1. Introduction
Italy was the first European country involved in the Coronavirus disease 2019 (COVID-19) pandemic. The general attitude suggested by health authorities was postponing deferrable interventions, which lead to a drop in the number of people seeking hospital care. As reported elsewhere, people suffering from neurologic [
1] and cardiac [
2] diseases have vanished from emergency departments (EDs), feeding the suspicion of increased overall mortality as the most devastating consequences of the pandemic on the care of diseases other than COVID-19. For instance, it was estimated that the total number of deaths in December 2020 was over 25,000 in Italy [
3]. Despite the fear of contagion and the general recommendation to avoid unnecessary visits to EDs, we hypothesized that a lower volume but unchanged pattern of ED visits for urgent conditions occurred in 2020 compared to 2019.
The aim of the present analysis is to investigate the pattern of presentations to the ED of Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico in Milano, a metropolitan ED of a tertiary level university hospital in Lombardia.
2. Materials and Methods
We retrospectively analyzed the number of all ED presentations during 2019 and 2020, together with demographic data and symptoms. We excluded women with obstetric or gynecologic conditions and patients aged <18 years who were managed in another dedicated ED within the same hospital. Data are expressed as absolute numbers and proportions or means and standard deviations. The main findings are presented as the difference between proportions or mean difference, with a 95% confidence interval (CI). The Wilcoxon Rank Sum test was used to test the difference between continuous data.
P-values < 0.05 denote statistically significant results. Analyses were performed using R Core Team, version 4.0.3 [
4].
3. Results
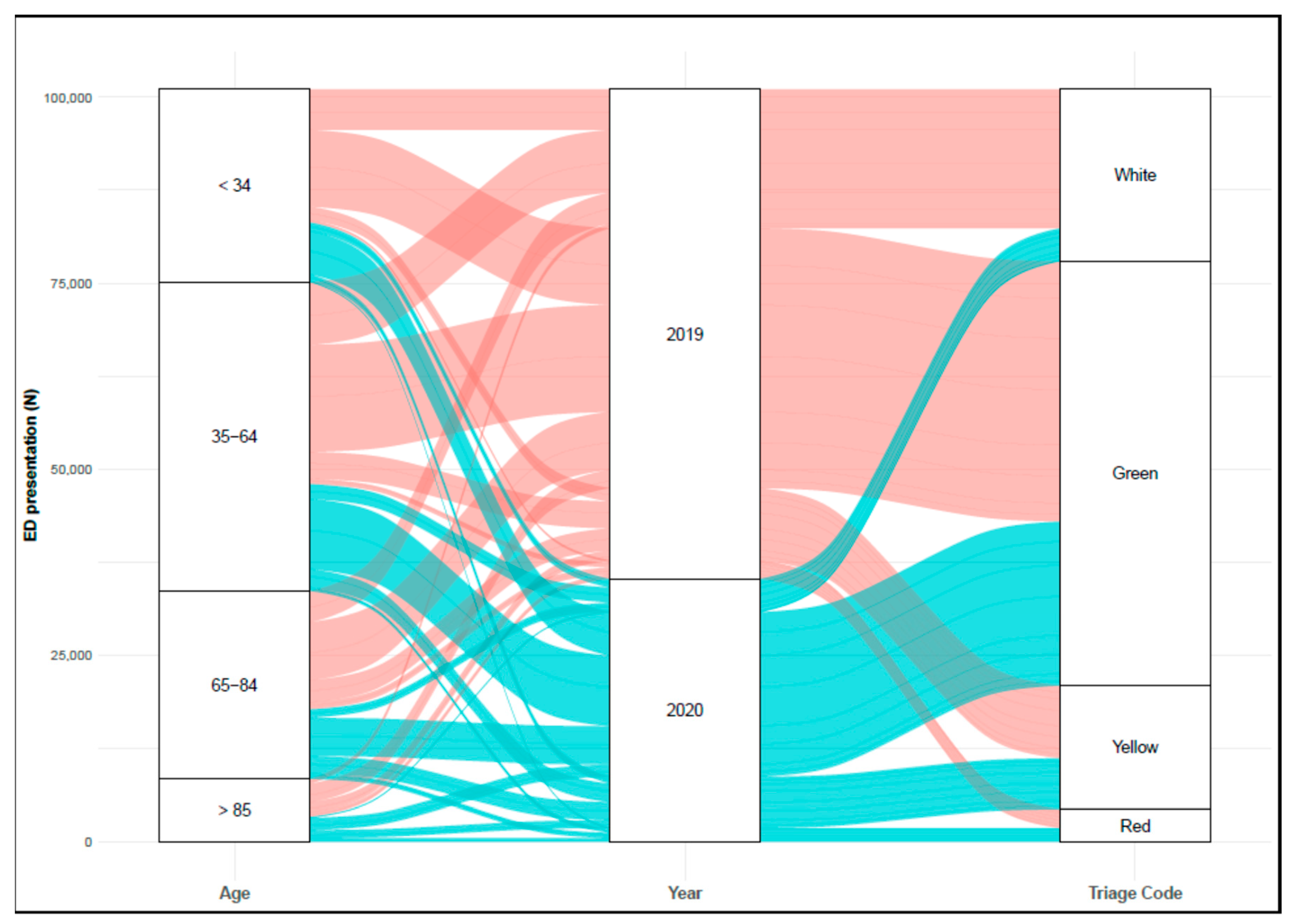
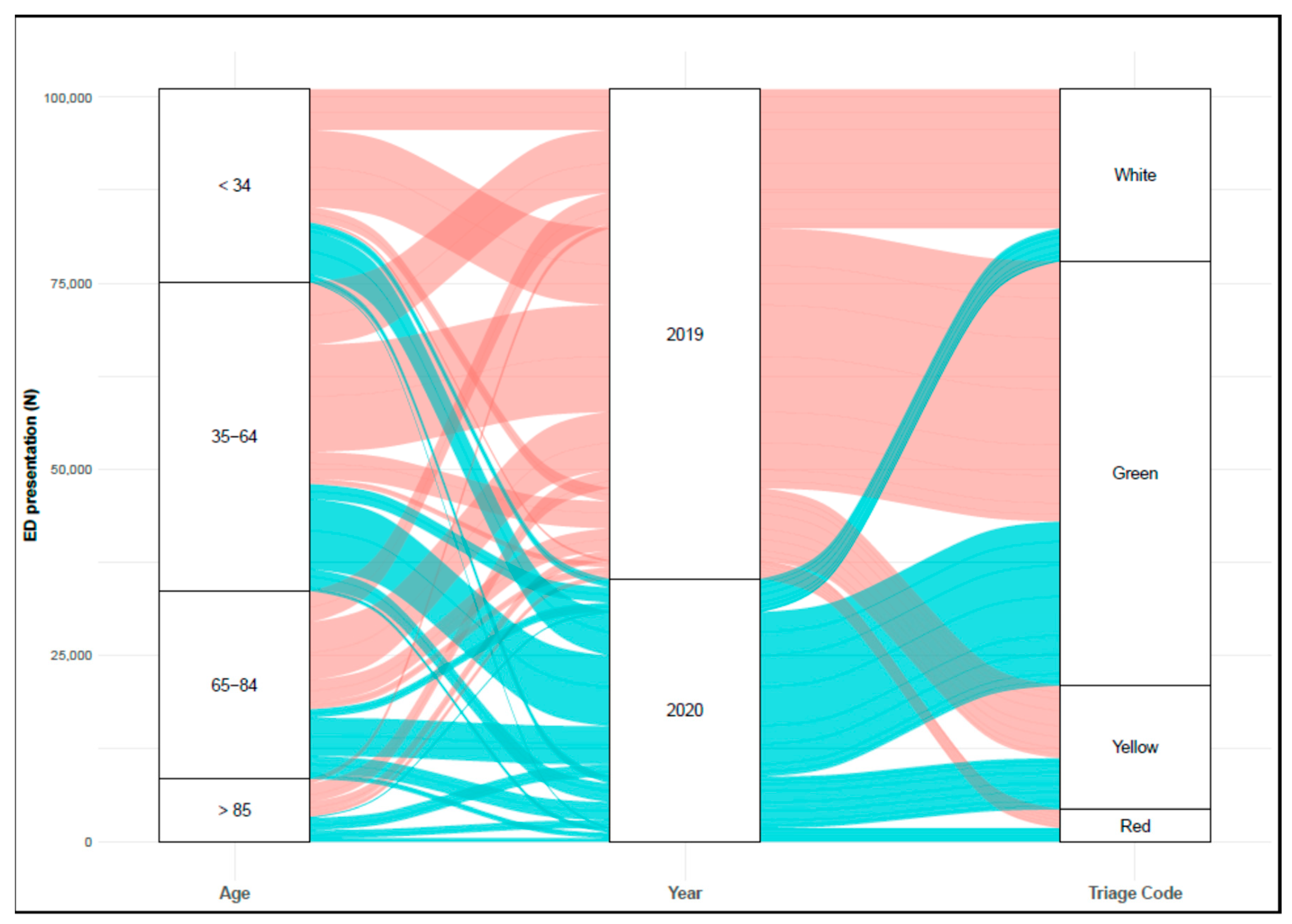
There were 35,249 ED presentations in our hospital in 2020, compared to 65,804 in 2019 (
Figure 1), which resulted in a reduction of 46.4%, and involved fewer females compared to the male population, 50.2% versus 42.5%, respectively.
