
Relationship between Respiratory Muscle Function and Postural Stability in Male Soccer Players: A Case-Control Study

 , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
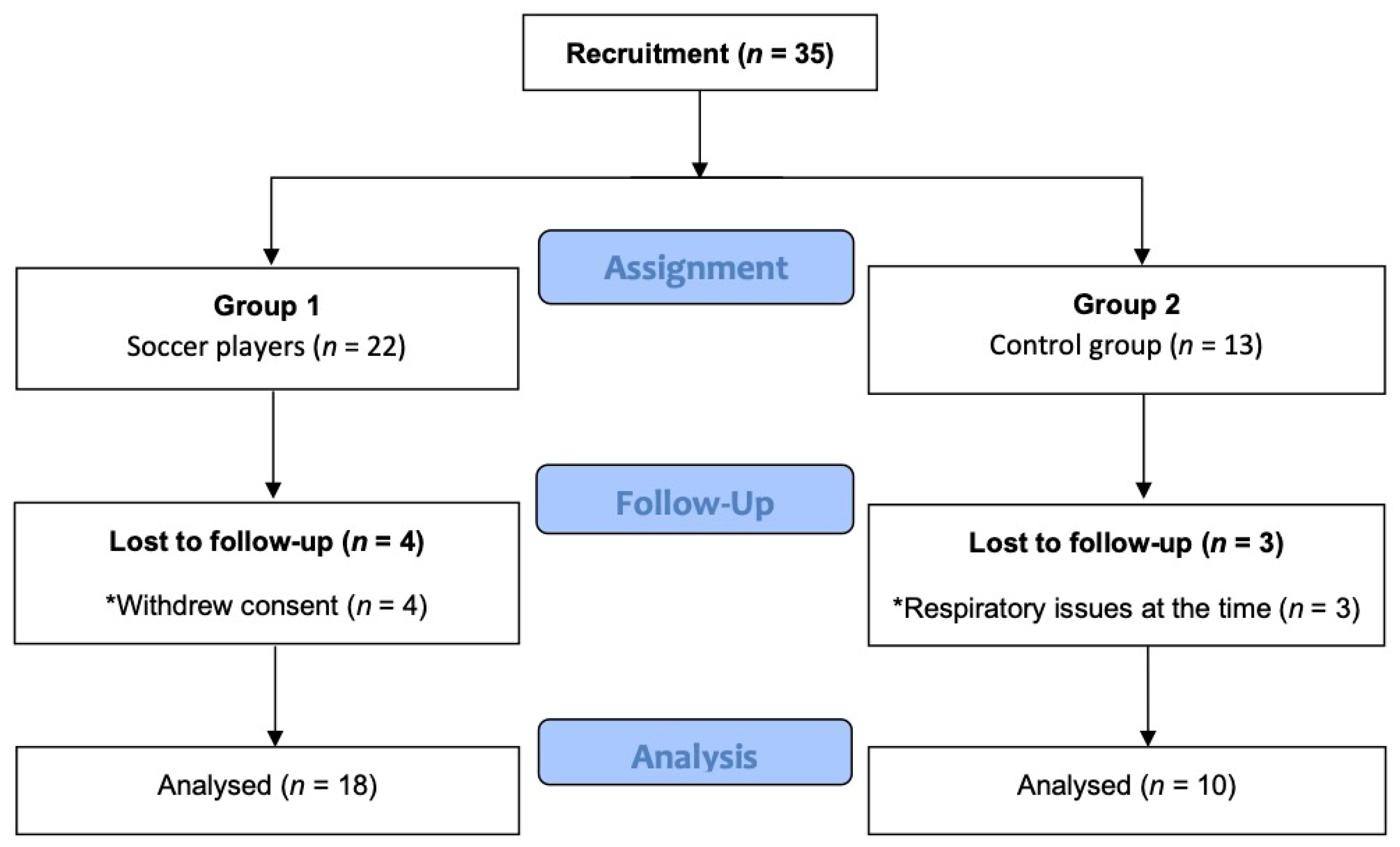
2.1. Study Design
2.2. Participants
2.3. Measurement Variables and Procedures
2.3.1. Respiratory Muscle Function
2.3.2. Stabilometric Variables
2.4. Statistical Analysis
3. Results
4. Discussion
4.1. Implications for Practice
4.2. Limitations and Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Winearls, J. Posture: Its function in efficient use of the human organism as a total concept. Agressologie 1972, 13 (Suppl. B), 99-1. [Google Scholar]
- Paillard, T. Relationship between sport expertise and postural skills. Front. Psychol. 2019, 10, 25. [Google Scholar] [CrossRef] [PubMed]
- Orchard, J. Is there a relationship between ground and climatic conditions and injuries in football? Sport. Med. 2002, 32, 419–432. [Google Scholar] [CrossRef] [PubMed]
- Gerbino, P.G.; Griffin, E.D.; Zurakowski, D. Comparison of standing balance between female collegiate dancers and soccer players. Gait Posture 2007, 26, 501–507. [Google Scholar] [CrossRef]
- Hamaoui, A.; Gonneau, E.; Le Bozec, S. Respiratory disturbance to posture varies according to the respiratory mode. Neurosci. Lett. 2010, 475, 141–144. [Google Scholar] [CrossRef]
- Hamaoui, A.; Hudson, A.L.; Laviolette, L.; Nierat, M.C.; Do, M.C.; Similowski, T. Postural disturbances resulting from unilateral and bilateral diaphragm contractions: A phrenic nerve stimulation study. J. Appl. Physiol. 2014, 117, 825–832. [Google Scholar] [CrossRef]
- Stephens, R.J.; Haas, M.; Moore, W.L.; Emmil, J.R.; Sipress, J.A.; Williams, A. Effects of Diaphragmatic Breathing Patterns on Balance: A Preliminary Clinical Trial. J. Manip. Physiol. Ther. 2017, 40, 169–175. [Google Scholar] [CrossRef]
- Gurfinkel’, V.S.; Kireeva, T.B.; Lebik, I.S. Effect of postural muscle vibration on equilibrium maintenance in the frontal plane at various levels of stability. Fiziol. Cheloveka 1996, 22, 83–92. [Google Scholar]
- Goldie, P.A.; Bach, T.M.; Evans, O.M. Force platform measures for evaluating postural control: Reliability and validity. Arch. Phys. Med. Rehabil. 1989, 70, 510–517. [Google Scholar]
- Demura, S.; Yamaji, S.; Kitabayashi, T.; Yamada, T.; Uchiyama, M. Attention of postural control on foot somatosensor disturbance caused by the compression of blood vessels. J. Hum. Ergol. 2008, 37, 91–102. [Google Scholar]
