
Activating Partnership Assets to Produce Synergy in Primary Health Care: A Mixed Methods Study


Abstract
1. Introduction
1.1. Primary Health Care
1.2. Partnership Evaluation and Partnership Synergy
2. Materials and Methods
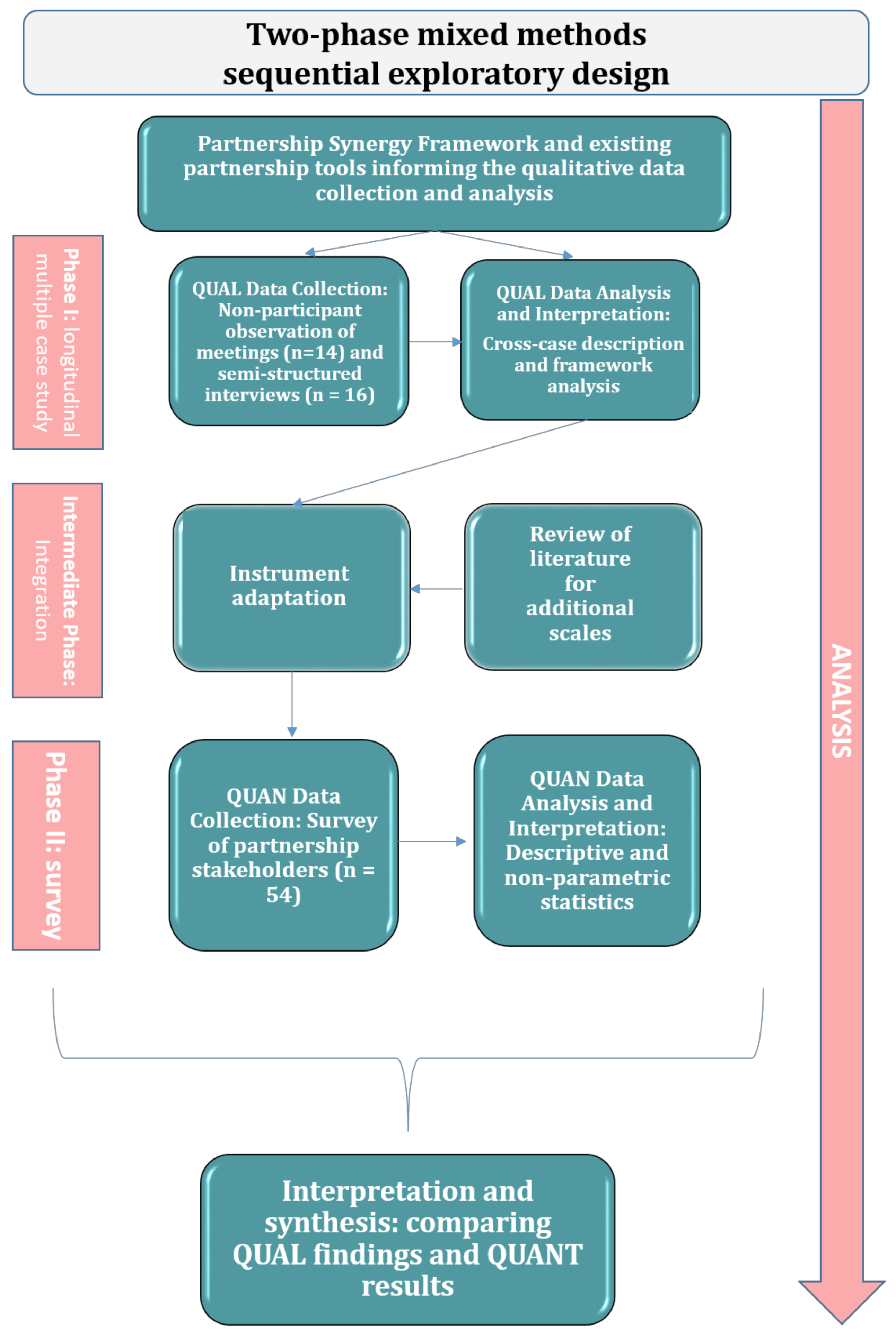
2.1. Study Design
2.2. Background Work
2.3. Phase I: Qualitative Data Collection and Analysis
2.4. Building on Qualitative Findings
2.5. Phase II: Quantitative Data Collection and Analysis
3. Results
3.1. Study Participants
3.2. Qualitative Findings
3.2.1. Partnership Assets
Partnership Acquired Assets
Partnership Generated Assets
3.2.2. Partnership Enabling Processes
Resource Management
Leadership
Administration and Management
Communication
Decision-Making
Contextual Adaptation
3.2.3. Partnership Synergy
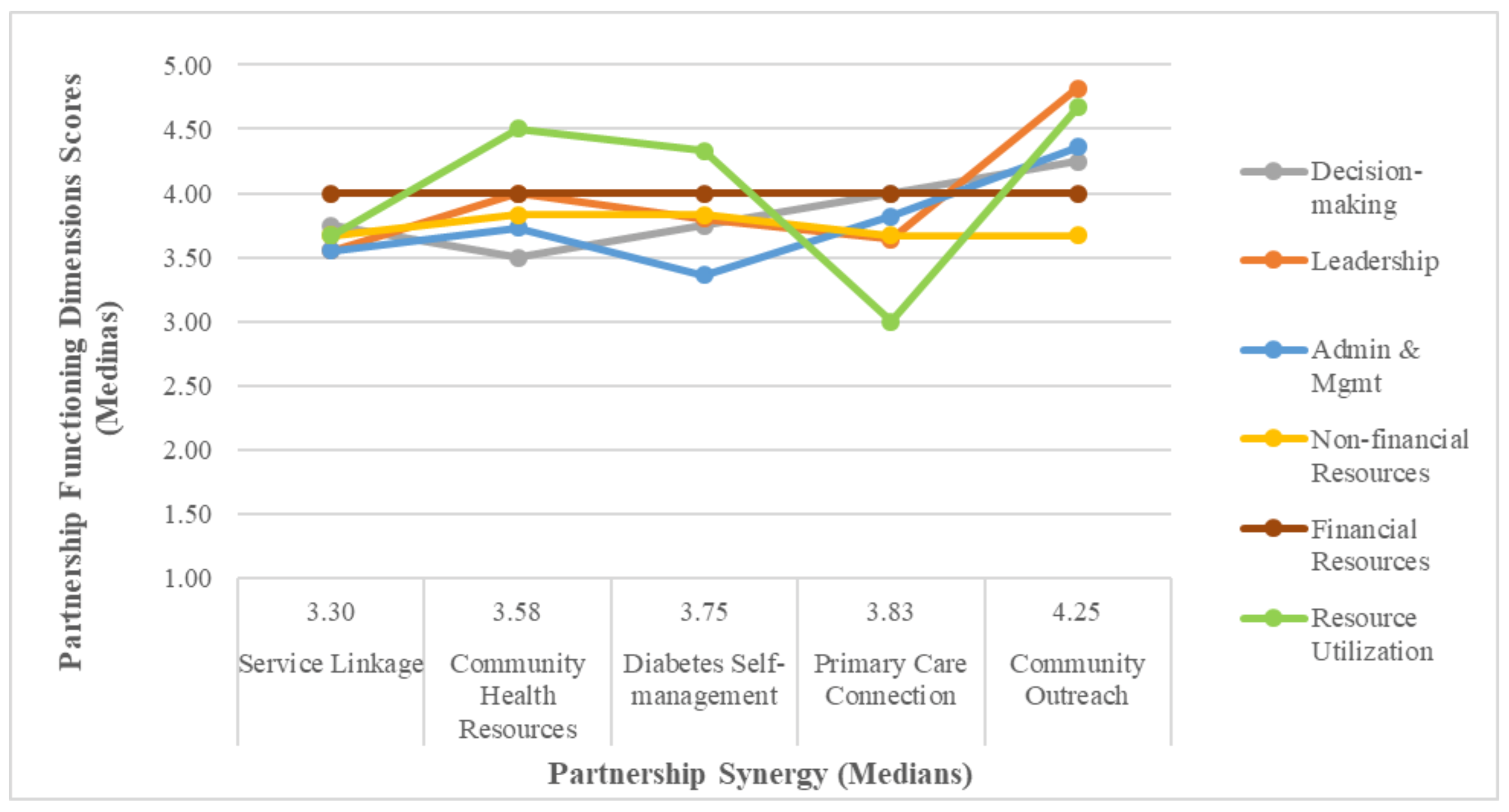
3.3. Quantitative Results
3.4. Integration of Qualitative Findings and Quantitative Results
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- El Ansari, W.; Phillips, C.J.; Hammick, M. Collaboration and partnerships: Developing the evidence base. Health Soc. Care Community 2001, 9, 215–227. [Google Scholar] [CrossRef]
- Butt, G.; Markle-Reid, M.; Browne, G. Interprofessional partnerships in chronic illness care: A conceptual model for measuring partnership effectiveness. Int. J. Integr. Care 2008, 8, e08. [Google Scholar] [CrossRef]
- Hernandez-Aguado, I.; Zaragoza, A.G. Support of public–private partnerships in health promotion and conflicts of interest. BMJ Open 2016, 6, e009342. [Google Scholar] [CrossRef] [PubMed]
- Popay, J.; Williams, G. Partnership in health: Beyond the rhetoric. J. Epidemiol. Community Health 1998, 52, 410–411. [Google Scholar] [CrossRef]
- Drahota, A.; Meza, R.D.; Brikho, B.; Naaf, M.; Estabillo, J.; Gomez, E.D.; Vejnoska, S.F.; Dufek, S.; Stahmer, A.C.; Aarons, G.A. Community-Academic Partnerships: A Systematic Review of the State of the Literature and Recommendations for Future Research. Milbank Q. 2016, 94, 163–214. [Google Scholar] [CrossRef] [PubMed]
- Jones, J.; Barry, M.M. Exploring the relationship between synergy and partnership functioning factors in health promotion partnerships. Health Promot. Int. 2011, 26, 408–420. [Google Scholar] [CrossRef]
- Kreuter, M.W.; Lezin, N.A.; Young, L.A. Evaluating Community-Based Collaborative Mechanisms: Implications for Practitioners. Health Promot. Pract. 2000, 1, 49–63. [Google Scholar] [CrossRef]
- Lasker, R.D.; Weiss, E.S.; Miller, R. Partnership Synergy: A Practical Framework for Studying and Strengthening the Collaborative Advantage. Milbank Q. 2001, 79, 179–205. [Google Scholar] [CrossRef]
- Mitchell, S.M.; Shortell, S.M. The Governance and Management of Effective Community Health Partnerships: A Typology for Research, Policy, and Practice. Milbank Q. 2000, 78, 241–289. [Google Scholar] [CrossRef]
