
Systematic Review of Sleep Characteristics in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome

 ,
, 

{kind=link}
Abstract
1. Introduction
2. Methods
2.1. Inclusion/ Exclusion Criteria
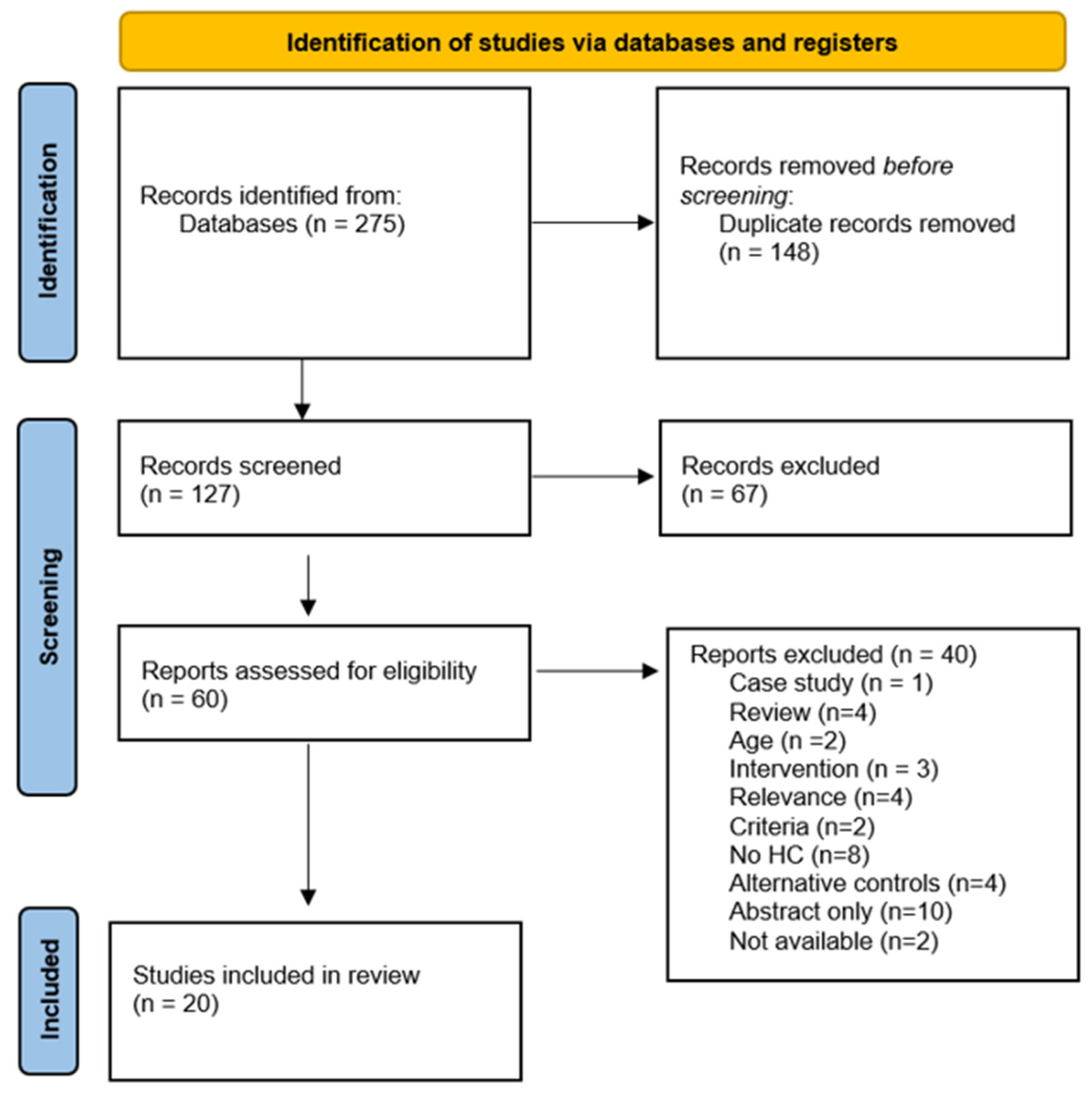
2.2. Selection of Studies
2.3. Data Extraction
2.4. Quality Analysis
3. Results
3.1. Participant and Study Characteristics
3.2. Literature Reporting Changes in Objective Sleep Measures
3.3. Literature Reporting Changes in Spectral Activity
3.4. Literature Reporting Changes in MSLT
3.5. Literature Reporting Changes in Secondary Outcomes
3.6. Quality Assessment
4. Discussion
Quality Assessment
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Carruthers, B.M.; Van de Sande, M.I.; De Meirleir, K.L.; Klimas, N.G.; Broderick, G.; Mitchell, T.; Staines, D.; Powles, A.C.P.; Speight, N.; Vallings, R.; et al. Myalgic Encephalomyelitis: International Consensus Criteria. J. Intern. Med. 2011, 270, 327–338. [Google Scholar] [CrossRef] [PubMed]
- Nisenbaum, R.; Jones, J.F.; Unger, E.R.; Reyes, M.; Reeves, W.C. A Population-Based Study of the Clinical Course of Chronic Fatigue Syndrome. Health Qual. Life Outcomes 2003, 1, 49. [Google Scholar] [CrossRef] [PubMed]
- Eaton-Fitch, N.; Johnston, S.C.; Zalewski, P.; Staines, D.; Marshall-Gradisnik, S. Health-Related Quality of Life in Patients with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: An Australian Cross-Sectional Study. Qual. Life Res. 2020, 29, 1521–1531. [Google Scholar] [CrossRef] [PubMed]