- Fujiwara, K.; Asai, H.; Miyaguchi, A.; Toyama, H.; Kunita, K.; Inoue, K. Perceived standing position after reduction of foot-pressure sensation by cooling the sole. Percept. Mot. Skills 2003, 96, 381–399. [Google Scholar] [CrossRef]
- Caron, O.; Fontanari, P.; Cremieux, J.; Joulia, F. Effects of ventilation on body sway during human standing. Neurosci. Lett. 2004, 366, 6–9. [Google Scholar] [CrossRef]
- Malakhov, M.; Makarenkova, E.; Melnikov, A. The influence of different modes of ventilation on standing balance of athletes. Asian J. Sports Med. 2014, 5, 22767. [Google Scholar] [CrossRef] [PubMed]
- Hodges, P.W.; Butler, J.E.; McKenzie, D.K.; Gandevia, S.C. Contraction of the human diaphragm during rapid postural adjustments. J. Physiol. 1997, 505, 539–548. [Google Scholar] [CrossRef]
- Hodges, P.W.; Gandevia, S.C. Activation of the human diaphragm during a repetitive postural task. J. Physiol. 2000, 522, 165–175. [Google Scholar] [CrossRef] [PubMed]
- Kocjan, J.; Adamek, M.; Gzik-Zroska, B.; Czyżewski, D.; Rydel, M. Network of breathing. Multifunctional role of the diaphragm: A review. Adv. Respir. Med. 2017, 85, 224–232. [Google Scholar] [CrossRef] [PubMed]
- Bordoni, B.; Zanier, E. Anatomic connections of the diaphragm: Influence of respiration on the body system. J. Multidiscip. Healthc. 2013, 6, 281–291. [Google Scholar] [CrossRef]
- Hodges, P.W.; Heijnen, I.; Gandevia, S.C. Postural activity of the diaphragm is reduced in humans when respiratory demand increases. J. Physiol. 2001, 537, 999–1008. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.; Park, D.; Lee, G.C. Progressive Respiratory Muscle Training for Improving Trunk Stability in Chronic Stroke Survivors: A Pilot Randomized Controlled Trial. J. Stroke Cerebrovasc. Dis. 2019, 28, 1200–1211. [Google Scholar] [CrossRef]
- Penafortes, J.T.S.; Guimarães, F.S.; Moço, V.J.R.; Almeida, V.P.; Menezes, S.L.S.; Lopes, A.J. Relationship between body balance, lung function, nutritional status and functional capacity in adults with cystic fibrosis. Braz. J. Phys. Ther. 2013, 17, 450–457. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Ann. Intern. Med. 2007, 147, 573–577. [Google Scholar] [CrossRef]
- Nici, L.; Donner, C.; Wouters, E.; Zuwallack, R.; Ambrosino, N.; Bourbeau, J.; Carone, M.; Celli, B.; Engelen, M.; Fahy, B.; et al. American thoracic society/European respiratory society statement on pulmonary rehabilitation. Am. J. Respir. Crit. Care Med. 2006, 173, 1390–1413. [Google Scholar] [CrossRef]
