
Humoral Immune Response in IBD Patients Three and Six Months after Vaccination with the SARS-CoV-2 mRNA Vaccines mRNA-1273 and BNT162b2

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
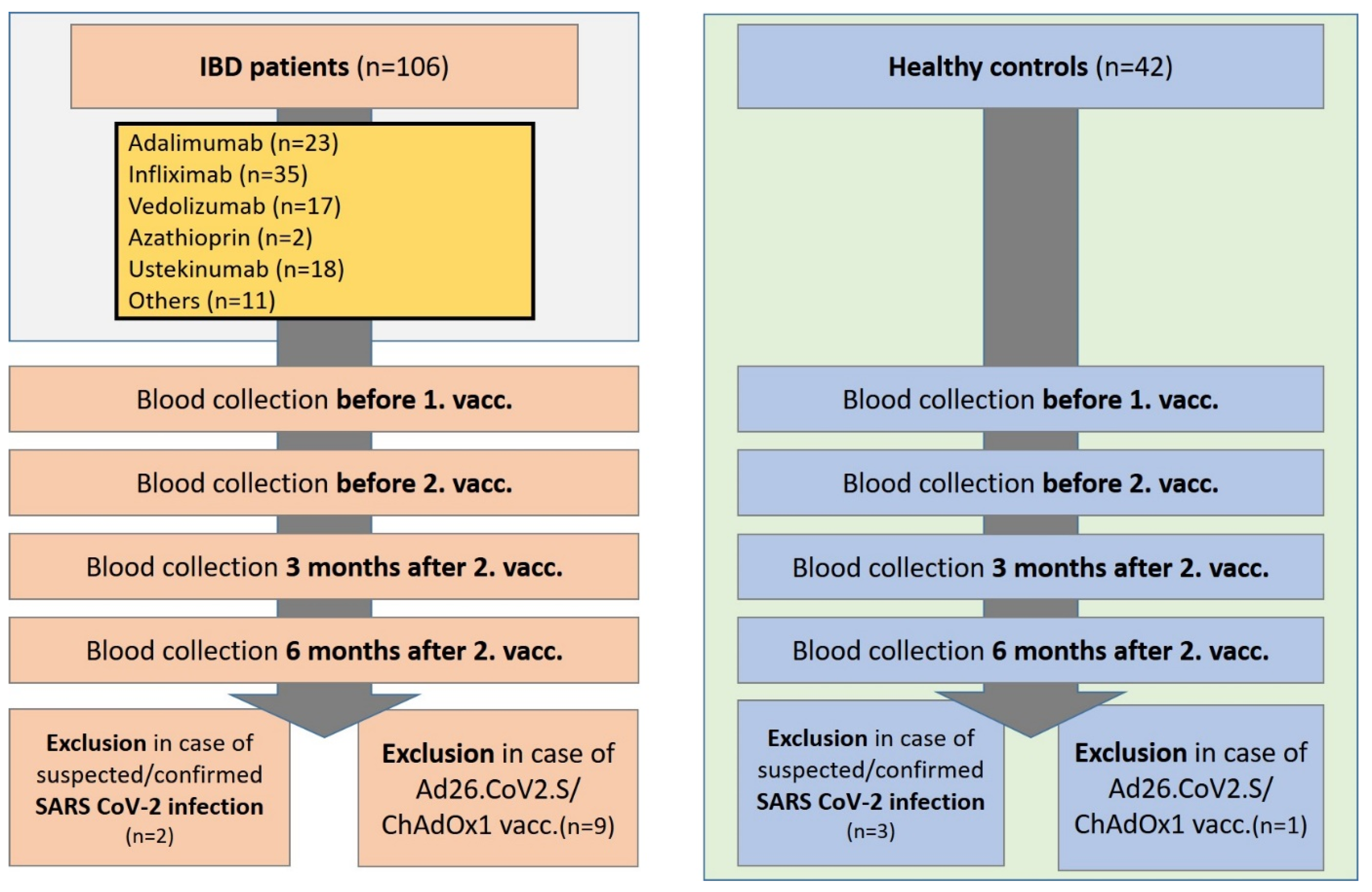
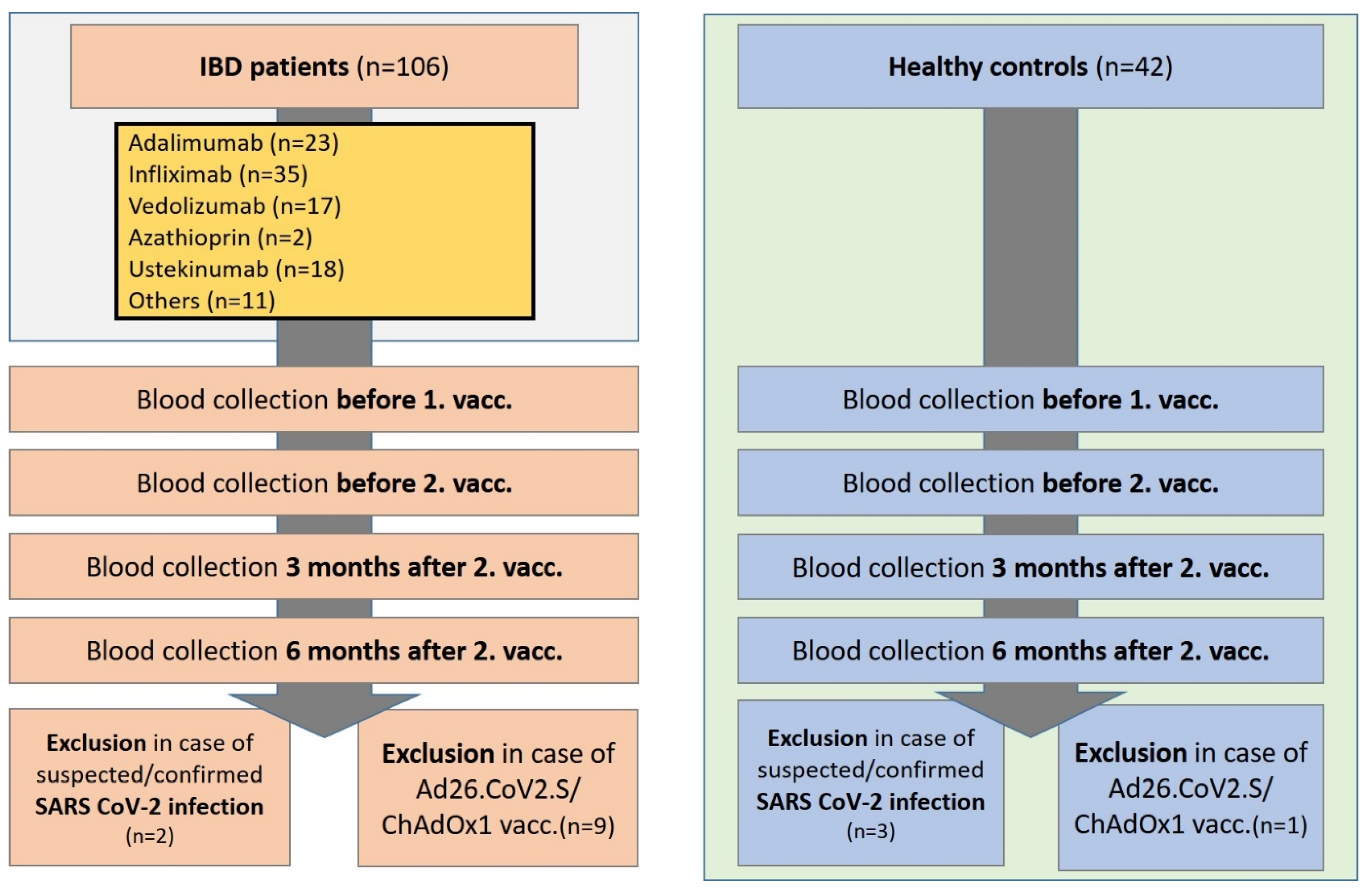
2.1. Study Subjects and Samples
2.2. Quantification of Serum Markers
2.3. SARS-CoV-2 Vaccines
2.4. Statistical Analysis
3. Results
3.1. Cohort Characteristics
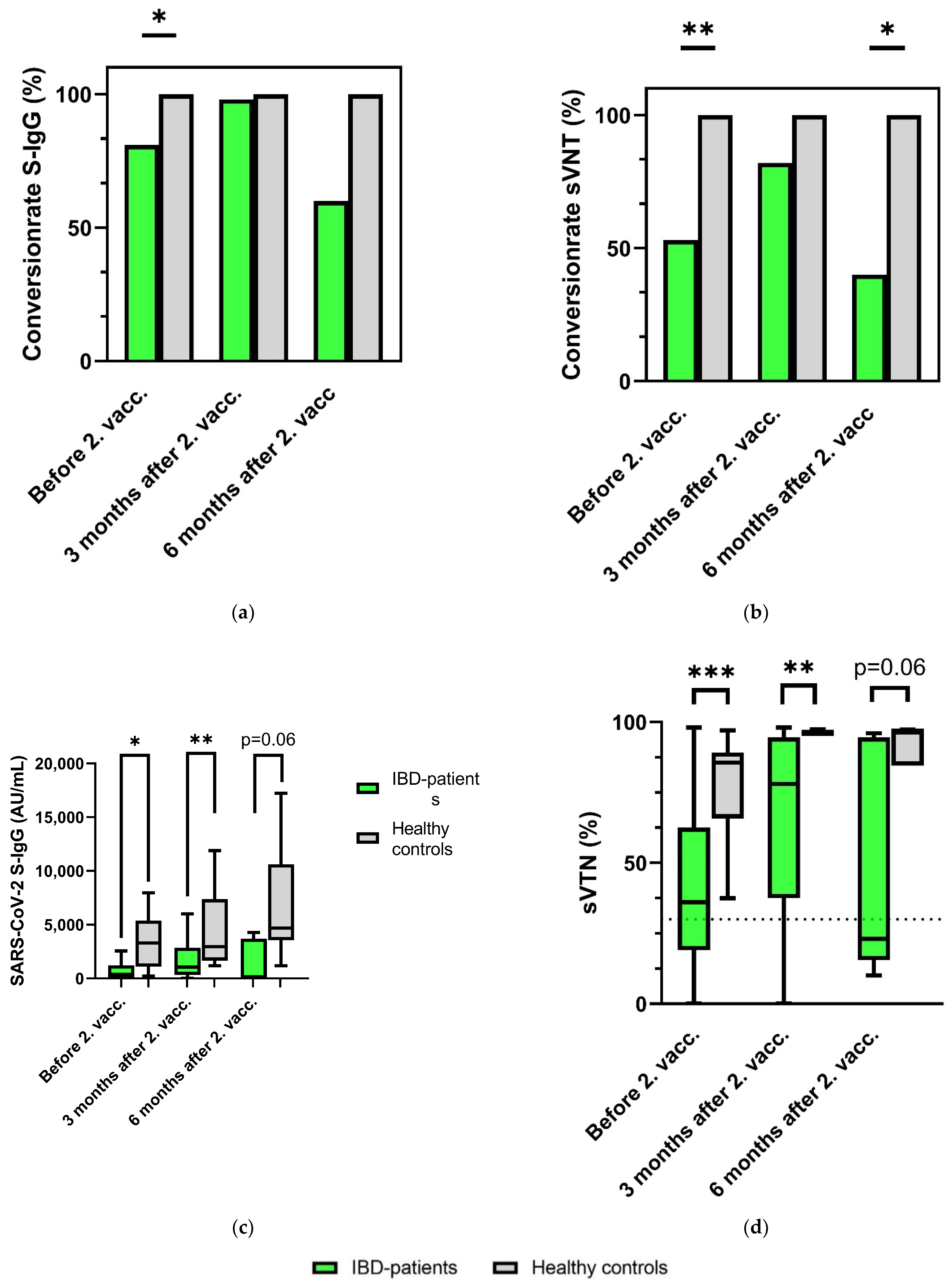
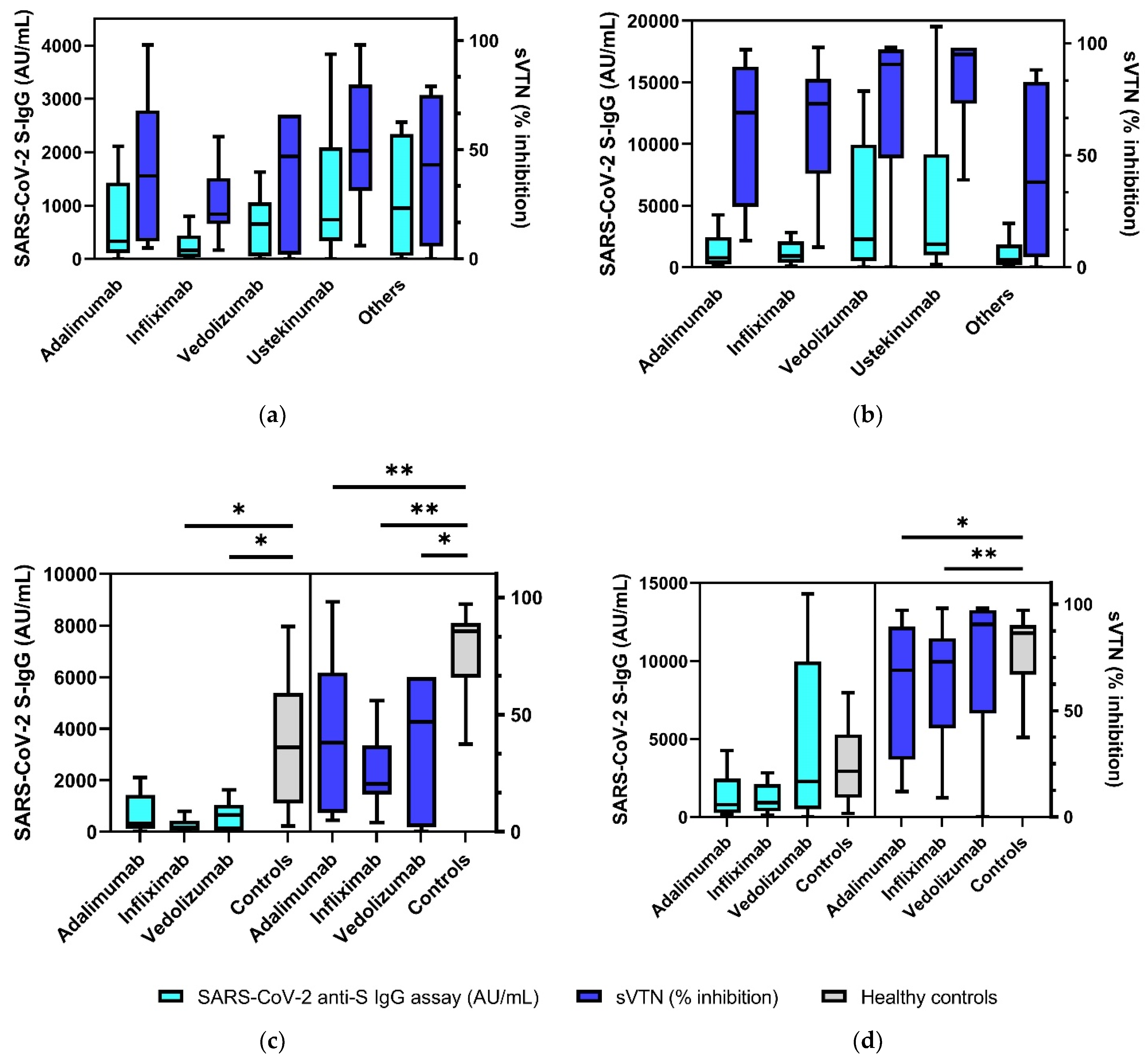
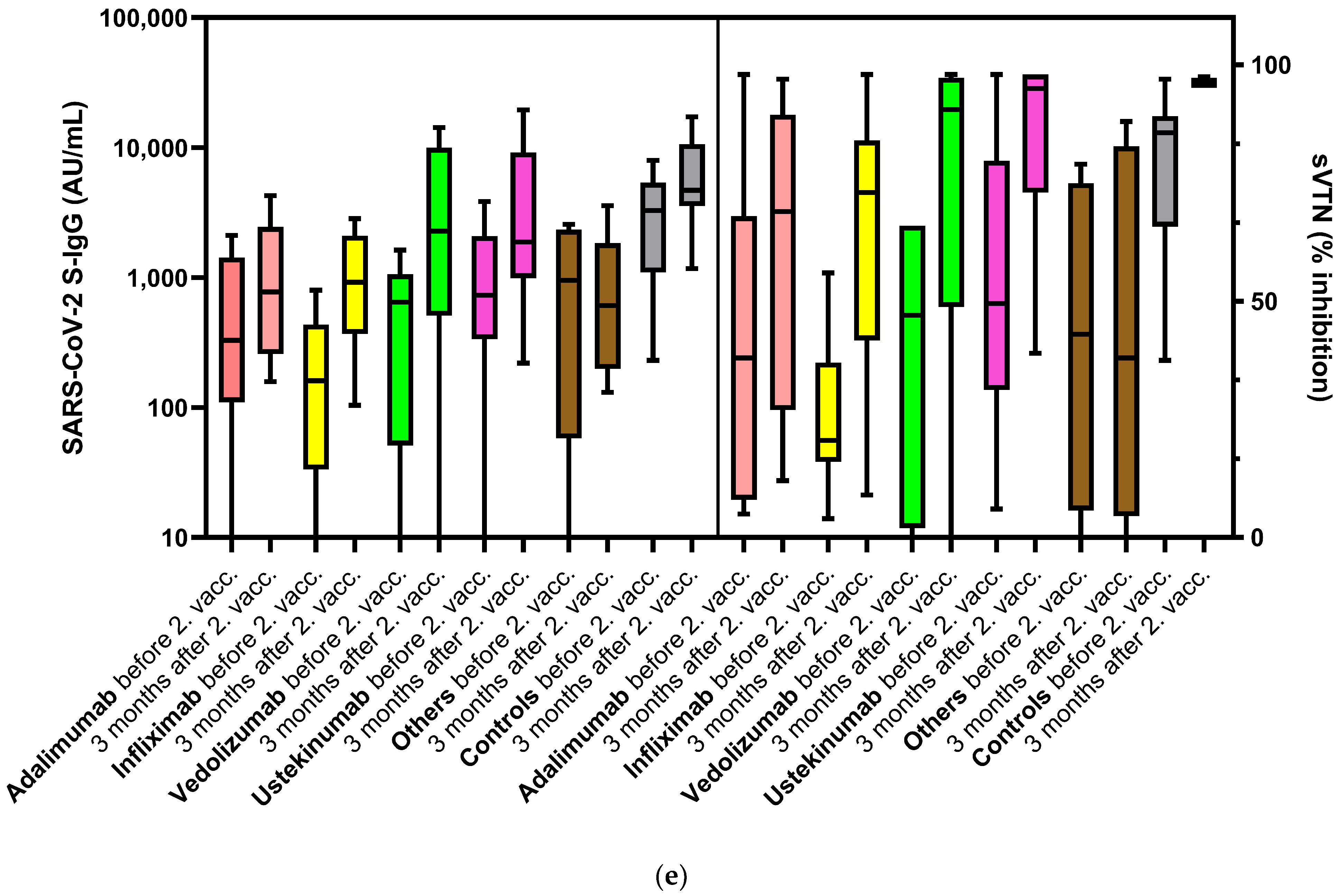
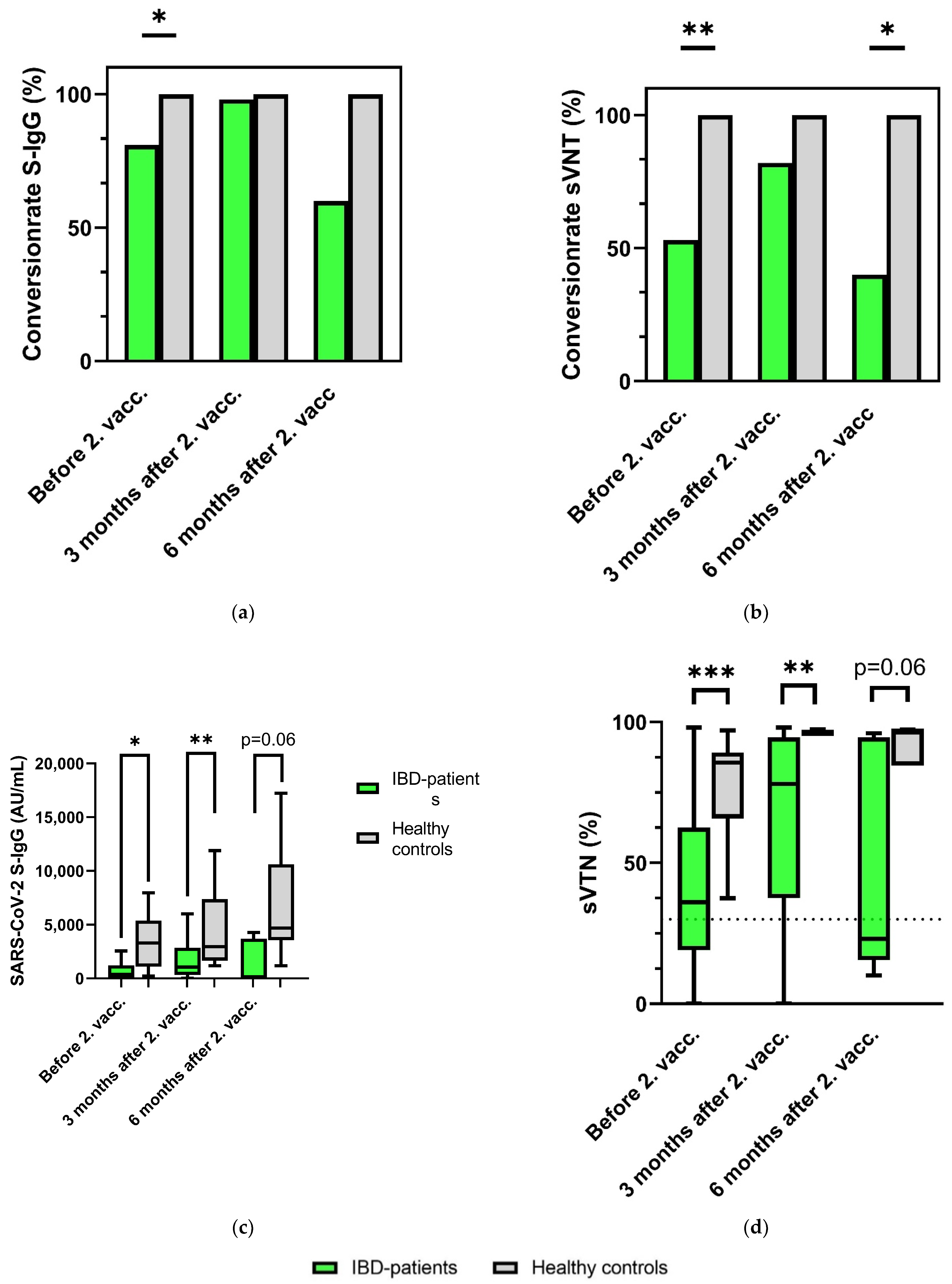
3.2. Significantly Decreased SARS-CoV-2 S-IgG and sVNT Inhibition Levels in IBD Patients 3 Months after Second Vaccination
3.3. Seroconversion Rates in IBD Patients after SARS-CoV-2 Vaccination
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Gorbalenya, A.E.; Baker, S.C.; Baric, R.S.; de Groot, R.J.; Drosten, C.; Gulyaeva, A.A.; Haagmans, B.L.; Lauber, C.; Leontovich, A.M.; Neuman, B.W.; et al. The species Severe acute respiratory syndrome-related coronavirus: Classifying 2019-nCoV and naming it SARS-CoV-2. Nat. Microbiol. 2020, 5, 536–544. [Google Scholar] [CrossRef] [Green Version]
- Vollenberg, R.; Matern, P.; Nowacki, T.; Fuhrmann, V.; Padberg, J.-S.; Ochs, K.; Schütte-Nütgen, K.; Strauß, M.; Schmidt, H.; Tepasse, P.-R. Prone Position in Mechanically Ventilated COVID-19 Patients: A Multicenter Study. J. Clin. Med. 2021, 10, 1046. [Google Scholar] [CrossRef]
- Tepasse, P.-R.; Hafezi, W.; Lutz, M.; Kühn, J.; Wilms, C.; Wiewrodt, R.; Sackarnd, J.; Keller, M.; Schmidt, H.H.; Vollenberg, R. Persisting SARS-CoV-2 viraemia after rituximab therapy: Two cases with fatal outcome and a review of the literature. Br. J. Haematol. 2020, 190, 185–188. [Google Scholar] [CrossRef]
- Cummings, M.J.; Baldwin, M.R.; Abrams, D.; Jacobson, S.D.; Meyer, B.J.; Balough, E.M.; Aaron, J.G.; Claassen, J.; Rabbani, L.E.; Hastie, J.; et al. Epidemiology, clinical course, and outcomes of critically ill adults with COVID-19 in New York City: A prospective cohort study. Lancet 2020, 395, 1763–1770. [Google Scholar] [CrossRef]
- Kessel, C.; Vollenberg, R.; Masjosthusmann, K.; Hinze, C.; Wittkowski, H.; Debaugnies, F.; Nagant, C.; Corazza, F.; Vély, F.; Kaplanski, G.; et al. Discrimination of COVID-19 From Inflammation-Induced Cytokine Storm Syndromes Using Disease-Related Blood Biomarkers. Arthritis Rheumatol. 2021, 73, 1791–1799. [Google Scholar] [CrossRef]
