
Diabetes Mellitus Mediates Risk of Depression in Danish Women with Polycystic Ovary Syndrome—A National Cohort Study
 , ,
, ,
Abstract
:1. Introduction
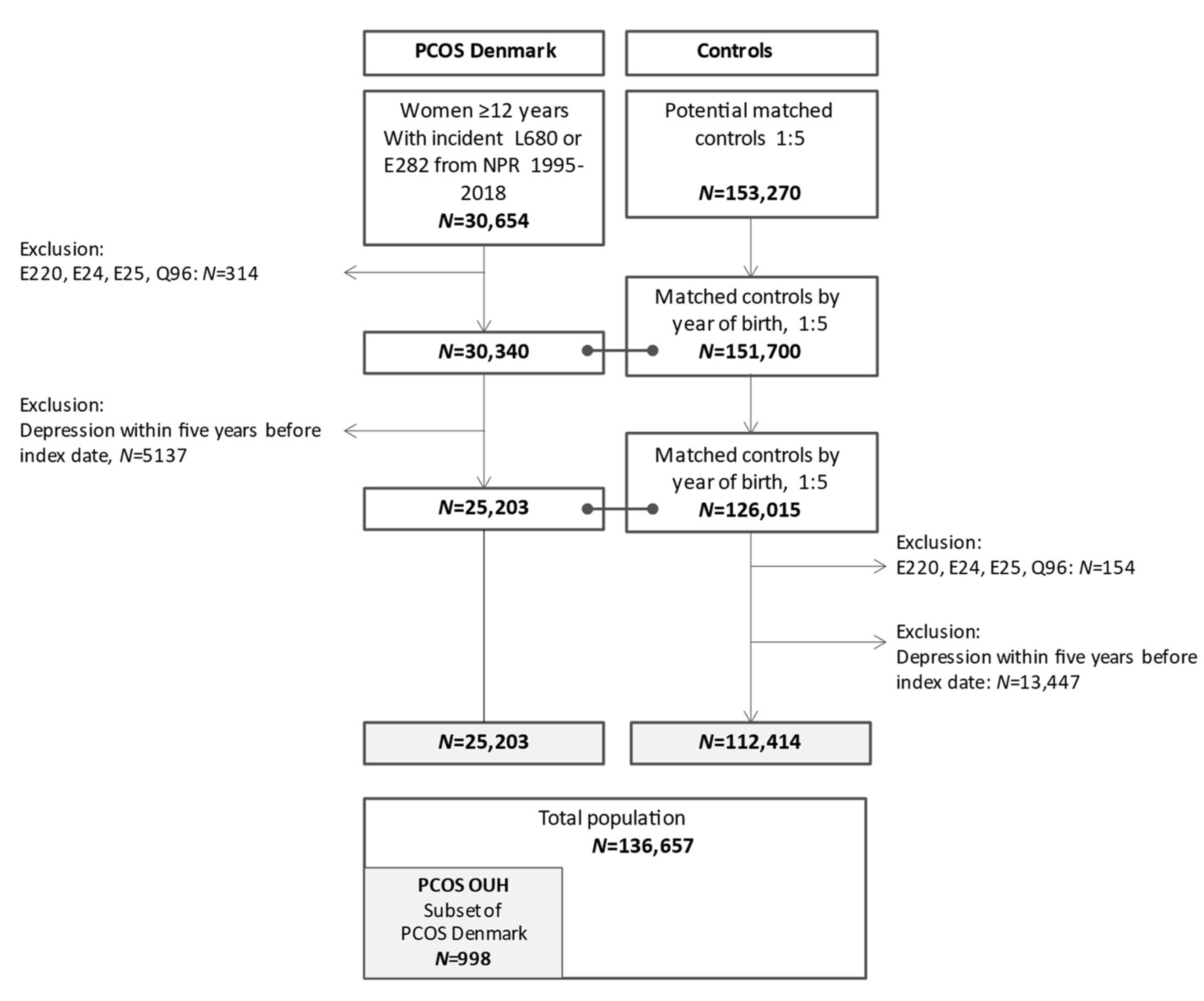
2. Material and Methods
2.1. Definition of Study Parameters
2.1.1. Outcome
2.1.2. Covariates
2.2. PCOS OUH
2.3. Statistical Analyses
2.4. Ethics
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Conway, G.; Dewailly, D.; Diamanti-Kandarakis, E.; Escobar-Morreale, H.; Franks, S.; Gambineri, A.; Kelestimur, F.; Macut, D.; Micic, D.; Pasquali, R.; et al. The polycystic ovary syndrome: A position statement from the European Society of Endocrinology. Eur. J. Endocrinol. 2014, 171, P1–P29. [Google Scholar] [CrossRef] [PubMed]
- Eshre, T.R.; ASRM-Sponsored PCOS Consensus Workshop Group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Fertil. Steril. 2004, 81, 19–25. [Google Scholar]
- Yin, X.; Ji, Y.; Chan, C.L.W.; Chan, C.H.Y. The mental health of women with polycystic ovary syndrome: A systematic review and meta-analysis. Arch Womens Ment Health 2021, 24, 11–27. [Google Scholar] [CrossRef]
- Castelo-Branco, C.; Naumova, I. Quality of life and sexual function in women with polycystic ovary syndrome: A comprehensive review. Gynecol. Endocrinol. 2019, 36, 96–103. [Google Scholar] [CrossRef] [PubMed]
- Dokras, A.; Stener-Victorin, E.; Yildiz, B.O.; Li, R.; Ottey, S.; Shah, D.; Epperson, N.; Teede, H. Androgen Excess- Polycystic Ovary Syndrome Society: Position statement on depression, anxiety, quality of life, and eating disorders in polycystic ovary syndrome. Fertil. Steril. 2018, 109, 888–899. [Google Scholar] [CrossRef]
- Jones, G.; Hall, J.; Balen, A.; Ledger, W. Health-related quality of life measurement in women with polycystic ovary syndrome: A systematic review. Hum. Reprod. Updat. 2007, 14, 15–25. [Google Scholar] [CrossRef]
- Hahn, S.; Janssen, O.E.; Tan, S.; Pleger, K.; Mann, K.; Schedlowski, M.; Kimmig, R.; Benson, S.; Balamitsa, E.; Elsenbruch, S. Clinical and psychological correlates of quality-of-life in polycystic ovary syndrome. Eur. J. Endocrinol. 2005, 153, 853–860. [Google Scholar] [CrossRef] [PubMed]
- Cooney, L.G.; Lee, I.; Sammel, M.D.; Dokras, A. High prevalence of moderate and severe depressive and anxiety symptoms in polycystic ovary syndrome: A systematic review and meta-analysis. Hum. Reprod. 2017, 32, 1075–1091. [Google Scholar] [CrossRef]
