
Photobiomodulation Therapy vs. Corticosteroid for the Management of Erosive/Ulcerative and Painful Oral Lichen Planus. Assessment of Success Rate during One-Year Follow-Up: A Retrospective Study

 ,
,  ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Inclusion and Exclusion Criteria
Exclusion criteria were as follows:
- Pregnant or breastfeeding woman;
- Patients who were having any other treatment for OLP;
- Patients who had used anti-inflammatory drugs (topic or systemic) in the last 30 days;
- Patients who reported drug-related development of oral lichenoid lesions, including imatinib, methyldopa, IFN-alpha and/or infliximab;
- Patients with an uncontrolled systemic disease;
- OLP with epithelial dysplasia or malignant transformation in the histopathological evaluation.
2.4. Treatment of Oral Lichen Planus by Topical Medication
2.5. Photobiomodulation Therapy (PBM Group)
2.6. Assessment Method: Pain and Patients’ Discomfort
2.7. Assessment of the Recurrence
2.8. Statistical Analysis
3. Results
3.1. Pain Assessment
3.2. REU Score
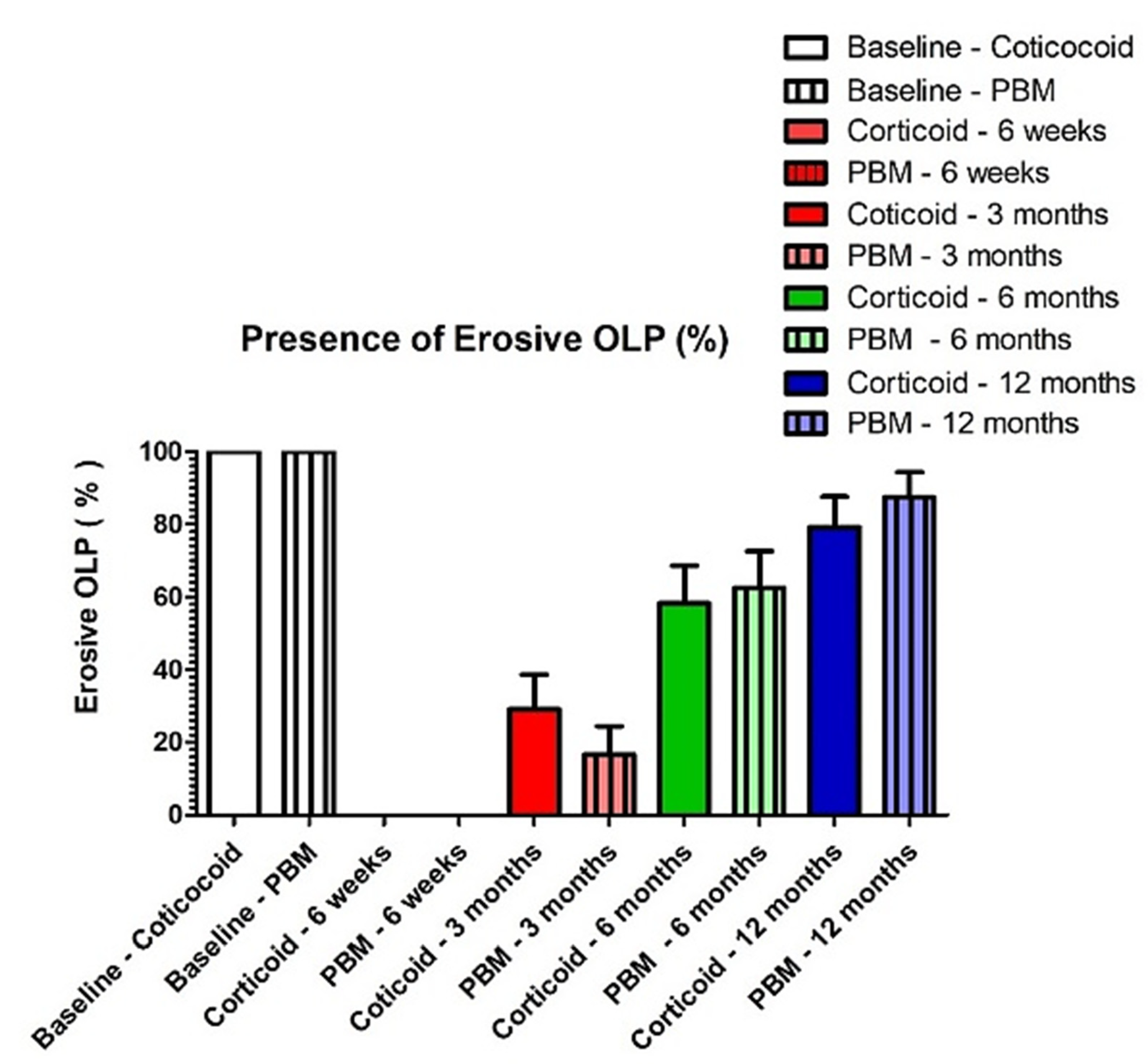
3.3. Recurrence Rate
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Kemper, K.J. “Let There Be Light.” Research on Phototherapy, Light Therapy, and Photobiomodulation for Healing—Alternative Therapy Becomes Mainstream. Complementary Ther. Med. 2018, 41, A1–A6. [Google Scholar] [CrossRef] [PubMed]
- Cronshaw, M.; Parker, S.; Anagnostaki, E.; Mylona, V.; Lynch, E.; Grootveld, M. Photobiomodulation and Oral Mucositis: A Systematic Review. Dent. J. 2020, 8, 87. [Google Scholar] [CrossRef]
- El Mobadder, M.; Farhat, F.; Nammour, S. Photobiomodulation Therapy in the Treatment of Chronic Dysphagia Post Hormonal Therapy in a Breast Cancer Patient. Dent. J. 2019, 7, 53. [Google Scholar] [CrossRef] [Green Version]
- Zecha, J.A.; Raber-Durlacher, J.E.; Nair, R.G.; Epstein, J.B.; Sonis, S.T.; Elad, S.; Hamblin, M.R.; Barasch, A.; Migliorati, C.A.; Milstein, D.M.; et al. Low level laser therapy/photobiomodulation in the management of side effects of chemoradiation therapy in head and neck cancer: Part 1: Mechanisms of action, dosimetric, and safety considerations. Supportive Care Cancer 2016, 6, 2781–2792. [Google Scholar] [CrossRef] [Green Version]
- Olson, M.A.; Rogers, R.S.; Bruce, A.J. Oral Lichen Planus. Clin. Dermatol. 2016, 34, 495–504. [Google Scholar] [CrossRef] [PubMed]
- Alrashdan, M.S.; Cirillo, N.; McCullough, M. Oral Lichen Planus: A Literature Review and Update. Arch. Derm. Res. 2016, 308, 539–551. [Google Scholar] [CrossRef] [PubMed]