- Eilbert, K.W. A Community Health Partnership Model: Using Organizational Theory to Strengthen Collaborative Public Health Practice. Ph.D. Thesis, George Washington University, Ann Arbor, MI, USA, May 2003. [Google Scholar]
- United Nations General Assembly. Enhanced Cooperation between the United Nations and All Relevant Partners, in Particular the Private Sector: Report of the Secretary-General; UN: New York, NY, USA, 2003. [Google Scholar]
- Schoen, C.; Osborn, R.; Huynh, P.T.; Doty, M.; Davis, K.; Zapert, K.; Peugh, J. Primary Care and Health System Performance: Adults’ Experiences In Five Countries. Health Aff. 2004, 23 (Suppl. 1), W4-487–W4-503. [Google Scholar] [CrossRef] [PubMed]
- Starfield, B.; Shi, L.; Macinko, J. Contribution of Primary Care to Health Systems and Health. Milbank Q. 2005, 83, 457–502. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. The World Health Report 2008—Primary Health Care (Now More Than Ever); World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- Starfield, B. Is Primary Care Essential? Lancet: London, UK, 1994; Volume 344, pp. 1129–1133. [Google Scholar]
- Kringos, D.; Boerma, W.; Bourgueil, Y.; Cartier, T.; Dedeu, T.; Hasvold, T.; Hutchinson, A.; Lember, M.; Oleszczyk, M.; Pavlic, D.R.; et al. The strength of primary care in Europe: An international comparative study. Br. J. Gen. Pract. 2013, 63, e742–e750. [Google Scholar] [CrossRef] [PubMed]
- Van Weel, C.; Kidd, M.R. Why strengthening primary health care is essential to achieving universal health coverage. CMAJ 2018, 190, E463–E466. [Google Scholar] [CrossRef] [PubMed]
- Breton, M.; Levesque, J.-F.; Pineault, R.; Hogg, W. Primary Care Reform: Can Quebec’s Family Medicine Group Model Benefit from the Experience of Ontario’s Family Health Teams? Healthc. Policy 2011, 7, e122–e135. [Google Scholar] [CrossRef] [PubMed]
- Levesque, J.F.; Pineault, R.; Hamel, M.; Roberge, D.; Kapetanakis, C.; Simard, B.; Prud’homme, A. Emerging organisational models of primary healthcare and unmet needs for care: Insights from a population-based survey in Quebec province. BMC Fam. Pract. 2012, 13, 66. [Google Scholar] [CrossRef] [PubMed]
- McCusker, J.; Tousignant, P.; Da Silva, R.B.; Ciampi, A.; Lévesque, J.-F.; Vadeboncoeur, A.; Sanche, S. Factors predicting patient use of the emergency department: A retrospective cohort study. Can. Med. Assoc. J. 2012, 184, E307–E316. [Google Scholar] [CrossRef]
- Social, D. Science Integration Directorate. Report summary—The Direct Economic Burden of Socioeconomic Health Inequalities in Canada: An Analysis of Health Care Costs by Income Level. Health Promot. Chronic Dis. Prev. Can. Res. Policy Pract. 2016, 36, 118–119. [Google Scholar]