- Committee on the Diagnostic Criteria for Myalgic Encephalomyelitis/Chronic Fatigue Syndrome; Board on the Health of Select Populations; Institute of Medicine. Beyond Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Redefining an Illness; The National Academies Collection: Reports funded by National Institutes of Health; National Academies Press (US): Washington, DC, USA, 2015; ISBN 978-0-309-31689-7. [Google Scholar]
- Fukuda, K.; Straus, S.E.; Hickie, I.; Sharpe, M.C.; Dobbins, J.G.; Komaroff, A. The Chronic Fatigue Syndrome: A Comprehensive Approach to Its Definition and Study. International Chronic Fatigue Syndrome Study Group. Ann. Intern. Med. 1994, 121, 953–959. [Google Scholar] [CrossRef]
- Carruthers, B.M.; Jain, A.K.; Meirleir, K.L.D.; Peterson, D.L.; Klimas, N.G.; Lerner, A.M.; Bested, A.C.; Flor-Henry, P.; Joshi, P.; Powles, A.C.P.; et al. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. J. Chronic Fatigue Syndr. 2003, 11, 7–115. [Google Scholar] [CrossRef]
- Jackson, M.L.; Bruck, D. Sleep Abnormalities in Chronic Fatigue Syndrome/Myalgic Encephalomyelitis: A Review. J. Clin. Sleep Med. JCSM Off. Publ. Am. Acad. Sleep Med. 2012, 8, 719–728. [Google Scholar] [CrossRef]
- Purves, D.; Augustine, G.J.; Fitzpatrick, D.; Katz, L.C.; LaMantia, A.-S.; McNamara, J.O.; Williams, S.M. Stages of Sleep. Available online: https://www.ncbi.nlm.nih.gov/books/NBK10996/ (accessed on 11 May 2021).
