
Prevalence of Balance Impairment and Factors Associated with Balance among Patients with Stroke. A Cross Sectional Retrospective Case Control Study


Abstract
1. Introduction
2. Materials and Methods
Analysis
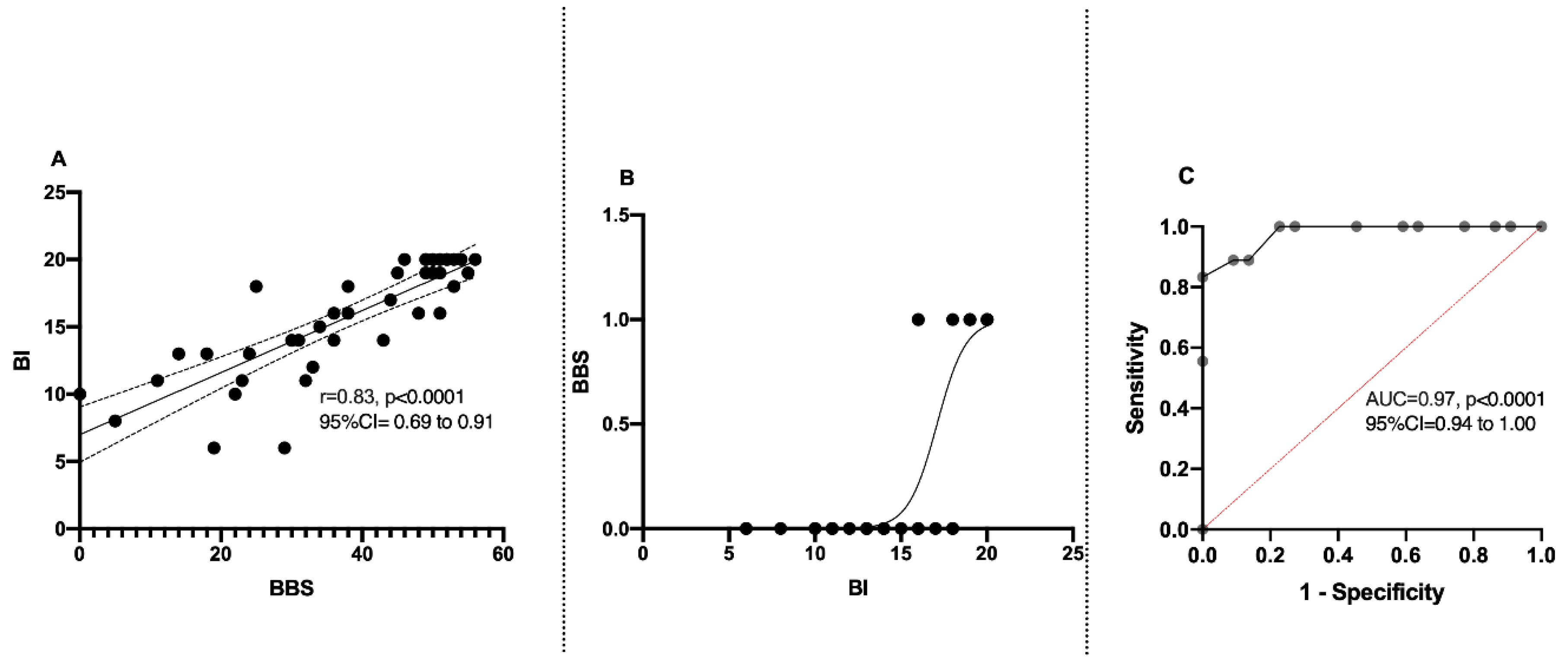
3. Results
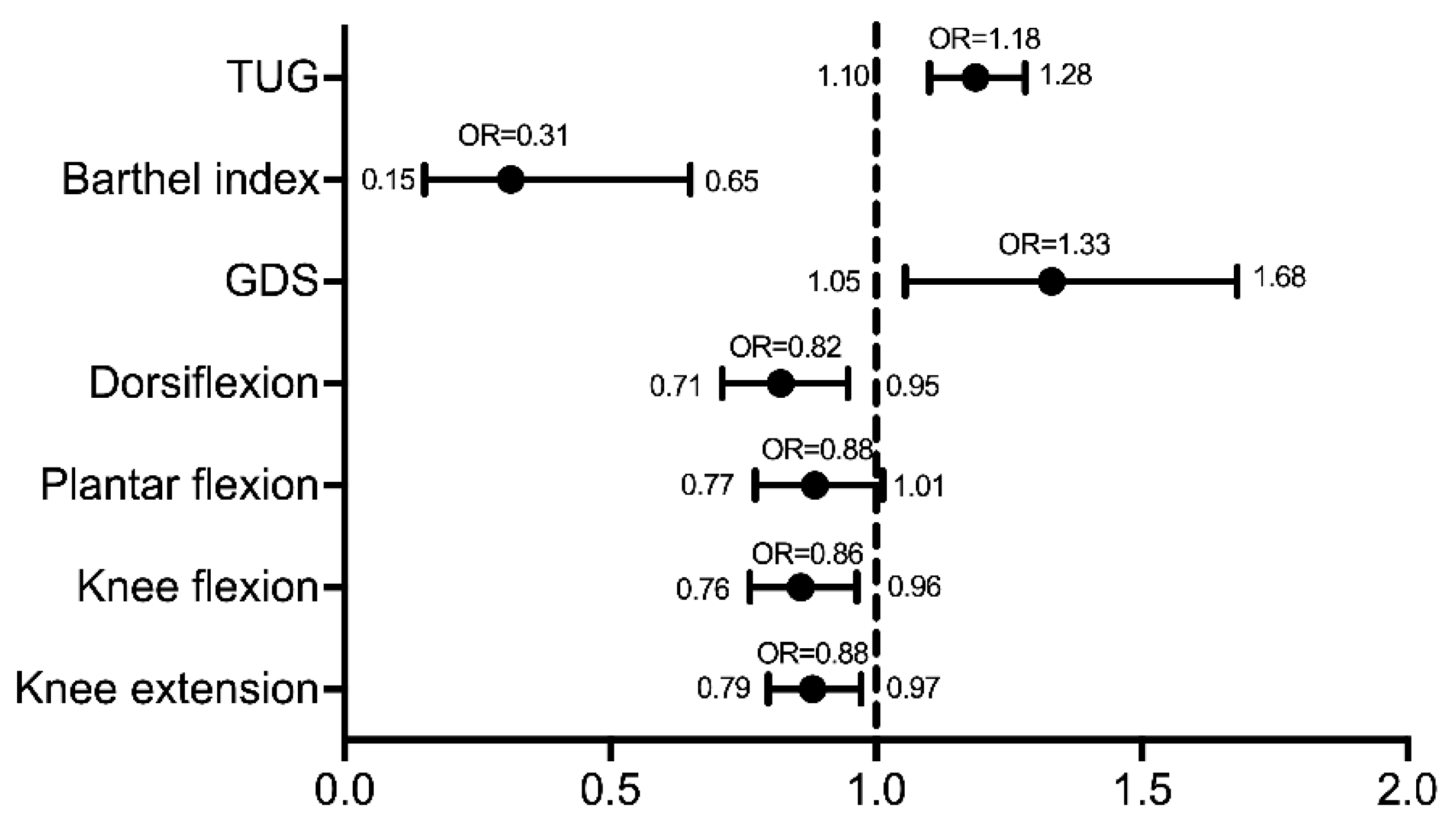
Regression Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| TUG | Timed up and go test |
| BBS | Berg balance scale |
| BI | Barthel index |
| GDS | Geriatric depression scale |
| mRS | modified Rankin scale |
References
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, Regional, and National Incidence, Prevalence, and Years Lived with Disability for 354 Diseases and Injuries for 195 Countries and Territories, 1990–2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet Lond. Engl. 2018, 392, 1789–1858. [CrossRef]
- Roger, V.L.; Go, A.S.; Lloyd-Jones, D.M.; Benjamin, E.J.; Berry, J.D.; Borden, W.B.; Bravata, D.M.; Dai, S.; Ford, E.S.; Fox, C.S.; et al. Heart Disease and Stroke Statistics—2012 Update: A Report from the American Heart Association. Circulation 2012, 125, e2–e220. [Google Scholar] [CrossRef]
- Donovan, N.J.; Kendall, D.L.; Heaton, S.C.; Kwon, S.; Velozo, C.A.; Duncan, P.W. Conceptualizing Functional Cognition in Stroke. Neurorehabil. Neural Repair 2008, 22, 122–135. [Google Scholar] [CrossRef]
- Lo Coco, D.; Lopez, G.; Corrao, S. Cognitive Impairment and Stroke in Elderly Patients. Vasc. Health Risk Manag. 2016, 12, 105–116. [Google Scholar] [CrossRef]
- Tang, E.Y.; Amiesimaka, O.; Harrison, S.L.; Green, E.; Price, C.; Robinson, L.; Siervo, M.; Stephan, B.C. Longitudinal Effect of Stroke on Cognition: A Systematic Review. J. Am. Heart Assoc. 2018, 7, e006443. [Google Scholar] [CrossRef]
- Khattab, S.; Wiley, E.; Fang, H.; Richardson, J.; MacDermid, J.; Tang, A. The Effects of Exercise on Cognition Post-Stroke: Are There Sex Differences? A Systematic Review and Meta-Analysis. Disabil. Rehabil. 2020, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Schmid, A.A.; Van Puymbroeck, M.; Altenburger, P.A.; Miller, K.K.; Combs, S.A.; Page, S.J. Balance Is Associated with Quality of Life in Chronic Stroke. Top. Stroke Rehabil. 2013, 20, 340–346. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.-H.; Park, E.-Y. Balance Self-Efficacy in Relation to Balance and Activities of Daily Living in Community Residents with Stroke. Disabil. Rehabil. 2014, 36, 295–299. [Google Scholar] [CrossRef]