- Glintborg, D.; Rubin, K.H.; Nybo, M.; Abrahamsen, B.; Andersen, M. Morbidity and medicine prescriptions in a nationwide Danish population of patients diagnosed with polycystic ovary syndrome. Eur. J. Endocrinol. 2015, 172, 627–638. [Google Scholar] [CrossRef] [PubMed]
- Cesta, C.E.; Månsson, M.; Palm, C.; Lichtenstein, P.; Iliadou, A.N.; Landén, M. Polycystic ovary syndrome and psychiatric disorders: Co-morbidity and heritability in a nationwide Swedish cohort. Psychoneuroendocrinology 2016, 73, 196–203. [Google Scholar] [CrossRef] [PubMed]
- Altinok, M.L.; Glintborg, D.; Christensen, R.D.; Hallas, J.; Andersen, M. Prescription of antidepressants is increased in Danish patients with polycystic ovary syndrome and is associated with hyperandrogenism. A population-based cohort study. Clin. Endocrinol. 2013, 80, 884–889. [Google Scholar] [CrossRef] [PubMed]
- Lee, I.O.; Kim, J.C.; Seo, J.W.; Pak, H.Y.; Chung, J.E. Risk of developing major depressive disorder in polycystic ovary syndrome: A retrospective cohort study. J. Obstet. Gynaecol. 2021, 41, 1157–1161. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, J.; Wang, X.; Xu, L.; Wu, T.; Kang, D. Antidepressants for polycystic ovary syndrome. Cochrane Database Syst. Rev. 2013, 5, CD008575. [Google Scholar] [CrossRef]
- Glintborg, D.; Andersen, M. An update on the pathogenesis, inflammation, and metabolism in hirsutism and polycystic ovary syndrome. Gynecol. Endocrinol. 2010, 26, 281–296. [Google Scholar] [CrossRef] [PubMed]
- Dokras, A.; Clifton, S.; Futterweit, W.; Wild, R. Increased Risk for Abnormal Depression Scores in Women With Polycystic Ovary Syndrome: A Systematic Review and Meta-Analysis. Obstet. Gynecol. Surv. 2011, 66, 284–285. [Google Scholar] [CrossRef]
- Glintborg, D.; Andersen, M. MANAGEMENT OF ENDOCRINE DISEASE: Morbidity in polycystic ovary syndrome. Eur. J. Endocrinol. 2017, 176, R53–R65. [Google Scholar] [CrossRef]
- Rubin, K.H.; Glintborg, D.; Nybo, M.; Abrahamsen, B.; Andersen, M. Development and Risk Factors of Type 2 Diabetes in a Nationwide Population of Women With Polycystic Ovary Syndrome. J. Clin. Endocrinol. Metab. 2017, 102, 3848–3857. [Google Scholar] [CrossRef] [PubMed]
- Beran, M.; Muzambi, R.; Geraets, A.; Albertorio-Diaz, J.R.; Adriaanse, M.C.; Iversen, M.M.; Kokoszka, A.; Nefs, G.; Nouwen, A.; Pouwer, F.; et al. The bidirectional longitudinal association between depressive symptoms and HbA1c: A systematic review and meta-analysis. Diabet. Med. 2021, 39, e14671. [Google Scholar] [CrossRef] [PubMed]