- Jose, R.J.; Manuel, A. COVID-19 cytokine storm: The interplay between inflammation and coagulation. Lancet Respir. Med. 2020, 8, e46–e47. [Google Scholar] [CrossRef]
- Varghese, J.; Sandmann, S.; Ochs, K.; Schrempf, I.-M.; Frömmel, C.; Dugas, M.; Schmidt, H.H.; Vollenberg, R.; Tepasse, P.-R. Persistent symptoms and lab abnormalities in patients who recovered from COVID-19. Sci. Rep. 2021, 11, 12775. [Google Scholar] [CrossRef]
- Deer, R.R.; Rock, M.A.; Vasilevsky, N.; Carmody, L.; Rando, H.; Anzalone, A.J.; Basson, M.D.; Bennett, T.D.; Bergquist, T.; Boudreau, E.A.; et al. Characterizing Long COVID: Deep Phenotype of a Complex Condition. EBioMedicine 2021, 74, 103722. [Google Scholar] [CrossRef] [PubMed]
- Nasserie, T.; Hittle, M.; Goodman, S.N. Assessment of the Frequency and Variety of Persistent Symptoms Among Patients With COVID-19: A Systematic Review. JAMA Netw. Open 2021, 4, e2111417. [Google Scholar] [CrossRef] [PubMed]
- Torres, J.; Mehandru, S.; Colombel, J.-F.; Peyrin-Biroulet, L. Crohn’s disease. Lancet 2017, 389, 1741–1755. [Google Scholar] [CrossRef]
- Ungaro, R.; Mehandru, S.; Allen, P.B.; Peyrin-Biroulet, L.; Colombel, J.-F. Ulcerative colitis. Lancet 2017, 389, 1756–1770. [Google Scholar] [CrossRef]
- Beaugerie, L.; Rahier, J.-F.; Kirchgesner, J. Predicting, Preventing, and Managing Treatment-Related Complications in Patients with Inflammatory Bowel Diseases. Clin. Gastroenterol. Hepatol. 2020, 18, 1324–1335.e2. [Google Scholar] [CrossRef]
- Singh, A.K.; Jena, A.; Kumar-M, P.; Sharma, V.; Sebastian, S. Risk and outcomes of coronavirus disease in patients with inflammatory bowel disease: A systematic review and meta-analysis. United Eur. Gastroenterol. J. 2021, 9, 159–176. [Google Scholar] [CrossRef] [PubMed]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Sadoff, J.; Gray, G.; Vandebosch, A.; Cárdenas, V.; Shukarev, G.; Grinsztejn, B.; Goepfert, P.A.; Truyers, C.; Fennema, H.; Spiessens, B.; et al. Safety and Efficacy of Single-Dose Ad26.COV2.S Vaccine against Covid-19. N. Engl. J. Med. 2021, 384, 2187–2201. [Google Scholar] [CrossRef]
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: An interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 2021, 397, 99–111. [Google Scholar] [CrossRef]