- Park, J.; Kim, T.-H. The Effects of Balance and Gait Function on Quality of Life of Stroke Patients. NeuroRehabilitation 2019, 44, 37–41. [Google Scholar] [CrossRef] [PubMed]
- Xie, J.; Wu, E.Q.; Zheng, Z.-J.; Croft, J.B.; Greenlund, K.J.; Mensah, G.A.; Labarthe, D.R. Impact of Stroke on Health-Related Quality of Life in the Noninstitutionalized Population in the United States. Stroke 2006, 37, 2567–2572. [Google Scholar] [CrossRef]
- Baert, I.; Feys, H.; Daly, D.; Troosters, T.; Vanlandewijck, Y. Are Patients 1 Year Post-Stroke Active Enough to Improve Their Physical Health? Disabil. Rehabil. 2012, 34, 574–580. [Google Scholar] [CrossRef] [PubMed]
- Boden-Albala, B.; Litwak, E.; Elkind, M.S.V.; Rundek, T.; Sacco, R.L. Social Isolation and Outcomes Post Stroke. Neurology 2005, 64, 1888–1892. [Google Scholar] [CrossRef]
- Morris, R.; Jones, J.; Wilcox, J.; Cole, S. Depression and Anxiety Screening after Stroke: Adherence to Guidelines and Future Directions. Disabil. Rehabil. 2012, 34, 733–739. [Google Scholar] [CrossRef]
- Lincoln, N.B.; Brinkmann, N.; Cunningham, S.; Dejaeger, E.; De Weerdt, W.; Jenni, W.; Mahdzir, A.; Putman, K.; Schupp, W.; Schuback, B.; et al. Anxiety and Depression after Stroke: A 5 Year Follow-Up. Disabil. Rehabil. 2013, 35, 140–145. [Google Scholar] [CrossRef]
- Forster, A.; Young, J. Incidence and Consequences of Falls Due to Stroke: A Systematic Inquiry. BMJ 1995, 311, 83–86. [Google Scholar] [CrossRef]
- Andersson, A.G.; Kamwendo, K.; Seiger, A.; Appelros, P. How to Identify Potential Fallers in a Stroke Unit: Validity Indexes of 4 Test Methods. J. Rehabil. Med. 2006, 38, 186–191. [Google Scholar] [CrossRef] [PubMed]
- Soyuer, F.; Oztürk, A. The Effect of Spasticity, Sense and Walking Aids in Falls of People after Chronic Stroke. Disabil. Rehabil. 2007, 29, 679–687. [Google Scholar] [CrossRef]
- Goljar, N.; Globokar, D.; Puzić, N.; Kopitar, N.; Vrabič, M.; Ivanovski, M.; Vidmar, G. Effectiveness of a Fall-Risk Reduction Programme for Inpatient Rehabilitation after Stroke. Disabil. Rehabil. 2016, 38, 1811–1819. [Google Scholar] [CrossRef]
