of scientific evidence for THC:CBD oromucosal spray (nabiximols) in the management of chronic pain. J. Pain Res. 2020, 13, 399–410. [Google Scholar] [CrossRef]
- Dykukha, I.; Malessa, R.; Essner, U.; Überall, M.A. Nabiximols in chronic neuropathic pain: A meta-analysis of randomized placebo-controlled trials. Pain Med. 2021, 22, 861–874. [Google Scholar] [CrossRef]
- Sainsbury, B.; Bloxham, J.; Pour, M.H.; Padilla, M.; Enciso, R. Efficacy of cannabis-based medications compared to placebo for the treatment of chronic neuropathic pain: A systematic review with meta-analysis. J. Dent. Anesthesia Pain Med. 2021, 21, 479–506. [Google Scholar] [CrossRef]
- Ueberall, M.A.; Silván, C.V.; Essner, U.; Mueller-Schwefe, G.H.H. Effectiveness, Safety, and Tolerability of Nabiximols Oromucosal Spray vs Typical Oral Long-Acting Opioid Analgesics in Patients with Severe Neuropathic Back Pain: Analysis of 6-Month Real-World Data from the German Pain e-Registry. Pain Med. 2022, 23, 745–760. [Google Scholar] [CrossRef]
- Guindon, J.; Deng, L.; Fan, B.; Wager-Miller, J.; Hohmann, A.G. Optimization of a cisplatin model of chemotherapy-induced peripheral neuropathy in mice: Use of vitamin C and sodium bicarbonate pretreatments to reduce nephrotoxicity and improve animal health status. Mol. Pain 2014, 10, 56. [Google Scholar] [CrossRef]
- Foss, J.D.; Farkas, D.J.; Huynh, L.M.; Kinney, W.A.; Brenneman, D.E.; Ward, S.J. Behavioural and pharmacological effects of cannabidiol (CBD) and the cannabidiol analogue KLS-13019 in mouse models of pain and reinforcement. J. Cereb. Blood Flow Metab. 2021, 178, 3067–3078. [Google Scholar] [CrossRef]
- Somani, S.J.; Modi, K.P.; Majumdar, A.S.; Sadarani, B.N. Phytochemicals and their potential usefulness in inflammatory bowel disease. Phytother. Res. 2015, 29, 339–350. [Google Scholar] [CrossRef]
- Nuutinen, T. Medicinal properties of terpenes found in Cannabis sativa and Humulus lupulus. Eur. J. Med. Chem. 2018, 157, 198–228. [Google Scholar] [CrossRef]
- McDonagh, M.S.; Morasco, B.J.; Wagner, J.; Ahmed, A.Y.; Fu, R.; Kansagara, D.; Chou, R. Cannabis-based products for chronic pain: A systematic review. Ann. Intern. Med. 2022, 175, 1143–1153. [Google Scholar] [CrossRef]
- Russo, E.; Guy, G.W. A tale of two cannabinoids: The therapeutic rationale for combining tetrahydrocannabinol and cannabidiol. Med. Hypotheses 2006, 66, 234–246. [Google Scholar] [CrossRef]
- Russo, E.B. Taming THC: Potential cannabis synergy and phytocannabinoid-terpenoid entourage effects. Br. J. Pharmacol. 2011, 163, 1344–1364. [Google Scholar] [CrossRef]
- Freeman, A.M.; Petrilli, K.; Lees, R.; Hindocha, C.; Mokrysz, C.; Curran, H.V.; Saunders, R.; Freeman, T.P. How does cannabidiol (CBD) influence the acute effects of delta-9-tetrahydrocannabinol (THC) in humans? A systematic review. Neurosci. Biobehav. Rev. 2019, 107, 696–712. [Google Scholar] [CrossRef]
- Russo, E.B. The case for the entourage effect and conventional breeding of clinical cannabis: No “strain,” no gain. Front. Plant Sci. 2018, 9, 1969. [Google Scholar] [CrossRef] [PubMed]
- Arkell, T.R.; Lintzeris, N.; Kevin, R.C.; Ramaekers, J.G.; Vandrey, R.; Irwin, C.; Haber, P.S.; McGregor, I.S. Cannabidiol (CBD) content in vaporized cannabis does not prevent tetrahydrocannabinol (THC)-induced impairment of driving and cognition. Psychopharmacology 2019, 236, 2713–2724. [Google Scholar] [CrossRef] [PubMed]
