
Comparison of Intaglio Surface Trueness of Interim Dental Crowns Fabricated with SLA 3D Printing, DLP 3D Printing, and Milling Technologies




Abstract
1. Introduction
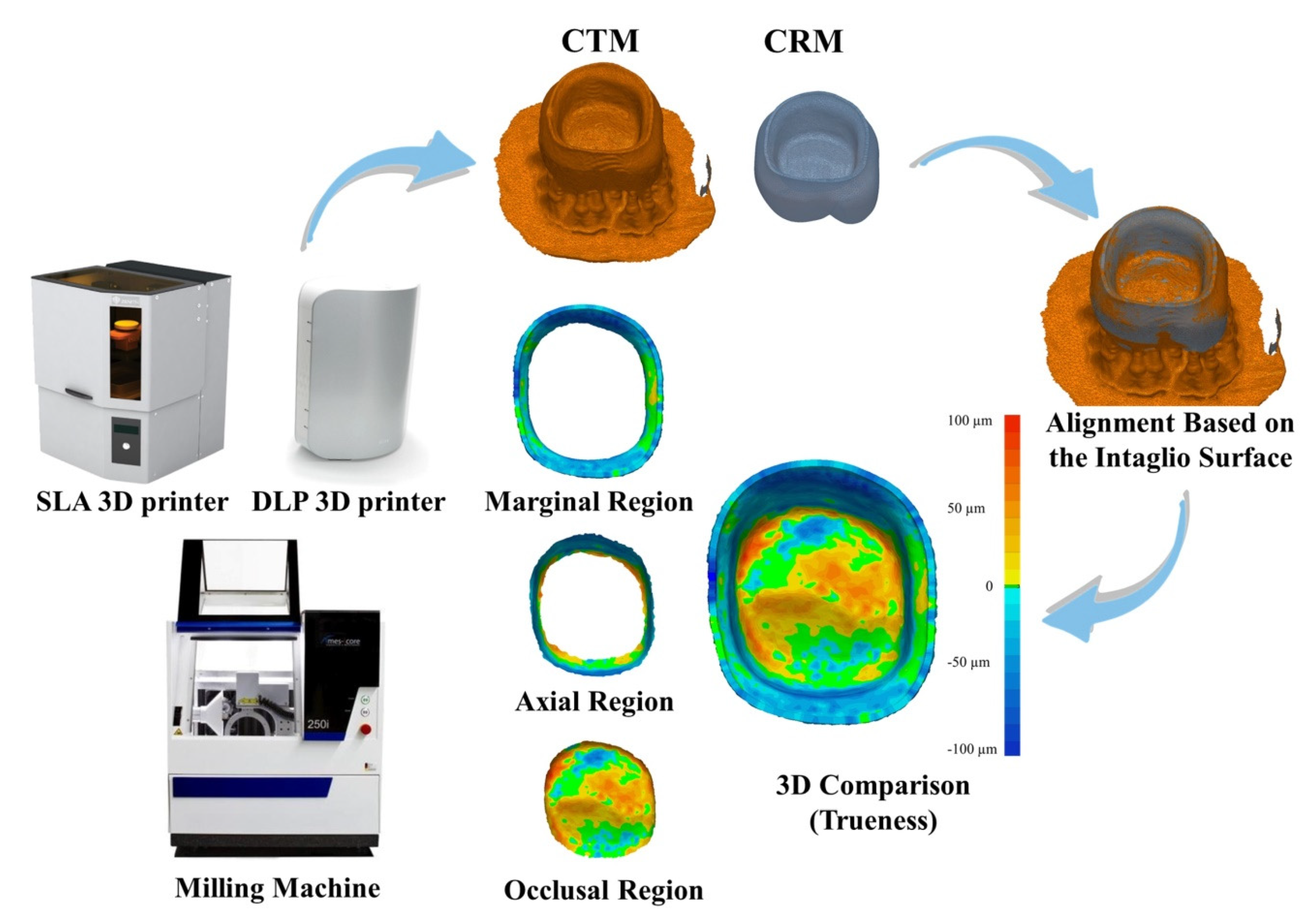
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kale, E.; Cilli, M.; Özçelik, T.B.; Yilmaz, B. Marginal fit of CAD-CAM monolithic zirconia crowns fabricated by using cone beam computed tomography scans. J. Prosthet. Dent. 2020, 123, 731–737. [Google Scholar] [CrossRef] [PubMed]
- Son, K.; Lee, K.B. Effect of finish line locations of tooth preparation on the accuracy of intraoral scanners. Int. J. Comput. Dent. 2021, 24, 29–40. [Google Scholar]
- Angwarawong, T.; Reeponmaha, T.; Angwaravong, O. Influence of thermomechanical aging on marginal gap of CAD-CAM and conventional interim restorations. J. Prosthet. Dent. 2020, 124, 566.e1–566.e6. [Google Scholar] [CrossRef] [PubMed]
- Ahn, J.J.; Bae, E.B.; Lee, J.J.; Choi, J.W.; Jeon, Y.C.; Jeong, C.M.; Huh, J.B. Clinical evaluation of the fit of lithium disilicate crowns fabricated with three different CAD-CAM systems. J. Prosthet. Dent. 2020, in press. [Google Scholar] [CrossRef] [PubMed]
- Baba, N.Z.; Goodacre, B.J.; Goodacre, C.J.; Müller, F.; Wagner, S. CAD/CAM complete denture systems and physical properties: A review of the literature. J. Prosthodont. 2021, 30, 113–124. [Google Scholar] [CrossRef] [PubMed]
- Kirsch, C.; Ender, A.; Attin, T.; Mehl, A. Trueness of four different milling procedures used in dental CAD/CAM systems. Clin. Oral Investig. 2017, 21, 551–558. [Google Scholar] [CrossRef]
- Son, K.; Yu, B.Y.; Yoon, T.H.; Lee, K.B. Comparative study of the trueness of the inner surface of crowns fabricated from three types of lithium disilicate blocks. Appl. Sci. 2019, 9, 1798. [Google Scholar] [CrossRef]
- Lee, J.J.; Son, K.; Bae, E.B.; Choi, J.W.; Lee, K.B.; Huh, J.B. Comparison of the trueness of lithium disilicate crowns fabricated from all-in-one and combination CAD/CAM systems. Int. J. Prosthodont. 2019, 32, 352–354. [Google Scholar] [CrossRef]
- Taha, D.; Nour, M.; Zohdy, M.; El-Etreby, A.; Hamdy, A.; Salah, T. The effect of different wax pattern fabrication techniques on the marginal fit of customized lithium disilicate implant abutments. J. Prosthodont. 2019, 28, 1018–1023. [Google Scholar] [CrossRef]
- Kim, M.K.; Son, K.; Yu, B.Y.; Lee, K.B. Effect of the volumetric dimensions of a complete arch on the accuracy of scanners. J. Adv. Prosthodont. 2020, 12, 361–368. [Google Scholar] [CrossRef] [PubMed]
- Martínez, S.; Cuesta, E.; Barreiro, J.; Álvarez, B. Analysis of laser scanning and strategies for dimensional and geometrical control. J. Adv. Manuf. Technol. 2010, 46, 621–629. [Google Scholar] [CrossRef]