- Kiani, Z.; Simbar, M.; Hajian, S.; Zayeri, F. The prevalence of depression symptoms among infertile women: A systematic review and meta-analysis. Fertil. Res. Pr. 2021, 7, 1–10. [Google Scholar] [CrossRef]
- Teede, H.; Tassone, E.C.; Piltonen, T.; Malhotra, J.; Mol, B.W.; Peña, A.; Witchel, S.F.; Joham, A.; McAllister, V.; Romualdi, D.; et al. Effect of the combined oral contraceptive pill and/or metformin in the management of polycystic ovary syndrome: A systematic review with meta-analyses. Clin. Endocrinol. 2019, 91, 479–489. [Google Scholar] [CrossRef] [PubMed]
- Skovlund, C.W.; Mørch, L.S.; Kessing, L.V.; Lidegaard, Ø. Association of Hormonal Contraception With Depression. JAMA Psychiatry 2016, 73, 1154–1162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmidt, M.; Schmidt, S.A.J.; Sandegaard, J.L.; Ehrenstein, V.; Pedersen, L.; Sørensen, H.T. The Danish National Patient Registry: A review of content, data quality, and research potential. Clin. Epidemiol. 2015, 7, 449–490. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.; Pedersen, L.; Sørensen, H.T. The Danish Civil Registration System as a tool in epidemiology. Eur. J. Epidemiol. 2014, 29, 541–549. [Google Scholar] [CrossRef] [PubMed]
- Pottegård, A.; Schmidt, S.A.J.; Wallach-Kildemoes, H.; Sørensen, H.T.; Hallas, J.; Schmidt, M. Data Resource Profile: The Danish National Prescription Registry. Int. J. Epidemiol. 2016, 46, 798–798f. [Google Scholar] [CrossRef] [PubMed]
- Baadsgaard, M.; Quitzau, J. Danish registers on personal income and transfer payments. Scand. J. Public Heal. 2011, 39 (Suppl. 7), 103–105. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.; Schmidt, S.A.J.; Adelborg, K.; Sundbøll, J.; Laugesen, K.; Ehrenstein, V.; Sørensen, H.T. The Danish health care system and epidemiological research: From health care contacts to database records. Clin. Epidemiology 2019, 11, 563–591. [Google Scholar] [CrossRef]
- Rubin, K.H.; Glintborg, D.; Nybo, M.; Andersen, M.; Abrahamsen, B. Fracture Risk Is Decreased in Women With Polycystic Ovary Syndrome: A Register-Based and Population-Based Cohort Study. J. Bone Miner. Res. 2015, 31, 709–717. [Google Scholar] [CrossRef]
- Glintborg, D.; Rubin, K.H.; Nybo, M.; Abrahamsen, B.; Andersen, M. Cardiovascular disease in a nationwide population of Danish women with polycystic ovary syndrome. Cardiovasc. Diabetol. 2018, 17, 37. [Google Scholar] [CrossRef]