- Bennardo, F.; Liborio, F.; Barone, S.; Antonelli, A.; Buffone, C.; Fortunato, L.; Giudice, A. Efficacy of platelet-rich fibrin compared with triamcinolone acetonide as injective therapy in the treatment of symptomatic oral lichen planus: A pilot study. Clin. Oral Investig. 2021, 25, 3747–3755. [Google Scholar] [CrossRef]
- González-Moles, M.Á.; Warnakulasuriya, S.; González-Ruiz, I.; González-Ruiz, L.; Ayén, Á.; Lenouvel, D.; Ruiz-Ávila, I.; Ramos-García, P. Worldwide Prevalence of Oral Lichen Planus: A Systematic Review and Meta-analysis. Oral Dis. 2021, 27, 813–828. [Google Scholar] [CrossRef] [PubMed]
- Silverman, S. Oral lichen planus: A potentially premalignant lesion. J. Oral Maxillofac. Surg. 2000, 58, 1286–1288. [Google Scholar] [CrossRef] [PubMed]
- Zecha, J.A.; Raber-Durlacher, J.E.; Nair, R.G.; Epstein, J.B.; Elad, S.; Hamblin, M.R.; Barasch, A.; Migliorati, C.A.; Milstein, D.M.; Genot, M.T.; et al. Low-level laser therapy/photobiomodulation in the management of side effects of chemoradiation therapy in head and neck cancer: Part 2: Proposed applications and treatment protocols. Supportive Care Cancer 2016, 6, 2793–2805. [Google Scholar] [CrossRef] [Green Version]
- El Mobadder, M.; Farhat, F.; El Mobadder, W.; Nammour, S. Photobiomodulation Therapy in the Treatment of Oral Mucositis, Dysgeusia and Oral Dryness as Side-Effects of Head and Neck Radiotherapy in a Cancer Patient: A Case Report. Dent. J. 2018, 4, 64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, B.; Fan, J.; Wang, L.; Chai, L. Photobiomodulation Therapy/Photodynamic Therapy Versus Steroid Therapy for Oral Lichen Planus: A Systematic Review and Meta-Analysis. Photobiomodulation Photomed. Laser Surg. 2021, 39, 145–154. [Google Scholar] [CrossRef] [PubMed]
- Piboonniyom, S.O.; Treister, N.; Pitiphat, W.; Woo, S.B. Scoring system for monitoring oral lichenoid lesions: A preliminary study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2005, 99, 696–703. [Google Scholar] [CrossRef] [PubMed]
- Thongprasom, K.; Dhanuthai, K. Steriods in the treatment of lichen planus: A review. J. Oral Sci. 2008, 50, 377–385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takeda, K.; Arase, S.; Takahashi, S. Side effects of topical corticosteroids and their prevention. Drugs 1988, 36, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Mehta, A.B.; Nadkarni, N.J.; Patil, S.P.; Godse, K.V.; Gautam, M.; Agarwal, S. Topical corticosteroids in dermatology. Indian J. Dermatol. Venereol. Leprol. 2016, 82, 371–378. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, J.G.F.; Dos Santos, S.S.; de Almeida, P.; Marcos, R.L.; Lino-Dos-Santos-Franco, A. Effect of systemic photobiomodulation in the course of acute lung injury in rats. Lasers Med. Sci. 2021, 36, 965–973. [Google Scholar] [CrossRef]