- Hutchison, B.; Levesque, J.-F.; Strumpf, E.; Coyle, N. Primary Health Care in Canada: Systems in Motion. Milbank Q. 2011, 89, 256–288. [Google Scholar] [CrossRef]
- Saltman, R.B.; Rico, A.; Boerma, W.G.W. Primary Care in the Driver’s Seat? Organizational Reform in European Primary Care; Open University Press: Maidenhead, UK, 2006. [Google Scholar]
- Asada, Y.; Kephart, G. Equity in health services use and intensity of use in Canada. BMC Health Serv. Res. 2007, 7, 41. [Google Scholar] [CrossRef]
- National Health and Hospitals Reform Commission. A Healthier Future for All Australians—Final Report; Commonwealth of Australia: Sydney, Australia, 2009. [Google Scholar]
- Romanow, R.J. Building on Values: The Future of Health Care in Canada: Final Report; Commission on the Future of Health Care in Canada: Saskatoon, SK, Canada, 2002. [Google Scholar]
- Kirby, M.J.L. Reforming Health Protection and Promotion in Canada: Time to Act; The Standing Senate Committee on Social Affairs, Science and Technology: Ottawa, ON, Canada, 2003. [Google Scholar]
- Clair, M. Emerging Solutions—Report and Recommendations; Commission d’Étude Sur les Services de Santé et les Services Sociaux: Quebec City, QC, Canada, 2001. [Google Scholar]
- Hutchison, B. A Long Time Coming: Primary Healthcare Renewal in Canada. Healthc. Pap. 2008, 8, 10–24. [Google Scholar] [CrossRef]
- Verma, J.; Petersen, S.; Samis, S.; Akunov, N.; Graham, J. Healthcare Priorities in Canada: A Backgrounder; Canadian Foundation for Healthcare Improvement: Ottawa, ON, Canada, 2014. [Google Scholar]
- Gray, B. Collaborating: Finding Common Ground for Multiparty Problems, 1st ed.; Jossey-Bass Management Series; Jossey-Bass: San Francisco, CA, USA, 1989. [Google Scholar]
- Zuckerman, H.S.; Kaluzny, A.D.; Ricketts, T.C. Alliances in health care: What we know, what we think we know, and what we should know. Health Care Manag. Rev. 1995, 20, 54–64. [Google Scholar] [CrossRef]
- Russell, G.; Kunin, M.; Harris, M.; Levesque, J.-F.; Descôteaux, S.; Scott, C.; Lewis, V.; Dionne, É.; Advocat, J.; Dahrouge, S.; et al. Improving access to primary healthcare for vulnerable populations in Australia and Canada: Protocol for a mixed-method evaluation of six complex interventions. BMJ Open 2019, 9, e027869. [Google Scholar] [CrossRef] [PubMed]
- Dahrouge, S.; Gauthier, A.; Chiocchio, F.; Presseau, J.; Kendall, C.; Lemonde, M.; Chomienne, M.-H.; Perna, A.; Toal-Sullivan, D.; Devlin, R.A.; et al. Access to Resources in the Community Through Navigation: Protocol for a Mixed-Methods Feasibility Study. JMIR Res. Protoc. 2019, 8, e11022. [Google Scholar] [CrossRef]
