
Effective Preventive Strategies to Prevent Secondary Transmission of COVID-19 in Hemodialysis Unit: The First Month of Community Outbreak in Taiwan

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Subject Characteristics
2.2. Formation of COVID-19 Joint Rapid Response Team
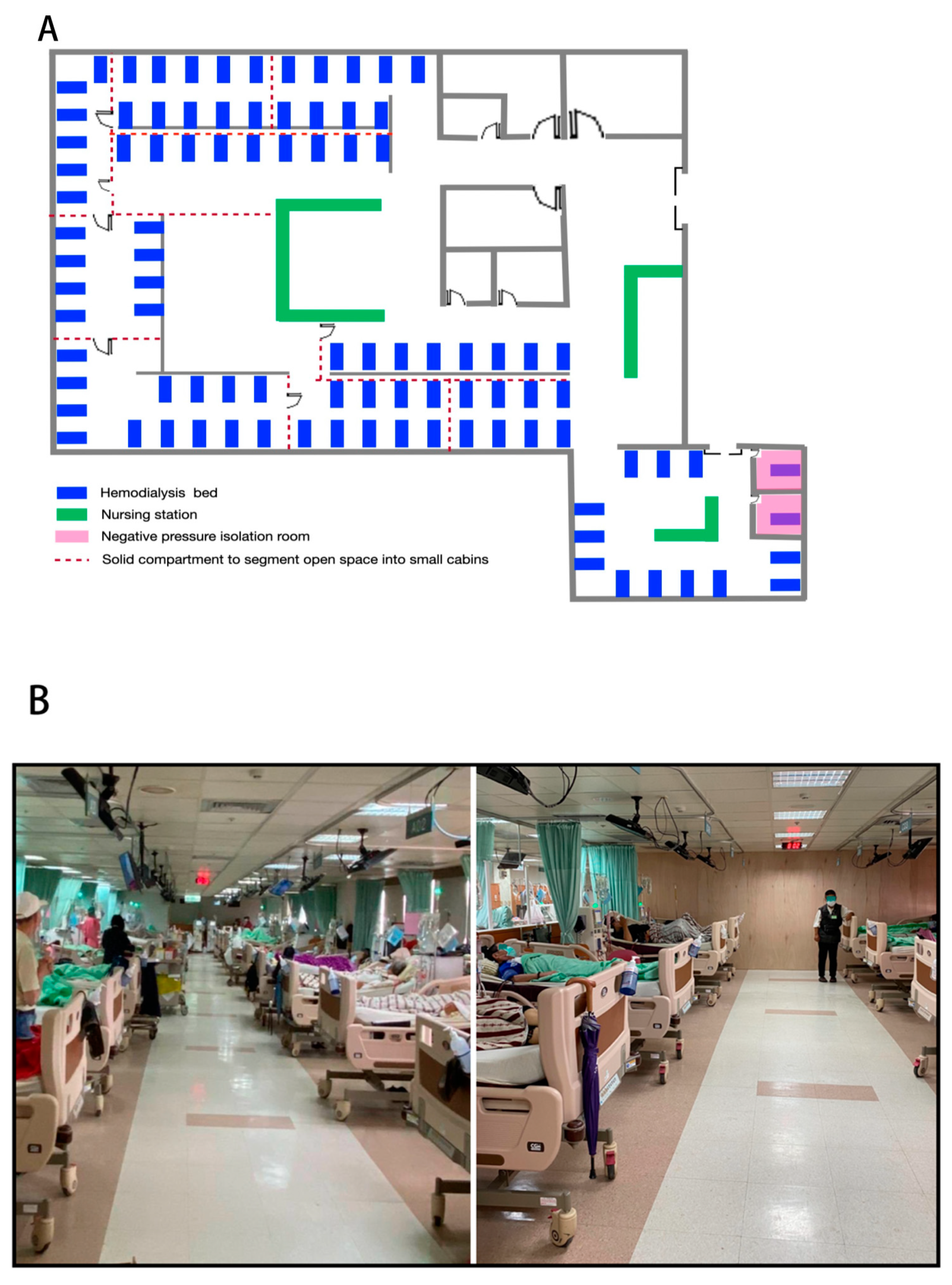
2.3. Specific Preventive Strategies in HD Center of Chang Gung Memorial Hospital at Keelung
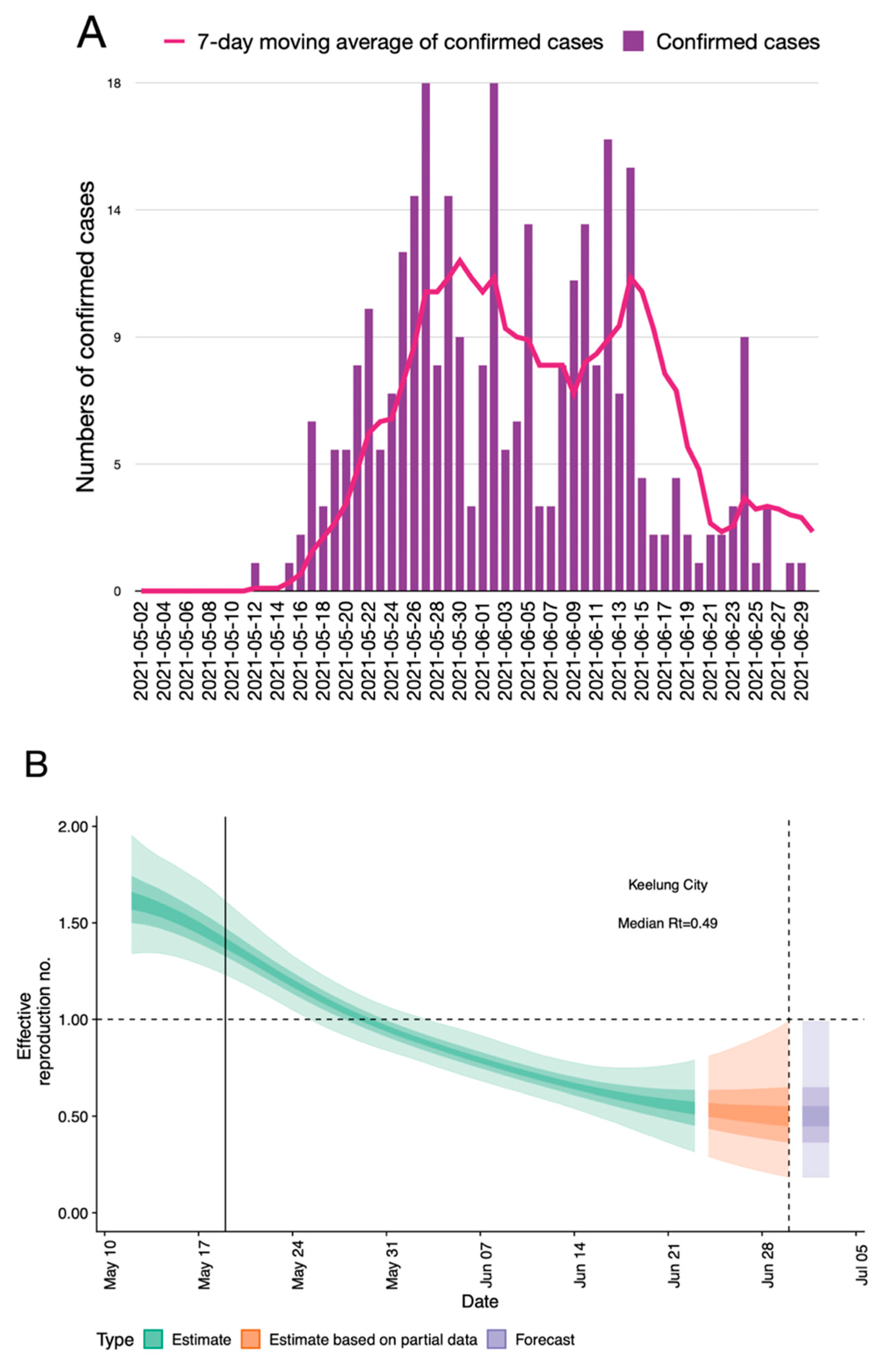
2.4. Adjustment of Preventive Measures According to Reproduction Number (Rt)
2.5. Laboratory Confirmation for SARS-CoV-2 Infection: Rapid Antigen Test and RT-PCR Analysis
2.6. Data Source of Local and National Burden
2.7. Statistical Analyses
3. Results
3.1. Study Subject Characteristics
3.2. An Overview of the Pandemic in Northern Taiwan in the First Month of Outbreak
3.3. Outcomes of Strict Implementation of Specific Preventive Strategies in HD Unit
3.4. Outcomes of COVID-19 Confirmed HD Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 1 August 2021).
- National Center for High-Performance Computing. Daily New Diagnoses in Each County, City and Region. Available online: https://covid-19.nchc.org.tw/city_confirmed.php?mycity (accessed on 1 August 2021).