- Gotts, Z.M.; Deary, V.; Newton, J.L.; Ellis, J.G. A Comparative Polysomnography Analysis of Sleep in Healthy Controls and Patients with Chronic Fatigue Syndrome. Fatigue Biomed. Health Behav. 2016, 4, 80–93. [Google Scholar] [CrossRef]
- Shrivastava, D.; Jung, S.; Saadat, M.; Sirohi, R.; Crewson, K. How to Interpret the Results of a Sleep Study. J. Community Hosp. Intern. Med. Perspect. 2014, 4. [Google Scholar] [CrossRef]
- Arand, D.L.; Bonnet, M.H. Chapter 26—The multiple sleep latency test. In Handbook of Clinical Neurology; Levin, K.H., Chauvel, P., Eds.; Clinical Neurophysiology: Basis and Technical Aspects; Elsevier: Amsterdam, The Netherlands, 2019; Volume 160, pp. 393–403. [Google Scholar]
- Chapter 4: Searching for and Selecting Studies. Available online: /handbook/current/chapter-04 (accessed on 14 December 2020).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Neu, D.; Mairesse, O.; Montana, X.; Gilson, M.; Corazza, F.; Lefevre, N.; Linkowski, P.; Le Bon, O.; Verbanck, P. Dimensions of Pure Chronic Fatigue: Psychophysical, Cognitive and Biological Correlates in the Chronic Fatigue Syndrome. Eur. J. Appl. Physiol. 2014, 114, 1841–1851. [Google Scholar] [CrossRef]
- Armitage, R.; Landis, C.; Hoffmann, R.; Lentz, M.; Watson, N.; Goldberg, J.; Buchwald, D. Power Spectral Analysis of Sleep EEG in Twins Discordant for Chronic Fatigue Syndrome. J. Psychosom. Res. 2009, 66, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Ball, N.; Buchwald, D.S.; Schmidt, D.; Goldberg, J.; Ashton, S.; Armitage, R. Monozygotic Twins Discordant for Chronic Fatigue Syndrome: Objective Measures of Sleep. J. Psychosom. Res. 2004, 56, 207–212. [Google Scholar] [CrossRef]
- Watson, N.F.; Kapur, V.; Arguelles, L.M.; Goldberg, J.; Schmidt, D.F.; Armitage, R.; Buchwald, D. Comparison of Subjective and Objective Measures of Insomnia in Monozygotic Twins Discordant for Chronic Fatigue Syndrome. Sleep 2003, 26, 324–328. [Google Scholar] [CrossRef] [PubMed]
- Watson, N.F.; Jacobsen, C.; Goldberg, J.; Kapur, V.; Buchwald, D. Subjective and Objective Sleepiness in Monozygotic Twins Discordant for Chronic Fatigue Syndrome. Sleep 2004, 27, 973–977. [Google Scholar] [CrossRef]
- Majer, M.; Jones, J.F.; Unger, E.R.; Youngblood, L.S.; Decker, M.J.; Gurbaxani, B.; Heim, C.; Reeves, W.C. Perception versus Polysomnographic Assessment of Sleep in CFS and Non-Fatigued Control Subjects: Results from a Population-Based Study. BMC Neurol. 2007, 7, 40. [Google Scholar] [CrossRef]
- Decker, M.J.; Tabassum, H.; Lin, J.-M.S.; Reeves, W.C. Electroencephalographic Correlates of Chronic Fatigue Syndrome. Behav. Brain Funct. BBF 2009, 5, 43. [Google Scholar] [CrossRef]
- Le Bon, O.; Neu, D.; Valente, F.; Linkowski, P. Paradoxical NREMS Distribution in “Pure” Chronic Fatigue Patients a Comparison with Sleep Apnea-Hypopnea Patients and Healthy Control Subjects. J. Chronic Fatigue Syndr. 2008, 14, 45–59. [Google Scholar] [CrossRef]
- Le Bon, O.; Neu, D.; Berquin, Y.; Lanquart, J.-P.; Hoffmann, R.; Mairesse, O.; Armitage, R. Ultra-Slow Delta Power in Chronic Fatigue Syndrome. Psychiatry Res. 2012, 200, 742–747. [Google Scholar] [CrossRef]
- Neu, D.; Hoffmann, G.; Moutrier, R.; Verbanck, P.; Linkowski, P.; Le Bon, O. Are Patients with Chronic Fatigue Syndrome Just “tired” or Also “Sleepy”? J. Sleep Res. 2008, 17, 427–431. [Google Scholar] [CrossRef]