- Vučković, S.; Srebro, D.; Vujović, K.S.; Vučetić, Č.; Prostran, M. Cannabinoids and pain: New insights from old molecules. Front. Pharmacol. 2018, 9, 1259. [Google Scholar] [CrossRef]
- Louis-Gray, K.; Tupal, S.; Premkumar, L.S. TRPV1: A common denominator mediating antinociceptive and antiemetic effects of cannabinoids. Int. J. Mol. Sci. 2022, 23, 10016. [Google Scholar] [CrossRef]
- Casey, S.L.; Mitchell, V.A.; Sokolaj, E.E.; Winters, B.L.; Vaughan, C.W. Intrathecal actions of the cannabis constituents Δ(9)-tetrahydrocannabinol and cannabidiol in a mouse neuropathic pain model. Int. J. Mol. Sci. 2022, 23, 8649. [Google Scholar] [CrossRef] [PubMed]
- Sepulveda, D.E.; Morris, D.P.; Raup-Konsavage, W.M.; Sun, D.; Vrana, K.E.; Graziane, N.M. Cannabigerol (CBG) attenuates mechanical hypersensitivity elicited by chemotherapy-induced peripheral neuropathy. Eur. J. Pain 2022, 26, 1950–1966. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Ratio | THC (mg/kg) | CBD (mg/kg) |
|---|---|---|
| 0:1 | 0 | 6 |
| 1:2 | 2 | 4 |
| 1:1 | 3 | 3 |
| 2:1 | 4 | 2 |
| 1:0 | 6 | 0 |
| Cannabinoid | CBD Extract | THC Extract |
|---|---|---|
| CBC | 0.03 | |
| CBD | 1.8 | 0.005 |
| CBDA | 0.003 | |
| CBDV | 0.03 | |
| CBG | 0.067 | |
| CBGA | 0.002 | |
| CBN | 0.048 | |
| THCA | 0.002 | |
| Δ9-THC | 0.04 | 1.8 |
| Total Cannabinoid | 1.87 | 1.957 |
| Terpene | CBD Extract | THC Extract |
|---|---|---|
| β-Farnesene | 3.13 | |
| β-Caryophyllene | 191.72 | 20.97 |
| α-Humulene | 55.67 | 4.11 |
| (−) α-Bisabolol | 3.61 | 2.06 |
| β-Myrcene | 0.16 | 2.51 |
| R(+) Limonene | 0.17 | 1.33 |
| Endo-Fenchyl Alcohol | 4.33 | 1.14 |
| Guaiol | 1.4 | |
| α-Pinene | 0.01 | 3.58 |
| Linalool | 2.87 | 1.54 |
| (−) Caryophyllene Oxide | 37.91 | |
| Trans-Nerolidol | 3.91 | 0.61 |
| Valencene | 8.2 | |
| β-Pinene | 1.74 | |
| Total Terpene | 301.63 | 55.27 |
| Total Terpene (mg/mL) | 0.30 | 0.06 |
| Ratio | THC (mg/kg) | CBD (mg/kg) |
|---|---|---|
| 0:1 | 0.13 | 6 |
| 1:2 | 2.09 | 4.01 |
| 1:1 | 3.07 | 3.01 |
| 2:1 | 4.04 | 2.01 |
| 1:0 | 6 | 0.02 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sepulveda, D.E.; Vrana, K.E.; Graziane, N.M.; Raup-Konsavage, W.M. Combinations of Cannabidiol and Δ9-Tetrahydrocannabinol in Reducing Chemotherapeutic Induced Neuropathic Pain. Biomedicines 2022, 10, 2548. https://doi.org/10.3390/biomedicines10102548
Sepulveda DE, Vrana KE, Graziane NM, Raup-Konsavage WM. Combinations of Cannabidiol and Δ9-Tetrahydrocannabinol in Reducing Chemotherapeutic Induced Neuropathic Pain. Biomedicines. 2022; 10(10):2548. https://doi.org/10.3390/biomedicines10102548
Chicago/Turabian StyleSepulveda, Diana E., Kent E. Vrana, Nicholas M. Graziane, and Wesley M. Raup-Konsavage. 2022. "Combinations of Cannabidiol and Δ9-Tetrahydrocannabinol in Reducing Chemotherapeutic Induced Neuropathic Pain" Biomedicines 10, no. 10: 2548. https://doi.org/10.3390/biomedicines10102548
APA StyleSepulveda, D. E., Vrana, K. E., Graziane, N. M., & Raup-Konsavage, W. M. (2022). Combinations of Cannabidiol and Δ9-Tetrahydrocannabinol in Reducing Chemotherapeutic Induced Neuropathic Pain. Biomedicines, 10(10), 2548. https://doi.org/10.3390/biomedicines10102548