- Cheng, S.-Y.; Wang, C.J.; Shen, A.C.-T.; Chang, S.-C. How to safely reopen colleges and universities during COVID-19: Experiences from Taiwan. Ann. Intern. Med. 2020, 173, 638–641. [Google Scholar] [CrossRef] [PubMed]
- Cheng, H.-Y.; Jian, S.-W.; Liu, D.-P.; Ng, T.-C.; Huang, W.-T.; Lin, H.-H.; The Taiwan COVID-19 Outbreak Investigation Team. Contact tracing assessment of COVID-19 transmission dynamics in Taiwan and risk at different exposure periods before and after symptom onset. JAMA Intern. Med. 2020, 180, 1156–1163. [Google Scholar] [CrossRef]
- Wang, C.J.; Ng, C.; Brook, R.H. Response to COVID-19 in Taiwan: Big data analytics, new technology, and proactive testing. JAMA 2020, 323, 1341. [Google Scholar] [CrossRef] [PubMed]
- WHO. Weekly Epidemiological Update on COVID-19. Available online: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20210720_weekly_epi_update_49.pdf?sfvrsn=e036283e_4&download=true (accessed on 20 July 2021).
- Davies, N.G.; Jarvis, C.I.; Edmunds, W.J.; Jewell, N.P.; Diaz-Ordaz, K.; Keogh, R.H. Increased mortality in community-tested cases of SARS-CoV-2 lineage B.1.1.7. Nat. Cell Biol. 2021, 593, 270–274. [Google Scholar] [CrossRef]
- Davies, N.G.; Abbott, S.; Barnard, R.C.; Jarvis, C.I.; Kucharski, A.J.; Munday, J.D.; Pearson, C.A.B.; Russell, T.W.; Tully, D.C.; Washburne, A.D.; et al. Estimated transmissibility and impact of SARS-CoV-2 lineage B.1.1.7 in England. Science 2021, 372, eabg3055. [Google Scholar] [CrossRef]
- Taiwan Centers for Disease Control. COVID-19 Statistics of Taiwan. Available online: https://sites.google.com/cdc.gov.tw/2019ncov/taiwan?authuser=0 (accessed on 15 January 2020).
- Chen, C.-Y.; Shao, S.-C.; Chen, Y.-T.; Hsu, C.-K.; Hsu, H.-J.; Lee, C.-C.; Sun, C.-Y.; Chen, Y.-C.; Hung, M.-J.; Wu, I.-W. Incidence and clinical impacts of COVID-19 infection in patients with hemodialysis: Systematic review and meta-analysis of 396,062 hemodialysis patients. Healthcare 2021, 9, 47. [Google Scholar] [CrossRef] [PubMed]
- United States Renal Data System. 2020 USRDS Annual Data Report: Epidemiology of Kidney Disease in the United States; National Institutes of Health: Bethesda, MD, USA; National Institute of Diabetes and Digestive and Kidney Diseases: Bethesda, MD, USA, 2020.
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Rao, K.-S.; Suryaprakash, V.; Senthilkumar, R.; Preethy, S.; Katoh, S.; Ikewaki, N.; Abraham, S.J.K. Role of immune dysregulation in increased mortality among a specific subset of COVID-19 patients and immune-enhancement strategies for combatting through nutritional supplements. Front. Immunol. 2020, 11, 1548. [Google Scholar] [CrossRef]
- Betjes, M.G.H. Immune cell dysfunction and inflammation in end-stage renal disease. Nat. Rev. Nephrol. 2013, 9, 255–265. [Google Scholar] [CrossRef] [PubMed]
- Taiwan Centers of Disease Control. Guidelines on Infection Control Measures for Medical Institutions with Hemodialysis Facilities in Response to COVID-19. Available online: https://www.cdc.gov.tw/File/Get/Cvg5lnAeQ2ySM301hyg6pw (accessed on 1 August 2021).