- Romero-Franco, N.; Martínez-Lopez, E.J.; Lomas-Vega, R.; Hita-Contreras, F.; Osuna-Perez, M.C.; Martínez-Amat, A. Short-term effects of proprioceptive training with unstable platform on athletes’ stabilometry. J. Strength Cond. Res. 2013, 27, 2189–2197. [Google Scholar] [CrossRef] [PubMed]
- Hrysomallis, C. Balance ability and athletic performance. Sport. Med. 2011, 41, 221–232. [Google Scholar] [CrossRef]
- Romero-Franco, N.; Gallego-Izquierdo, T.; Martínez-López, E.J.; Hita-Contreras, F.; Osuna-Pérez, M.C.; Martínez-Amat, A. Postural stability and subsequent sports injuries during indoor season of athletes. J. Phys. Ther. Sci. 2014, 26, 683–687. [Google Scholar] [CrossRef]
- Kocjan, J.; Gzik-Zroska, B.; Nowakowska, K.; Burkacki, M.; Suchoń, S.; Michnik, R.; Czyżewski, D.; Adamek, M. Impact of diaphragm function parameters on balance maintenance. PLoS ONE 2018, 13, e0208697. [Google Scholar] [CrossRef] [PubMed]
- Sakellari, V.; Bronstein, A.M. Hyperventilation effect on postural sway. Arch. Phys. Med. Rehabil. 1997, 78, 730–736. [Google Scholar] [CrossRef]
- Sakellari, V.; Bronstein, A.M.; Corna, S.; Hammon, C.A.; Jones, S.; Wolsley, C.J. The effects of hyperventilation on postural control mechanisms. Brain 1997, 120, 1659–1673. [Google Scholar] [CrossRef] [PubMed]
- Jadczak, Ł.; Grygorowicz, M.; Dzudziński, W.; Śliwowski, R. Comparison of Static and Dynamic Balance at Different Levels of Sport Competition in Professional and Junior Elite Soccer Players. J. Strength Cond. Res. 2019, 33, 3384–3391. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Soccer (n = 18) | Control (n = 10) | p |
|---|---|---|---|
| Age (years) | 20.28 ± 0.89 | 22.70 ± 4.29 | 0.11 |
| Weight (Kg) | 73.90 ± 6.49 | 75.32 ± 8.38 | 0.62 |
| Height (m) | 178.16 ± 4.90 | 177.10 ± 6.93 | 0.63 |
| MIP (cmH2O) | 163.88 ± 33.20 | 138.40 ± 28.87 | 0.05 |
| MIP (%pred) | 105.69 ± 22.20 | 90.33 ± 19.23 | 0.07 |
| MVV (liters) | 194.49 ± 23.44 | 184.64 ± 23.23 | 0.29 |
| MVV (bpm) | 99.37 ± 33.45 | 175.74 ± 26.38 | <0.001 |
| OE_length (mm) | 3803.09 ± 1608.33 | 3308.13 ± 434.95 | 0.35 |
| OE_area (mm2) | 138.61 ± 106.38 | 337.63 ± 484.51 | 0.23 |
| OE_X range (mm) | 12.59 ± 6.03 | 14.78 ± 11.53 | 0.51 |
| OE_Y range (mm) | 14.21 ± 5.93 | 14.97 ± 7.04 | 0.76 |
| CE_length (mm) | 4028.74 ± 1552.15 | 3836.40 ± 642.72 | 0.71 |
