
“Hesitating and Puzzling”: The Experiences and Decision Process of Acute Ischemic Stroke Patients with Prehospital Delay after the Onset of Symptoms

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants and Setting
2.3. Data Collection
2.4. Data Analysis
2.5. Rigor
2.6. Ethical Consideration
3. Results
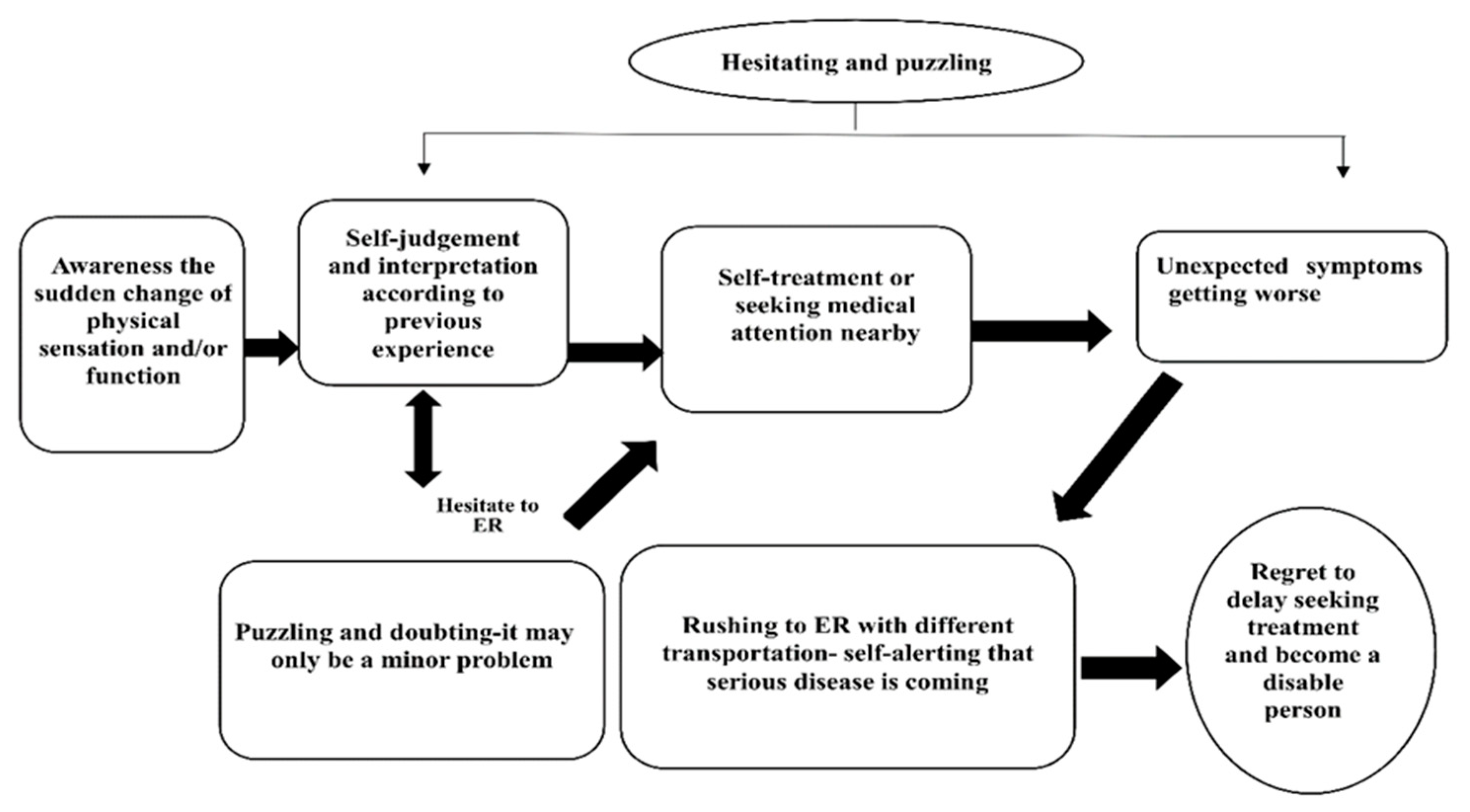
3.1. Hesitating and Puzzling
When I went shopping on foot, I kicked my left foot all the way to the floor because it felt like it was weak and numb. I thought it was just too tired. Because my hands and feet still moved, I didn’t think it was a stroke. So my husband took me to get a massage … Stick the Chinese medicine patches on the thigh, and I went home to sleep after folk therapy. I thought it should be all right. I didn’t expect to wake up the next morning and find that my left foot couldn’t be lifted. I was scared … I called my son to my room right away … When my son saw me like this, he got me up immediately. I didn’t change my clothes. I limped to his car. He drove me to the hospital very fast … When I got to the hospital, the doctor said it was a stroke … but we missed the golden cure. I was very depressed … because there was no chance of a thrombolytic injection (P15).