- Melmed, G.Y.; Botwin, G.J.; Sobhani, K.; Li, D.; Prostko, J.; Figueiredo, J.; Cheng, S.; Braun, J.; Mcgovern, D.P.B. Antibody Responses After SARS-CoV-2 mRNA Vaccination in Adults With Inflammatory Bowel Disease. Ann. Intern. Med. 2021, 174, 1768–1770. [Google Scholar] [CrossRef]
- Chanchlani, N.; Lin, S.; Chee, D.; Hamilton, B.; Nice, R.; Zehra, A.; Bewshea, C.; Cipriano, B.; Derikx, L.A.A.P.; Dunlop, A.; et al. Adalimumab and infliximab impair SARS-CoV-2 antibody responses: Results from a therapeutic drug monitoring study in 11422 biologic-treated patients. J. Crohns Colitis 2021. online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Tepasse, P.-R.; Vollenberg, R.; Nowacki, T. Vaccination against SARS-CoV-2 in Patients with Inflammatory Bowel Diseases: Where Do We Stand? Life 2021, 11, 1220. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, N.A.; Goodhand, J.R.; Bewshea, C.; Nice, R.; Chee, D.; Lin, S.; Chanchlani, N.; Butterworth, J.; Cooney, R.; Croft, N.M.; et al. Anti-SARS-CoV-2 antibody responses are attenuated in patients with IBD treated with infliximab. Gut 2021, 70, 865–875. [Google Scholar] [CrossRef]
- Wong, S.-Y.; Dixon, R.; Martinez Pazos, V.; Gnjatic, S.; Colombel, J.-F.; Cadwell, K. Serologic Response to Messenger RNA Coronavirus Disease 2019 Vaccines in Inflammatory Bowel Disease Patients Receiving Biologic Therapies. Gastroenterology 2021, 161, 715–718.e4. [Google Scholar] [CrossRef]
- Kappelman, M.D.; Weaver, K.N.; Boccieri, M.; Firestine, A.; Zhang, X.; Long, M.D. Humoral Immune Response to Messenger RNA COVID-19 Vaccines Among Patients with Inflammatory Bowel Disease. Gastroenterology 2021, 161, 1340–1343.e2. [Google Scholar] [CrossRef]
- Pozdnyakova, V.; Botwin, G.J.; Sobhani, K.; Prostko, J.; Braun, J.; Mcgovern, D.P.B.; Melmed, G.Y.; Appel, K.; Banty, A.; Feldman, E.; et al. Decreased Antibody Responses to Ad26.COV2.S Relative to SARS-CoV-2 mRNA Vaccines in Patients with Inflammatory Bowel Disease. Gastroenterology 2021, 161, 2041–2043. [Google Scholar] [CrossRef] [PubMed]
- Spencer, E.A.; Klang, E.; Dolinger, M.; Pittman, N.; Dubinsky, M.C. Seroconversion Following SARS-CoV-2 Infection or Vaccination in Pediatric IBD Patients. Inflamm. Bowel Dis. 2021, 27, 1862–1864. [Google Scholar] [CrossRef] [PubMed]