- Li, Y.-J. Prolong of Level 3 Alert, Recommendations for Medical Responses of Dialysis Facilities in Taiwan. Available online: https://www.tsn.org.tw/tsnFile/authority/F8D926898A85F502/%E5%BB%B6%E9%95%B7%E4%B8%89%E7%B4%9A%E8%AD%A6%E6%88%92%20%E5%85%A8%E5%8F%B0%E9%80%8F%E6%9E%90%E9%99%A2%E6%89%80%E9%86%AB%E7%99%82%E8%B3%87%E6%BA%90%E6%95%B4%E5%82%99%E6%87%89%E8%AE%8A%E5%BB%BA%E8%AD%B0_20210530_%E7%AC%AC%E4%B8%89%E7%89%88.pdf (accessed on 10 August 2021). (In Chinese).
- Lee, J.-J.; Hwang, S.-J.; Huang, J.-F. Review of the present features and the infection control challenges of COVID-19 pandemic in dialysis facilities. Kaohsiung J. Med. Sci. 2020, 36, 393–398. [Google Scholar] [CrossRef]
- Lee, J.-J.; Lin, C.-Y.; Chiu, Y.-W.; Hwang, S.-J. Take proactive measures for the pandemic COVID-19 infection in the dialysis facilities. J. Formos. Med. Assoc. 2020, 119, 895–897. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Emergency Response Team. Specifications of Dialysis Facilities Prevent COVID-19 Management Specifications. Available online: https://www.tsn.org.tw/tsnFile/authority/F8D7DD61F9E8EC28/20200406-%E9%80%8F%E6%9E%90%E9%86%AB%E7%99%82%E9%99%A2%E6%89%80%E5%9B%A0%E6%87%89%E6%AD%A6%E6%BC%A2%E8%82%BA%E7%82%8ECOVID-19%E6%84%9F%E6%9F%93%E8%99%95%E7%BD%AE%E8%A6%8F%E7%AF%84(%E5%85%AC%E5%91%8A%E7%89%88%E7%AC%AC%E4%B8%89%E7%89%88)-TSN.pdf (accessed on 12 August 2021). (In Chinese).
- Inglesby, T.V. Public health measures and the reproduction number of SARS-CoV-2. JAMA 2020, 323, 2186. [Google Scholar] [CrossRef] [PubMed]
- Abbott, S.; Hellewell, J.; Thompson, R.N.; Sherratt, K.; Gibbs, H.P.; Bosse, N.I.; Munday, J.D.; Meakin, S.; Doughty, E.L.; Chun, J.Y.; et al. Estimating the time-varying reproduction number of SARS-CoV-2 using national and subnational case counts [version 1; peer review: Awaiting peer review]. Wellcome Open Res. 2020, 5, 112. [Google Scholar] [CrossRef]
- Rubin, D.; Huang, J.; Fisher, B.T.; Gasparrini, A.; Tam, V.; Song, L.; Wang, X.; Kaufman, J.; Fitzpatrick, K.; Jain, A.; et al. Association of social distancing, population density, and temperature with the instantaneous reproduction number of SARS-CoV-2 in counties across the United States. JAMA Netw. Open 2020, 3, e2016099. [Google Scholar] [CrossRef] [PubMed]
- Pan, A.; Liu, L.; Wang, C.; Guo, H.; Hao, X.; Wang, Q.; Huang, J.; He, N.; Yu, H.; Lin, X.; et al. Association of public health interventions with the epidemiology of the COVID-19 outbreak in Wuhan, China. JAMA 2020, 323, 1915–1923. [Google Scholar] [CrossRef] [Green Version]
- Hsueh, P.R.; Yang, P.C. Severe acute respiratory syndrome epidemic in Taiwan, 2003. J. Microbiol. Immunol. Infect. 2005, 38, 82–88. [Google Scholar]
- Kwan, B.C.-H.; Leung, C.-B.; Szeto, C.-C.; Wong, V.W.-S.; Cheng, Y.-L.; Yu, A.W.-Y.; Li, P.K.-T. Severe acute respiratory syndrome in dialysis patients. J. Am. Soc. Nephrol. 2004, 15, 1883–1888. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Assiri, A.; McGeer, A.; Perl, T.M.; Price, C.S.; Al Rabeeah, A.A.; Cummings, D.A.; Alabdullatif, Z.N.; Assad, M.; Almulhim, A.; Makhdoom, H.; et al. Hospital outbreak of middle east respiratory syndrome coronavirus. N. Engl. J. Med. 2013, 369, 407–416. [Google Scholar] [CrossRef]
