
SmartCards as Analogous Tools to Operate Tablet Computers for Elderly—A Feasibility Study

Abstract
:1. Introduction
2. Methods
2.1. Participants
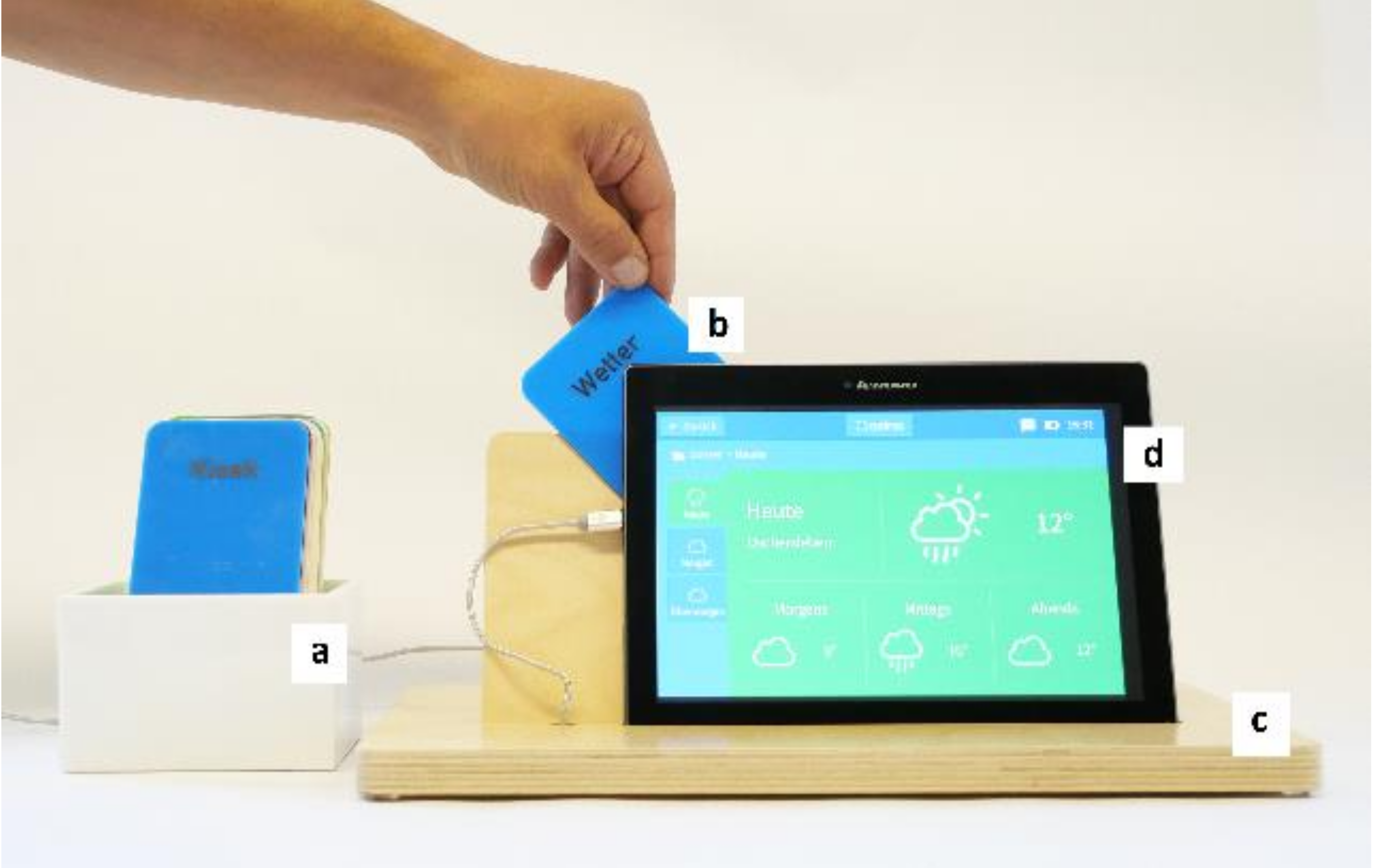
2.2. Materials and Procedure
3. Study Design and Statistical Analyses
4. Results
4.1. Descriptive Statistics
4.2. Hypothesis 1
4.3. Hypothesis 2
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McGaughey, R.E.; Zeltmann, S.M.; McMurtrey, M.E. Motivations and obstacles to smartphone use by the elderly: Developing a research framework. Int. J. Electron. Financ. 2013, 7, 177. [Google Scholar] [CrossRef]
- Peek, S.T.M.; Luijkx, K.G.; Vrijhoef, H.J.M.; Nieboer, M.E.; Aarts, S.; van der Voort, C.S.; Wouters, E.J.M. Origins and consequences of technology acquirement by independent-living seniors: Towards an integrative model. BMC Geriatr. 2017, 17, 1–18. [Google Scholar] [CrossRef] [Green Version]
- Seilbeck, C.; Langmeyer, A. Ergebnisse der Studie “Generationenübergreifende Zeitverwendung: Großeltern, Eltern, Enkel”; Deutsches Jugendinstitut e.V.: München, Germany, 2018. [Google Scholar]
- Boamah, S.A.; Weldrick, R.; Lee, T.S.J.; Taylor, N. Social Isolation Among Older Adults in Long-Term Care: A Scoping Review. J. Aging Health 2021, 08982643211004174. [Google Scholar] [CrossRef]
- Repetto, M.; Trentin, G. ICT and lifelong learning for senior citizens. J. E-Learn. Knowl. Soc. 2008, 4, 189–198. [Google Scholar]
- Wong, Y.C.; Chen, H.; Lee, V.W.; Fung, J.Y.; Law, C.K. Empowerment of senior citizens via the learning of information and communication technology. Ageing Int. 2014, 39, 144–162. [Google Scholar] [CrossRef]
- Gu, Y.; Suh, A.; Liu, L. Motivations and obstacles for seniors to adopt social network services. In Proceedings of the PACIS 2015, Singapore, 5–9 July 2015; pp. 1–13. Available online: https://aisel.aisnet.org/pacis2015/152 (accessed on 3 September 2021).
- Griffin, S.C.; Williams, A.B.; Mladen, S.N.; Perrin, P.B.; Dzierzewski, J.M.; Rybarczyk, B.D. Reciprocal effects between loneliness and sleep disturbance in older Americans. J. Aging Health 2020, 32, 1156–1164. [Google Scholar] [CrossRef]
- Lara, E.; Caballero, F.F.; Rico-Uribe, L.A.; Olaya, B.; Haro, J.M.; Ayuso-Mateos, J.L.; Miret, M. Are loneliness and social isolation associated with cognitive decline? Int. J. Geriatr. Psychiatry 2019, 34, 1613–1622. [Google Scholar] [CrossRef]
- Shankar, A.; Hamer, M.; McMunn, A.; Steptoe, A. Social Isolation and Loneliness: Relationships With Cognitive Function During 4 Years of Follow-up in the English Longitudinal Study of Ageing. Psychosom. Med. 2013, 75, 161–170. [Google Scholar] [CrossRef]