- Reuken, P.A.; Andreas, N.; Grunert, P.C.; Glöckner, S.; Kamradt, T.; Stallmach, A. T cell response after SARS-CoV-2 vaccination in immunocompromised patients with inflammatory bowel disease. J. Crohns Colitis 2021. online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- von Rhein, C.; Scholz, T.; Henss, L.; Kronstein-Wiedemann, R.; Schwarz, T.; Rodionov, R.N.; Corman, V.M.; Tonn, T.; Schnierle, B.S. Comparison of potency assays to assess SARS-CoV-2 neutralizing antibody capacity in COVID-19 convalescent plasma. J. Virol. Methods 2021, 288, 114031. [Google Scholar] [CrossRef] [PubMed]
- Tan, C.W.; Chia, W.N.; Qin, X.; Liu, P.; Chen, M.I.-C.; Tiu, C.; Hu, Z.; Chen, V.C.-W.; Young, B.E.; Sia, W.R.; et al. A SARS-CoV-2 surrogate virus neutralization test based on antibody-mediated blockage of ACE2-spike protein-protein interaction. Nat. Biotechnol. 2020, 38, 1073–1078. [Google Scholar] [CrossRef] [PubMed]
- Kapetanovic, M.C.; Saxne, T.; Nilsson, J.-A.; Geborek, P. Influenza vaccination as model for testing immune modulation induced by anti-TNF and methotrexate therapy in rheumatoid arthritis patients. Rheumatology 2007, 46, 608–611. [Google Scholar] [CrossRef] [Green Version]
- Park, S.H.; Yang, S.-K.; Park, S.-K.; Kim, J.W.; Yang, D.-H.; Jung, K.W.; Kim, K.-J.; Ye, B.D.; Byeon, J.-S.; Myung, S.-J.; et al. Efficacy of hepatitis A vaccination and factors impacting on seroconversion in patients with inflammatory bowel disease. Inflamm. Bowel Dis. 2014, 20, 69–74. [Google Scholar] [CrossRef]
- Kapetanovic, M.C.; Saxne, T.; Sjöholm, A.; Truedsson, L.; Jönsson, G.; Geborek, P. Influence of methotrexate, TNF blockers and prednisolone on antibody responses to pneumococcal polysaccharide vaccine in patients with rheumatoid arthritis. Rheumatology 2006, 45, 106–111. [Google Scholar] [CrossRef] [Green Version]
- Andrade, P.; Santos-Antunes, J.; Rodrigues, S.; Lopes, S.; Macedo, G. Treatment with infliximab or azathioprine negatively impact the efficacy of hepatitis B vaccine in inflammatory bowel disease patients. J. Gastroenterol. Hepatol. 2015, 30, 1591–1595. [Google Scholar] [CrossRef]
- Papp, K.A.; Haraoui, B.; Kumar, D.; Marshall, J.K.; Bissonnette, R.; Bitton, A.; Bressler, B.; Gooderham, M.; Ho, V.; Jamal, S.; et al. Vaccination Guidelines for Patients With Immune-Mediated Disorders on Immunosuppressive Therapies. J. Cutan. Med. Surg. 2019, 23, 50–74. [Google Scholar] [CrossRef] [Green Version]