- Levesque, J.-F.; University of New South Wales, Sydney, Australia; Russell, G.M.; Monash University, Notting Hill, Australia; Haggerty, J.; McGill University, Montreal, Canada; Dahrouge, S.; University of Ottawa, Ottawa, Canada; Harris, M.; University of New South Wales, Sydney, Australia; Scott, C.; University of Calgary, Calgary, Canada; Christley, S.; South Australia Health, Adelaide, Australia; Lemelin, J.; University of Ottawa, Ottawa, Canada; Rodrigue, J.; Direction de Santé Publique de la Montérégie, Longueuil, Canada; Lewis, V.; La Trobe University, Melbourne, Australia. Innovative Models Promoting Access-to-Care Transformation (IMPACT). Proposal to the Canadian Institutes for Health Care Research, & Australian Primary Health Care Research Institute, Unpublished grant. 2013. [Google Scholar]
- Zakocs, R.C.; Edwards, E. What Explains Community Coalition Effectiveness?: A Review of the Literature. Am. J. Prev. Med. 2006, 30, 351–361. [Google Scholar] [CrossRef] [PubMed]
- Butterfoss, F.D.; Francisco, V.T. Evaluating Community Partnerships and Coalitions with Practitioners in Mind. Health Promot. Pract. 2004, 5, 108–114. [Google Scholar] [CrossRef] [PubMed]
- Kegler, M.C.; Steckler, A.; McLeroy, K.; Malek, S.H. Factors That Contribute to Effective Community Health Promotion Coalitions: A Study of 10 Project ASSIST Coalitions in North Carolina. Health Educ. Behav. 1998, 25, 338–353. [Google Scholar] [CrossRef]
- Larkan, F.; Uduma, O.; Lawal, S.A.; van Bavel, B. Developing a framework for successful research partnerships in global health. Glob. Health 2016, 12, 1–9. [Google Scholar] [CrossRef]
- Ramaswamy, R.; Kallam, B.; Kopic, D.; Pujic, B.; Owen, M.D. Global Health Partnerships: Building Multi-National Collaborations to Achieve Lasting Improvements in Maternal and Neonatal Health. Glob. Health 2016, 12, 22. [Google Scholar] [CrossRef]
- Kelly, C. Measuring the Performance of Partnerships: Why, What, How, When? Measuring the performance of partnerships. Geogr. Compass 2012, 6, 149–162. [Google Scholar] [CrossRef]
- Watson, D.E.; Broemeling, A.M.; Reid, R.J.; Black, C. A Results-Based Logic Model for Primary Health Care: Laying an Evidence-Based Foundation to Guide Performance Measurement, Monitoring and Evaluation; Centre for Health Services and Policy Research, the University of British Columbia: Vancouver, BC, Canada, 2004. [Google Scholar]
- McLaughlin, J.A.; Jordan, G.B. Logic models: A tool for telling your programs performance story. Eval. Program Plan. 1999, 22, 65–72. [Google Scholar] [CrossRef]
- Clarke, A.; Macdonald, A. Outcomes to Partners in Multi-Stakeholder Cross-Sector Partnerships: A Resource-Based View. Bus. Soc. 2016, 58, 298–332. [Google Scholar] [CrossRef]
- Halliday, J.; Asthana, S.N.M.; Richardson, S. Evaluating Partnership: The Role of Formal Assessment Tools. Evaluation 2004, 10, 285–303. [Google Scholar] [CrossRef]