- Neu, D.; Mairesse, O.; Verbanck, P.; Linkowski, P.; Le Bon, O. Non-REM Sleep EEG Power Distribution in Fatigue and Sleepiness. J. Psychosom. Res. 2014, 76, 286–291. [Google Scholar] [CrossRef]
- Neu, D.; Mairesse, O.; Verbanck, P.; Le Bon, O. Slow Wave Sleep in the Chronically Fatigued: Power Spectra Distribution Patterns in Chronic Fatigue Syndrome and Primary Insomnia. Clin. Neurophysiol. Off. J. Int. Fed. Clin. Neurophysiol. 2015, 126, 1926–1933. [Google Scholar] [CrossRef] [PubMed]
- Reeves, W.C.; Heim, C.; Maloney, E.M.; Youngblood, L.S.; Unger, E.R.; Decker, M.J.; Jones, J.F.; Rye, D.B. Sleep Characteristics of Persons with Chronic Fatigue Syndrome and Non-Fatigued Controls: Results from a Population-Based Study. BMC Neurol. 2006, 6, 41. [Google Scholar] [CrossRef] [PubMed]
- Togo, F.; Natelson, B.H. Heart Rate Variability during Sleep and Subsequent Sleepiness in Patients with Chronic Fatigue Syndrome. Auton. Neurosci. Basic Clin. 2013, 176, 85–90. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Togo, F.; Natelson, B.H.; Cherniack, N.S.; FitzGibbons, J.; Garcon, C.; Rapoport, D.M. Sleep Structure and Sleepiness in Chronic Fatigue Syndrome with or without Coexisting Fibromyalgia. Arthritis Res. Ther. 2008, 10, R56. [Google Scholar] [CrossRef]
- Sharpley, A.; Clements, A.; Hawton, K.; Sharpe, M. Do Patients with “Pure” Chronic Fatigue Syndrome (Neurasthenia) Have Abnormal Sleep? Psychosom. Med. 1997, 59, 592–596. [Google Scholar] [CrossRef]
- Kishi, A.; Struzik, Z.R.; Natelson, B.H.; Togo, F.; Yamamoto, Y. Dynamics of Sleep Stage Transitions in Healthy Humans and Patients with Chronic Fatigue Syndrome. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2008, 294, R1980–R1987. [Google Scholar] [CrossRef]
- Neu, D.; Mairesse, O.; Hoffmann, G.; Dris, A.; Lambrecht, L.J.; Linkowski, P.; Verbanck, P.; Le Bon, O. Sleep Quality Perception in the Chronic Fatigue Syndrome: Correlations with Sleep Efficiency, Affective Symptoms and Intensity of Fatigue. Neuropsychobiology 2007, 56, 40–46. [Google Scholar] [CrossRef]
- Bileviciute-Ljungar, I.; Friberg, D. Emotional Awareness Correlated With Number of Awakenings From Polysomnography in Patients With Myalgic Encephalomyelitis/Chronic Fatigue Syndrome—A Pilot Study. Front. Psychiatry 2020, 11. [Google Scholar] [CrossRef]
- Maksoud, R.; Preez, S.d.; Eaton-Fitch, N.; Thapaliya, K.; Barnden, L.; Cabanas, H.; Staines, D.; Marshall-Gradisnik, S. A Systematic Review of Neurological Impairments in Myalgic Encephalomyelitis/ Chronic Fatigue Syndrome Using Neuroimaging Techniques. PLoS ONE 2020, 15, e0232475. [Google Scholar] [CrossRef]
- Prins, J.B.; van der Meer, J.W.; Bleijenberg, G. Chronic Fatigue Syndrome. Lancet 2006, 367, 346–355. [Google Scholar] [CrossRef]
- Chu, L.; Valencia, I.J.; Garvert, D.W.; Montoya, J.G. Onset Patterns and Course of Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Front. Pediatr. 2019, 7. [Google Scholar] [CrossRef] [PubMed]
- Collin, S.M.; Nuevo, R.; Putte, E.M.v.d.; Nijhof, S.L.; Crawley, E. Chronic Fatigue Syndrome (CFS) or Myalgic Encephalomyelitis (ME) Is Different in Children Compared to in Adults: A Study of UK and Dutch Clinical Cohorts. BMJ Open 2015, 5, e008830. [Google Scholar] [CrossRef] [PubMed]
- Stores, G.; Fry, A.; Crawford, C. Sleep Abnormalities Demonstrated by Home Polysomnography in Teenagers with Chronic Fatigue Syndrome. J. Psychosom. Res. 1998, 45, 85–91. [Google Scholar] [CrossRef]