- Harrington, J.E.; Hamilton, R.E.; Ganley-Leal, L.; Farraye, F.A.; Wasan, S.K. The Immunogenicity of the Influenza, Pneumococcal, and Hepatitis B Vaccines in Patients with Inflammatory Bowel Disease Treated with Vedolizumab. Crohn’s Colitis 2020, 2, 3762–3779. [Google Scholar] [CrossRef]
- Wyant, T.; Leach, T.; Sankoh, S.; Wang, Y.; Paolino, J.; Pasetti, M.F.; Feagan, B.G.; Parikh, A. Vedolizumab affects antibody responses to immunisation selectively in the gastrointestinal tract: Randomised controlled trial results. Gut 2015, 64, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Scribano, M.L. Vedolizumab for inflammatory bowel disease: From randomized controlled trials to real-life evidence. World J. Gastroenterol. 2018, 24, 2457–2467. [Google Scholar] [CrossRef]
- Lu, Y.; Jacobson, D.L.; Ashworth, L.A.; Grand, R.J.; Meyer, A.L.; McNeal, M.M.; Gregas, M.C.; Burchett, S.K.; Bousvaros, A. Immune response to influenza vaccine in children with inflammatory bowel disease. Am. J. Gastroenterol. 2009, 104, 444–453. [Google Scholar] [CrossRef] [PubMed]
- Askling, H.H.; Rombo, L.; van Vollenhoven, R.; Hallén, I.; Thörner, Å.; Nordin, M.; Herzog, C.; Kantele, A. Hepatitis A vaccine for immunosuppressed patients with rheumatoid arthritis: A prospective, open-label, multi-centre study. Travel Med. Infect. Dis. 2014, 12, 134–142. [Google Scholar] [CrossRef]
- Cerna, K.; Duricova, D.; Lukas, M.; Machkova, N.; Hruba, V.; Mitrova, K.; Kubickova, K.; Kostrejova, M.; Teplan, V.; Vasatko, M.; et al. Anti-SARS-CoV-2 Vaccination and Antibody Response in Patients With Inflammatory Bowel Disease on Immune-modifying Therapy: Prospective Single-Tertiary Study. Inflamm. Bowel Dis. 2021. [Google Scholar] [CrossRef] [PubMed]
- Perkmann, T.; Perkmann-Nagele, N.; Koller, T.; Mucher, P.; Radakovics, A.; Marculescu, R.; Wolzt, M.; Wagner, O.F.; Binder, C.J.; Haslacher, H. Anti-Spike Protein Assays to Determine SARS-CoV-2 Antibody Levels: A Head-to-Head Comparison of Five Quantitative Assays. Microbiol. Spectr. 2021, 9, e0024721. [Google Scholar] [CrossRef] [PubMed]
- Nace, D.A.; Kip, K.E.; Palmer, O.M.P.; Shurin, M.R.; Mulvey, K.; Crandall, M.; Kane, A.L.; Lukanski, A.; Kip, P.L.; Wells, A.L. Antibody Responses in Elderly Residential Care Persons following COVID-19 mRNA Vaccination. medRxiv 2021, preprint. [Google Scholar]
