
Educational Needs of Nurses for Respiratory Communicable Infectious Disease Care: A Cross-Sectional Descriptive Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Location and Participant
2.2. Instruments
2.3. Data Collection
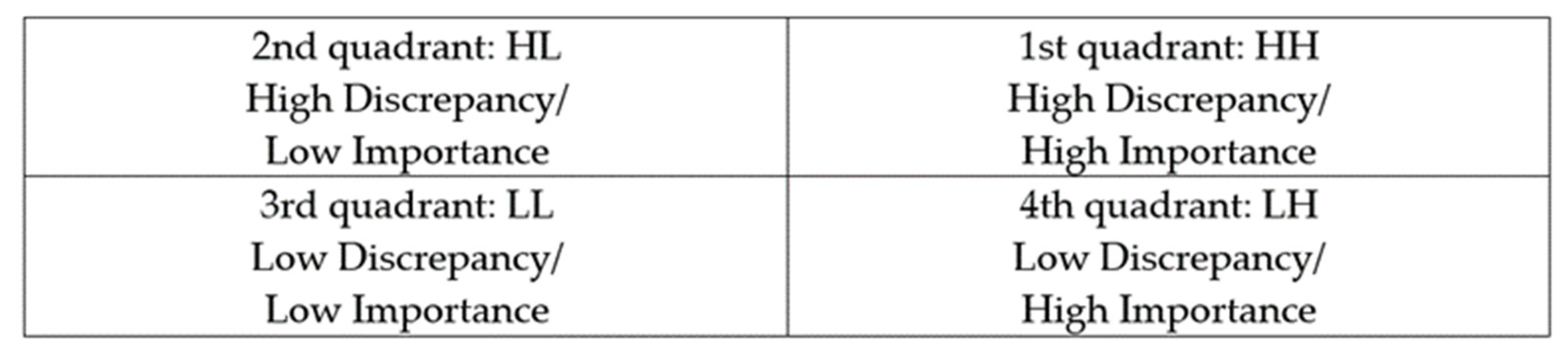
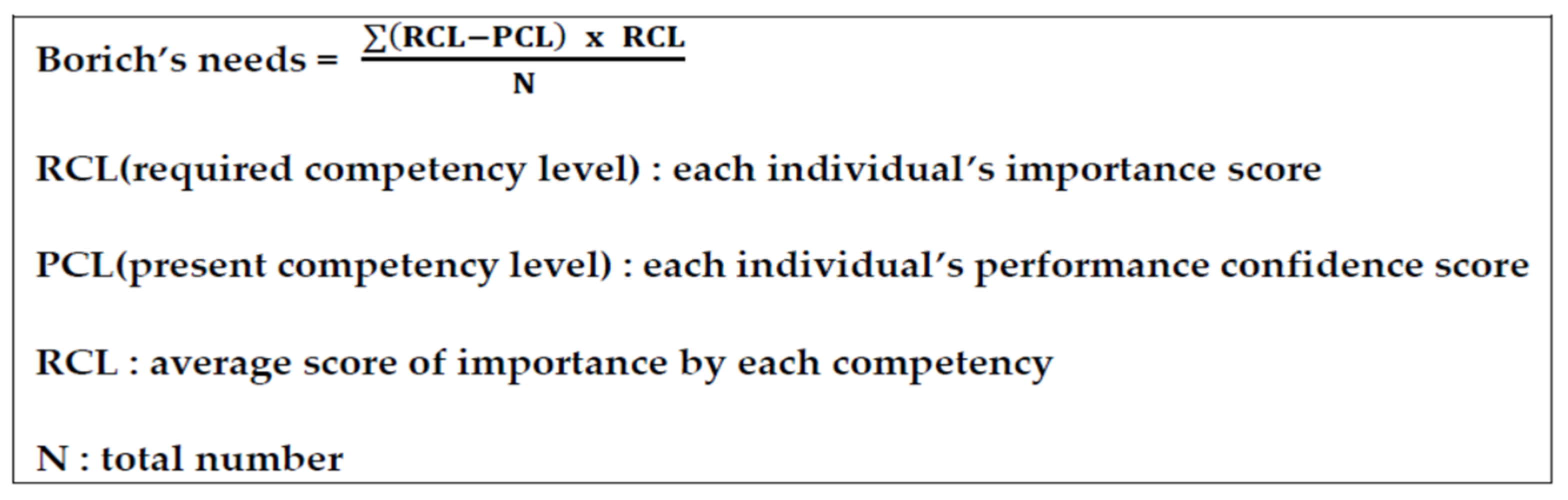
2.4. Data Analysis
3. Results
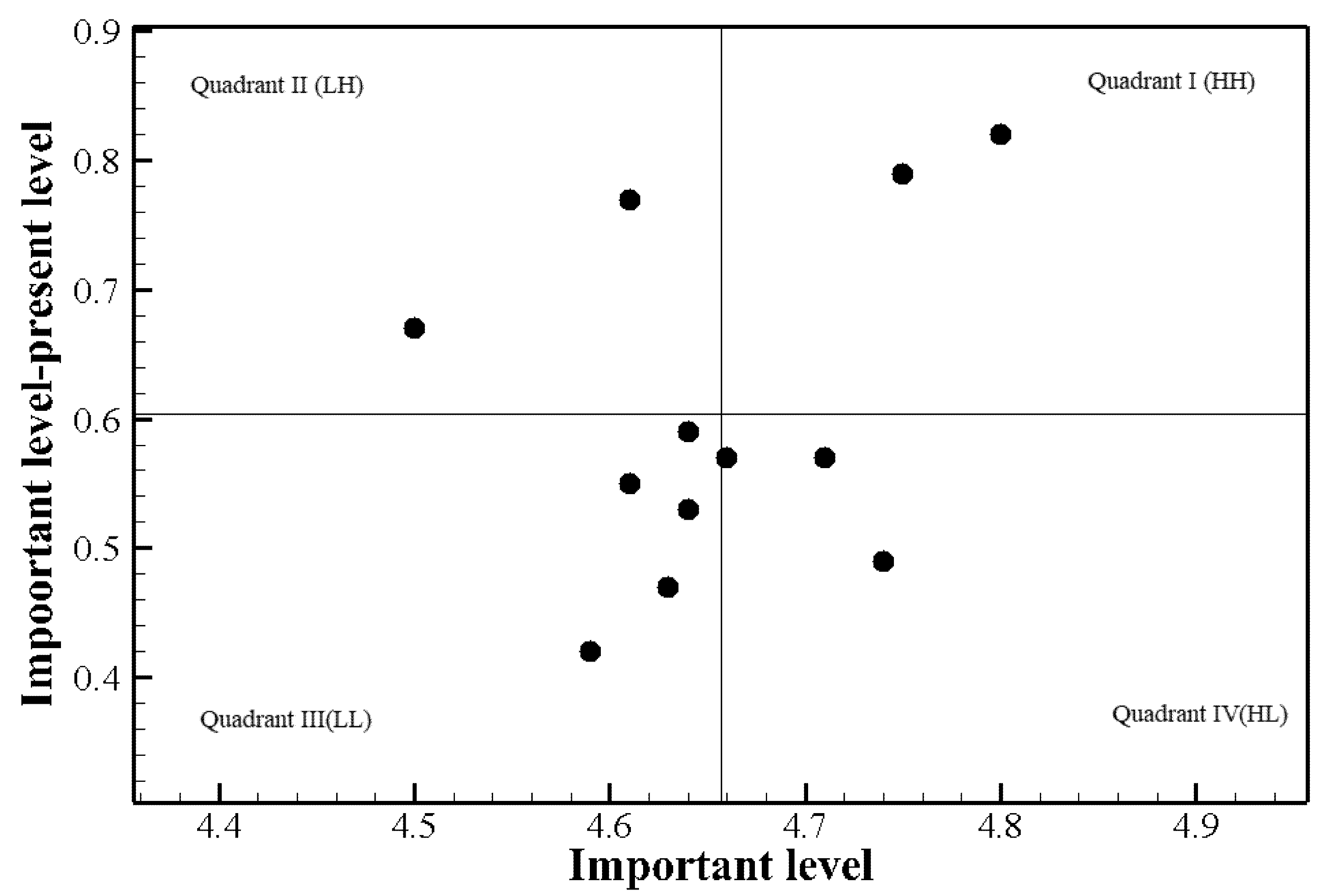
3.1. Analysis of Training Needs and Priority of Training among Participants with Prior COVID-19 Patient Care Experience
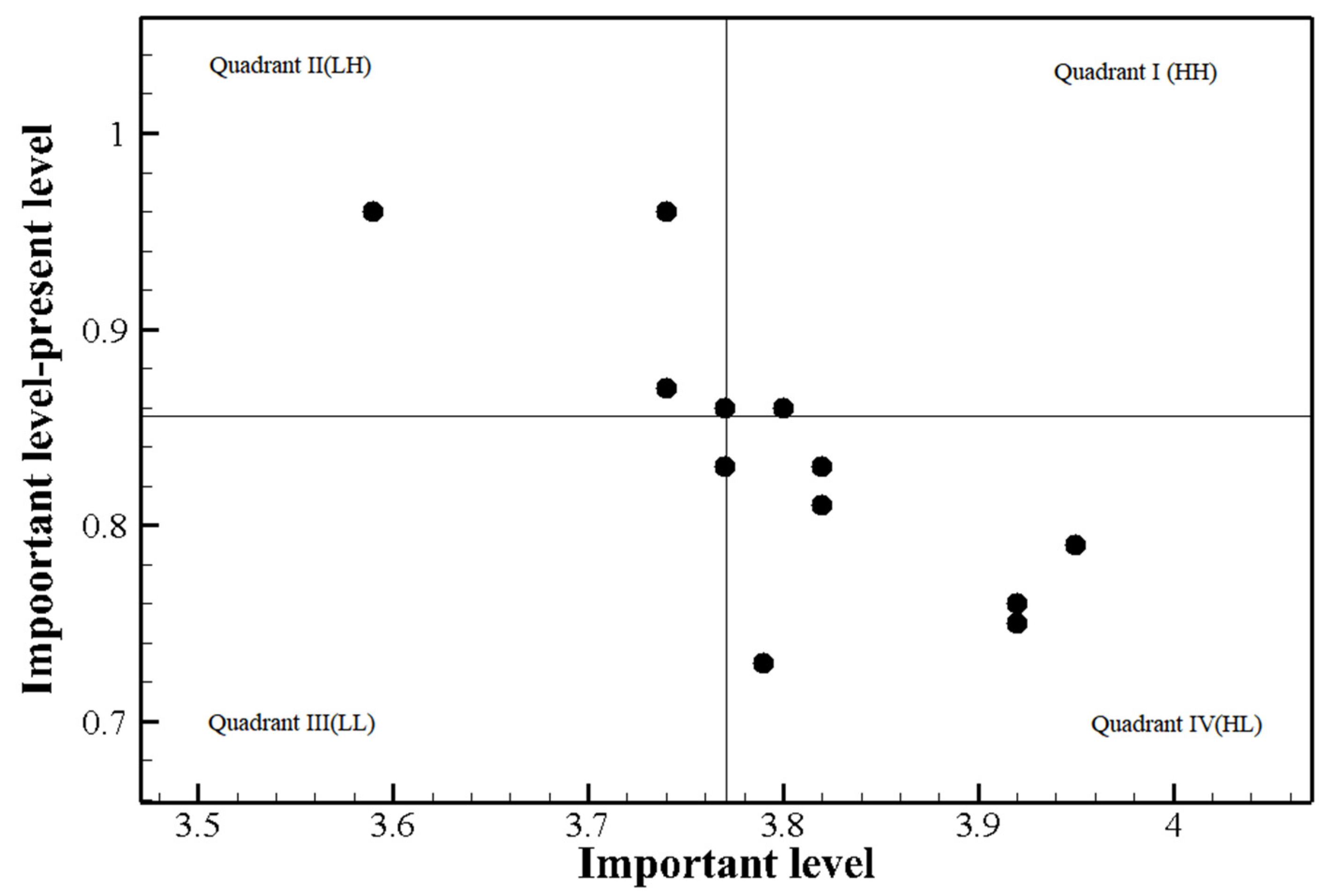
3.2. Analysis of Training Needs and Priority of Training among Participants without Prior Experience in COVID-19 Patient Care
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Muniyappa, R.; Gubbi, S. COVID-19 pandemic, coronaviruses, and diabetes mellitus. Am. J. Physiol. Endocrinol. Metab. 2020, 318, e736–e741. [Google Scholar] [CrossRef] [Green Version]
- Young, H.M.; Fick, D.M. Public health and ethics intersect at new levels with gerontological nursing in COVID-19 pandemic. J. Gerontol. Nurs. 2020, 46, 