- Nader, S. Hyperandrogenism during puberty in the development of polycystic ovary syndrome. Fertil. Steril. 2013, 100, 39–42. [Google Scholar] [CrossRef]
- Forman, M.R.; Mangini, L.D.; Thelus-Jean, R.; Hayward, M.D. Life-course origins of the ages at menarche and menopause. Adolesc. Heal. Med. Ther. 2013, 4, 1–21. [Google Scholar] [CrossRef]
- Rubin, K.H.; Andersen, M.S.; Abrahamsen, B.; Glintborg, D. Socioeconomic status in Danish women with polycystic ovary syndrome: A register-based cohort study. Acta Obstet. Gynecol. Scand. 2018, 98, 440–450. [Google Scholar] [CrossRef] [PubMed]
- Linder, A.; Gerdtham, U.-G.; Trygg, N.; Fritzell, S.; Saha, S. Inequalities in the economic consequences of depression and anxiety in Europe: A systematic scoping review. Eur. J. Public Health 2019, 30, 767–777. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Quan, H.; Sundararajan, V.; Halfon, P.; Fong, A.; Burnand, B.; Luthi, J.-C.; Saunders, L.D.; Beck, C.A.; Feasby, T.E.; Ghali, W.A. Coding Algorithms for Defining Comorbidities in ICD-9-CM and ICD-10 Administrative Data. Med. Care 2005, 43, 1130–1139. [Google Scholar] [CrossRef]
- Quan, H.; Li, B.; Couris, C.M.; Fushimi, K.; Graham, P.; Hider, P.; Januel, J.-M.; Sundararajan, V. Updating and Validating the Charlson Comorbidity Index and Score for Risk Adjustment in Hospital Discharge Abstracts Using Data From 6 Countries. Am. J. Epidemiol. 2011, 173, 676–682. [Google Scholar] [CrossRef]
- Nielsen, T.L.; Hagen, C.; Wraae, K.; Brixen, K.; Petersen, P.H.; Haug, E.; Larsen, R.; Andersen, M. Visceral and Subcutaneous Adipose Tissue Assessed by Magnetic Resonance Imaging in Relation to Circulating Androgens, Sex Hormone-Binding Globulin, and Luteinizing Hormone in Young Men. J. Clin. Endocrinol. Metab. 2007, 92, 2696–2705. [Google Scholar] [CrossRef]
- VanderWeele, T.J. A unification of mediation and interaction: A 4-way decomposition. Epidemiology 2014, 25, 749–761. [Google Scholar] [CrossRef]
- Hung, J.-H.; Hu, L.-Y.; Tsai, S.-J.; Yang, A.C.; Huang, M.-W.; Chen, P.-M.; Wang, S.-L.; Lu, T.; Shen, C.-C. Risk of Psychiatric Disorders following Polycystic Ovary Syndrome: A Nationwide Population-Based Cohort Study. PLoS ONE 2014, 9, e97041. [Google Scholar] [CrossRef]
- Cinar, N.; Kizilarslanoglu, M.C.; Harmanci, A.; Aksoy, D.Y.; Bozdag, G.; Demir, B.; Yıldız, B.O. Depression, anxiety and cardiometabolic risk in polycystic ovary syndrome. Hum. Reprod. 2011, 26, 3339–3345. [Google Scholar] [CrossRef]