- Naaber, P.; Tserel, L.; Kangro, K.; Sepp, E.; Jürjenson, V.; Adamson, A.; Haljasmägi, L.; Rumm, A.P.; Maruste, R.; Kärner, J.; et al. Dynamics of antibody response to BNT162b2 vaccine after six months: A longitudinal prospective study. Lancet Reg. Health Eur. 2021, 10, 100208. [Google Scholar] [CrossRef] [PubMed]
- Naschitz, J.E.; Kertes, J.; Pinto, G.; Zaigraykin, N.; Oz, D.; Goland, E.; Nasser, S.; Supino-Rosin, L.; Lazar, R.; Ekka-Zohar, A. Comparison of Covid-19 antibody status after vaccination between residents in long-term geriatric care and residents assisted-living facilities. Infect. Dis. 2021, 1–5. [Google Scholar] [CrossRef]
- Sourij, C.; Tripolt, N.J.; Aziz, F.; Aberer, F.; Forstner, P.; Obermayer, A.M.; Kojzar, H.; Kleinhappl, B.; Pferschy, P.N.; Mader, J.K.; et al. Humoral immune response to Covid-19 vaccination in diabetes: Age-dependent but independent of type of diabetes and glycaemic control—The prospective COVAC-DM cohort study. Diabetes Obes. Metab. medRxiv 2022, preprint. [Google Scholar] [CrossRef] [PubMed]
- Khan, N.; Mahmud, N. Effectiveness of SARS-CoV-2 Vaccination in a Veterans Affairs Cohort of Patients with Inflammatory Bowel Disease with Diverse Exposure to Immunosuppressive Medications. Gastroenterology 2021, 161, 827–836. [Google Scholar] [CrossRef] [PubMed]
- Steensels, D.; Pierlet, N.; Penders, J.; Mesotten, D.; Heylen, L. Comparison of SARS-CoV-2 Antibody Response Following Vaccination with BNT162b2 and mRNA-1273. JAMA 2021, 326, 1533–1535. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients | IBD (n = 95) | Adalimumab (n = 21) | Infliximab (n = 31) | Vedolizumab (n = 15) | Ustekinumab (n = 18) | Others (n = 9) | p-Value | |
|---|---|---|---|---|---|---|---|---|
| Patient characteristics | Age, years median (IQR) | 46 (33–55) | 37 (31–56) | 49 (44–54) | 46 (34–60) | 41 (27–57) | 33 (30–48) | 0.093 |
| Sex, male (%) | 50 (53) | 13 (62) | 15 (48) | 10 (67) | 7 (39) | 4 (44) | 0.474 | |
| BMI | 25 (22–28) | 25 (22–28) | 24 (22–27) | 26 (21–31) | 25 (22–29) | 25 (23–28) | 0.970 | |
| Death (abs.) | 0 | 0 | 0 | 0 | 0 | 0 | 1 | |
| SARS-CoV-2 vaccine | mRNA-1273 (%) | 6 (6) | 3 (14) | 1 (3) | 0 (0) | 2 (11) | 0 (0) | 0.273 |
| BNT162b2 (%) | 89 (94) | 18 (86) | 30 (97) | 15 (100) | 16 (89) | 9 (100) | 0.273 | |