- Joss, N.; Keleher, H. Partnership tools for health promotion: Are they worth the effort? Glob. Health Promot. 2011, 18, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Jolley, G.; Lawless, A.; Hurley, C. Framework and tools for planning and evaluating community participation, collaborative partnerships and equity in health promotion. Health Promot. J. Aust. 2008, 19, 152–157. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Stolp, S.; Bottorff, J.L.; Seaton, C.L.; Jones-Bricker, M.; Oliffe, J.L.; Johnson, S.T.; Errey, S.; Medhurst, K.; Lamont, S. Measurement and evaluation practices of factors that contribute to effective health promotion collaboration functioning: A scoping review. Eval. Program Plan. 2017, 61, 38–44. [Google Scholar] [CrossRef]
- Senge, P.M. The Fifth Discipline: The Art and Practice of The Learning Organization; Rev. and Updated. ed. A Currency Book; Doubleday/Currency: New York, NY, USA, 2006. [Google Scholar]
- Weiss, E.S.; Anderson, R.M.; Lasker, R.D. Making the Most of Collaboration: Exploring the Relationship Between Partnership Synergy and Partnership Functioning. Health Educ. Behav. 2002, 29, 683–698. [Google Scholar] [CrossRef] [PubMed]
- Hart, S.L. A Natural-Resource-Based View of the Firm. Acad. Manag. Rev. 1995, 20, 986–1014. [Google Scholar] [CrossRef]
- Lev, B. Sharpening the intangibles edge. Harv. Bus. Rev. 2004, 82, 109–116. [Google Scholar]
- Boydell, L.; Hoggett, P.; Rugkåsa, J.; Cummins, A.-M. Intersectoral partnerships, the knowledge economy and intangible assets. Policy Politics 2008, 36, 209–224. [Google Scholar] [CrossRef]
- Corbin, J.H.; Mittelmark, M.B. Partnership lessons from the Global Programme for Health Promotion Effectiveness: A case study. Health Promot. Int. 2008, 23, 365–371. [Google Scholar] [CrossRef]
- Cramm, J.M.; Phaff, S.; Nieboer, A.P. The role of partnership functioning and synergy in achieving sustainability of innovative programmes in community care. Health Soc. Care Community 2012, 21, 209–215. [Google Scholar] [CrossRef]
- Cramm, J.M.; Nieboer, A.P. Disease-management partnership functioning, synergy and effectiveness in delivering chronic-illness care. Int. J. Qual. Health Care 2012, 24, 279–285. [Google Scholar] [CrossRef] [PubMed]
- Project Management Institute. A Guide to the Project Management Body of Knowledge (PMBOK® Guide), 5th ed.; Project Management Institute, Inc.: Newtown Square, PA, USA, 2013. [Google Scholar]
- Jones, J.; Barry, M.M. Developing a scale to measure synergy in health promotion partnerships. Glob. Health Promot. 2011, 18, 36–44. [Google Scholar] [CrossRef] [PubMed]
- Center for the Advancement of Collaborative Strategies in Health. Partnership Self-Assessment Tool Questionnaire. 2002. Available online: https://www.nccmt.ca/registry/resource/pdf/10.pdf (accessed on 18 August 2021).