3.2. Awareness the Sudden Change of Physical Sensation and/or Function
At six o’clock in the morning, when I got up, I couldn’t stand stably. I felt that my left foot had no strength to walk, so I leaned to one side. The glass bottle in my left hand fell to the ground … My mouth was dripping all the time (P1).
When I walked, I suddenly felt dizzy and unstable walking. Both hands and feet had no strength, and my hands and feet on one side were numb (P2).
When I was talking to my wife, my face suddenly turned crooked (P4).
3.3. Puzzling and Doubting—It May Only Be a Minor Problem
If I had a stroke, it seemed that I could not move my hands and feet, that’s it … I could still move! (P7).
I didn’t have a problem with high triglyceride levels. It’s just high blood sugar … It’s just the numbness of the feet … I’m not fat either (P12).
I want to say that I am so young … maybe it’s work that causes numbness and weakness (P14).
I take medicine to prevent stroke every day … It’s impossible to have a stroke (P23).
3.4. Self-Judgment and Interpretation According to Previous Experience
Because of the problem of nerve compression, I may be a little slow in walking (P5).
This foot had fasciitis before … I wonder if it caused it (P10).
Dizziness …I thought it was an inner ear disorder (P13).
It’s too hot to be comfortable … Maybe it’s too tired to drive (P11).
3.5. Self-Treatment or Seeking Medical Attention Nearby
Massage thighs or legs … used scissors to stab the index finger and middle finger, pressing philtrum (P10).
I kicked my left foot all the way to the floor … it was weak and numb … my husband took me to get a massage …stick the Chinese medicine patches on the thigh (P15).
Went to the nearby pharmacy to take Chinese medicine … went to the clinic for a sore injection (P17).
3.6. Unexpected Symptoms Getting Worse
I still felt dizzy and start to vomit. Speaking was very unclear … The wife said that my face was asymmetric (P2).
When I went to the toilet, I suddenly fell to the ground when my feet were weak … One foot couldn’t walk. It’s walking by dragging (P17).
Hands and feet became more numb, holding things in the hands couldn’t hold, fell on the ground … couldn’t lift the left foot when walking (P22).
3.7. Rushing to ER with Different Transportation—Self-Alerting That Serious Disease Is Coming
Told my wife to drive over to the hospital immediately … It must be a big problem (P7).
Stroke … My son’s wife quickly called a taxi to take me to the hospital (P17).
The doctor said that there might be a stroke… so I drove to the emergency room (P14).
It’s a stroke. My wife was looking for help from the neighbor, who carried me from the second floor to the first floor, my wife called 119 and called an ambulance to the emergency room (P12).
3.8. Regret to Delay Seeking Treatment and Become a Disable Person
I have a stroke now, like this … (with tears), my hands and feet are weak and I need my husband’s help now (P9).
I didn’t dare to go out when I just came home from hospital. I stayed in my room … didn’t want to talk to anyone … I didn’t think it was a stroke at the time, so I didn’t come to the hospital right away … It’s a pity that I’ve delayed my golden therapy, because it’s going to take a lot of time to recover now, and I would cry when I thought of becoming like this (P10).