- Park, L.T.; Zarate, C.A., Jr. Depression in the Primary Care Setting. N. Engl. J. Med. 2019, 380, 559–568. [Google Scholar] [CrossRef]
- Habib, S.; Sangaraju, S.L.; Yepez, D.; Grandes, X.A.; Manjunatha, R.T. The Nexus Between Diabetes and Depression: A Narrative Review. Cureus 2022, 14, e25611. [Google Scholar] [CrossRef] [PubMed]
- Kolhe, J.V.; Chhipa, A.S.; Butani, S.; Chavda, V.; Patel, S.S. PCOS and Depression: Common Links and Potential Targets. Reprod. Sci. 2021, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Cinar, N.; Harmanci, A.; Demir, B.; Yildiz, B.O. Effect of an oral contraceptive on emotional distress, anxiety and depression of women with polycystic ovary syndrome: A prospective study. Hum. Reprod. 2012, 27, 1840–1845. [Google Scholar] [CrossRef] [PubMed]
- Altinok, M.L.; Ravn, P.; Andersen, M.; Glintborg, D. Effect of 12-month treatment with metformin and/or oral contraceptives on health-related quality of life in polycystic ovary syndrome. Gynecol. Endocrinol. 2018, 34, 859–863. [Google Scholar] [CrossRef] [PubMed]
- Dokras, A.; Sarwer, D.B.; Allison, K.C.; Milman, L.; Kris-Etherton, P.; Kunselman, A.R.; Stetter, C.M.; Williams, N.I.; Gnatuk, C.L.; Estes, S.J.; et al. Weight Loss and Lowering Androgens Predict Improvements in Health-Related Quality of Life in Women With PCOS. J. Clin. Endocrinol. Metab. 2016, 101, 2966–2974. [Google Scholar] [CrossRef]
- Glintborg, D.; Sidelmann, J.J.; Altinok, M.L.; Mumm, H.; Andersen, M. Increased thrombin generation in women with polycystic ovary syndrome: A pilot study on the effect of metformin and oral contraceptives. Metabolism 2015, 64, 1272–1278. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| PCOS OUH | PCOS Denmark | Controls | ||||
|---|---|---|---|---|---|---|
| (N = 998) | (N = 25,203) | (N = 112,414) | p a | p b | ||
| Age (y) at diagnosis PCOS median (Q1–Q3) | 28(21; 34) | 28 (23; 35) | 28 (22; 35) | |||
| ICD-10 codes | ||||||
| Diabetes mellitus | E10,11,13,14, O24 | 132 (13.2%) | 2642 (10.5%) | 3910 (3.5%) | 0.004 | 0.000 |
| Comorbidity at index | 26 (2.6%) | 979 (3.9%) | 2944 (2.6%) | 0.033 | 0.000 | |
| Infertility | N97, Z35 | 494 (49.5%) | 10,443 (41.4%) | 26,352 (23.4%) | 0.000 | 0.000 |
| Number of births | 0 | 531 (53.2%) | 12,680 (50.3%) | 55,660 (49.5%) | 0.062 | 0.022 |
| 1 | 171 (17.1%) | 4497 (17.8%) | 16,850 (15.0%) | 0.551 | 0.000 | |
| ≥2 | 296 (29.7%) | 8026 (31.8%) | 39,904 (35.5%) | 0.130 | 0.000 | |
| Medicine prescriptions | ||||||
| Antidiabetics | A10 | 78 (7.8%) | 1552 (6.2%) | 1996 (1.8%) | 0.026 | 0.000 |
