
Physical Activity during COVID-19 Lockdown: Data from an Italian Survey

 , ,
, ,  ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Descriptive Characteristics
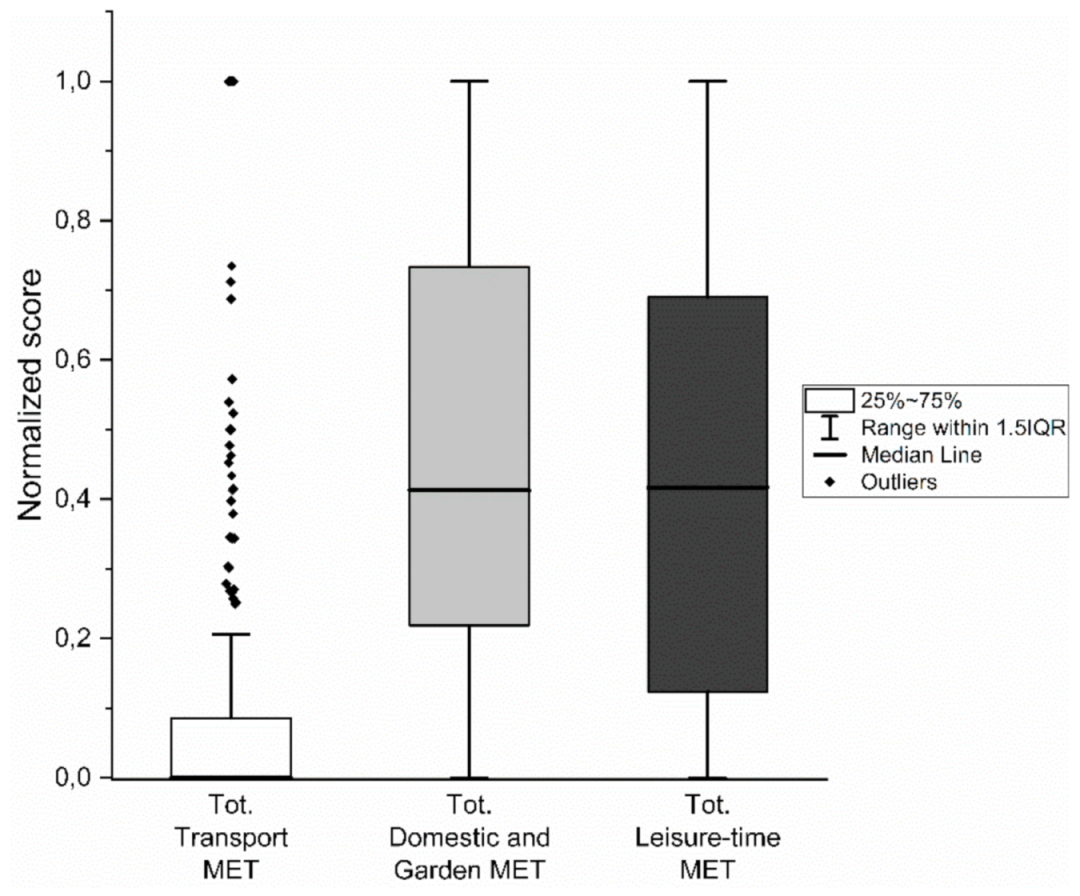
3.2. IPAQ
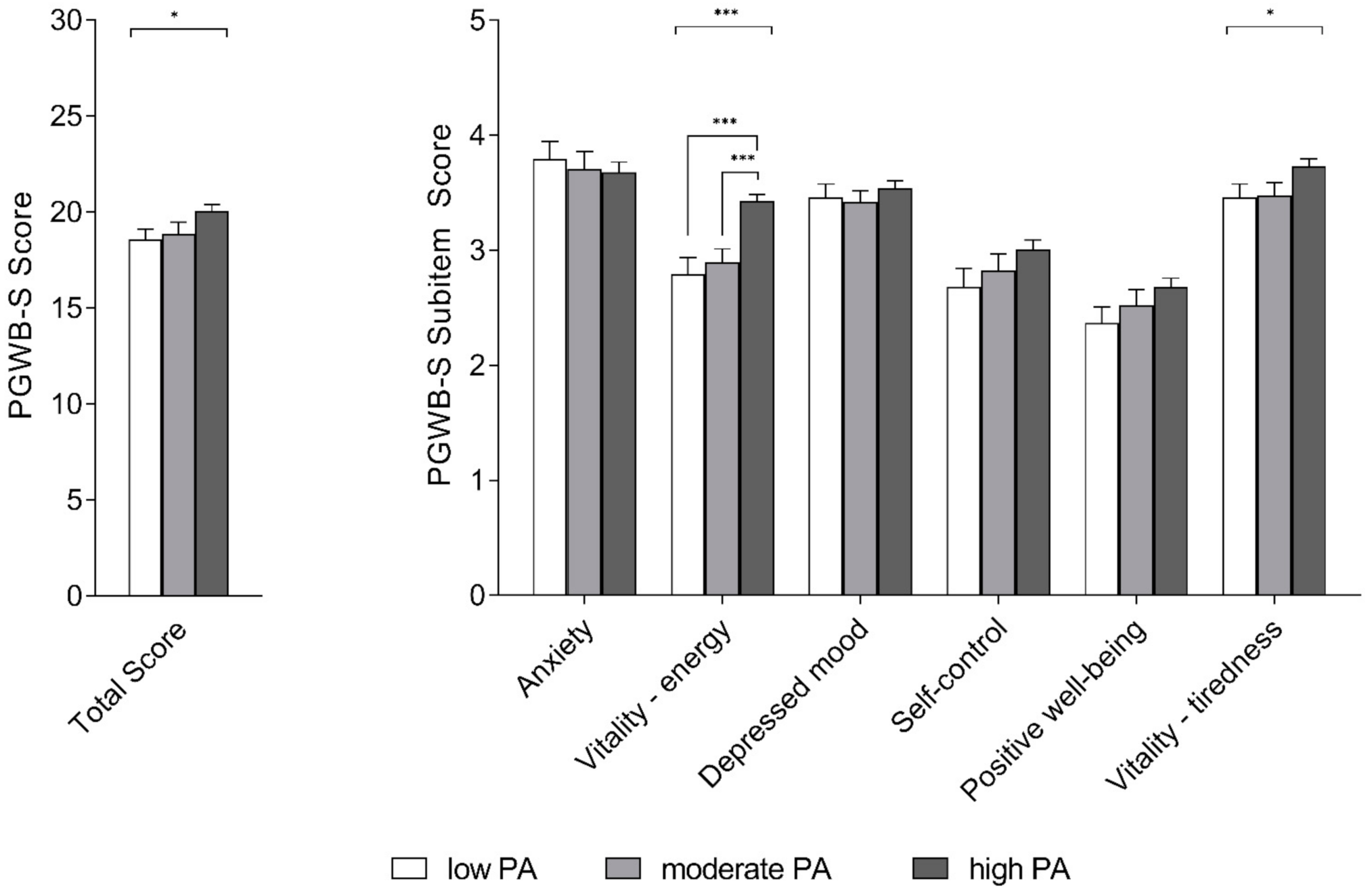
3.3. PGWB-S
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Director-General’s Opening Remarks at the Media Briefing on COVID-19. Available online: https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19 (accessed on 11 March 2020).