- Choi, Y.K.; Banerjee, A. Tool path generation and tolerance analysis for free-form surfaces. Int. J. Mach. Tools Manuf. 2007, 47, 689–696. [Google Scholar] [CrossRef]
- Xiao, Z.; Yang, Y.; Xiao, R.; Bai, Y.; Song, C.; Wang, D. Evaluation of topology-optimized lattice structures manufactured via selective laser melting. Mater. Des. 2018, 143, 27–37. [Google Scholar] [CrossRef]
- Bosch, G.; Ender, A.; Mehl, A. A 3-dimensional accuracy analysis of chairside CAD/CAM milling processes. J. Prosthet. Dent. 2014, 112, 1425–1431. [Google Scholar] [CrossRef] [PubMed]
- Jeong, Y.G.; Lee, W.S.; Lee, K.B. Accuracy evaluation of dental models manufactured by CAD/CAM milling method and 3D printing method. J. Adv. Prosthodont. 2018, 10, 245–251. [Google Scholar] [CrossRef]
- Park, H.N.; Lim, Y.J.; Yi, W.J.; Han, J.S.; Lee, S.P. A comparison of the accuracy of intraoral scanners using an intraoral environment simulator. J. Adv. Prosthodont. 2018, 10, 58–64. [Google Scholar] [CrossRef]
- Tan, F.B.; Wang, C.; Dai, H.W.; Fan, Y.B.; Song, J.L. Accuracy and reproducibility of 3D digital tooth preparations made by gypsum materials of various colors. J. Adv. Prosthodont. 2018, 10, 8–17. [Google Scholar] [CrossRef] [PubMed]
- Wong, K.Y.; Esguerra, R.J.; Chia, V.A.P.; Tan, Y.H.; Tan, K.B.C. Three-dimensional accuracy of digital static interocclusal registration by three intraoral scanner systems. J. Prosthodont. 2018, 27, 120–128. [Google Scholar] [CrossRef]
- Motel, C.; Kirchner, E.; Adler, W.; Wichmann, M.; Matta, R.E. Impact of different scan bodies and scan strategies on the accuracy of digital implant impressions assessed with an intraoral scanner: An in vitro study. J. Prosthodont. 2020, 29, 309–314. [Google Scholar] [CrossRef]
- Fluegge, T.; Att, W.; Metzger, M.; Nelson, K. A novel method to evaluate precision of optical implant impressions with commercial scan bodies—An experimental approach. J. Prosthodont. 2017, 26, 34–41. [Google Scholar] [CrossRef]
- Zarone, F.; Ruggiero, G.; Ferrari, M.; Mangano, F.; Joda, T.; Sorrentino, R. Accuracy of a chairside intraoral scanner compared with a laboratory scanner for the completely edentulous maxilla: An in vitro 3-dimensional comparative analysis. J. Prosthet. Dent. 2020, 124, 761.e1–761.e7. [Google Scholar] [CrossRef] [PubMed]
- Mejía, J.B.C.; Wakabayashi, K.; Nakamura, T.; Yatani, H. Influence of abutment tooth geometry on the accuracy of conventional and digital methods of obtaining dental impressions. J. Prosthet. Dent. 2017, 118, 392–399. [Google Scholar] [CrossRef]
- Jeong, I.D.; Kim, W.C.; Park, J.; Kim, C.M.; Kim, J.H. Ceramic molar crown reproducibility by digital workflow manufacturing: An in vitro study. J. Adv. Prosthodont. 2017, 9, 252–256. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Revilla-León, M.; Subramanian, S.G.; Özcan, M.; Krishnamurthy, V.R. Clinical study of the influence of ambient light scanning conditions on the accuracy (trueness and precision) of an intraoral scanner. J. Prosthodont. 2020, 29, 107–113. [Google Scholar] [CrossRef]