| Fertility treatment | G03GA, G03GB | 259 (26.0%) | 7885 (31.3%) | 9736 (8.7%) | 0.000 | 0.000 |
| Hormonal anticonception | G03AA, G03AB G03HB01, G03AC G02BA03 | 848 (85.0%) | 20,313 (80.6%) | 87,940 (78.2%) | 0.000 | 0.000 |
| Combined covariates | ||||||
| Diabetes | 143 (14.3%) | 3015 (12.0%) | 4399 (3.9%) | 0.019 | 0.000 | |
| Infertility | 525 (52.6%) | 11,589 (46.0%) | 28,603 (25.4%) | 0.000 | 0.000 | |
| Family income at index year | ||||||
| High | 141 (14.1%) | 8540 (33.9%) | 37,170 (33.1%) | 0.000 | 0.013 | |
| Middle | 356 (35.7%) | 7994 (31.7%) | 37,706 (33.5%) | 0.006 | 0.000 | |
| Low | 501 (50.2%) | 8669 (34.4%) | 37,538 (33.4%) | 0.000 | 0.002 | |
| PCOS OUH (N = 998) | PCOS Denmark (N = 25,203) | Controls (N = 112,414) | |||||
|---|---|---|---|---|---|---|---|
| N (%) | Incidence Rate per 1000 PY | N (%) | INCIDENCE Rate per 1000 PY | N (%) | Incidence Rate per 1000 PY | p ^ | |
| ICD-10 depression | |||||||
| Depressive episode (F320-F329) | 17 (1.7%) | 1.12 (0.68; 1.86) | 316 (1.3%) | 1.22 (1.09; 1.36) | 978 (0.9%) | 0.84 (0.79; 0.90) | 0.000 |
| Major depressive disorder, recurrent (F330-F339) | 54 (5.4%) | 4.16 (3.18; 5.43) | 742 (2.9%) | 2.92 (2.71; 3.14) | 2392 (2.1%) | 2.08 (2.00; 2.17) | 0.000 |
| Total ICD-10 (F32-F33) | 71 (7.1%) | 5.35 (4.23; 6.78) | 1058 (4.2%) | 4.19 (3.94; 4.45) | 3370 (3.0%) | 2.94 (2.85; 3.05) | 0.000 |
| Antidepressants | |||||||
| SSRI (N06AB) | 224 (22.4%) | 18.64 (16.29; 21.31) | 4071 (16.2%) | 18.18 (17.62; 18.75) | 13,449 (12.0%) | 12.81 (12.60; 13.03) | 0.000 |
| MAO inhibitors (N06AF, N06AG) | 0 (0%) | NA | 10 (0.0%) | 0.04 (0.02; 0.07) | 34 (0.0%) | 0.03 (0.02; 0.04) | 0.449 |
| Other (N06AX) | 160 (16.0%) | 12.80 (10.95; 14.97) | 2693 (10.7%) | 11.26 (10.84; 11.70) | 8542 (7.6%) | 7.76 (7.59; 7.92) | 0.000 |
| TCA (N06AA) | 83 (8.3%) | 6.31 (5.08; 7.85) | 1426 (5.7%) | 5.73 (5.44; 6.04) | 3942 (3.5%) | 3.46 (3.35; 3.57) | 0.000 |
| Total (N06A) | 299 (30.0%) | 26.55 (23.65; 29.80) | 5495 (21.8%) | 25.81 (25.12; 26.51) | 18,231 (16.2%) | 18.02 (17.76; 18.28) | 0.000 |
| Total event rate of depression | 307 (30.8%) | 27.44 (24.48; 30.75) | 5598 (22.2%) | 26.37 (25.68; 27.07) | 18,613 (16.6%) | 18.44 (18.17; 18.70) | 0.000 |
| Exposure | Mediating Factor | HRTotal (95% CI) | HRCDE (95% CI) | HEPE (95% CI) | PE (% (95%)) |
|---|---|---|---|---|---|
| PCOS | 1.42 (1.38; 1.47) | ||||
| 0.000 | |||||
| Diabetes mellitus | 1.37 (1.33; 1.41) | 1.04 (1.03; 1.04) | 12.5 (10.4; 14.5) | ||