- Priori, A.; Baisi, A.; Banderali, G.; Biglioli, F.; Bulfamante, G.; Canevini, M.P.; Cariati, M.; Carugo, S.; Cattaneo, M.; Cerri, A.; et al. The Many Faces of Covid-19 at a Glance: A University Hospital Multidisciplinary Account From Milan, Italy. Front. Public Health 2021, 8, 575029. [Google Scholar] [CrossRef]
- Parmet, W.E.; Sinha, M.S. Covid-19—The law and limits of quarantine. N. Engl. J. Med. 2020, 382, E281–E283. [Google Scholar] [CrossRef]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef]
- Cavicchioli, M.; Ferrucci, R.; Guidetti, M.; Canevini, M.P.; Pravettoni, G.; Galli, F. What Will Be the Impact of the COVID-19 Quarantine on Psychological Distress? Considerations Based on a Systematic Review of Pandemic Outbreaks. Healthcare 2021, 9, 101. [Google Scholar] [CrossRef]
- Chen, P.; Mao, L.; Nassis, G.P.; Harmer, P.; Ainsworth, B.E.; Li, F. Coronavirus disease (COVID-19): The need to maintain regular physical activity while taking precautions. J. Sport Health Sci. 2020, 9, 103–104. [Google Scholar] [CrossRef]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sport Med. 1451, 54, 20. [Google Scholar]
- Jurak, G.; Morrison, S.A.; Leskošek, B.; Kovač, M.; Hadžić, V.; Vodičar, J.; Truden, P.; Starc, G. Physical activity recommendations during the COVID-19 virus outbreak. J. Sport Health Sci. 2020, 9, 325–327. [Google Scholar] [CrossRef]
- World Health Organization. Global Recommendations on Physical Activity for Health. Available online: https://www.who.int/publications/i/item/97892415999792010 (accessed on 2 November 2020).
- Gazzetta Ufficialee. Available online: https://www.gazzettaufficiale.it/eli/id/2020/03/11/20A01605/sg (accessed on 2 November 2020).
- Mannocci, A.; Di Thiene, D.; Del Cimmuto, A.; Masala, D.; Boccia, A.; De Vito, E.; La Torre, G. International Physical Activity Questionnaire: Validation and assessment in an Italian sample. Ital. J. Public Health 2010, 7, 369–376. [Google Scholar]
- Guidelines for Data Processing Analysis of the International Physical Activity Questionnaire (IPAQ)—Short and Long Forms—ScienceOpen. Available online: https://www.scienceopen.com/document?vid=b223350f-d159-4043-9b48-e2031f210a3c (accessed on 6 July 2020).
- Grossi, E.; Groth, N.; Mosconi, P.; Cerutti, R.; Pace, F.; Compare, A.; Apolone, G. Development and validation of the short version of the Psychological General Well-Being Index (PGWB-S). Health Qual. Life Outcomes 2006, 4, 88. [Google Scholar] [CrossRef] [PubMed]
- Hall, G.; Laddu, D.R.; Phillips, S.A.; Lavie, C.J.; Arena, R. A tale of two pandemics: How will COVID-19 and global trends in physical inactivity and sedentary behavior affect one another? Prog. Cardiovasc. Dis. 2020, 64, 108–110. [Google Scholar] [CrossRef] [PubMed]
- Qin, F.; Song, Y.; Nassis, G.P.; Zhao, L.; Dong, Y.; Zhao, C.; Feng, Y.; Zhao, J. Physical activity, screen time, and emotional well-being during the 2019 novel coronavirus outbreak in China. Int. J. Environ. Res. Public Health 2020, 17, 5170. [Google Scholar] [CrossRef] [PubMed]