I really regret coming to the hospital so slowly … My daily life now depends on the help of my family … If I come early, maybe I could get a thrombus injection (P17).
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kim, Y.S.; Park, S.S.; Bae, H.J.; Cho, A.H.; Cho, Y.J.; Han, M.K.; Heo, J.H.; Kang, K.; Kim, D.E.; Kim, H.Y.; et al. Stroke awareness decreases prehospital delay after acute ischemic stroke in Korea. BMC Neurol. 2011, 11, 2–8. [Google Scholar] [CrossRef]
- Yanagida, T.; Fujimoto, S.; Inoue, T.; Suzuki, S. Causes of prehospital delay in stroke patients in an urban aging society. J. Gerontol. Geriatr. 2014, 5, 77–81. [Google Scholar] [CrossRef][Green Version]
- Department of Health. The National Stroke Strategy. London: DH. 2007. Available online: http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_081062 (accessed on 20 March 2020).
- Department of Health. Stroke: Act. F.A.S.T. London: Department of Health. 2009. Available online: http://www.nhs.uk/Actfast/Pages/stroke.aspx (accessed on 20 March 2020).
- Nasr, D.M.; Brinjikji, W.; Cloft, H.J.; Rabinstein, A.A. Utilization of intravenous thrombolysis is increasing in the United States. Int. J. Stroke 2013, 8, 681–688. [Google Scholar] [CrossRef] [PubMed]
- Singer, O.C.; Hamann, G.F.; Misselwitz, B.; Steinmetz, H.; Foerch, C.; Arbeitsgruppe Schlaganfall Hessen. Time trends in systemic thrombolysis in a large hospital-based stroke registry. Cerebrovasc. Dis. 2012, 33, 316–321. [Google Scholar] [CrossRef] [PubMed]
- Hoffmeister, L.; Lavados, P.M.; Mar, J.; Comas, M.; Arrospide, A.; Castells, X. Minimum intravenous thrombolysis utilization rates in acute ischemic stroke to achieve population effects on disability: A discrete-event simulation model. J. Neurol. Sci. 2016, 365, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Hacke, W.; Lyden, P.; Emberso, J.; Baigent, C.; Blackwell, L.; Albers, G.; Bluhmki, E.; Brott, T.; Cohen, G.; Davis, S.M.; et al. Stroke Thrombolysis Trialists’ Collaborators Group. Effects of alteplase for acute stroke according to criteria defining the European Union and United States marketing authorizations: Individual-patient-data meta-analysis of randomized trials. Int. J. Stroke 2018, 13, 175–189. [Google Scholar] [CrossRef]
- Lachkhem, Y.; Rican, S.; Minvielle, E. Understanding delays in acute stroke care: A systematic review of reviews. Eur. J. Public Health 2018, 28, 426–433. [Google Scholar] [CrossRef] [PubMed]
- Appelros, P.; Jonsson, F.; Asberg, S.; Asplund, K.; Glader, E.L.; Åsberg, K.H.; Norrving, B.; Stegmayr, B.; Terént, A. Riks-Stroke Collaboration Trends in stroke treatment and outcome between 1995 and 2010: Observations from risks-stroke, the Swedish Stroke Register. Cerebrovasc. Dis. 2014, 37, 22–29. [Google Scholar] [CrossRef]
- Eissa, A.; Krass, I.; Bajorek, B.V. Optimizing the management of acute ischaemic stroke: A review of the utilization of intravenous recombinant tissue plasminogen activator (tPA). J. Clin. Pharm. Ther. 2012, 37, 620–629. [Google Scholar] [CrossRef]
- Hsieh, C.Y.; Chen, C.H.; Chen, Y.C.; Kao, Y.H. National survey of thrombolytic therapy for acute ischemic stroke in Taiwan 2003–2010. J. Stroke Cerebrovasc. Dis. 2013, 22, 620–627. [Google Scholar] [CrossRef]