| 0.000 | |||||
| Medical comorbidity | 1.42 (1.37; 1.46) | 1.00 (1.00; 1.01) | 1.5 (1.0; 2.0) | ||
| 0.000 | |||||
| Infertility | 1.41 (1.37; 1.46) | 1.01 (1.00; 1.01) | 2.3 (0.3; 4.3) | ||
| 0.000 | |||||
| Hormonal anticonception | 1.42 (1.38; 1.46) | 1.00 (1.00; 1.00) | 0.4 (0.2; 0.7) | ||
| 0.000 | |||||
| Low family income | 1.42 (1.37; 1.46) | 1.00 (1.00; 1.01) | 1.5 (0.2; 2.8) | ||
| 0.000 | |||||
| All mediating factors | 1.35 (1.31; 1.39) | 1.05 (1.04; 1.06) | 17.1 (14.3; 19.8) | ||
| 0.000 |
| Development of Depression in PCOS | Development of Depression in Controls | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Total | Yes A | No B | Total | Yes C | No D | PCOS vs. Controls | P A vs. B | P A vs. C | |
| Development of depression | 25,203 | 5598 | 19,605 | 112,414 | 18,613 | 93,801 | |||
| Age at diagnosis (y) Median (Q1, Q3) | 28 (23;35) | 29 (23;36) | 28 (23;35) | 28 (22;35) | 29 (23;36) | 28 (22;34) | 0.000 | 0.000 | 0.415 |
| N (%) | N (%) | N (%) | N (%) | N (%) | N (%) | ||||
| Age <20 years | 3724 (14.8%) | 779 (13.9%) | 2945 (15.0%) | 17,953 (16.0%) | 2771 (14.9%) | 15,182 (16.2%) | 0.000 | 0.040 | 0.000 |
| Characteristics | |||||||||
| Diabetes mellitus | 3015 (12.0%) | 967 (17.3%) | 2048 (10.4%) | 4399 (3.9%) | 1189 (6.4%) | 3210 (3.4%) | 0.000 | 0.000 | 0.000 |
| Comorbidity | 979 (3.9%) | 274 (4.9%) | 705 (3.6%) | 2944 (2.6%) | 661 (3.6%) | 2283 (2.4%) | 0.000 | 0.000 | 0.000 |
| Infertility | 11,589 (46.0%) | 2576 (46.0%) | 9013 (46.0%) | 28,603 (25.4%) | 5388 (28.9%) | 23,215 (24.7%) | 0.000 | 0.954 | 0.000 |
| Hormonal anticonception | 20,313 (80.6%) | 4443 (79.4%) | 15,870 (80.9%) | 87,940 (78.2%) | 14,463 (77.7%) | 73,477 (78.3%) | 0.000 | 0.008 | 0.057 |
| Low family income | 8669 (34.4%) | 2681 (47.9%) | 5988 (30.5%) | 37,538 (33.4%) | 8856 (47.6%) | 28,682 (30.6%) | 0.000 | 0.000 | 0.000 |
| All | Depression | ||||
|---|---|---|---|---|---|
| Yes N = 307 | No N = 691 | ||||
| Baseline Characteristics | N (%) | Median (Q1–Q3) | Median (Q1–Q3) | Median (Q1–Q3) | p # |
| Age (years) | 998 (100%) | 28 (21; 34) | 29 (22; 35) | 27 (21; 34) | 0.058 |
| BMI (kg/m2) | 930 (93.2%) | 26.8 (23.0; 32.2) | 27.7 (23.7; 33.6) | 26.4 (22.7; 31.2) | 0.002 |
| Waist (cm) | 628 (63%) | 88 (78; 103) | 90 (78; 106) | 88 (77; 101) | 0.077 |
| FG-score | 882 (88%) | 11 (5; 15) | 12 (7; 16) | 10 (5; 15) | 0.005 |
| Total testosterone (nmol/L) | 690 (69.1%) | 1.7 (1.3; 2.4) | 1.7 (1.3; 2.3) | 1.7 (1.2; 2.4) | 0.791 |