- Bourdas, D.I.; Zacharakis, E.D. Impact of COVID-19 Lockdown on Physical Activity in a Sample of Greek Adults. Sports 2020, 8, 139. [Google Scholar] [CrossRef]
- López-Sánchez, G.F.; López-Bueno, R.; Gil-Salmerón, A.; Zauder, R.; Skalska, M.; Jastrzębska, J.; Jastrzębski, Z.; Schuch, F.B.; Grabovac, I.; Tully, M.A.; et al. Comparison of physical activity levels in Spanish adults with chronic conditions before and during COVID-19 quarantine. Eur. J. Public Health 2020, 31, 161–166. [Google Scholar] [CrossRef]
- Maugeri, G.; Castrogiovanni, P.; Battaglia, G.; Pippi, R.; D’Agata, V.; Palma, A.; Di Rosa, M.; Musumeci, G. The impact of physical activity on psychological health during Covid-19 pandemic in Italy. Heliyon 2020, 6, e04315. [Google Scholar] [CrossRef] [PubMed]
- Giustino, V.; Parroco, A.M.; Gennaro, A.; Musumeci, G.; Palma, A.; Battaglia, G. Physical Activity Levels and Related Energy Expenditure during COVID-19 Quarantine among the Sicilian Active Population: A Cross-Sectional Online Survey Study. Sustainability 2020, 12, 4356. [Google Scholar] [CrossRef]
- Gallo, L.A.; Gallo, T.F.; Young, S.L.; Moritz, K.M.; Akison, L.K. The impact of isolation measures due to covid-19 on energy intake and physical activity levels in australian university students. Nutrients 2020, 12, 1865. [Google Scholar] [CrossRef]
- Fallon, K. Exercise in the Time of COVID-19. Aust. J. Gen. Pract. 2020, 49. Available online: https://www1.racgp.org.au/ajgp/coronavirus/exercise-in-the-time-of-covid-19 (accessed on 22 April 2020). [CrossRef] [PubMed]
- Ribeiro de Souza, F.; Motta-Santos, D.; dos Santos Soares, D.; Beust de Lima, J.; Gonçalves Cardozo, G.; Santos Pinto Guimarães, L.; Eduardo Negrão, C.; Rodrigues dos Santos, M. Physical Activity Decreases the Prevalence of COVID-19-associated Hospitalization: Brazil EXTRA Study. medRxiv 2020. [Google Scholar] [CrossRef]
- Nieman, D.C.; Wentz, L.M. The compelling link between physical activity and the body’s defense system. J. Sport Health Sci. 2019, 8, 201–217. [Google Scholar] [CrossRef] [PubMed]
- Gleeson, M.; Bishop, N.C.; Stensel, D.J.; Lindley, M.R.; Mastana, S.S.; Nimmo, M.A. The anti-inflammatory effects of exercise: Mechanisms and implications for the prevention and treatment of disease. Nat. Rev. Immunol. 2011, 11, 607–610. [Google Scholar] [CrossRef] [PubMed]
- Ferrucci, R.; Dini, M.; Groppo, E.; Rosci, C.; Reitano, M.R.; Bai, F.; Poletti, B.; Brugnera, A.; Silani, V.; D’Arminio Monforte, A.; et al. Long-Lasting Cognitive Abnormalities after COVID-19. Brain Sci. 2021, 11, 235. [Google Scholar] [CrossRef]
- Constandt, B.; Thibaut, E.; De Bosscher, V.; Scheerder, J.; Ricour, M.; Willem, A. Exercising in Times of Lockdown: An Analysis of the Impact of COVID-19 on Levels and Patterns of Exercise among Adults in Belgium. Int. J. Environ. Res. Public Health Artic. 2020, 17, 4144. [Google Scholar] [CrossRef]