- Creswell, J.W.; Plano Clark, V.L. Designing and Conducting Mixed Methods Research, 2nd ed.; SAGE Publications: Los Angeles, CA, USA, 2011. [Google Scholar]
- Yin, R.K. Case Study Research: Design and Methods, 5th ed.; Sage Publications: Los Angeles, CA, USA, 2014. [Google Scholar]
- Loban, E.; Scott, C.; Lewis, V.; Haggerty, J. Improving primary health care through partnerships: Key insights from a cross-case analysis of multi-stakeholder partnerships in two Canadian provinces. Health Sci. Rep. 2021, Submitted. [Google Scholar]
- Loban, E.; Scott, C.; Lewis, V.; Haggerty, J. Measuring partnership synergy and functioning: Multi-stakeholder collaboration in primary health care. PLoS ONE 2021, 16, e0252299. [Google Scholar] [CrossRef] [PubMed]
- Green, J.; Thorogood, N. Qualitative Methods for Health Research, 4th ed.; Sage: London, UK, 2018. [Google Scholar]
- Wilkinson, S. Focus Groups in Health Research: Exploring the Meanings of Health and Illness. J. Health Psychol. 1998, 3, 329–348. [Google Scholar] [CrossRef] [PubMed]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Pluye, P.; Hong, Q.N. Combining the power of stories and the power of numbers: Mixed methods research and mixed studies reviews. Annu. Rev. Public Health 2014, 35, 29–45. [Google Scholar] [CrossRef]
- QSR International. NVivo 12. 2018. Available online: https://nvivo-spain.com/ufaqs/how-do-i-cite-qsr-software-in-my-work/ (accessed on 18 August 2021).
- Fetters, M.D.; Curry, L.A.; Creswell, J.W. Achieving Integration in Mixed Methods Designs-Principles and Practices. Health Serv. Res. 2013, 48, 2134–2156. [Google Scholar] [CrossRef]
- Dillman, D.A.; Smyth, J.D.; Christian, L.M. Internet, Phone, Mail, and Mixed-Mode Surveys: The Tailored Design Method, 4th ed.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2014. [Google Scholar]
- Qualtrics; September 2018 ed.; Provo, UT, USA. 2005. Available online: https://www.qualtrics.com/blog/citing-qualtrics/ (accessed on 18 August 2021).
- IBM Corp. IBM SPSS Statistics for Windows; IBM: Armonk, NY, USA, 2015. [Google Scholar]
- Huxham, C.; Vaugen, S. Ambiguity, complexity and dynamics in the membership of collaboration. Hum. Relat. 2000, 53, 771–806. [Google Scholar] [CrossRef]
- Hermens, N.; Verkooijen, K.T.; Koelen, M.A. Associations between partnership characteristics and perceived success in Dutch sport-for-health partnerships. Sport Manag. Rev. 2019, 22, 142–152. [Google Scholar] [CrossRef]
- Spooner, C.; Lewis, V.; Scott, C.; Dahrouge, S.; Haggerty, J.; Russell, G.; Dionne, E.; Stocks, N.; Harris, M. Improving Access to Primary Health Care: A Cross-Case Comparison Based on an a Priori Program Theory. Int. J. Equity Health. 2022. [Google Scholar]
- Currie, G.; Lockett, A. Distributing Leadership in Health and Social Care: Concertive, Conjoint or Collective? Int. J. Manag. Rev. 2011, 13, 286–300. [Google Scholar] [CrossRef]
- Denis, J.-L.; Langley, A.; Sergi, V. Leadership in the Plural. Acad. Manag. Ann. 2012, 6, 1–73. [Google Scholar] [CrossRef]
- Himmelman, A.T. Collaboration for a Change (Revised January 2002): Definitions, Decision-Making Models, Roles, and Collaboration Process Guide; Himmelman Consulting: Minneapolis, MN, USA, 2002. [Google Scholar]
- Fiedler, F.E. A theory of leadership effectiveness. In McGraw-Hill Series in Management; McGraw-Hill: New York, NY, USA, 1967. [Google Scholar]
- Hofler, D.; Barnett, T. Contingency Approach to Management. In Encyclopedia of Management; Helms, M.M., Thomson, G., Eds.; Thomson Gale: Detroit, MI, USA, 2006. [Google Scholar]
- Morgan, G. Images of Organization: Updated Edition of the International Bestseller, Updated ed.; Sage Publications: Thousand Oaks, CA, USA, 2006. [Google Scholar]
- Hunter, D.; Perkins, N. Partnership Working in Public Health: The Implications for Governance of a Systems Approach. J. Health Serv. Res. Policy 2012, 17, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Lucero, J.E.; Boursaw, B.; Eder, M.; Greene-Moton, E.; Wallerstein, N.; Oetzel, J.G. Engage for Equity: The Role of Trust and Synergy in Community-Based Participatory Research. Health Educ. Behav. 2020, 47, 372–379. [Google Scholar] [CrossRef]
- Johnson-Lafleur, J.; Papazian-Zohrabian, G.; Rousseau, C.C. Learning from partnership tensions in transcultural interdisciplinary case discussion seminars: A qualitative study of collaborative youth mental health care informed by game theory. Soc. Sci. Med. 2019, 237, 112443. [Google Scholar] [CrossRef]
- Khodyakov, D.; Stockdale, S.; Jones, F.; Ohito, E.; Jones, A.; Lizaola, E.; Mango, J. An Exploration of the Effect of Community Engagement in Research on Perceived Outcomes of Partnered Mental Health Services Projects. Soc. Ment. Health 2011, 1, 185–199. [Google Scholar] [CrossRef] [PubMed]
- Horton, D.; Prain, G.; Thiele, G. Perspectives on Partnership: A Literature Review; CIP: Lima, Peru, 2009. [Google Scholar]
