
Trust in Intensive Care Patients, Family, and Healthcare Professionals: The Development of a Conceptual Framework Followed by a Case Study


Abstract
1. Introduction
2. Objectives
3. Contextual Background
“Care used to treat sudden, often unexpected, urgent or emergent episodes of injury and illness that can lead to death or disability without rapid intervention.”
4. Healthcare Professionals
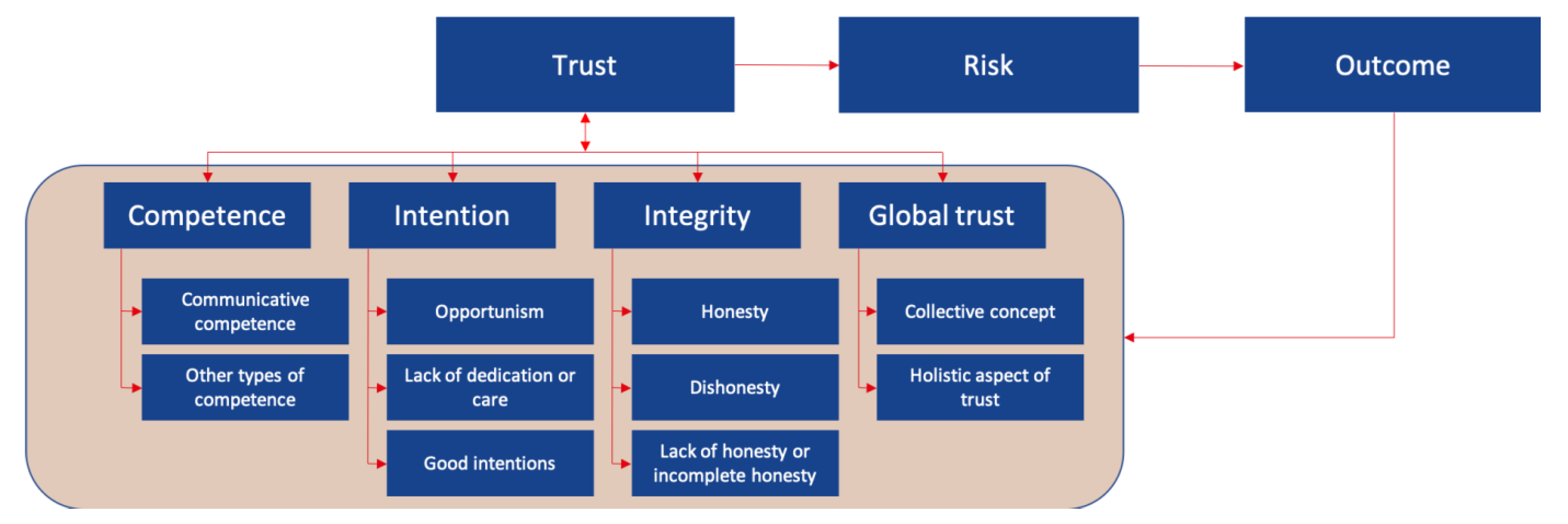
5. Development of a Conceptual Framework
5.1. Competence
5.2. Intention
5.3. Integrity
5.4. Global Trust
5.5. Perceived Risk, Risk-Taking in Relations and Outcome
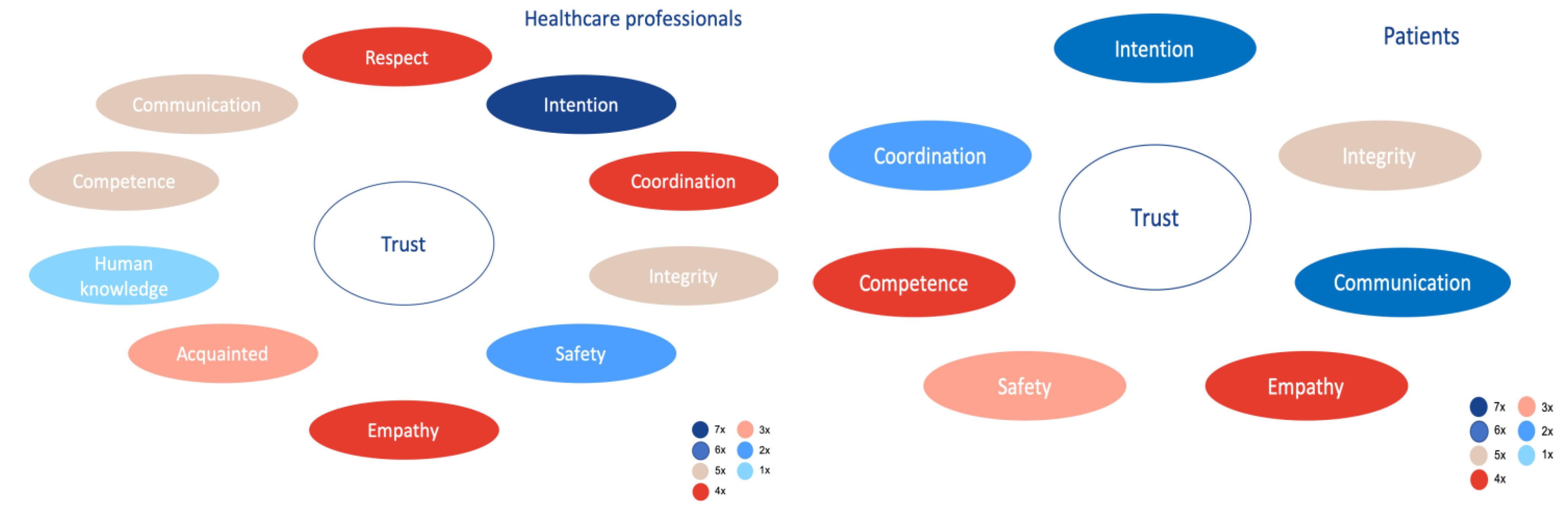
6. Case Study
6.1. Methods
6.2. Ethical Considerations
6.3. Respondents
6.4. Data Analysis
6.5. Results
6.5.1. Competence
“They (other HCPs ed.) also have to have good communicative qualities. I mean there are doctors who are very smart and can treat very well but they cannot communicate this appropriately to family and even though good actions are done, you will not be able to build trust. (…) a bad doctor can have more trust than a good doctor (Healthcare professional 2).”
6.5.2. Intention
“The most important thing that has to come across is that the patient gets the idea that the physician is going to work for you. You come with a complaint, if it is understood of not. You want to have the feeling that that physician has the goal to find out what is wrong with you and cure that”