- Di Renzo, L.; Gualtieri, P.; Pivari, F.; Soldati, L.; Attinà, A.; Cinelli, G.; Cinelli, G.; Leggeri, C.; Caparello, G.; Barrea, L.; et al. Eating habits and lifestyle changes during COVID-19 lockdown: An Italian survey. J. Transl. Med. 2020, 18, 229. [Google Scholar] [CrossRef]
- Kong, C.; Teh, A.; Rashid, A. Heart rate, oxygen uptake, and energy cost of ascending and descending the stairs. Med. Sci. Sports Exerc. 2002, 34, 695–699. [Google Scholar]
- Saalim, M.; Sansare, K.; Karjodkar, F.R.; Ali, I.K.; Sharma, S.R.; Kapoor, R.; Mehra, A.; Rahman, B. Oral submucous fibrosis and its impact on psychological stress: A case-control study. Psychol. Health Med. 2020. [Google Scholar] [CrossRef]
- Ferrucci, R.; Marino, D.; Reitano, M.R.; Ruggiero, F.; Mameli, F.; Poletti, B.; Pravettoni, G.; Barbieri, S.; Priori, A.; Averna, A. Psychological Impact During an Epidemic: Data from Italy’s First Outbreak of COVID-19. SSRN Electron. J. 2020. [Google Scholar] [CrossRef]
- Panzeri, M.; Ferrucci, R.; Cozza, A.; Fontanesi, L. Changes in Sexuality and Quality of Couple Relationship During the COVID-19 Lockdown. Front. Psychol. 2020, 11. [Google Scholar] [CrossRef] [PubMed]
- Penedo, F.J.; Dahn, J.R. Exercise and well-being: A review of mental and physical health benefits associated with physical activity. Curr. Opin. Psychiatry 2005, 18, 189–193. [Google Scholar] [CrossRef] [PubMed]
- Rimmele, U.; Zellweger, B.C.; Marti, B.; Seiler, R.; Mohiyeddini, C.; Ehlert, U.; Heinrichs, M. Trained men show lower cortisol, heart rate and psychological responses to psychosocial stress compared with untrained men. Psychoneuroendocrinology 2007, 32, 627–635. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Category | Subjects |
|---|---|---|
| n | 317 | |
| Age-n (%) | 18–30 years | 166 (52.4%) |
| 31–65 years | 132 (41.6%) | |
| >65 years | 19 (6%) | |
| Sex-n (%) | Male | 123 (38.8%) |
| Female | 194 (61.2%) | |
| Education-n (%) | 5–8 years | 11 (3.5%) |
| 8–13 years | 17 (5.4%) | |
| 13–17 years | 90 (28.4%) | |
| >17 years | 199 (62.8%) | |
| City size-n (%) | <10 thousand residents | 128 (40.4%) |
| 10–100 thousand residents | 126 (39.7%) | |
| >100 thousand residents | 58 (18.3%) | |
| Missing | 5 (1.6%) |
| IPAQ-Levels 1 | IPAQ-Domains 2 | |||||||
|---|---|---|---|---|---|---|---|---|
| Low Physical Activity | Moderate Physical Activity | High Physical Activity | Active Transportation | Domestic and Garden Activity | Leisure Time | Total Score | ||
| Total (n = 317) | 55 (17.4%) | 69 (21.8%) | 193 (60.9%) | 0 (198) | 878 (2051.5) | 1070 (1902.5) | 2408 (3460.5) | |
| Age | 18–30 years | 27 (16.3%) | 29 (17.5%) | 110 (66.3%) | 0 (148) | 810 (1552,5) | 1260 (1829.3) | 2547 (2735.3) |
| 31–65 years | 26 (19.7%) | 33 (25%) | 73 (55.3%) | 0 (248) | 986 (2499) | 791 (1901.5) | 2233 (4090.5) | |