- Palermi, S.; Sacco, A.M.; Belviso, I.; Marino, N.; Gambardella, F.; Loiacono, C.; Sirico, F. Effectiveness of Tai Chi on Balance Improvement in Type 2 Diabetes Patients: A Systematic Review and Meta-Analysis. J. Aging Phys. Act. 2020, 28, 787–797. [Google Scholar] [CrossRef]
- Ramnemark, A.; Nilsson, M.; Borssén, B.; Gustafson, Y. Stroke, a Major and Increasing Risk Factor for Femoral Neck Fracture. Stroke 2000, 31, 1572–1577. [Google Scholar] [CrossRef] [PubMed]
- Tyson, S.F.; Hanley, M.; Chillala, J.; Selley, A.; Tallis, R.C. Balance Disability after Stroke. Phys. Ther. 2006, 86, 30–38. [Google Scholar] [CrossRef] [PubMed]
- Vincent-Onabajo, G.; Musa, H.Y.; Joseph, E. Prevalence of Balance Impairment Among Stroke Survivors Undergoing Neurorehabilitation in Nigeria. J. Stroke Cerebrovasc. Dis. Off. J. Natl. Stroke Assoc. 2018, 27, 3487–3492. [Google Scholar] [CrossRef] [PubMed]
- Iwasaki, S.; Yamasoba, T. Dizziness and Imbalance in the Elderly: Age-Related Decline in the Vestibular System. Aging Dis. 2015, 6, 38–47. [Google Scholar] [CrossRef]
- Gath, C.F.; Gianella, M.G.; Bonamico, L.; Olmos, L.; Russo, M.J. Prediction of Balance After Inpatient Rehabilitation in Stroke Subjects with Severe Balance Alterations at the Admission. J. Stroke Cerebrovasc. Dis. Off. J. Natl. Stroke Assoc. 2021, 30, 105627. [Google Scholar] [CrossRef] [PubMed]
- Torkia, C.; Best, K.L.; Miller, W.C.; Eng, J.J. Balance Confidence: A Predictor of Perceived Physical Function, Perceived Mobility, and Perceived Recovery 1 Year After Inpatient Stroke Rehabilitation. Arch. Phys. Med. Rehabil. 2016, 97, 1064–1071. [Google Scholar] [CrossRef] [PubMed]
- Pollock, C.L.; Hunt, M.A.; Garland, S.J.; Ivanova, T.D.; Wakeling, J.M. Relationships Between Stepping-Reaction Movement Patterns and Clinical Measures of Balance, Motor Impairment, and Step Characteristics after Stroke. Phys. Ther. 2021. [Google Scholar] [CrossRef]
- Moon, H.I.; Lee, H.J.; Yoon, S.Y. Lesion Location Associated with Balance Recovery and Gait Velocity Change after Rehabilitation in Stroke Patients. Neuroradiology 2017, 59, 609–618. [Google Scholar] [CrossRef]
- Robert, A.A.; Zamzami, M.M. Stroke in Saudi Arabia: A Review of the Recent Literature. Pan Afr. Med. J. 2014, 17, 14. [Google Scholar] [CrossRef]