4–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marks, S.; Edwards, S.; Jerge, E.H. Rapid deployment of critical care nurse education during the COVID-19 pandemic. Nurse Lead. 2021, 19, 165–169. [Google Scholar] [CrossRef] [PubMed]
- Purba, A.K. How should the role of the nurse change in response to Covid-19? Nurs. Times 2020, 116, 25–28. [Google Scholar]
- García-Martín, M.; Roman, P.; Rodriguez-Arrastia, M.; Diaz-Cortes, M.D.M.; Soriano-Martin, P.J.; Ropero-Padilla, C. Novice nurse’s transitioning to emergency nurse during COVID-19 pandemic: A qualitative study. J. Nurs. Manag. 2021, 29, 258–267. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Kakade, M.; Fuller, C.J.; Fan, B.; Fang, Y.; Kong, J.; Wu, P. Depression after exposure to stressful events: Lessons learned from the severe acute respiratory syndrome epidemic. Compr. Psychiatry 2012, 53, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Catton, H. Nursing in the COVID-19 pandemic and beyond: Protecting, saving, supporting and honouring nurses. Int. Nurs. Rev. 2020, 67, 157–159. [Google Scholar] [CrossRef] [PubMed]
- Pappa, S.; Ntella, V.; Giannakas, T.; Giannakoulis, V.G.; Papoutsi, E.; Karsaounou, P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Brain Behav. Immun. 2020, 88, 901–907. [Google Scholar] [CrossRef] [PubMed]
- Al-Tawfiq, J.A.; Rothwell, S.; Mcgregor, H.A.; Khouri, Z.A. A multi-faceted approach of a nursing led education in response to MERS-CoV infection. J. Infect. Public Health 2018, 11, 260–264. [Google Scholar] [CrossRef] [PubMed]
- Ji, Y.J. Nurses’ Knowledge, Educational Needs, and Practice Regarding MERS Infection Control. Master’s Thesis, Woosuk University, Jeollabuk-do, Korea. Available online: http://www.riss.kr/search/detail/DetailView.do?p_mat_type=be54d9b8bc7cdb09&control_no=ee6fd46b58a247c8ffe0bdc3ef48d419 (accessed on 30 May 2020).
- Nour, M.O.; Babilghith, A.O.; Natto, H.A.; Al-Amin, F.O.; Alawneh, S.M. Knowledge and attitude and practices of healthcare providers towards MERS-Cov infection at Makkah hospitals, KSA. Int. Res. J. Med. Med. Sci. 2015, 3, 103–112. [Google Scholar]
- Holloway, K.; Arcus, K.; Orsborn, G. Training needs analysis–The essential first step for continuing professional development design. Nurse Educ. Pract. 2018, 28, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Saleh, J.M.; Man, N.B. Training requirements of agricultural extension officers using Borich needs assessment model. J. Agric. Food Inf. 2017, 18, 110–122. [Google Scholar] [CrossRef]
- Borich, G.D. A needs assessment model for conducting follow-up studies. J. Teach. Educ. 1980, 31, 39–42. [Google Scholar] [CrossRef]
- Lomazzi, M.; Borisch, B.; Laaser, U. The millennium development goals: Experiences, achievements and what’s next. Glob. Health 2014, 7, e23695. [Google Scholar] [CrossRef] [PubMed]
- Murray, R.B.; Zentner, J.P. Nursing Concepts for Health Promotion; Prentice Hall: Hoboken, NJ, USA, 1979. [Google Scholar]
- Korea Center for Disease Control and Prevention Agency. Response Manual for Middle East Respiratory Syndrome Coronavirus (MERS-CoV). Available online: http://www.kdca.go.kr/board.es?mid=a20507020000&bid=0019&act=view&list_no=143205 (accessed on 1 October 2020).