- Wildridge, V.; Childs, S.; Cawthra, L.; Madge, B. How to create successful partnerships-a review of the literature. Health Inf. Libr. J. 2008, 21, 3–19. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Partnership Title | Service Linkage | Community Health Resources | Diabetes Self-Management | Primary Care Connection | Community Outreach | Residential Aged Care |
|---|---|---|---|---|---|---|
| Target population and access problem | Vulnerable clients of community-based chronic disease services without a primary care provider. | Primary care patients with complex health and social needs not receiving available community services that would optimize their illness management. | Patients with low health literacy and other social vulnerabilities presenting to general practice with poorly controlled diabetes. | Unattached patients in high deprivation neighbourhoods who have trouble connecting effectively to newly assigned family physicians from centralized wait lists. | Individuals and groups of socially vulnerable populations living in a geographic area with few PHC ** services and high concentration of marginalized populations. | Aged and frail residents of long-term care facilities who have complex chronic health needs. |
| Type of vulnerability | Low socioeconomic status, social isolation due to the fact of geographic distance/public transport, chronic illness and developmental disability. | Socially complex patients, including one of Canada’ linguistic minorities. | Low socioeconomic status, geographic isolation and culturally and linguistically diverse backgrounds. | Low income, unemployment and low social support. | Recent immigrants, Aboriginal people, seniors and homeless persons. | Socially isolated frail elders who rely on others for the provision of care. |
| Intervention type | Brokerage service to link identified patients to one of a panel of volunteer family practitioners. | Training provided to primary care providers to increase their awareness of community health resources; community-based intervention by a lay patient navigator to facilitate access to these resources. | A website that provides information and referral options to support diabetes self-management. | Telephone outreach by lay volunteer navigators to relay access-related and visit preparation information. | Mobile (pop-up) outreach by a variety of PHC and social service providers catering to the needs of attendees, held at different locations. | Training and policy and procedure redesign in participating long-term care facilities to improve the quality, consistency and responsiveness of PHC **. |
| Intended consequence | Successful linkage with a PHC ** practice. | Increased referrals to community health resources and improved access to these services. | Successful affiliation to a coordinating primary care physician and improved diabetes self-management skills. | Successful affiliation to a family physician. | Enduring relationships between PCH and social service providers and the users of mobile pop-up services. | Reduction in preventable hospitalizations and improvements in the delivery and management of care to frail elderly residents. |
| Partnerships | Total Number of Participants (n = 54) | Gender | Mean Length of Time in Partnership | Minimum/Maximum Length of Time in Partnership | Main Role |
|---|---|---|---|---|---|
| Percent Female | |||||
| Service Linkage | 9 | 78% (7) | 3.8 years | 2–6 years | Academic representative—4 Decision maker—1 Health care manager—4 |
| Community Health Resources | 19 | 68% (13) | 2.6 years | 1–4 years | Academic representative—5 Community organization representative—3 Decision maker—2 Health care manager—4 Patient representative—3 Primary care physician—2 |
| Diabetes Self-Management | 7 | 71% (5) | 3.1 years | 0.7–5 years | Academic representative—3 Community representative—1 Decision maker—1 Health care manager—1 Primary care physician—1 |
| Primary Care Connection | 12 | 83% (10) | 3 years | 1–5 years | Academic representative—5 Decision maker—1 Health care manager—3 Patient representative—1 Primary care physician—2 |
| Community Outreach | 8 | 86% (7) | 2.8 years | 2.5–5 years | Academic representative—6 Decision maker—1 Health care manager—1 |
| Partnership Synergy Processes | Communication | Decision-Making | Leadership | Administration and Management | Non-Financial Resources | Financial Resources | Resource Utilization | External Environment | |
|---|---|---|---|---|---|---|---|---|---|
| Partnership synergy outcomes | 0.61 | 0.34 | 0.60 | 0.69 | 0.60 | 0.39 | 0.18 | 0.46 | 0.15 |
| Partnership synergy processes | 0.44 | 0.59 | 0.60 | 0.48 | 0.51 | 0.35 | 0.45 | 0.26 | |
| Total partnership synergy | 0.40 | 0.66 | 0.74 | 0.61 | 0.51 | 0.28 | 0.50 | 0.22 | |
| Communication | 0.47 | 0.50 | 0.45 | 0.38 | 0.32 | 0.39 | 0.10 | ||
| Decision-making | 0.65 | 0.52 | 0.40 | 0.07 | 0.29 | 0.25 | |||
| Leadership | 0.74 | 0.42 | 0.13 | 0.53 | −0.08 | ||||
| Administration and management | 0.42 | 0.05 | 0.50 | −0.06 | |||||
| Non-financial resources | 0.56 | 0.32 | −0.21 | ||||||
| Financial resources | 0.28 | −0.18 | |||||||
| Resource utilization | −0.17 |