- Yu, K.H.; Bae, H.J.; Kwon, S.U.; Kang, D.W.; Hong, K.S.; Lee, Y.S.; Rha, J.H.; Koo, J.S.; Kim, J.S.; Kim, J.H.; et al. Analysis of 10,811 cases with acute ischemic stroke from Korean stroke registry: Hospital-based multicenter prospective registration study. J. Korean Neurosurg. Soc. 2006, 24, 535–543. [Google Scholar]
- Dombrowski, S.U.; Mackintosh, J.E.; Sniehotta, F.F.; Araujo-Soares, V.; Rodgers, H.; Thomson, R.G.; Murtagh, M.J.; Ford, G.A.; Eccles, M.P.; White, M. The impact of the UK “Act FAST” stroke awareness campaign: Content analysis of patients, witness and primary care clinicians’ perceptions. BMC Public Health 2013, 13, 915. [Google Scholar] [CrossRef] [PubMed]
- Mackintosh, J.E.; Murtagh, M.J.; Rodgers, H.; Thomson, R.G.; Ford, G.A.; White, M. Why people do, or do not, immediately contact emergency medical services following the onset of acute stroke: Qualitative interview study. PLoS ONE 2012, 7, e46124. [Google Scholar] [CrossRef]
- Pulvers, J.N.; Watson, J.D.G. If time is brain where is the improvement in prehospital time after stroke? Front. Neurol. 2017, 8, 617. [Google Scholar] [CrossRef]
- Mellor, R.M.; Bailey, S.; Sheppard, J.; Carr, P.; Quinn, T.; Boyal, A.; Sandler, D.; Sims, D.G.; Mant, J.; Greenfield, S.; et al. Decisions and delays within stroke patients’ route to the hospital: A qualitative study. Ann. Emerg. Med. 2015, 65, 279–287. [Google Scholar] [CrossRef] [PubMed]
- Shin, C.N.; An, K.; Sim, J. Facilitators of and barriers to emergency medical service use by acute ischemic stroke patients: A retrospective survey. Int. J. Nurs. Sci. 2017, 4, 52–57. [Google Scholar] [CrossRef]
- Glaser, B.G. Theoretical Sensitivity: Advancesin the Methodology of Grounded Theory; The Sociology Press: Mill Valley, CA, USA, 1978. [Google Scholar]
- Glaser, B.G.; Strauss, A. The Discovery of Grounded Theory: Strategies for Qualitative Research; Aldine: Chicago, IL, USA, 1967. [Google Scholar]
- Strauss, A.; Corbin, J. Basic of Qualitative Research: Grounded Theory Procedures and Techniques; SAGE: Newbury Park, CA, USA, 1990. [Google Scholar]
- Lecouturier, J.; Murtagh, M.; Thomson, R.; Ford, G.; White, M.; Eccles, M.; Rodgers, H. Response to symptoms of stroke and TIA in the UK: A systematic review. BMC Health Serv. Res. 2010, 8, 157. [Google Scholar] [CrossRef]
- Birks, M.; Mills, J. Grounded theory: A practical guide. In Data Generation and Collection, 2nd ed.; SAGE: London, UK, 2015; pp. 85–107. [Google Scholar]
- Urquhart, C. Grounded Theory for Qualitative Research: A Practical Guide; SAGE: Thousand Oaks, CA, USA, 2013; p. 194. [Google Scholar]
- de Haan, R.; Limburg, M.; Bossuyt, P.; van der Meulen, J.; Aaronson, N. The clinical meaning of Ranking handicap grades after stroke. Stroke 1995, 26, 2027–2030. [Google Scholar] [CrossRef]
- Lincoln, Y.S.; Guba, E.G. Naturalistic Inquiry; SAGE: Beverly Hills, CA, USA, 1985. [Google Scholar]
- Ahasan, H.A.M.N.; Kumar, S.P.; Das, A.; Ayaz, K.; Dey, P.; Ahmed-Siddique, A.; Chowdhury, M.K.; Hossain, M.Y.; Minnat, B.; Hussain, D.A.S. Delay in hospital arrival of stroke patients: An observational study. J. Med. 2013, 14, 106–109. [Google Scholar] [CrossRef]