- Mink, O.G.; Shultz, J.M.; Mink, B.P. Developing and Managing Open Organizations: A Model and Method for Maximizing Organizational Potential; Somerset Consulting Group: Austin, TX, USA, 1991. [Google Scholar]
- Halcomb, E.; McInnes, S.; Williams, A.; Ashley, C.; James, S.; Fernandez, R.; Calma, K. The experiences of primary healthcare nurses during the COVID-19 pandemic in Australia. J. Nurs. Scholarsh. 2020, 52, 553–563. [Google Scholar] [CrossRef] [PubMed]
- Etkind, S.N.; Bone, A.E.; Lovell, N.; Cripps, R.L.; Harding, R.; Higginson, I.J.; Sleeman, K.E. The role and response of palliative care and hospice services in epidemics and pandemics: A rapid review to inform practice during the COVID-19 pandemic. J. Pain Symptom Manag. 2020, 60, e31–e40. [Google Scholar] [CrossRef] [PubMed]
- Bolina, A.F.; Bomfim, E.; Lopes-Júnior, L.C. Frontline Nursing care: The COVID-19 pandemic and the Brazilian Health System. SAGE Open Nurs. 2020, 6, 2377960820963771. [Google Scholar] [CrossRef] [PubMed]
- Al-Thobaity, A.; Alshammari, F. Nurses on the frontline against the COVID-19 Pandemic: An integrative review. Dubai Med. J. 2020, 3, 87–92. [Google Scholar] [CrossRef]
- Goniewicz, K.; Goniewicz, M.; Burkle, F.M.; Khorram-Manesh, A. Cohort research analysis of disaster experience, preparedness, and competency-based training among nurses. PLoS ONE 2021, 16, e0244488. [Google Scholar] [CrossRef] [PubMed]
- Younos, T.B.; Hasan, M.K.; Nasreen, M. Are nurses ready? Bangladeshi nurses’ perceived preparedness for disasters: A mixed-methods approach. Int. J. Disaster Risk Reduct. 2021, 58, 102195. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Category | Participants with Prior Experience in COVID-19 Patient Care (n = 219) | Participants without Prior Experience in COVID-19 Patient Care (n = 153) |
|---|---|---|---|
| n (%) | n (%) | ||
| Gender | Man | 13(5.9) | 19(12.4) |
| Woman | 206(94.1) | 134(87.6) | |
| Age (years) | <30 | 88(40.2) | 82(53.6) |
| ≥30 | 131(59.8) | 71(46.4) | |
| Marital status | Married | 111(50.7) | 50(32.7) |
| Single and other | 108(49.3) | 103(67.3) | |
| Education | Associate’s degree | 47(21.5) | 31(20.3) |
| Bachelor’s degree | 157(71.7) | 112(73.2) | |
| Graduate school or higher | 15(6.8) | 10(6.5) | |
| Total clinical period (month) | <36 | 41(18.7) | 48(31.4) |
| 36–60 | 30(13.7) | 26(17.0) | |
| >60 | 148(67.6) | 79(51.6) | |
| The current department period (month) | <36 | 117(53.4) | 85(55.6) |
| ≥36 | 102(46.4) | 68(44.4) | |
| Work department | General ward | 159(72.6) | 99(64.7) |
| Special ward | 60(27.4) | 54(35.3) | |
| Number of infection control education | 1 | 60(27.4) | 38(24.8) |
| 2 | 48(21.9) | 33(21.6) | |
| 3 or more times | 111(50.7) | 82(53.6) | |
| Education hours (min per session) | Less than 30 | 89(40.6) | 55(35.9) |
| 30–60 | 22(10.0) | 23(15.0) | |
| More than 60 | 108(49.3) | 75(49.0) | |
| Main learning methods | Lecture | 44(20.1) | 34(22.2) |
| Online education | 23(10.5) | 19(12.4) | |
| Clinical training | 131(59.8) | 72(47.1) | |
| Other | 21(9.6) | 28(18.3) | |
| Effective learning methods | Lecture | 28(12.8) | 29(19.0) |