| IBD | Crohn’s disease (%) | 60 (63) | 11 (52) | 23 (74) | 4 (27) | 13 (72) | 8 (89) | 0.005 |
| CDAI score, median (IQR) | 0 (0–85) | 0 (0–103) | 0 (0–10) | 161 (79–233) | 0 (0–130) | 0 (0–148) | 0.025 | |
| Ulcerative colitis (%) | 35 (37) | 10 (48) | 8 (26) | 11 (73) | 5 (28) | 1 (11) | 0.005 | |
| Mayo score, median (IQR) | 3 (0–5) | 0 (0–3) | 3 (1–4) | 4 (2–7) | 5 (3–9) | 0 (0–0) | 0.044 | |
| Medication | Prednisolone p.o. (%) | 11 (12) | 0 (0) | 1 (3) | 4 (27) | 3 (17) | 3 (33) | 0.018 |
| Budesonide p.o. (%) | 4 (4) | 0 (0) | 2 (7) | 0 (0) | 1 (6) | 1 (11) | 0.578 | |
| Budesonide supp. (%) | 9 (10) | 0 (0) | 2 (7) | 5 (33) | 1 (6) | 1 (11) | 0.012 | |
| Mesalazine p.o. (%) | 44 (46) | 11 (52) | 11 (36) | 9 (60) | 7 (39) | 6 (67) | 0.399 | |
| Mesalazine supp (%) | 14 (15) | 3 (14) | 1 (3) | 4 (27) | 4 (22) | 2 (22) | 0.200 | |
| Pre-existing conditions | Cardiovascular disease | 21 (22) | 3 (14) | 9 (29) | 6 (40) | 2 (11) | 1 (11) | 0.164 |
| Respiratory disease (%) | 9 (10) | 1 (5) | 2 (7) | 4 (27) | 1 (6) | 1 (1) | 0.173 | |
| Kidney insufficiency (%) | 3 (3) | 0 (0) | 2 (7) | 1 (7) | 0 (0) | 0 (0) | 0.509 | |
| Metastatic neoplasm (%) | 1 (1) | 0 (0) | 1 (3) | 0 (0) | 0 (0) | 0 (0) | 0.720 | |
| Diabetes (%) | 3 (3) | 0 (0) | 2 (7) | 1 (7) | 0 (0) | 0 (0) | 0.509 | |
| Hematologic malignancy (%) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 |
| Patients | IBD (n = 95) | Controls (n = 38) | p-Value | Adalimumab (n = 21) | Infliximab (n = 31) | Vedolizumab (n = 15) | Ustekinumab (n = 18) | Others (n = 9) | p-Value | |
|---|---|---|---|---|---|---|---|---|---|---|
| Before 2nd vaccination | Samples (n) | 52 | 22 | 11 | 17 | 7 | 12 | 4 | ||
| SARS-CoV-2 S-IgG (AU/mL), median (IQR) | 329 (86–1058) | 3285 (1094–5385) | <0.001 | 329 (110–1428) | 161 (34–435) | 649 (51–1058) | 732 (334–2091) | 952 (58–2338) | 0.136 | |
| Seroconversion rateS-IgG (%) | 81 | 100 | 0.022 | 82 | 72 | 86 | 92 | 75 | 0.742 | |
| sVNT (%), median (IQR) | 36 (19–63) | 85 (64–89) | <0.001 | 38 (8–68) | 21 (16–37) | 47 (2–66) | 50 (31–80) | 43 (6–75) | 0.201 | |
| Seroconversion rate sVNT (%) | 53 | 100 | <0.001 | 55 | 35 | 57 | 75 | 50 | 0.337 | |
| 3 months after 2nd vaccination | Samples (n) | 60 | 11 | 13 | 20 | 10 | 11 | 6 | ||
| SARS-CoV-2 S-IgG (AU/mL), median (IQR) | 1116 (360–3214) | 4684 (3552–10,630) | 0.001 | 777 (258–2451) | 920 (367–2100) | 2281 (510–9964) | 1867 (988–9177) | 609 (198–1841) | 0.176 | |