- O’Connell, E.; Hartigan, I. Recognition of stroke symptoms by stroke survivors. Br. J. Neurosci. Nurs. 2011, 7, 541–546. [Google Scholar] [CrossRef]
- Harrison, M.; Ryan, T.; Gardiner, C.; Jones, A. Patients’ and carers’ experiences of gaining access to acute stroke care: A qualitative study. Emerg. Med. J. 2012, 30, 1033–1037. [Google Scholar] [CrossRef] [PubMed]
- Harding, G.; Taylor, K. Health, illness and seeking health care. Pharm. J. 2002, 269, 526–528. [Google Scholar]
- Liao, C.C.; Lin, J.G.; Tsai, C.C.; Lane, H.L.; Su, T.C.; Wang, H.H.; Sung, F.C.; Chen, T.L.; Shih, C.C. An investigation of the use of traditional Chinese medicine in stroke patients in Taiwan. Evid. Based Complementary Altern. Med. 2012, 2012, 387164. [Google Scholar] [CrossRef] [PubMed]
- Shih, C.C.; Liao, C.C.; Su, Y.C.; Yeh, T.F.; Lin, J.G. The association between socioeconomic status and traditional Chinese medicine use among children in Taiwan. BMC Health Serv. Res. 2012, 12, 27. [Google Scholar] [CrossRef]
- Shih, C.C.; Lee, H.H.; Chen, T.L.; Tsai, C.C.; Lane, H.L.; Chiu, W.T.; Liao, C.C. Reduced use of emergency care and hospitalization in patients with traumatic brain injury receiving acupuncture treatment. Evid. Based Complementary Altern. Med. 2013, 2013, 262039. [Google Scholar] [CrossRef]
- Shih, C.C.; Huang, L.H.; Lane, H.L.; Tsai, C.C.; Lin, J.G.; Chen, T.L.; Yeh, C.C. Use of folk therapy in Taiwan: A nationwide cross-sectional survey of prevalence and associated factors. Evid. Based Complement. Alternat. Med. 2015, 2015, 649265. [Google Scholar] [CrossRef] [PubMed]
- Chi, C. Integrating traditional medicine into modern health care systems: Examining the role of Chinese medicine in Taiwan. Soc. Sci. Med. 1994, 39, 307–321. [Google Scholar] [CrossRef]
- Taiwan’s Health Promotion Administration, Ministry of Health and Welfare. Stroke Pricking Bloodletting. Available online: https://www.hpa.gov.tw/Pages/Detail.aspx?nodeid (accessed on 10 May 2020).
- Wongwiangjunt, S.; Komoltri, C.; Poungvarin, N.; Nilanont, Y. Stroke awareness and factors influencing hospital arrival time: A prospective observational study. J. Med. Assoc. Thai. 2015, 98, 260–264. [Google Scholar]
- Kutlubaev, M.A.; Hackett, M.L. Part II: Predictors of depression after stroke and impact of depression on stroke outcome: An updated systematic review of observational studies. Int. J. Stroke 2014, 9, 1026–1036. [Google Scholar] [CrossRef]
- Robinson, R.G.; Jorge, R.E. Post-stroke depression: A review. Am. J. Psychiatry 2016, 173, 221–231. [Google Scholar] [CrossRef]


{kind=link}
| Case No. | Gender/Age (Years)/Education Level | Diagnosis | History | MRS/*Time |
|---|---|---|---|---|
| 1 | Male/60/ Vocational high school | Right medial cerebellum infarcts | HTN; DM; hyperlipidemia | 1/28 h |
| 2 | Female/62/ Vocational high school | Left pons infarcts | Arrhythmia | 2/48 h |
| 3 | Male/63/ Junior college | Left pons infarcts | HTN; hyperlipidemia | 2/4 h |
| 4 | Female/56/ Primary school | Right basal ganglia, right insular cortex, and right F-T-P lobes infarcts | Heart disease | 2/9 h |