- Chang, T.; Gajasinghe, S.; Arambepola, C. Prevalence of Stroke and Its Risk Factors in Urban Sri Lanka: Population-Based Study. Stroke 2015, 46, 2965–2968. [Google Scholar] [CrossRef]
- Khan, F.R.; Chevidikunnan, M.F.; BinMulayh, E.A.; Gaowgzeh, R.A. Physical Therapists’ Perspectives on Improving Walking Capacity in Patients with Stroke: A Cross-Sectional Study from Saudi Arabia. J. Musculoskelet. Neuronal Interact. 2020, 20, 223–233. [Google Scholar]
- De Haart, M.; Geurts, A.C.; Huidekoper, S.C.; Fasotti, L.; van Limbeek, J. Recovery of Standing Balance in Postacute Stroke Patients: A Rehabilitation Cohort Study. Arch. Phys. Med. Rehabil. 2004, 85, 886–895. [Google Scholar] [CrossRef] [PubMed]
- Peurala, S.H.; Könönen, P.; Pitkänen, K.; Sivenius, J.; Tarkka, I.M. Postural Instability in Patients with Chronic Stroke. Restor. Neurol. Neurosci. 2007, 25, 101–108. [Google Scholar] [PubMed]
- Wilkins, S.S.; Akhtar, N.; Salam, A.; Bourke, P.; Joseph, S.; Santos, M.; Shuaib, A. Acute Post Stroke Depression at a Primary Stroke Center in the Middle East. PLoS ONE 2018, 13, e0208708. [Google Scholar] [CrossRef]
- Spera, R.; Belviso, I.; Sirico, F.; Palermi, S.; Massa, B.; Mazzeo, F.; Montesano, P. Jump and Balance Test in Judo Athletes with or without Visual Impairments. J. Hum. Sport Exerc. 2019, 14, S937–S947. [Google Scholar] [CrossRef]
- Clarke, D.J.; Forster, A. Improving Post-Stroke Recovery: The Role of the Multidisciplinary Health Care Team. J. Multidiscip. Healthc. 2015, 8, 433–442. [Google Scholar] [CrossRef] [PubMed]
- Della Valle, E.; Palermi, S.; Aloe, I.; Marcantonio, R.; Spera, R.; Montagnani, S.; Sirico, F. Effectiveness of Workplace Yoga Interventions to Reduce Perceived Stress in Employees: A Systematic Review and Meta-Analysis. J. Funct. Morphol. Kinesiol. 2020, 5, 33. [Google Scholar] [CrossRef]
- Eng, J.J. Strength Training in Individuals with Stroke. Physiother. Can. Physiother. Can. 2004, 56, 189–201. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Value |
|---|---|
| n (n%) | |
| Gender | |
| Male | 64 (79%) |
| Female | 17 (21%) |
| Side of Weakness | |
| Right | 34 (42%) |
| Left | 47 (58%) |
| Mean ± SD (range) | |
| Age (years) | 58.36 ± 14.06 (25 to 94) |
| Time since stroke (Months) | 16.96 ± 32.43 (1 to 223) |
| Ankle dorsiflexion strength (kg) | 3.97 ± 3.76 (0 to 18) |