- Kelly, M.E.; Duff, H.; Kelly, S.; McHugh Power, J.E.; Brennan, S.; Lawlor, B.A.; Loughrey, D.G. The impact of social activities, social networks, social support and social relationships on the cognitive functioning of healthy older adults: A systematic review. Syst. Rev. 2017, 6, 1–18. [Google Scholar] [CrossRef]
- Smith, G.L.; Banting, L.; Eime, R.; O’ Sullivan, G.; van Uffelen Jannique, G.Z. The association between social support and physical activity in older adults: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 1–21. [Google Scholar] [CrossRef]
- Uchino, B.N.; Trettevik, R.; Kent de Grey Robert, G.; Cronan, S.; Hogan, J.; Baucom, B.R.W. Social support, social integration, and inflammatory cytokines: A meta-analysis. Health Psychol. 2018, 37, 462–471. [Google Scholar] [CrossRef]
- Ajzen, I. The Theory of Planned Behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Ajzen, I.; Fishbein, M. Understanding Attitudes and Predicting Social Behavior; Prentice-Hall: Englewood Cliffs, NJ, USA, 1980. [Google Scholar]
- Fishbein, M.A. Reasoned Action Approach to Health Promotion. Med. Decis. Mak. 2008, 28, 834–844. [Google Scholar] [CrossRef] [PubMed]
- Venkatesh, V.; Morris, M.G.; Davis, G.B.; Davis, F.D. User acceptance of information technology: Toward a unified view. MIS Q. 2003, 27, 425–478. [Google Scholar] [CrossRef] [Green Version]
- Chan, M.Y.; Haber, S.; Drew, L.M.; Park, D.C. Training older adults to use tablet computers: Does it enhance cognitive function? Gerontologist 2016, 56, 475–484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Myhre, J.W.; Mehl, M.R.; Glisky, E.L. Cognitive benefits of online social networking for healthy older adults. J. Gerontol. B 2017, 72, 752–760. [Google Scholar] [CrossRef] [Green Version]
- Quinn, K. Cognitive Effects of Social Media Use: A Case of Older Adults. Soc. Media Soc. 2018, 4, 2056305118787203. [Google Scholar] [CrossRef]
- Hong, S.G.; Trimi, S.; Kim, D.W. Smartphone use and internet literacy of senior citizens. J. Assist. Technol. 2016, 10, 27–38. [Google Scholar] [CrossRef]
- Goumopoulos, C.; Papa, I.; Stavrianos, A. Development and evaluation of a mobile application suite for enhancing the social inclusion and well-being of seniors. Informatics 2017, 4, 15. [Google Scholar] [CrossRef] [Green Version]