| SHBG (nmol/L) | 923 (92%) | 44 (31; 66) | 44 (29; 64) | 44 (31; 67) | 0.454 |
| Free testosterone (nmol/L) | 680 (68.136%) | 0.033 (0.021;0.048) | 0.034 (0.022;0.048) | 0.032 (0.021;0.048) | 0.418 |
| Fasting blood glucose (mmol/L) | 460 (46.1%) | 4.6 (4.2; 5.0) | 4.6 (4.3; 5.0) | 4.6 (4.2; 5.0) | 0.412 |
| N (%) | N (%) | N (%) | p¤ | ||
| BMI ≥ 25 kg/m2 | 562 (60.4%) | 187 (66.1%) | 375 (58.0%) | 0.020 | |
| BMI < 25 kg/m2 | 368 (39.6%) | 96 (33.9%) | 272 (42.0%) | 0.020 | |
| Waist ≥ 88 cm | 326 (51.9%) | 98 (56.3%) | 228 (50.2%) | 0.171 | |
| Waist < 88 cm | 302 (48.1%) | 76 (43.7%) | 226 (49.8%) | 0.171 | |
| FG score ≥ 7 | 628 (71.2%) | 206 (77.2%) | 422 (68.6%) | 0.010 | |
| FG score < 7 | 254 (28.8%) | 61 (22.8%) | 193 (31.4%) | 0.010 | |
| Depression | |||||
|---|---|---|---|---|---|
| Crude HR (95% CI) | N | p-Value | Age and BMI Adjusted HR a (95% CI) | p-Value | |
| Age (years) | 1.00 (0.99; 1.02) | 930 | 0.590 | 1.00 (0.99; 1.01) | 0.837 |
| BMI (kg/m2) | 1.02 (1.01; 1.04) | 930 | 0.003 | 1.02 (1.01; 1.04) | 0.003 |
| Waist (cm) | 1.01 (1.00; 1.02) | 616 | 0.014 | 1.03 (1.00; 1.05) | 0.022 |
| FG-score | 1.02 (1.00; 1.03) | 834 | 0.043 | 1.02 (1.00; 1.03) | 0.041 |
| Total testosterone (nmol/L) | 0.97 (0.85; 1.10) | 649 | 0.619 | 0.95 (0.83; 1.09) | 0.467 |
| SHBG (nmol/L) | 1.00 (1.00; 1.00) | 863 | 0.525 | 0.95 (0.83; 1.09) | 0.467 |
| Free testosterone (nmol/L) | 0.58 (0.04; 8.08) | 639 | 0.685 | 0.19 (0.01; 3.91) | 0.280 |
| Fasting blood glucose (mmol/L) | 1.20 (1.01; 1.42) | 441 | 0.037 | 1.18 (1.00; 1.39) | 0.055 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Glintborg, D.; Petersen, T.G.; Rubin, K.H.; Andersen, M.S. Diabetes Mellitus Mediates Risk of Depression in Danish Women with Polycystic Ovary Syndrome—A National Cohort Study. Biomedicines 2022, 10, 2396. https://doi.org/10.3390/biomedicines10102396
Glintborg D, Petersen TG, Rubin KH, Andersen MS. Diabetes Mellitus Mediates Risk of Depression in Danish Women with Polycystic Ovary Syndrome—A National Cohort Study. Biomedicines. 2022; 10(10):2396. https://doi.org/10.3390/biomedicines10102396
Chicago/Turabian StyleGlintborg, Dorte, Tanja Gram Petersen, Katrine Hass Rubin, and Marianne Skovsager Andersen. 2022. "Diabetes Mellitus Mediates Risk of Depression in Danish Women with Polycystic Ovary Syndrome—A National Cohort Study" Biomedicines 10, no. 10: 2396. https://doi.org/10.3390/biomedicines10102396