- Wang, W.; Yu, H.; Liu, Y.; Jiang, X.; Gao, B. Trueness analysis of zirconia crowns fabricated with 3-dimensional printing. J. Prosthet. Dent. 2019, 121, 285–291. [Google Scholar] [CrossRef]
- Li, R.; Chen, H.; Wang, Y.; Zhou, Y.; Shen, Z.; Sun, Y. Three-dimensional trueness and margin quality of monolithic zirconia restorations fabricated by additive 3D gel deposition. J. Prosthodont. Res. 2020, 64, 478–484. [Google Scholar] [CrossRef]
- Yu, B.Y.; Son, K.; Lee, K.B. Evaluation of intaglio surface trueness and margin quality of interim crowns in accordance with the build angle of stereolithography apparatus 3-dimensional printing. J. Prosthet. Dent. 2020, in press. [Google Scholar] [CrossRef]
- Lee, B.I.; You, S.G.; You, S.M.; Kang, S.Y.; Kim, J.H. Effect of rinsing time on the accuracy of interim crowns fabricated by digital light processing: An in vitro study. J. Adv. Prosthodont. 2021, 13, 24–35. [Google Scholar] [CrossRef]
- Srinivasan, M.; Cantin, Y.; Mehl, A.; Gjengedal, H.; Müller, F.; Schimmel, M. CAD/CAM milled removable complete dentures: An in vitro evaluation of trueness. Clin. Oral Investig. 2017, 21, 2007–2019. [Google Scholar] [CrossRef] [PubMed]
- Kalberer, N.; Mehl, A.; Schimmel, M.; Müller, F.; Srinivasan, M. CAD-CAM milled versus rapidly prototyped (3D-printed) complete dentures: An in vitro evaluation of trueness. J. Prosthet. Dent. 2019, 121, 637–643. [Google Scholar] [CrossRef]
- Jang, D.; Son, K.; Lee, K.B. A Comparative study of the fitness and trueness of a three-unit fixed dental prosthesis fabricated using two digital workflows. Appl. Sci. 2019, 9, 2778. [Google Scholar] [CrossRef]
- Ender, A.; Attin, T.; Mehl, A. In vivo precision of conventional and digital methods of obtaining complete-arch dental impressions. J. Prosthet. Dent. 2016, 115, 313–320. [Google Scholar] [CrossRef]
- Fukazawa, S.; Odaira, C.; Kondo, H. Investigation of accuracy and reproducibility of abutment position by intraoral scanners. J. Prosthodont. Res. 2017, 61, 450–459. [Google Scholar] [CrossRef] [PubMed]
- Methani, M.M.; Revilla-León, M.; Zandinejad, A. The potential of additive manufacturing technologies and their processing parameters for the fabrication of all-ceramic crowns: A review. J. Esthet. Dent. 2020, 32, 182–192. [Google Scholar] [CrossRef]