- Kalhori, K.A.M.; Vahdatinia, F.; Jamalpour, M.R.; Vescovi, P.; Fornaini, C.; Merigo, E.; Fekrazad, R. Photobiomodulation in Oral Medicine. Photobiomodul. Photomed. Laser Surg. 2019, 37, 837–861. [Google Scholar] [CrossRef] [PubMed]
- Flores Luna, G.L.; de Andrade, A.L.M.; Brassolatti, P.; Bossini, P.S.; Anibal, F.F.; Parizotto, N.A.; Leal, Â.M.O. Biphasic Dose/Response of Photobiomodulation Therapy on Culture of Human Fibroblasts. Photobiomodul. Photomed. Laser Surg. 2020, 38, 413–418. [Google Scholar] [CrossRef] [PubMed]
- Dompe, C.; Moncrieff, L.; Matys, J.; Grzech-Leśniak, K.; Kocherova, I.; Bryja, A.; Bruska, M.; Dominiak, M.; Mozdziak, P.; Skiba, T.H.; et al. Photobiomodulation—Underlying Mechanism and Clinical Applications. J. Clin. Med. 2020, 9, 1724. [Google Scholar] [CrossRef] [PubMed]
- Muili, K.A.; Gopalakrishnan, S.; Meyer, S.L.; Eells, J.T.; Lyons, J.A. Amelioration of experimental autoimmune encephalomyelitis in C57BL/6 mice by photobiomodulation induced by 670 nm light. PLoS ONE 2012, 7, e30655. [Google Scholar] [CrossRef] [Green Version]
- Ailioaie, L.M.; Litscher, G. Molecular and Cellular Mechanisms of Arthritis in Children and Adults: New Perspectives on Applied Photobiomodulation. Int. J. Mol. Sci. 2020, 21, 6565. [Google Scholar] [CrossRef]
- Ferri, E.P.; Cunha, K.R.; Abboud, C.S.; de Barros Gallo, C.; de Sousa Sobral, S.; de Fatima Teixeira da Silva, D.; Horliana, A.C.R.; Franco, A.L.D.S.; Rodrigues, M.F.S.D. Photobiomodulation is effective in oral lichen planus: A randomized, controlled, double-blind study. Oral Dis. 2021, 27, 1205–1216. [Google Scholar] [CrossRef]
- Gambino, A.; Cabras, M.; Cafaro, A.; Broccoletti, R.; Carossa, S.; Hopper, C.; Conrotto, D.; Porter, S.R.; Arduino, P.G. Preliminary evaluation of the utility of optical coherence tomography in detecting structural changes during photobiomodulation treatment in patients with atrophic-erosive oral lichen planus. Photodiagnosis Photodyn. Ther. 2021, 34, 102255. [Google Scholar] [CrossRef]
- He, Y.; Deng, J.; Zhao, Y.; Tao, H.; Dan, H.; Xu, H.; Chen, Q. Efficacy evaluation of photodynamic therapy for oral lichen planus: A systematic review and meta-analysis. BMC Oral Health 2020, 20, 302. [Google Scholar] [CrossRef]
- Kwiatkowski, S.; Knap, B.; Przystupski, D.; Saczko, J.; Kędzierska, E.; Knap-Czop, K.; Kotlińska, J.; Michel, O.; Kotowski, K.; Kulbacka, J. Photodynamic therapy—Mechanisms, photosensitizers and combinations. Biomed Pharmacother. 2018, 106, 1098–1107. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total Participants | Gender | Mean Age Range (Years) | Average Size of OLP (cm2) | |
|---|---|---|---|---|
| 96 | Female | Male | 48 (min 42; max 68) | 2.2 (min 1.5; max 3.4) |
| 64 | 32 | |||