Overall, the number of resulting hospital admissions were 7281 (11.1%) in 2019 compared to 6353 (18.0%) in 2020 (p < 0.001). Furthermore, we reported more deaths in our ED (192 versus 285) in 2020, which corresponds to a 0.5% difference in mortality (95% CI: 0.4 to 0.6%). The population visiting the ED in the 2020 period was older, 54.8 (21.4) versus 52.2 (21.4) years in 2019. Only people with minor trauma, abdominal or chest pain, and ear-nose-throat-related conditions did show a statistically significant variation in age between 2019 and 2020. Mean difference in age was, respectively, 1.2 (95% CI:0.4 to 2.0), 1.5 (95% CI:0.6 to 2.5), 1.5 (95% CI:0.3 to 2.8), and 1.8 (95% CI:0.7 to 2.9) years.
The top-10 reported conditions or symptoms in patients referred to the ED in 2019 are displayed in
Table 1.
Despite numbers being almost halved in 2020, it is interesting to note that the proportion of people presenting with chest pain was constant over time (i.e., 4% versus 3.9%), despite it affecting older individuals in 2020 compared to the previous year, +1.5 (95% CI: 0.3 to 2.8) years old. We also witnessed a lower proportion of people referred to ED for dermatologic and ophthalmologic conditions, ear-nose-throat-related issues, and single-arm pain. The number of people with dyspnea abruptly increased by 14.6%, without a clinically significant difference in age, −0.1 (95% CI −1.1 to 1.1) years.
Compared to 2019, it is worth noting that we also recorded a 0.5% (95% CI: 0.4 to 0.6) and 0.1% (95% CI: −0.01 to 0.1) increase in the number of discharge and abandonment cases in people presented with dyspnea, respectively.
Among the priority codes of access (i.e., triage codes), we recorded a −15.7% difference in the proportion of patients admitted with white codes in 2020. On the contrary, green, yellow, and red codes showed a positive difference of 9.5%, 4.7%, and 1.5%, respectively. Presentations with major urgency (i.e., yellow) in 2020 showed the greatest difference in age, +3.2 (95% CI: 2.5 to 3.8) years compared to 2019. Non-urgent conditions (i.e., white and green codes) represented 90.6% and 89.5% of people with other symptoms both in 2019 and 2020.
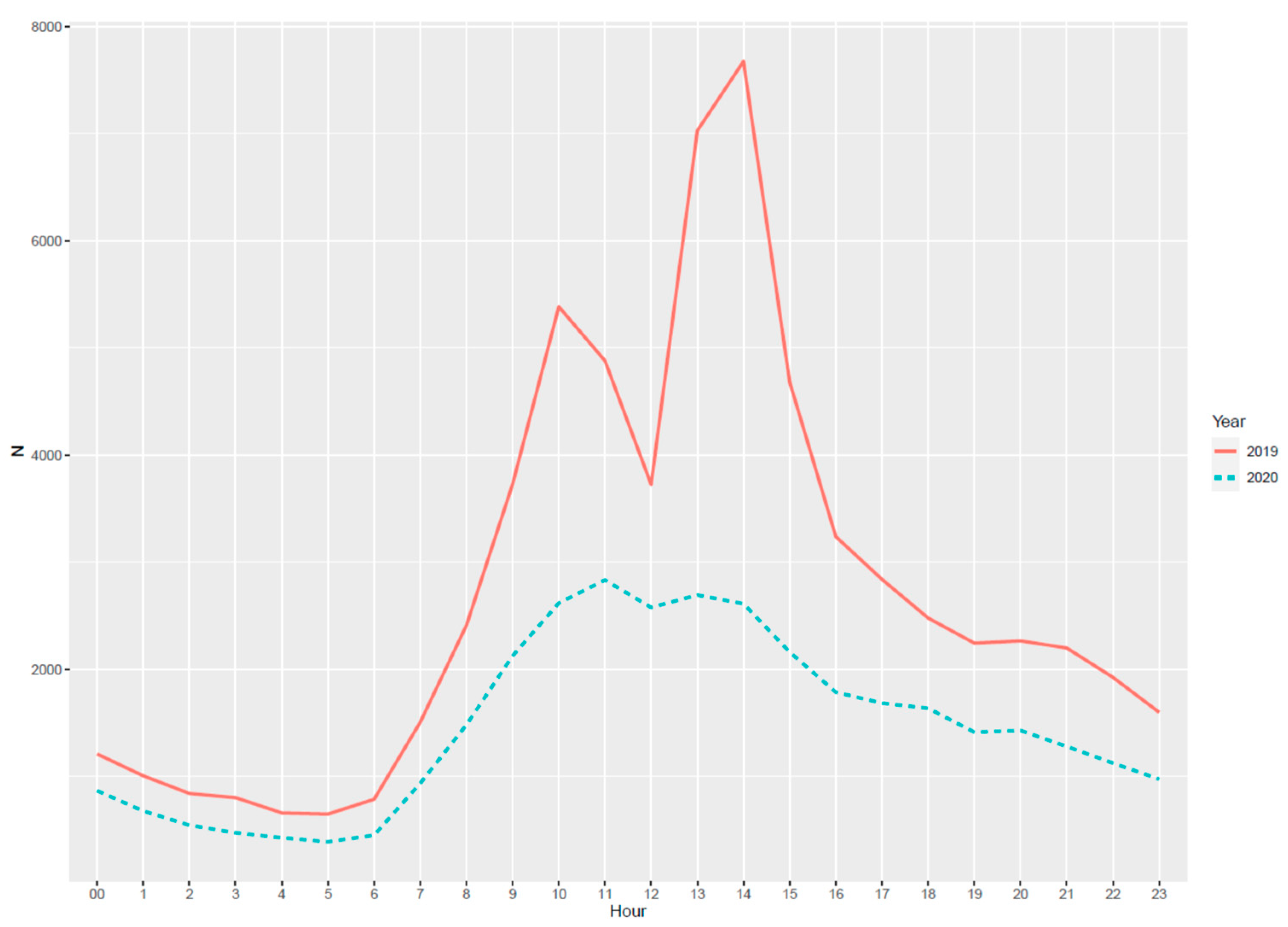
In terms of ED performance, overall median waiting time-to-visit decreased by 17 min (