- Ahmed, A.E.; Alshukairi, A.N.; Al-Jahdali, H.; Alaqeel, M.; Siddiq, S.S.; Alsaab, H.A.; Sakr, E.A.; Alyahya, H.A.; Alandonisi, M.M.; Subedar, A.T.; et al. Development of a risk-prediction model for Middle East respiratory syndrome coronavirus infection in dialysis patients. Hemodial. Int. 2018, 22, 474–479. [Google Scholar] [CrossRef]
- Albalate, M.; Arribas, P.; Torres, E.; Cintra, M.; Alcázar, R.; Puerta, M.; Ortega, M.; Procaccini, F.; Martin, J.; Jiménez, E.; et al. High prevalence of asymptomatic COVID-19 in haemodialysis: Learning day by day in the first month of the COVID-19 pandemic. Nefrología 2020, 40, 279–286. [Google Scholar] [CrossRef]
- Wang, R.; Liao, C.; He, H.; Hu, C.; Wei, Z.; Hong, Z.; Zhang, C.; Liao, M.; Shui, H. COVID-19 in hemodialysis patients: A report of 5 cases. Am. J. Kidney Dis. 2020, 76, 141–143. [Google Scholar] [CrossRef] [PubMed]
- Corbett, R.W.; Blakey, S.; Nitsch, D.; Loucaidou, M.; McLean, A.; Duncan, N.; Ashby, D.R.; The West London Renal and Transplant Center. Epidemiology of COVID-19 in an Urban Dialysis Center. J. Am. Soc. Nephrol. 2020, 31, 1815–1823. [Google Scholar] [CrossRef] [PubMed]
- Kikuchi, K.; Nangaku, M.; Ryuzaki, M.; Yamakawa, T.; Hanafusa, N.; Sakai, K.; Kanno, Y.; Ando, R.; Shinoda, T.; Nakamoto, H.; et al. COVID-19 of dialysis patients in Japan: Current status and guidance on preventive measures. Ther. Apher. Dial. 2020, 24, 361–365. [Google Scholar] [CrossRef] [PubMed]
- La Milia, V.; Bacchini, G.; Bigi, M.C.; Casartelli, D.; Cavalli, A.; Corti, M.; Crepaldi, M.; Limardo, M.; Longhi, S.; Manzoni, C.; et al. COVID-19 outbreak in a large hemodialysis center in Lombardy, Italy. Kidney Int. Rep. 2020, 5, 1095–1099. [Google Scholar] [CrossRef] [PubMed]
- Cho, J.-H.; Kang, S.H.; Park, H.C.; Kim, D.K.; Lee, S.-H.; Do, J.Y.; Park, J.W.; Kim, S.N.; Kim, M.S.; Jin, K.; et al. Hemodialysis with cohort isolation to prevent secondary transmission during a COVID-19 outbreak in Korea. J. Am. Soc. Nephrol. 2020, 31, 1398–1408. [Google Scholar] [CrossRef]
- Wang, H. Maintenance hemodialysis and COVID-19: Saving lives with caution, care, and courage. Kidney Med. 2020, 2, 365–366. [Google Scholar] [CrossRef]
- Su, K.; Ma, Y.; Wang, Y.; Song, Y.; Lv, X.; Wei, Z.; Shi, M.; Ding, G.; Shen, B.; Wang, H. How we mitigated and contained the COVID-19 outbreak in a hemodialysis center: Lessons and experience. Infect. Control Hosp. Epidemiol. 2020, 41, 1240–1242. [Google Scholar] [CrossRef] [Green Version]
- Alberici, F.; Delbarba, E.; Manenti, C.; Econimo, L.; Valerio, F.; Pola, A.; Maffei, C.; Possenti, S.; Lucca, B.; Cortinovis, R.; et al. A report from the brescia renal COVID task force on the clinical characteristics and short-term outcome of hemodialysis patients with SARS-CoV-2 infection. Kidney Int. 2020, 98, 20–26. [Google Scholar] [CrossRef]