- Quan, H.; Zhang, T.; Xu, H.; Luo, S.; Nie, J.; Zhu, X. Photo-curing 3D printing technique and its challenges. Bioact. Mater. 2020, 5, 110–115. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Goyanes, A.; Gaisford, S.; Basit, A.W. Stereolithographic (SLA) 3D printing of oral modified-release dosage forms. Int. J. Pharm. 2016, 503, 207–212. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.; Zhao, L.; Jian, M.; Mao, Y.; Yu, M.; Guo, X. EHMP-DLP: Multi-projector DLP with energy homogenization for large-size 3D printing. Rapid Prototyp. J. 2018, 24, 1500–1510. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Evaluated Region | Manufacturing | Mean | SD | 95% Confidence Interval (CI) | Minimum | Maximum | F | p | |
|---|---|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||||
| Whole region | SLA | 25.7 A | 5.1 | 22.8 | 28.6 | 18 | 34.2 | 66.684 | <0.001 * |
| DLP | 29.5 A | 3.3 | 27.6 | 31.3 | 24.4 | 36.8 | |||
| Milling | 44.8 B | 5.5 | 41.7 | 47.9 | 33 | 53.2 | |||
| Marginal region | SLA | 26.7 A | 4.4 | 24.2 | 29.2 | 20.2 | 34 | 45.267 | <0.001 * |
| DLP | 27.0 A | 4.7 | 24.3 | 29.6 | 20.4 | 37.3 | |||
| Milling | 45.2 B | 8.2 | 40.6 | 49.8 | 35.8 | 59.4 | |||
| Axial region | SLA | 27.6 A | 6.5 | 24 | 31.3 | 17.6 | 40.9 | 47.674 | <0.001 * |
| DLP | 30.9 A | 5.6 | 27.8 | 34 | 23.6 | 40.6 | |||
| Milling | 50.5 B | 8.3 | 45.9 | 55.2 | 34 | 63.1 | |||
| Occlusal region | SLA | 23.6 A | 5.3 | 20.6 | 26.5 | 17 | 33.4 | 32.288 | <0.001 * |
| DLP | 29.0 B | 3.6 | 26.9 | 31 | 24.3 | 35.5 | |||
| Milling | 36.9 C | 4.4 | 34.4 | 39.3 | 29.1 | 45.5 | |||
| Evaluated Region | SLA | DLP | Milling |
|---|---|---|---|
| Whole region | 25.7 ± 5.1 | 29.5 ± 3.3 | 44.8 ± 5.5 A |
| Marginal region | 26.7 ± 4.4 | 27.0 ± 4.4 | 45.2 ± 8.2 A |
| Axial region | 27.6 ± 6.5 | 30.9 ± 5.6 | 50.5 ± 8.3 A |
| Occlusal region | 23.6 ± 5.3 | 29.0 ± 3.6 | 36.9 ± 4.4 B |
| F | 1.52 | 2.016 | 10.025 |
| p | 0.219 | 0.122 | <0.001 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Son, K.; Lee, J.-H.; Lee, K.-B. Comparison of Intaglio Surface Trueness of Interim Dental Crowns Fabricated with SLA 3D Printing, DLP 3D Printing, and Milling Technologies. Healthcare 2021, 9, 983. https://doi.org/10.3390/healthcare9080983
Son K, Lee J-H, Lee K-B. Comparison of Intaglio Surface Trueness of Interim Dental Crowns Fabricated with SLA 3D Printing, DLP 3D Printing, and Milling Technologies. Healthcare. 2021; 9(8):983. https://doi.org/10.3390/healthcare9080983
Chicago/Turabian StyleSon, Keunbada, Jung-Ho Lee, and Kyu-Bok Lee. 2021. "Comparison of Intaglio Surface Trueness of Interim Dental Crowns Fabricated with SLA 3D Printing, DLP 3D Printing, and Milling Technologies" Healthcare 9, no. 8: 983. https://doi.org/10.3390/healthcare9080983
APA StyleSon, K., Lee, J.-H., & Lee, K.-B. (2021). Comparison of Intaglio Surface Trueness of Interim Dental Crowns Fabricated with SLA 3D Printing, DLP 3D Printing, and Milling Technologies. Healthcare, 9(8), 983. https://doi.org/10.3390/healthcare9080983