p < 0.001) in 2020 compared to the year before. If we consider the time of ED presentation during the whole day, we reported the same pattern between the observed years (
Figure 2).
4. Discussion
This retrospective analysis supports other groups’ findings reporting a reduction in patients’ accesses to the ED [
5,
6], however, we cannot claim that COVID-19 dramatically changed the pattern of urgent visits to our ED. Over recent years, we have seen the ED becoming multi-professional outpatient clinics, where patients ask for timely interventions in response to the difficulties of access to general practitioner (GP) primary care and advanced examinations, usually subjected to long waitlists. The ED is quicker than getting an appointment with the GP, and there is all the medical expertise required to solve the perceived acuity of the condition.
Regarding the reduction in the number of ED presentations, it is likely that self-selection of inappropriate ED presentations occurred during the COVID-19 pandemic. Some people with deferrable conditions respected the stay-home recommendation for fear of contagion, and these might have presented with dermatologic, ophthalmologic, and single-arm pain-related issues. To this, we should also consider that some people decided to leave big cities and headed back to their native homes because of the pandemic, which exposed fewer people to noxious events. On the other hand, some others continued to seek medical attention, mostly because they felt it urgent. Indeed, minor traumatic injuries and pain were the most frequent reasons for showing up to the ED. Pain is strictly related to the perceived acuity and urgency of the condition, eliciting abnormal reactions at the emotional level, which requires immediate control. Media contributed to increasing the arousal level in the population about dyspnea, which was appointed as highly indicative for COVID-19.
Independently from the pandemic, the bottom line is that people decided to spend hours waiting for a visit in the ED during working daytime rather than going to their GP, as depicted in
Figure 2. In a metropolitan area like Milano, patients seeking emergency care should be expected during out-of-hours care when GP outpatients are closed. With a differential of 30,555 ED presentations in 2020, 88.6% were non-urgent visits.