- Akbarialiabad, H.; Kavousi, S.; Ghahramani, A.; Bastani, B.; Ghahramani, N. COVID-19 and maintenance hemodialysis: A systematic scoping review of practice guidelines. BMC Nephrol. 2020, 21, 1–9. [Google Scholar] [CrossRef]
- Valeri, A.M.; Robbins-Juarez, S.Y.; Stevens, J.S.; Ahn, W.; Rao, M.K.; Radhakrishnan, J.; Gharavi, A.G.; Mohan, S.; Husain, S.A. Presentation and outcomes of patients with ESKD and COVID-19. J. Am. Soc. Nephrol. 2020, 31, 1409–1415. [Google Scholar] [CrossRef]
- Hsu, C.M.; Weiner, D.E.; Aweh, G.; Miskulin, D.C.; Manley, H.J.; Stewart, C.; Ladik, V.; Hosford, J.; Lacson, E.C.; Johnson, D.S.; et al. COVID-19 among US dialysis patients: Risk factors and outcomes from a national dialysis provider. Am. J. Kidney Dis. 2021, 77, 748–756. [Google Scholar] [CrossRef] [PubMed]
- Wand, O.; Mor, O.; Zuckerman, N.; Fadeela, A.; Benchetrit, S.; Nacasch, N.; Cohen-Hagai, K. Outcomes from infections with variant strains of SARS-CoV-2 among patients receiving maintenance hemodialysis. Am. J. Kidney Dis. 2021. [Google Scholar] [CrossRef]
- Nyberg, T.; Twohig, K.A.; Harris, R.J.; Seaman, S.R.; Flannagan, J.; Allen, H.; Charlett, A.; De Angelis, D.; Dabrera, G.; Presanis, A.M. Risk of hospital admission for patients with SARS-CoV-2 variant B.1.1.7: Cohort analysis. BMJ 2021, 373, n1412. [Google Scholar] [CrossRef] [PubMed]
- Patone, M.; Thomas, K.; Hatch, R.; Tan, P.S.; Coupland, C.; Liao, W.; Mouncey, P.; Harrison, D.; Rowan, K.; Horby, P.; et al. Mortality and critical care unit admission associated with the SARS-CoV-2 lineage B.1.1.7 in England: An observational cohort study. Lancet Infect. Dis. 2021. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All HD Patients (n = 497) | |
|---|---|
| Male, n (%) | 263 (53) |
| Age, year | 66.03 ± 13.28 |
| White blood cell count (×1000/uL) | 6.62 ± 2.87 |
| Hemoglobin (g/dL) | 10.06 ± 1.25 |
| Platelet (×1000/uL) | 190.47 ± 68.53 |
| Albumin (g/dL) | 4.00 ± 0.48 |
| Aspartate transaminase (IU/L) | 18.49 ± 10.31 |
| Alanine aminotransferase (IU/L) | 17.87 ± 14.74 |
| Alkaline-P (IU/L) | 92 (71–137) * |
| Total bilirubin (mg/dL) | 0.38 ± 0.16 |
| Cholesterol (mg/dL) | 153.76 ± 36.27 |
| Triglyceride (mg/dL) | 151.77 ± 116.22 |
| Creatinine (mg/dL) | 9.40 ± 2.68 |
| Uric acid (mg/dL) | 6.43 ± 1.82 |
| Na (meq/L) | 138.10 ± 3.21 |
| K (meq/L) | 4.70 ± 0.83 |
| Ca (mg/dL) | 9.33 ± 0.90 |
| P (mg/dL) | 5.26 ± 1.55 |
| Kt/V (Daugirdes) | 1.67 ± 0.33 |
| Normalized protein catabolic rate (g/kg/day) | 1.08 ± 0.39 |
| Ferritin (ng/mL) | 496.46 ± 415.14 |
| Transferrin saturation (%) | 33.00 ± 14.51 |
| Intact-parathyroid hormone (pg/mL) | 285 (119, 672) * |
| Cardiac/thoracic ratio | 0.52 ± 0.07 |
| Ca × P product | 49.17 ± 15.67 |
| Districts | Confirmed Cases | Total Population # | Incidence Rate (%) |
|---|---|---|---|
| National | 14,804 | 23,816,775 | 0.062 |