- Van de Water, A.T.M.; Holmes, A.; Hurley, D.A. Objective Measurements of Sleep for Non-Laboratory Settings as Alternatives to Polysomnography--a Systematic Review. J. Sleep Res. 2011, 20, 183–200. [Google Scholar] [CrossRef] [PubMed]
- Fatt, S.J.; Beilharz, J.E.; Joubert, M.; Wilson, C.; Lloyd, A.R.; Vollmer-Conna, U.; Cvejic, E. Parasympathetic Activity Is Reduced during Slow-Wave Sleep, but Not Resting Wakefulness, in Patients with Chronic Fatigue Syndrome. J. Clin. Sleep Med. JCSM Off. Publ. Am. Acad. Sleep Med. 2020, 16, 19–28. [Google Scholar] [CrossRef]
- Neu, D.; Kajosch, H.; Peigneux, P.; Verbanck, P.; Linkowski, P.; Le Bon, O. Cognitive Impairment in Fatigue and Sleepiness Associated Conditions. Psychiatry Res. 2011, 189, 128–134. [Google Scholar] [CrossRef]
- Neu, D.; Cappeliez, B.; Hoffmann, G.; Verbanck, P.; Linkowski, P.; Le Bon, O. High Slow-Wave Sleep and Low-Light Sleep: Chronic Fatigue Syndrome Is Not Likely to Be a Primary Sleep Disorder. J. Clin. Neurophysiol. Off. Publ. Am. Electroencephalogr. Soc. 2009, 26, 207–212. [Google Scholar] [CrossRef]
- Çetin, B.; Sünbül, E.A.; Toktaş, H.; Karaca, M.; Ulutaş, Ö.; Güleç, H. Comparison of Sleep Structure in Patients with Fibromyalgia and Healthy Controls. Sleep Breath. Schlaf Atm. 2020. [Google Scholar] [CrossRef]
- Bigatti, S.M.; Hernandez, A.M.; Cronan, T.A.; Rand, K.L. Sleep Disturbances in Fibromyalgia Syndrome: Relationship to Pain and Depression. Arthritis Rheum. 2008, 59, 961–967. [Google Scholar] [CrossRef]
- Wang, B.; Duan, R.; Duan, L. Prevalence of Sleep Disorder in Irritable Bowel Syndrome: A Systematic Review with Meta-Analysis. Saudi J. Gastroenterol. Off. J. Saudi Gastroenterol. Assoc. 2018, 24, 141–150. [Google Scholar] [CrossRef]
- Ghorbani, S.; Nejad, A.; Law, D.; Chua, K.S.; Amichai, M.M.; Pimentel, M. Healthy Control Subjects Are Poorly Defined in Case-Control Studies of Irritable Bowel Syndrome. Ann. Gastroenterol. Q. Publ. Hell. Soc. Gastroenterol. 2015, 28, 87–93. [Google Scholar]
- Newell, J.; Mairesse, O.; Verbanck, P.; Neu, D. Is a One-Night Stay in the Lab Really Enough to Conclude? First-Night Effect and Night-to-Night Variability in Polysomnographic Recordings among Different Clinical Population Samples. Psychiatry Res. 2012, 200, 795–801. [Google Scholar] [CrossRef]
- Le Bon, O.; Minner, P.; Van Moorsel, C.; Hoffmann, G.; Gallego, S.; Lambrecht, L.; Pelc, I.; Linkowski, P. First-Night Effect in the Chronic Fatigue Syndrome. Psychiatry Res. 2003, 120, 191–199. [Google Scholar] [CrossRef]
- Miller, S.C.; Pandi, P.S.R.; Esquifino, A.I.; Cardinali, D.P.; Maestroni, G.J.M. The Role of Melatonin in Immuno-Enhancement: Potential Application in Cancer. Int. J. Exp. Pathol. 2006, 87, 81–87. [Google Scholar] [CrossRef]
- Eaton-Fitch, N.; Du Preez, S.; Cabanas, H.; Staines, D.; Marshall-Gradisnik, S. A Systematic Review of Natural Killer Cells Profile and Cytotoxic Function in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Syst. Rev. 2019, 8. [Google Scholar] [CrossRef] [PubMed]
- Van Hoof, E.; De Becker, P.; Lapp, C.; Cluydts, R.; De Meirleir, K. Defining the Occurrence and Influence of Alpha-Delta Sleep in Chronic Fatigue Syndrome. Am. J. Med. Sci. 2007, 333, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Armitage, R.; Landis, C.; Hoffmann, R.; Lentz, M.; Watson, N.F.; Goldberg, J.; Buchwald, D. The Impact of a 4-Hour Sleep Delay on Slow Wave Activity in Twins Discordant for Chronic Fatigue Syndrome. Sleep 2007, 30, 657–662. [Google Scholar] [CrossRef] [PubMed]