| Audiovisual education | 46(21.0) | 33(21.6) | |
| Lecture and training | 131(59.8) | 78(51.0) | |
| Online education and others | 14(6.4) | 13(8.5) |
| Contents | Importance | Confidence | Difference | t | p-Value | Borich Priority | Rank | The Locus for Focus Model |
|---|---|---|---|---|---|---|---|---|
| M ± SD | M ± SD | M ± SD | ||||||
| Initial response to communicable respiratory infection | 4.75 ± 0.51 | 3.96 ± 0.80 | 0.79 ± 0.86 | 13.46 | <0.001 | 3.75 | 1 | 1st quadrant (HH) |
| Management of aerosol-generating procedures in patients with communicable respiratory infection | 4.61 ± 0.57 | 3.83 ± 0.90 | 0.77 ± 0.91 | 12.57 | <0.001 | 3.58 | 2 | 2nd quadrant (LH) |
| Reporting of patients with communicable respiratory infection and death of patient | 4.5 ± 0.68 | 3.82 ± 0.93 | 0.67 ± 0.98 | 10.19 | <0.001 | 3.04 | 3 | 2nd quadrant (LH) |
| Characteristics of communicable respiratory infections | 4.80 ± 3.45 | 3.97 ± 0.77 | 0.82 ± 0.49 | 3.50 | 0.001 | 2.82 | 4 | 1st quadrant (HH) |
| Comunicable respiratory infection patients, nurse and medical staff movements (including admission to other hospitals and intensive care units, admission to isolation rooms, and check-out) | 4.64 ± 0.56 | 4.04 ± 0.80 | 0.59 ± 0.86 | 10.24 | <0.001 | 2.78 | 5 | 3rd quadrant (LL) |
| Guidelines for attention to patients with communicable respiratory infection | 4.71 ± 0.49 | 4.13 ± 0.75 | 0.57 ± 0.72 | 11.80 | <0.001 | 2.71 | 6 | 4th quadrant (HL) |
| Criteria for the confirmation and releasing patients from isolation with communicable respiratory infection | 4.66 ± 0.58 | 4.08 ± 0.83 | 0.57 ± 0.83 | 10.21 | <0.001 | 2.68 | 7 | 4th quadrant (HL) |
| Methods for assigning and operating isolation rooms for patients with communicable respiratory infection (including hospitalization rules) | 4.61 ± 0.61 | 4.05 ± 0.80 | 0.55 ± 0.87 | 9.44 | <0.001 | 2.57 | 8 | 3rd quadrant (LL) |
| Testing and management of patients with communicable respiratory infection | 4.64 ± 0.55 | 4.12 ± 0.79 | 0.53 ± 0.78 | 9.97 | <0.001 | 2.46 | 9 | 3rd quadrant (LL) |
| Recommended range and application of personal protective equipment | 4.74 ± 0.49 | 4.24 ± 0.72 | 0.49 ± 0.71 | 10.33 | <0.001 | 2.36 | 10 | 4th quadrant (HL) |
| Disinfection policy for equipment and sickroom environment (including disinfection of sickroom after discharge, laundry management, and medical waste management) | 4.63 ± 0.62 | 4.16 ± 0.73 | 0.47 ± 0.82 | 8.65 | <0.001 | 2.22 | 11 | 3rd quadrant (LL) |
| Management of family members, visitors, and caregivers when patients with communicable respiratory infection are hospitalized | 4.59 ± 0.59 | 4.17 ± 0.78 | 0.42 ± 0.77 | 8.09 | <0.001 | 1.95 | 12 | 3rd quadrant (LL) |
| Contents | Importance | Confidence | Difference | t | p-Value | Borich Priority | Rank | The Locus for Focus Model |
|---|---|---|---|---|---|---|---|---|
| M ± SD | M ± SD | M ± SD | ||||||
| Management of aerosol-generating procedures in patients with communicable respiratory infection | 4.52 ± 0.66 | 3.39 ± 0.94 | 1.12 ± 1.05 | 13.69 | <0.001 | 5.04 | 1 | 2nd quadrant (LH) |