| Ankle plantarflexion strength (kg) | 5.04 ± 3.41 (0 to 14) |
| Knee extension strength (kg) | 9.51 ± 5.44 (0 to 30) |
| Knee flexion strength (kg) | 5.94 ± 4.57 (0 to 20) |
| TUG (second) | 34.50 ± 27.28 (6.750 to 165.0) |
| Mean ± SD; Median (range) | |
| BBS | 39.94 ± 13.76; 45 (0 to 56) |
| BI | 15.63 ± 4.19; 16 (6 to 20) |
| GDS | 4.725 ± 3.52; 4.500 (0 to 13) |
| mRS | 2.575 ± 1.28; 2 (1 to 5) |
| Variable | Prevalence of Balance (%) | p Value | Odds Ratio | 95% CI |
|---|---|---|---|---|
| Gender | ||||
| Female | 52.9 | 0.657 | 1.28 | 0.437–3.723 |
| Male | 46.9 | - | 1 | Reference |
| Age (Years) | ||||
| ≥56 | 50 | 0.702 | 1.19 | 0.492–2.866 |
| <55 | 45.7 | - | 1 | Reference |
| Post stroke duration | ||||
| Acute/subacute | 53.8 | 0.324 | 1.556 | 0.647–3.741 |
| Chronic | 42.9 | - | 1 | Reference |
| Type of stroke | ||||
| Ischemic | 53.3 | 0.855 | 1.143 | 0.273–4.786 |
| Hemorrhagic | 50 | - | 1 | Reference |
| Side of Hemiplegia | ||||
| Left | 51.1 | 0.537 | 1.322 | 0.545–3.206 |
| Right | 44.1 | - | 1 | Reference |
| Aid | ||||
| With aid * | 77.8 | 0.0001 | 10.818 | 3.827–30.577 |
| Without aid | 24.4 | - | 1 | Reference |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khan, F.; Chevidikunnan, M.F. Prevalence of Balance Impairment and Factors Associated with Balance among Patients with Stroke. A Cross Sectional Retrospective Case Control Study. Healthcare 2021, 9, 320. https://doi.org/10.3390/healthcare9030320
Khan F, Chevidikunnan MF. Prevalence of Balance Impairment and Factors Associated with Balance among Patients with Stroke. A Cross Sectional Retrospective Case Control Study. Healthcare. 2021; 9(3):320. https://doi.org/10.3390/healthcare9030320
Chicago/Turabian StyleKhan, Fayaz, and Mohamed Faisal Chevidikunnan. 2021. "Prevalence of Balance Impairment and Factors Associated with Balance among Patients with Stroke. A Cross Sectional Retrospective Case Control Study" Healthcare 9, no. 3: 320. https://doi.org/10.3390/healthcare9030320
APA StyleKhan, F., & Chevidikunnan, M. F. (2021). Prevalence of Balance Impairment and Factors Associated with Balance among Patients with Stroke. A Cross Sectional Retrospective Case Control Study. Healthcare, 9(3), 320. https://doi.org/10.3390/healthcare9030320