- Chao, J.; Luo, P.; Yeh, Y.; Kao, H. The study of learning effects of mobile devices courses for Taiwanese senior citizens using the Kirkpatrick model. Int. J. Electr. Eng. Educ. 2018, 12, 1–27. [Google Scholar] [CrossRef]
- Van Grootven, B.; van Achterberg, T. The European Union’s Ambient and Assisted Living Joint Programme: An evaluation of its impact on population health and well-being. Health Inform. J. 2019, 25, 27–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maan, C.; Gunawardana, U. Barriers in acceptance of Ambient Assisted Living technologies among older Australians. In Proceedings of the 2017 IEEE Life Sciences Conference (LSC), Sydney, NSW, Australia, 13–15 December 2017; IEEE: Piscataway, NJ, USA, 2017; pp. 222–225. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Groups | Age | Number of Children | Level of Care 1 | Clock Drawing * | |
|---|---|---|---|---|---|
| home assistance service A | M | 81.75 | 1.75 | 1.29 | 2.17 |
| n | 12 | 12 | 7 | 12 | |
| SD | 4.20 | 0.62 | 0.49 | 1.19 | |
| Min | 78 | 1 | 1 | 1 | |
| Max | 88 | 3 | 2 | 4 | |
| retirement home B | M | 77.11 | 2.17 | 2.57 | 3.0 |
| n | 9 | 6 | 7 | 9 | |
| SD | 11.53 | 0.98 | 1.13 | 1.32 | |
| Min | 58 | 1 | 1 | 1 | |
| Max | 95 | 4 | 4 | 5 | |
| control group C | M | 86.11 | 1,89 | 2.29 | 3.56 |
| n | 9 | 9 | 7 | 9 | |
| SD | 4.46 | 0.78 | 0.49 | 1.93 | |
| Min | 81 | 1 | 2 | 1 | |
| Max | 95 | 3 | 3 | 6 | |
| Group | ||||||||
|---|---|---|---|---|---|---|---|---|
| A | B | C | Chi2 | Df | p | |||
| I find it complicated to use new technology. I just can’t operate it. | M | 2.92 | 3.11 | 4.44 | 8.09 | 2 | <0.05 | |
| perceived behavioral control | SD | 0.99 | 1.27 | 1.01 | ||||
| I would have liked to have learned to use a computer. | M | 4.50 | 2.33 | 3.44 | 8.44 | 2 | <0.05 | |
| SD | 1.17 | 1.80 | 1.94 | |||||
| I think I could handle technical devices well. | M | 4.08 | 2.43 | 2.67 | 7.07 | 2 | <0.05 | |
| SD | 0.99 | 1.27 | 1.66 | |||||
| It is a good idea to use the device. | M | 4.83 | 4.67 | 3.80 | 3.70 | 2 | 0.16 | |
| SD | 0.39 | 0.71 | 1.64 | |||||
| attitude towards the behavior | I am intending to try out the device extensively. | M | 4.75 | 4.11 | 3.40 | 4.13 | 2 | 0.137 |
| SD | 0.62 | 1.17 | 1.82 | |||||
| I like the notion to use the device. | M | 4.67 | 4.11 | 3.00 | 4.06 | 2 | 0.13 | |
| SD | 0.65 | 1.05 | 2.00 | |||||
| subjective norm | In the opinion of my family I should use technical assistance systems. | M | 5.00 | 4.00 | 2.89 | 9.50 | 2 | <0.01 |
| SD | 0.00 | 1.73 | 1.83 | |||||
| In the opinion of my friends and acquaintances I should use technical assistance systems. | M | 3.08 | 3.00 | 2.14 | 0.77 | 2 | 0.68 | |