6.5.3. Integrity
“Because then, you don’t notice what is happening with other patients, you don’t have to leave for privacy reasons, and the patients are not bothered by other patients”.
6.5.4. Global Trust
6.5.5. Risk
“The bulk of the communication disruptions with family, there is a basis of cultural differences why we have a different view regarding what is best for the patient. If it is so fundamentally different, you can understand each other but you will not come together.”
6.5.6. Outcome
7. Discussion
8. Conclusions
9. Recommendations
9.1. Short-Term
9.1.1. Change the Feedback Culture
9.1.2. Humanize Intensive Care
9.1.3. Intensify the Education on Communication of HCPs
9.2. Long-Term
9.2.1. Single Person Rooms
9.2.2. Create Opportunities for Patients to Get More Rest
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- van de Gevel, B.; Schot, E.; Kremer, J.; Meurs, P. Verantwoording in de Zorg kan Meer op Basis van Vertrouwen–Sociale Vraagstukken. 2019. Available online: https://www.socialevraagstukken.nl/verantwoording-in-de-zorg-kan-meer-op-basis-van-vertrouwen/ (accessed on 17 July 2019).
- RVS. Blijk van vertrouwen-Anders Verantwoorden Voor Goede Zorg | Advies | Raad voor Volksgezondheid en Samenleving. Den Haag. 2019. Available online: https://www.raadrvs.nl/documenten/publicaties/2019/05/14/advies-blijk-van-vertrouwen---anders-verantwoorden-voor-goede-zorg (accessed on 17 July 2019).