| Taipei City | 4470 | 2,581,006 | 0.173 |
| New Taipei City | 6503 | 4,027,730 | 0.161 |
| Keelung City | 303 | 367,088 | 0.083 |
| Overall HD patients at Keelung | 9 | 1351 | 0.666 |
| CGMH-HDR * | 0 * | 497 | 0.000 |
| Strategies | Contents of Measures |
|---|---|
| Space segmentation | Use of solid compartment to separate the open room into cabins of 8–10 beds, using wood, strengthened glass, and acrylic as materials. Use of acrylic partitions in the nursing station to limit droplet dissemination. Fixed care bundle: fixed patients and caregivers in pre-established bed or seat location cared by a fixed nursing team using fixed clinical carts. Installation of monitoring and loudspeaker system in negative pressure isolation room to limit frequent entries and exits of personnel. |
| Access control | Spacing between exchanges of HD sessions to avoid overlapping of patients at entry and exit of HD room. Double TOCC checking at both entry of hospital (by reading of NHI card) and at the door of HD unit (by personal verbal and written confirmation). Double-checking of clinical symptom and body temperature at both entry of hospital and at the door of HD unit. Double hand alcohol disinfection at both entry of hospital and at door of HD unit. Remove tables and chairs in the waiting area and set up a position mark on the ground of entry with 1.5 m of distancing to avoid clustering. Control of the total number of people in the hospital and in a single elevator. |
| Quarantine operations | Postering and broadcasting (at entry of HD room, in the beginning of every HD session) of our HD preventive measures. Caregiver limitation (do not stay in treatment area, or fixed caregiver if assistance needed) |
| Weekly rapid nasopharyngeal swab SARS-CoV-2 antigen testing for patients and fixed caregivers. Acceptance of new patients into our HD unit is prohibited during an outbreak. Triage algorithm should be followed for emergent cases (see Figure 3). Bedside vaccination program for all HD patients. | |
| Staff protection | All medical and nursing staff wore high-quality PPE, including face shields, goggles, N95 masks, gloves, and waterproof isolation gowns. Staff entering the dialysis room must perform a QR code scan to confirm location and contact tracking. |
| Provide the first dose of COVID-19 vaccine to all of the staff before the end of May. Staff who take care of confirmed patients should receive RT-PCR testing on a weekly basis. |
| Total Patients (n = 8) * | Alive (n = 3) $ | Deceased (n = 5) | p-Value | |
|---|---|---|---|---|
| Male, n (%) | 3 (37.5) | 1 (33.3) | 2 (40) | 0.714 |
| Age, year | 68.9 (60.88–97.00) | 63.1 (60.88–64.30) | 74.9 (61–97) | 0.143 |
| W.B.C. (×1000/uL) | 4.20 (1.00–6.80) | 5.30 (3.30–6.80) | 4.20 (1.00–5.00) | 0.250 |
| Hb (g/dL) | 9.55 (7.60–12.40) | 8.20 (7.60–12.40) | 10.5 (8.4–10.8) | 0.571 |
| Platelet (×1000/uL) | 125 (39–225) | 155 (76–173) | 103 (39–225) | 0.571 |
| Albumin (gm/dL) | 3.66 (3.06–4.15) | 3.76 (3.27–3.91) | 3.56 (3.06–4.15) | 1.000 |