| Partnership | Not Well at All or Not so Well | Moderately Well | Very Well or Extremely Well | Mean (Standard Deviation) |
|---|---|---|---|---|
| Service Linkage (n = 9) | 2 (22.2%) | 3 (33.3%) | 4 (44.4%) | 3.22 (1.20) |
| Community Health Resources (n = 15) | 0 | 5 (33.3%) | 10 (66.7%) | 3.87 (0.74) |
| Diabetes Self-Management (n = 7) | 0 | 2 (28.6%) | 5 (71.4%) | 3.86 (0.69) |
| Primary Care Connection (n = 10) | 1 (10%) | 2 (20%) | 7 (70%) | 3.60 (0.70) |
| Community Outreach (n = 7) | 0 | 1 (14.3%) | 6 (85.7%) | 4.14 (0.69) |
| Determinants of Partnership Synergy | Phase I Qualitative Findings Based on 14 Meeting Observations and 16 Interviews in Two Multi-Stakeholder Partnerships | Phase II Quantitative Results Based on Survey of 54 Partnership Stakeholders Representing Five Multi-Stakeholder Partnerships | Comparison of Qualitative Findings and Quantitative Results—Comments |
|---|---|---|---|
| Partnership Assets | |||
| Intangible assets—non-financial resources (can be acquired or generated) | Main acquired intangible assets:
|
| Both qualitative and quantitative findings suggest that intangible assets contributed to partnership synergy through having appropriately complementary and heterogeneous skill sets. Heterogeneity and complementarity were achieved by having a dynamic group composition that reflected the critical dimensions of the problem to be addressed and of the context that was likely to affect the work of the partnership. |
| Tangible assets—financial and other capital resources |
|
| Qualitative and quantitative findings are partially consistent, suggesting that the importance of financial resources for partnership synergy related principally to supporting the coordinating infrastructure and a number of partnership activities (such as evaluation and outreach). Non-financial resources seemed to be more critical for partnership synergy than financial resources. |
| Partnership Enabling Processes | |||
| Asset/resource management |
|
| Both qualitative and quantitative results indicate that high levels of stakeholder engagement were important to achieve partnership synergy. The nature of engagement has to be aligned with the function of the partnership and the need to fulfil project objectives, with particular attention to meaningful engagement of end users and addressing disengagement. Benefits related to respective organizations seem to be more critical than personal benefits. Managing incentives, so that benefits outweigh costs, is an important consideration. |
| Leadership |
|
| Qualitative and quantitative results suggest that partnership synergy was facilitated by leadership capable of mobilizing the various perspectives of stakeholders. Qualitative results also highlight the contribution to partnership synergy of more distributed forms of leadership; however, the quantitative results suggest the limitations of the sub-scale in terms of assessing the extent to which leadership was distributed. |
| Administration and management |
|
| Qualitative and quantitative results highlight the importance for partnership synergy of a core infrastructure and adaptive management approaches to support the work of the partnerships and facilitate the ability of partners to contribute meaningfully. |
| Communication |
|
| Qualitative findings point to the importance of timely and varied communication mechanisms in synergistic partnership learning. However, quantitative results were limited, precluding definitive conclusions regarding the contribution of communication to partnership synergy. |
| Decision-Making |
|
| Qualitative and quantitative findings highlight the importance to partnership synergy of distributed decision-making and collaborative approaches to problem-solving. |
| Contextual adaptation |
|
| Qualitative findings suggest that recognizing and dealing with changes in partnership context are important to achieve partnership synergy. Quantitative findings were limited in terms of assessing the contribution of external context to partnership synergy. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Loban, E.; Scott, C.; Lewis, V.; Law, S.; Haggerty, J. Activating Partnership Assets to Produce Synergy in Primary Health Care: A Mixed Methods Study. Healthcare 2021, 9, 1060. https://doi.org/10.3390/healthcare9081060
Loban E, Scott C, Lewis V, Law S, Haggerty J. Activating Partnership Assets to Produce Synergy in Primary Health Care: A Mixed Methods Study. Healthcare. 2021; 9(8):1060. https://doi.org/10.3390/healthcare9081060
Chicago/Turabian StyleLoban, Ekaterina, Catherine Scott, Virginia Lewis, Susan Law, and Jeannie Haggerty. 2021. "Activating Partnership Assets to Produce Synergy in Primary Health Care: A Mixed Methods Study" Healthcare 9, no. 8: 1060. https://doi.org/10.3390/healthcare9081060
APA StyleLoban, E., Scott, C., Lewis, V., Law, S., & Haggerty, J. (2021). Activating Partnership Assets to Produce Synergy in Primary Health Care: A Mixed Methods Study. Healthcare, 9(8), 1060. https://doi.org/10.3390/healthcare9081060