| SD | 2.02 | 1.94 | 1.46 | |||||
| Frequency of Use * | Duration of Use * | |||
|---|---|---|---|---|
| I find it complicated to use new technology. I just can’t operate it. | r | 0.164 | 0.050 | |
| perceived behavioral control | ||||
| I would have liked to have learned to use a computer. | r | −0.132 | 0.158 | |
| I think I could handle technical devices well. | r | −0.217 | −0.278 | |
| It is a good idea to use the device. | r | 0.117 | 0.140 | |
| attitude towards the behavior | I am intending to try out the device extensively. | r | 0.145 | 0.173 |
| I like the notion to use the device. | r | 0.364 | 0.204 | |
| In the opinion of my family I should use technical assistance systems. | r | −0.128 | 0.081 | |
| subjective norm | In the opinion of my friends and acquaintances I should use technical assistance systems. | r | 0.322 | 0.240 |
| Group | Wilcoxon Signed Ranks Test | Autonomy | Loneliness | Wellbeing | Cognitive Ability |
|---|---|---|---|---|---|
| A | z | −0.714 | −1.176 | −1.426 | −2.827 |
| p | 0.475 | 0.240 | 0.154 | <0.005 | |
| B | z | −0.740 | −1.378 | −0.816 | −2.014 |
| p | 0.459 | 0.168 | 0.414 | <0.05 | |
| C | z | −0.170 | −1.219 | −0.138 | −0.931 |
| p | 0.865 | 0.223 | 0.890 | 0.352 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mueller, S.M.; Göttke-Krogmann, B.; Kortus, J.; Wiechmann, M.; Weber, M.; Mozek, S.; Mau, W.; Golla, A.; Huebner, G. SmartCards as Analogous Tools to Operate Tablet Computers for Elderly—A Feasibility Study. Healthcare 2021, 9, 1198. https://doi.org/10.3390/healthcare9091198
Mueller SM, Göttke-Krogmann B, Kortus J, Wiechmann M, Weber M, Mozek S, Mau W, Golla A, Huebner G. SmartCards as Analogous Tools to Operate Tablet Computers for Elderly—A Feasibility Study. Healthcare. 2021; 9(9):1198. https://doi.org/10.3390/healthcare9091198
Chicago/Turabian StyleMueller, Stephanie M., Bettina Göttke-Krogmann, Julia Kortus, Melanie Wiechmann, Michael Weber, Sarina Mozek, Wilfried Mau, Andre Golla, and Gundula Huebner. 2021. "SmartCards as Analogous Tools to Operate Tablet Computers for Elderly—A Feasibility Study" Healthcare 9, no. 9: 1198. https://doi.org/10.3390/healthcare9091198
APA StyleMueller, S. M., Göttke-Krogmann, B., Kortus, J., Wiechmann, M., Weber, M., Mozek, S., Mau, W., Golla, A., & Huebner, G. (2021). SmartCards as Analogous Tools to Operate Tablet Computers for Elderly—A Feasibility Study. Healthcare, 9(9), 1198. https://doi.org/10.3390/healthcare9091198