| 5 | Male/73/ Vocational high school | Right putamen and left centrum semiovale infarcts | HTN; hyperlipidemia | 2/5 h |
| 6 | Male/64/ Vocational high school | Right corona radiata and right frontoparietal infarcts | DM | 2/54 h |
| 7 | Male/52/ Graduate school | Cerebral infarction due to stenosis of right middle cerebral artery | HTN; hyperlipidemia | 2/7 h |
| 8 | Male/67/ Primary school | Left internal capsule infarcts | HTN | 2/72 h |
| 9 | Female/58/ Vocational high school | Right thalamic infarcts | DM; hyperlipidemia | 2/26 h |
| 10 | Male/56/ Middle school | Left thalamus infarcts | Hyperlipidemia | 2/22 h |
| 11 | Female/61/ Primary school | Right cerebral infarcts | HTN | 2/28 h |
| 12 | Male/62/ Primary school | Left cerebellar infarcts | HTN Hyperlipidemia | 3/48 h |
| 13 | Male/64/ Junior college | Right thalamus infarcts | Hyperlipidemia | 2/72 h |
| 14 | Male/54/ Vocational high school | Left striatocapsule infarcts | Hyperlipidemia | 1/72 h |
| 15 | Female/68/ primary school | Right pons, infarcts | HTN; hyperlipidemia | 2/48 h |
| 16 | Male/63/ primary school | Left thalamus infarcts | Hyperlipidemia | 1/24 h |
| 17 | Male/66/ primary school | Left pons infarcts | HTN; DM; hyperlipidemia | 2/72 h |
| 18 | Male/65/ Middle school | Right posterior basal ganglia and corona radiate infarcts | DM | 2/6 h |
| 19 | Male/63/ Vocational high school | Right periventricular white matter infarcts | HTN; DM; hyperlipidemia | 2/5 h |
| 20 | Female/58/ Vocational high school | Left cerebral infarcts | HTN; DM; hyperlipidemia | 3/48 h |
| 21 | Male/53/ Vocational high school | Right MCA infarcts | Hyperlipidemia | 3/20 h |
| 22 | Female/58/ Vocational high school | Right MCA infarcts | HTN; hyperlipidemia | 2/18 h |
| 23 | Female/57/ Middle school | Left pons infarcts | HTN; DM | 2/72 h |
| 24 | Male/58/ Middle school | Right MCA infarction | HTN; hyperlipidemia | 2/9 h |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, P.-Y.; Tsao, L.-I.; Chen, Y.-W.; Lo, Y.-T.; Sun, H.-L. “Hesitating and Puzzling”: The Experiences and Decision Process of Acute Ischemic Stroke Patients with Prehospital Delay after the Onset of Symptoms. Healthcare 2021, 9, 1061. https://doi.org/10.3390/healthcare9081061
Wang P-Y, Tsao L-I, Chen Y-W, Lo Y-T, Sun H-L. “Hesitating and Puzzling”: The Experiences and Decision Process of Acute Ischemic Stroke Patients with Prehospital Delay after the Onset of Symptoms. Healthcare. 2021; 9(8):1061. https://doi.org/10.3390/healthcare9081061
Chicago/Turabian StyleWang, Pao-Yu, Lee-Ing Tsao, Yu-Wei Chen, Ying-Tao Lo, and Hui-Lin Sun. 2021. "“Hesitating and Puzzling”: The Experiences and Decision Process of Acute Ischemic Stroke Patients with Prehospital Delay after the Onset of Symptoms" Healthcare 9, no. 8: 1061. https://doi.org/10.3390/healthcare9081061
APA StyleWang, P.-Y., Tsao, L.-I., Chen, Y.-W., Lo, Y.-T., & Sun, H.-L. (2021). “Hesitating and Puzzling”: The Experiences and Decision Process of Acute Ischemic Stroke Patients with Prehospital Delay after the Onset of Symptoms. Healthcare, 9(8), 1061. https://doi.org/10.3390/healthcare9081061