| >65 years | 2 (10.5%) | 7 (36.8%) | 10 (52.6%) | 164 (370.5) | 1901 (6603.8) | 1040 (1211.8) | 3695 (7520.8) | |
| Sex | male | 16 (13%) | 28 (22.8%) | 79 (64.2%) | 50 (270) | 810 (2093) | 1260 (1800) | 2470 (3573) |
| female | 39 (20.1%) | 41 (21.1%) | 114 (58.8%) | 0 (148) | 945 (2036) | 900 (1909.5) | 2397 (3362) | |
| Education | 5–8 years | 4 (36.4%) | 1 (9.1%) | 6 (54.5%) | 99 (297) | 1185 (1755) | 0 (1040) | 2097 (4654) |
| 8–13 years | 5 (29.4%) | 3 (17.6%) | 9 (52.9%) | 0 (198) | 900 (2186) | 300 (2123) | 2150 (3867) | |
| 13–17 years | 8 (8.9%) | 24 (26.7%) | 58 (64.4%) | 0 (283.5) | 967.5 (2086.8) | 1240 (1985.5) | 2800.5 (3617.8) | |
| >17 years | 38 (19.1%) | 41 (20.6%) | 120 (60.3%) | 0 (156) | 859 (1946.3) | 1040 (1841) | 2404.5 (3392.3) | |
| City size | <10,000 residents | 21 (16.4%) | 26 (20.3%) | 81 (63.3%) | 0 (148) | 1312.5 (2715) | 1040 (2233.5) | 2886.5 (4370.5) |
| 10–100 thousand residents | 22 (17.5%) | 28 (22.2%) | 76 (60.3%) | 0 (156) | 761 (1426.5) | 1080 (1616) | 2303 (2464.3) | |
| >100 thousand residents | 11 (19%) | 12 (20.7%) | 35 (60.3%) | 74.5 (332.5) | 731.5 (1316.3) | 1110 (1670) | 2182.5 (3292.3) | |
| PGWB-S | Total | Activity Levels | p Value | ||
|---|---|---|---|---|---|
| Low 1 | Moderate 1 | High 1 | |||
| anxiety | 3.7 ± 1.21 | 3.80 ± 1.11 | 3.71 ± 1.24 | 3.68 ± 1.23 | 0.941 |
| vitality-energy | 3.21 ± 0.91 | 2.80 ± 1.05 | 2.90 ± 0.96 | 3.43 ± 0.78 | <0.0001 |
| depressed mood | 3.5 ± 0.84 | 3.46 ± 0.84 | 3.42 ± 0.83 | 3.54 ± 0.85 | 0.534 |
| self-control | 2.91 ± 1.21 | 2.69 ± 1.18 | 2.83 ± 1.18 | 3.01 ± 1.22 | 0.173 |
| positive well-being | 2.59 ± 1.09 | 2.37 ± 1 | 2.52 ± 1.13 | 2.68 ± 1.10 | 0.121 |
| vitality-tiredness | 3.63 ± 0.89 | 3.46 ± 0.84 | 3.48 ± 0.92 | 3.73 ± 0.88 | 0.041 |
| PGWB-S total score | 19.54 ± 4.65 | 18.57 ± 4.08 | 18.86 ± 4.99 | 20.07 ± 4.63 | 0.037 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guidetti, M.; Averna, A.; Castellini, G.; Dini, M.; Marino, D.; Bocci, T.; Ferrucci, R.; Priori, A. Physical Activity during COVID-19 Lockdown: Data from an Italian Survey. Healthcare 2021, 9, 513. https://doi.org/10.3390/healthcare9050513
Guidetti M, Averna A, Castellini G, Dini M, Marino D, Bocci T, Ferrucci R, Priori A. Physical Activity during COVID-19 Lockdown: Data from an Italian Survey. Healthcare. 2021; 9(5):513. https://doi.org/10.3390/healthcare9050513
Chicago/Turabian StyleGuidetti, Matteo, Alberto Averna, Greta Castellini, Michelangelo Dini, Daniela Marino, Tommaso Bocci, Roberta Ferrucci, and Alberto Priori. 2021. "Physical Activity during COVID-19 Lockdown: Data from an Italian Survey" Healthcare 9, no. 5: 513. https://doi.org/10.3390/healthcare9050513
APA StyleGuidetti, M., Averna, A., Castellini, G., Dini, M., Marino, D., Bocci, T., Ferrucci, R., & Priori, A. (2021). Physical Activity during COVID-19 Lockdown: Data from an Italian Survey. Healthcare, 9(5), 513. https://doi.org/10.3390/healthcare9050513