- Kishi, A.; Togo, F.; Cook, D.B.; Klapholz, M.; Yamamoto, Y.; Rapoport, D.M.; Natelson, B.H. The Effects of Exercise on Dynamic Sleep Morphology in Healthy Controls and Patients with Chronic Fatigue Syndrome. Physiol. Rep. 2013, 1, e00152. [Google Scholar] [CrossRef]
- Light, A.R.; Bateman, L.; Jo, D.; Hughen, R.W.; Vanhaitsma, T.A.; White, A.T.; Light, K.C. Gene Expression Alterations at Baseline and Following Moderate Exercise in Patients with Chronic Fatigue Syndrome and Fibromyalgia Syndrome. J. Intern. Med. 2012, 271, 64–81. [Google Scholar] [CrossRef]
- Libman, E.; Creti, L.; Baltzan, M.; Rizzo, D.; Fichten, C.S.; Bailes, S. Sleep Apnea and Psychological Functioning in Chronic Fatigue Syndrome. J. Health Psychol. 2009, 14, 1251–1267. [Google Scholar] [CrossRef]
- Bozzini, S.; Albergati, A.; Capelli, E.; Lorusso, L.; Gazzaruso, C.; Pelissero, G.; Falcone, C. Cardiovascular Characteristics of Chronic Fatigue Syndrome. Biomed. Rep. 2018, 8, 26–30. [Google Scholar] [CrossRef]
- Garner, R.; Baraniuk, J.N. Orthostatic Intolerance in Chronic Fatigue Syndrome. J. Transl. Med. 2019, 17. [Google Scholar] [CrossRef] [PubMed]
- Corbitt, M.; Eaton-Fitch, N.; Staines, D.; Cabanas, H.; Marshall-Gradisnik, S. A Systematic Review of Cytokines in Chronic Fatigue Syndrome/Myalgic Encephalomyelitis/Systemic Exertion Intolerance Disease (CFS/ME/SEID). BMC Neurol. 2019, 19, 207. [Google Scholar] [CrossRef] [PubMed]
- Fischler, B.; Le Bon, O.; Hoffmann, G.; Cluydts, R.; Kaufman, L.; De Meirleir, K. Sleep Anomalies in the Chronic Fatigue Syndrome. A Comorbidity Study. Neuropsychobiology 1997, 35, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Shan, Z.Y.; Kwiatek, R.; Burnet, R.; Del Fante, P.; Staines, D.R.; Marshall-Gradisnik, S.M.; Barnden, L.R. Medial Prefrontal Cortex Deficits Correlate with Unrefreshing Sleep in Patients with Chronic Fatigue Syndrome. NMR Biomed. 2017, 30. [Google Scholar] [CrossRef] [PubMed]
- Barnden, L.R.; Shan, Z.Y.; Staines, D.R.; Marshall-Gradisnik, S.; Finegan, K.; Ireland, T.; Bhuta, S. Intra Brainstem Connectivity Is Impaired in Chronic Fatigue Syndrome. NeuroImage Clin. 2019, 24, 102045. [Google Scholar] [CrossRef] [PubMed]
- Althubaiti, A. Information Bias in Health Research: Definition, Pitfalls, and Adjustment Methods. J. Multidiscip. Healthc. 2016, 9, 211–217. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maksoud, R.; Eaton-Fitch, N.; Matula, M.; Cabanas, H.; Staines, D.; Marshall-Gradisnik, S. Systematic Review of Sleep Characteristics in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Healthcare 2021, 9, 568. https://doi.org/10.3390/healthcare9050568
Maksoud R, Eaton-Fitch N, Matula M, Cabanas H, Staines D, Marshall-Gradisnik S. Systematic Review of Sleep Characteristics in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Healthcare. 2021; 9(5):568. https://doi.org/10.3390/healthcare9050568
Chicago/Turabian StyleMaksoud, Rebekah, Natalie Eaton-Fitch, Michael Matula, Hélène Cabanas, Donald Staines, and Sonya Marshall-Gradisnik. 2021. "Systematic Review of Sleep Characteristics in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome" Healthcare 9, no. 5: 568. https://doi.org/10.3390/healthcare9050568
APA StyleMaksoud, R., Eaton-Fitch, N., Matula, M., Cabanas, H., Staines, D., & Marshall-Gradisnik, S. (2021). Systematic Review of Sleep Characteristics in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Healthcare, 9(5), 568. https://doi.org/10.3390/healthcare9050568