| Seroconversion rateS-IgG (%) | 98 | 100 | 0.847 | 100 | 100 | 90 | 100 | 67 | 0.394 | |
| sVNT (%), median (IQR) | 78 (38–95) | 96 (95–97) | 0.002 | 69 (27–90) | 73 (42–84) | 90 (48–97) | 95 (73–98) | 38 (5–83) | 0.093 | |
| Seroconversion rate sVNT (%) | 82 | 100 | 0.138 | 69 | 85 | 90 | 91 | 67 | 0.585 | |
| 6 months after 2nd vaccination | Samples (n) | 4 | 7 | 1 | 3 | 0 | 0 | 0 | ||
| SARS-CoV-2 S-IgG (AU/mL), median (IQR) | 104 (0–3709) | 4289 (1674–8730) | 0.061 | 104 | 0 (0–0) | 0.755 | ||||
| Seroconversion rate S-IgG (%) | 60 | 100 | 0.152 | 100 | 33 | 0.329 | ||||
| sVNT (%), median (IQR) | 23 (15–95) | 97 (85–97) | 0.062 | 21 | 23 (10–23) | 0.344 | ||||
| Seroconversion rate sVNT (%) | 40 | 100 | 0.045 | 0 | 33 | 0.392 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vollenberg, R.; Tepasse, P.-R.; Kühn, J.E.; Hennies, M.; Strauss, M.; Rennebaum, F.; Schomacher, T.; Boeckel, G.; Lorentzen, E.; Bokemeyer, A.; et al. Humoral Immune Response in IBD Patients Three and Six Months after Vaccination with the SARS-CoV-2 mRNA Vaccines mRNA-1273 and BNT162b2. Biomedicines 2022, 10, 171. https://doi.org/10.3390/biomedicines10010171
Vollenberg R, Tepasse P-R, Kühn JE, Hennies M, Strauss M, Rennebaum F, Schomacher T, Boeckel G, Lorentzen E, Bokemeyer A, et al. Humoral Immune Response in IBD Patients Three and Six Months after Vaccination with the SARS-CoV-2 mRNA Vaccines mRNA-1273 and BNT162b2. Biomedicines. 2022; 10(1):171. https://doi.org/10.3390/biomedicines10010171
Chicago/Turabian StyleVollenberg, Richard, Phil-Robin Tepasse, Joachim Ewald Kühn, Marc Hennies, Markus Strauss, Florian Rennebaum, Tina Schomacher, Göran Boeckel, Eva Lorentzen, Arne Bokemeyer, and et al. 2022. "Humoral Immune Response in IBD Patients Three and Six Months after Vaccination with the SARS-CoV-2 mRNA Vaccines mRNA-1273 and BNT162b2" Biomedicines 10, no. 1: 171. https://doi.org/10.3390/biomedicines10010171
APA StyleVollenberg, R., Tepasse, P.-R., Kühn, J. E., Hennies, M., Strauss, M., Rennebaum, F., Schomacher, T., Boeckel, G., Lorentzen, E., Bokemeyer, A., & Nowacki, T. M. (2022). Humoral Immune Response in IBD Patients Three and Six Months after Vaccination with the SARS-CoV-2 mRNA Vaccines mRNA-1273 and BNT162b2. Biomedicines, 10(1), 171. https://doi.org/10.3390/biomedicines10010171