| Initial response to communicable respiratory infection | 4.70 ± 0.52 | 3.74 ± 0.79 | 0.96 ± 0.88 | 13.50 | <0.001 | 4.49 | 2 | 2nd quadrant (LH) |
| Reporting of patients with communicable respiratory infection and death of patient | 4.55 ± 0.64 | 3.59 ± 0.92 | 0.96 ± 0.92 | 11.59 | <0.001 | 4.34 | 3 | 2nd quadrant (LH) |
| Comunicable respiratory infection patients, nurse and medical staff movements (including admission to other hospitals and intensive care units, admission to isolation rooms, and check-out) | 4.61 ± 0.52 | 3.74 ± 0.87 | 0.87 ± 0.91 | 11.86 | <0.001 | 4.02 | 4 | 2nd quadrant (LH) |
| Testing and management of patients with communicable respiratory infection | 4.67 ± 0.52 | 3.80 ± 0.85 | 0.86 ± 0.93 | 11.44 | <0.001 | 4.00 | 5 | 1st quadrant (HH) |
| Disinfection policy for equipment and sickroom environment (including disinfection of sickroom after discharge, laundry management, and medical waste management) | 4.66 ± 0.57 | 3.82 ± 0.83 | 0.83 ± 0.96 | 10.74 | <0.001 | 3.87 | 6 | 4th quadrant (HL) |
| Methods for assigning and operating isolation rooms for patients with communicable respiratory infection (including hospitalization rules) | 4.60 ± 0.56 | 3.77 ± 0.87 | 0.83 ± 0.93 | 10.95 | <0.001 | 3.79 | 7 | 3rd quadrant (LL) |
| Criteria for the confirmation and releasing patients from isolation with communicable respiratory infection | 4.63 ± 0.55 | 3.82 ± 0.82 | 0.81 ± 0.91 | 11.06 | <0.001 | 3.76 | 8 | 4th quadrant (HL) |
| Recommended range and application of personal protective equipment | 4.74 ± 0.48 | 3.95 ± 0.84 | 0.79 ± 0.87 | 11.13 | <0.001 | 3.72 | 9 | 4th quadrant (HL) |
| Management of family members, visitors, and caregivers when patients with communicable respiratory infection are hospitalized | 4.69 ± 0.51 | 3.92 ± 0.80 | 0.76 ± 0.89 | 10.57 | <0.001 | 3.56 | 10 | 4th quadrant (HL) |
| Guidelines for attention to patients with communicable respiratory infection | 4.68 ± 0.52 | 3.92 ± 0.77 | 0.75 ± 0.81 | 11.55 | <0.001 | 3.52 | 11 | 4th quadrant (HL) |
| Characteristics of communicable respiratory infections | 4.52 ± 0.55 | 3.79 ± 0.77 | 0.73 ± 0.72 | 12.48 | <0.001 | 3.29 | 12 | 4th quadrant (HL) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Han, J.-W.; Kang, J.-S.; Park, J.-H. Educational Needs of Nurses for Respiratory Communicable Infectious Disease Care: A Cross-Sectional Descriptive Study. Healthcare 2021, 9, 1043. https://doi.org/10.3390/healthcare9081043
Han J-W, Kang J-S, Park J-H. Educational Needs of Nurses for Respiratory Communicable Infectious Disease Care: A Cross-Sectional Descriptive Study. Healthcare. 2021; 9(8):1043. https://doi.org/10.3390/healthcare9081043
Chicago/Turabian StyleHan, Jeong-Won, Ji-Soon Kang, and Jun-Hee Park. 2021. "Educational Needs of Nurses for Respiratory Communicable Infectious Disease Care: A Cross-Sectional Descriptive Study" Healthcare 9, no. 8: 1043. https://doi.org/10.3390/healthcare9081043
APA StyleHan, J.-W., Kang, J.-S., & Park, J.-H. (2021). Educational Needs of Nurses for Respiratory Communicable Infectious Disease Care: A Cross-Sectional Descriptive Study. Healthcare, 9(8), 1043. https://doi.org/10.3390/healthcare9081043