| Clinical Signs | Score of Signs |
|---|---|
| Reticulate/plaque-type (R) | 0 = none |
| 1 = white streaks or patches | |
| Congestive/atrophic (E) | 0 = none |
| 1 = lesions < 100 mm2 | |
| 2 = lesions 100 mm2 to 300 mm2 | |
| 3 = lesions > 300 mm2 | |
| Ulceration (U) | 0 = none |
| 1 = lesions < 100 mm2 | |
| 2 = 100 mm2 to 200 mm2 | |
| 3 = lesions > 300 mm2 |
| Before Treatment | At 6 Weeks of Follow-up | |
|---|---|---|
| Corticosteroid group | 80.65 ± 4.1 a | 0 b |
| PBM group | 83.54 ± 3.7 a | 0 b |
| REU Score | ||
|---|---|---|
| Before Treatment | After 6 Weeks of Treatment | |
| Corticosteroid group | R = 1 E = 2 U = 1 | R = 1 E = 0 U = 0 |
| Overall score 4 a | Overall score 1 b | |
| PBM group | R = 1 E = 2 U = 1 | R = 1 E = 0 U = 0 |
| Overall score 4 a | Overall score 1 b | |
| 6 Weeks | 3 Months | 6 Months | 12 Months | |
|---|---|---|---|---|
| Corticosteroid group (n = 48) | 0% a | 29% b (14 of 48) | 58% c (28 of 48) | 79 % d (38 of 48) |
| Photobiomodulation group (n = 48) | 0% a | 21 % b (10 of 48) | 62 % c (30 of 48) | 87.5 % d (42 of 48) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nammour, S.; El Mobadder, M.; Brugnera, A.J.; Namour, M.; Houeis, S.; Heysselaer, D.; Vanheusden, A.; Namour, A. Photobiomodulation Therapy vs. Corticosteroid for the Management of Erosive/Ulcerative and Painful Oral Lichen Planus. Assessment of Success Rate during One-Year Follow-Up: A Retrospective Study. Healthcare 2021, 9, 1137. https://doi.org/10.3390/healthcare9091137
Nammour S, El Mobadder M, Brugnera AJ, Namour M, Houeis S, Heysselaer D, Vanheusden A, Namour A. Photobiomodulation Therapy vs. Corticosteroid for the Management of Erosive/Ulcerative and Painful Oral Lichen Planus. Assessment of Success Rate during One-Year Follow-Up: A Retrospective Study. Healthcare. 2021; 9(9):1137. https://doi.org/10.3390/healthcare9091137
Chicago/Turabian StyleNammour, Samir, Marwan El Mobadder, Aldo Jr. Brugnera, Melanie Namour, Saad Houeis, Daniel Heysselaer, Alain Vanheusden, and Amaury Namour. 2021. "Photobiomodulation Therapy vs. Corticosteroid for the Management of Erosive/Ulcerative and Painful Oral Lichen Planus. Assessment of Success Rate during One-Year Follow-Up: A Retrospective Study" Healthcare 9, no. 9: 1137. https://doi.org/10.3390/healthcare9091137
APA StyleNammour, S., El Mobadder, M., Brugnera, A. J., Namour, M., Houeis, S., Heysselaer, D., Vanheusden, A., & Namour, A. (2021). Photobiomodulation Therapy vs. Corticosteroid for the Management of Erosive/Ulcerative and Painful Oral Lichen Planus. Assessment of Success Rate during One-Year Follow-Up: A Retrospective Study. Healthcare, 9(9), 1137. https://doi.org/10.3390/healthcare9091137