| CE_area (mm2) | 111.54 ± 105.58 | 78.59 ± 67.65 | 0.38 |
| CE_X range (mm) | 11.58 ± 4.70 | 11.85 ± 5.29 | 0.89 |
| CE_Y range (mm) | 14.02 ± 6.87 | 14.52 ± 6.86 | 0.85 |
| Variables | Trials | MIP (cmH20) | MIP (% pred) | MVV (l) | MVV (bpm) | ||||
|---|---|---|---|---|---|---|---|---|---|
| Soccer | Control | Soccer | Control | Soccer | Control | Soccer | Control | ||
| Area (mm2) | OE | −0.090 | −0.175 | −0.110 | −0.055 | 0.224 | −0.255 | 0.372 | 0.279 |
| CE | −0.106 | −0.108 | −0.093 | −0.035 | 0.118 | 0.013 | 0.422 | 0.343 | |
| Length (mm) | OE | −0.215 | 0.424 | −0.190 | 0.428 | 0.146 | −0.150 | 0.606 ** | −0.538 |
| CE | −0.535 * | −0.040 | −0.585 * | −0.167 | 0.318 | −0.180 | 0.465 | −0.570 | |
| X range (mm) | OE | 0.233 | 0.424 | 0.255 | 0.405 | 0.125 | −0.093 | 0.127 | −0.423 |
| CE | −0.527 * | 0.200 | −0.560 * | 0.073 | 0.403 | −0.261 | 0.295 | −0.306 | |
| Y range (mm) | OE | −0.290 | 0.155 | −0.304 | 0.137 | 0.231 | −0.507 | 0.558 * | 0.000 |
| CE | −0.223 | −0.110 | −0.308 | −0.245 | 0.259 | −0.207 | 0.196 | −0.516 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
León-Morillas, F.; Lozano-Quijada, C.; Lérida-Ortega, M.Á.; León-Garzón, M.C.; Ibáñez-Vera, A.J.; de Oliveira-Sousa, S.L. Relationship between Respiratory Muscle Function and Postural Stability in Male Soccer Players: A Case-Control Study. Healthcare 2021, 9, 644. https://doi.org/10.3390/healthcare9060644
León-Morillas F, Lozano-Quijada C, Lérida-Ortega MÁ, León-Garzón MC, Ibáñez-Vera AJ, de Oliveira-Sousa SL. Relationship between Respiratory Muscle Function and Postural Stability in Male Soccer Players: A Case-Control Study. Healthcare. 2021; 9(6):644. https://doi.org/10.3390/healthcare9060644
Chicago/Turabian StyleLeón-Morillas, Felipe, Carlos Lozano-Quijada, Miguel Ángel Lérida-Ortega, Martha Cecilia León-Garzón, Alfonso Javier Ibáñez-Vera, and Silvana Loana de Oliveira-Sousa. 2021. "Relationship between Respiratory Muscle Function and Postural Stability in Male Soccer Players: A Case-Control Study" Healthcare 9, no. 6: 644. https://doi.org/10.3390/healthcare9060644
APA StyleLeón-Morillas, F., Lozano-Quijada, C., Lérida-Ortega, M. Á., León-Garzón, M. C., Ibáñez-Vera, A. J., & de Oliveira-Sousa, S. L. (2021). Relationship between Respiratory Muscle Function and Postural Stability in Male Soccer Players: A Case-Control Study. Healthcare, 9(6), 644. https://doi.org/10.3390/healthcare9060644