Being aware that we are offering a partial perspective of a more complex phenomenon and that we relied on reasons for ED presentation based on patients’ reported symptoms, we wonder what future is planned for our hospitals within the current regional health system. As reported by Morello et al., ED overuse and overcrowding are phenomena that are not affordable [
7] and require specific interventions [
8]. To date, several strategies are available to improve the flow in the emergency department, such as the use of validated scores and the clinical judgment of the triage nurse [
9].
5. Conclusions
COVID-19 changed ED flows, likely causing an overall reduction in the number of deferrable conditions. However, the pattern for urgent conditions did not change abruptly in 2020. Potentiating territorial medicine and lower-acuity-care services would give back to EDs their role as hyper-specialistic places for urgent and emergency conditions rather than crowded outpatient services.
Author Contributions
Conceptualization, S.G. and D.L.; methodology, S.G. and O.P.; software, O.P. and P.B.; formal analysis, S.G.; investigation, O.P., A.G., F.B., and P.B.; resources, G.C. and D.L.; writing—original raft preparation, S.G., F.B., and A.G.; writing—review and editing, G.C. and D.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Data extraction did not involve the evaluation of individual medical records. Since the study focused on general ED flow analysis and was retrospective observational in nature, Ethics Committee approval is waived.
Informed Consent Statement
Informed consent was waived because the analysis used anonymous clinical data and did not involve the evaluation of individual medical records.
Data Availability Statement
Data are available from the authors upon reasonable request and with permission of Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Morelli, N.; Rota, E.; Terracciano, C.; Immovilli, P.; Spallazzi, M.; Colombi, D.; Zaino, D.; Michieletti, E.; Guidetti, D. The Baffling Case of Ischemic Stroke Disappearance from the Casualty Department in the COVID-19 Era. Eur. Neurol. 2020, 83, 213–215. [Google Scholar] [CrossRef] [PubMed]
- Campo, G.; Fortuna, D.; Berti, E.; De Palma, R.; Di Pasquale, G.; Galvani, M.; Navazio, A.; Piovaccari, G.; Rubboli, A.; Guardigli, G.; et al. In- and out-of-hospital mortality for myocardial infarction during the fi rst wave of the COVID-19 pandemic in Emilia-Romagna, Italy: A population-based observational study. Lancet Reg. Health-Eur. 2021, 3, 100055. [Google Scholar] [CrossRef]
- Alicandro, G.; La Vecchia, C.; Remuzzi, G.; Gerli, A.; Centanni, S. The impact of COVID-19 on total mortality in Italy up to November 2020. Panminerva Med. 2021. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing. 2019. Available online: https://www.r-project.org (accessed on 22 June 2021).
- Bellan, M.; Gavelli, F.; Hayden, E.; Patrucco, F.; Soddu, D.; Pedrinelli, A.R.; Cittone, M.G.; Rizzi, E.; Casciaro, G.F.; Vassia, V.; et al. Pattern of emergency department referral during the Covid-19 outbreak in Italy. Panminerva Med. 2020. [Google Scholar] [CrossRef]
- Ojetti, V.; Covino, M.; Brigida, M.; Petruzziello, C.; Saviano, A.; Migneco, A.; Candelli, M.; Franceschi, F. Non-COVID Diseases during the Pandemic: Where Have All Other Emergencies Gone? Medicina 2020, 56, 512. [Google Scholar] [CrossRef] [PubMed]
- Morello, F.; Bima, P.; Ferreri, E.; Chiarlo, M.; Balzaretti, P.; Tirabassi, G.; Petitti, P.; Aprà, F.; Vallino, D.; Carbone, G.; et al. After the first wave and beyond lockdown: Long-lasting changes in emergency department visit number, characteristics, diagnoses, and hospital admissions. Intern. Emerg. Med. 2021, 1–8. [Google Scholar] [CrossRef]
- Di Mauro, R.; Di Silvio, V.; Bosco, P.; Laquintana, D.; Galazzi, A. Case management programs in emergency department to reduce frequent user visits: A systematic review. Acta Biomed. 2019, 90, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Salvato, M.; Binda, F.; Iotti, M.; Bosco, P.; Laquintana, D. The prediction of hospitalization in triage: A comparison of instruments and methods of evaluation. A systematic revision. Assist. Inferm. Ric. AIR 2020, 39, 139–146. [Google Scholar] [PubMed]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 ,
, 

{kind=link}
{kind=link}