| AST (IU/L) | 25 (16–67) | 26 (16–61) | 24 (20–67) | 1.000 |
| ALT (IU/L) | 17 (9–34) | 31 (17–34) | 12.5 (9–18) | 0.114 |
| Alkaline-P (IU/L) | 110 (48–154) | 128 (48–154) | 110 (69–110) | 0.700 |
| Total Bilirubin (mg/dL) | 0.35 (0.3–0.6) | 0.3 (0.3–0.4) | 0.4 (0.3–0.6) | 0.393 |
| Cardiac/thoracic ratio | 0.59 (0.48–0.65) | 0.55 (0.48–0.57) | 0.61 (0.58–0.65) | 0.036 * |
| Creatinine (mg/dL) | 9.04 (4.00–15.18) | 9.04 (6.39–11.74) | 7.45 (4–15.18) | 0.857 |
| Na (meq/L) | 137.5 (121–141) | 138 (137–139) | 135 (121–141) | 0.393 |
| K (meq/L) | 3.70 (3.2–6.9) | 4.60 (3.20–5.70) | 3.70 (3.4–6.90) | 1.000 |
| Ca (mg/dL) | 8.90 (8.50–11.10) | 9.95 (8.8–11.10) | 8.9 (8.5–10.0) | 0.571 |
| P (mg/dL) | 5.00 (2.00–9.90) | 4.40 (2.8–6.0) | 5.0 (2.0–9.9) | 1.000 |
| Ferritin (ng/mL) | 869.5 (41.9–6954.0) | 877.0 (41.9–1100.0) | 862.0 (82.3–6954.0) | 0.786 |
| Ca × P product | 38.54 (20–88.11) | NA (31.08–52.80) | 46.00 (20.00–88.11) | 0.571 |
| Ct value | 17.50 (11.75–27.10) | 17.53 (11.75–27.10) | 17.47 (16.75–18.57) | 1.000 |
| CRP (mg/L) | 36.62 (15.17–70.79) | 17.2 (15.17–35.70) | 52.81 (20.60–70.79) | 0.071 |
| LDH (U/L) | 249 (185–355) | 249 (185–355) | 243.5 (219.0–290.0) | 1.000 |
| Lactate (mg/dL) | 46.35 (7.80–116.60) | 11.05 (7.80–14.30) | 97.5 (78.40–116.60) | 0.333 |
| Procalcitonin (ng/mL) | 0.535 (0.16–1.75) | 0.51 (0.16–0.56) | 0.56 (0.48–1.75) | 0.393 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, C.-Y.; Ye, J.-J.; Huang, T.-S.; Lee, C.-C.; Chen, Y.-T.; Hsu, C.-K.; Hsu, H.-J.; Sun, C.-Y.; Pan, H.-C.; Chen, K.-S.; et al. Effective Preventive Strategies to Prevent Secondary Transmission of COVID-19 in Hemodialysis Unit: The First Month of Community Outbreak in Taiwan. Healthcare 2021, 9, 1173. https://doi.org/10.3390/healthcare9091173
Chen C-Y, Ye J-J, Huang T-S, Lee C-C, Chen Y-T, Hsu C-K, Hsu H-J, Sun C-Y, Pan H-C, Chen K-S, et al. Effective Preventive Strategies to Prevent Secondary Transmission of COVID-19 in Hemodialysis Unit: The First Month of Community Outbreak in Taiwan. Healthcare. 2021; 9(9):1173. https://doi.org/10.3390/healthcare9091173
Chicago/Turabian StyleChen, Chun-Yu, Jung-Jr Ye, Ting-Shuo Huang, Chin-Chan Lee, Yih-Ting Chen, Cheng-Kai Hsu, Heng-Jung Hsu, Chiao-Yin Sun, Heng-Chih Pan, Kuo-Su Chen, and et al. 2021. "Effective Preventive Strategies to Prevent Secondary Transmission of COVID-19 in Hemodialysis Unit: The First Month of Community Outbreak in Taiwan" Healthcare 9, no. 9: 1173. https://doi.org/10.3390/healthcare9091173
APA StyleChen, C.-Y., Ye, J.-J., Huang, T.-S., Lee, C.-C., Chen, Y.-T., Hsu, C.-K., Hsu, H.-J., Sun, C.-Y., Pan, H.-C., Chen, K.-S., Kao, H.-H., Ko, C.-C., She, Y.-H., Wu, C.-Y., Lai, C.-C., Hwang, S.-J., & Wu, I.-W. (2021). Effective Preventive Strategies to Prevent Secondary Transmission of COVID-19 in Hemodialysis Unit: The First Month of Community Outbreak in Taiwan. Healthcare, 9(9), 1173. https://doi.org/10.3390/healthcare9091173