- Meyer, S.B.; Ward, P.R. Do Your Patients Trust You? A Sociological Understanding of the Implications of Patient Mistrust in Healthcare Professionals. 2008. Available online: https://dspace2.flinders.edu.au/xmlui/bitstream/handle/2328/26516/Meyer-Patients1.pdf?sequence=1&isAllowed=y (accessed on 8 March 2019).
- Brown, M.T.; Bussell, J.; Dutta, S.; Davis, K.; Strong, S.; Mathew, S. Medication adherence: Truth and consequences. Am. J. Med. Sci. 2016, 351, 387–399. [Google Scholar] [CrossRef]
- Egede, L.E.; Ellis, C. Development and testing of the multidimensional trust in health care systems scale. J. Gen. Intern. Med. 2008, 23, 808–815. [Google Scholar] [CrossRef] [PubMed]
- Trachtenberg, F.; Dugan, E.A.; Hall, M. How patients’ trust relates to their involvement in medical care. J. Fam. Pr. 2005, 54, 344–352. [Google Scholar]
- LaVeist, T.A.; Isaac, L.A.; Williams, K.P. Mistrust of health care organizations is associated with underutilization of health services. Health Serv. Res. 2009, 44, 2093–2105. [Google Scholar] [CrossRef]
- Lee, T.H.; McGlynn, E.A.; Safran, D.G. A framework for increasing trust between patients and the organizations that care for them. JAMA 2019, 321, 539–540. [Google Scholar] [CrossRef]
- Van Galen, L.S. Patient Safety in the Acute Healthcare Chain. Is It Safer @ Home? VU Amsterdam. 2017. Available online: https://www.netwerkacutezorgnoordwest.nl/app/uploads/2017/06/PDFThesisLSvanGalen.pdf (accessed on 5 January 2019).
- van Mol, M.M.C.; Nijkamp, M.D.; Bakker, J.; Schaufeli, W.B.; Kompanje, E.J. Counterbalancing work-related stress? Work engagement among intensive care professionals. Aust. Crit. Care 2018, 31, 234–241. [Google Scholar] [CrossRef] [PubMed]
- Seaman, J.B.; Cohen, T.R.; White, U.B. Reducing the stress on clinicians working in the ICU. JAMA 2018, 320, 1981–1982. [Google Scholar] [CrossRef]
- LoCurto, J.; Berg, G.M. Trust in healthcare settings: Scale development, methods, and preliminary determinants. SAGE Open Med. 2016, 4, 2050312116664224. [Google Scholar] [CrossRef]
- Laine, C.; Jama, F.D. Patient-centered medicine: A professional evolution. JAMA 1996, 272, 152–156. [Google Scholar] [CrossRef]
- Kuipers, S.J.; Cramm, J.M.; Nieboer, A.P. The importance of patient-centered care and co-creation of care for satisfaction with care and physical and social well-being of patients with multi-morbidity in the primary care setting. BMC Health Serv. Res. 2019, 19, 13. [Google Scholar] [CrossRef]
- Maarse, H.; Jeurissen, P.; Ruwaard, D. Results of the market-oriented reform in the Netherlands: A review. Health Econ. Policy Law 2016, 11, 161–178. [Google Scholar] [CrossRef]
- Groenewegen, P.P.; Hansen, J.; De Jong, J.D. Trust in times of health reform. Health Policy 2019, 123, 281–287. [Google Scholar] [CrossRef] [PubMed]
- Hirshon, J.M.; Risko, N.; Calvello, E.J.B.; De Ramirez, S.S.; Narayan, M.; Theodosis, C.; O’Neill, J. Health systems and services: The role of acute care. Bull. World Health Organ. 2013, 91, 386–388. [Google Scholar] [CrossRef]
- NVZ. Rapport De Brede Betekenis van Acute Zorg. 2013. Available online: https://www.nvz-ziekenhuizen.nl/_library/11583/De-brede-betekenis-van-acute-zorg-rapport-Twijnstra-Gudde.pdf (accessed on 21 February 2019).
- OLVG. Intensive Care | OLVG. 2019. Available online: https://www.olvg.nl/intensive-care (accessed on 17 July 2019).
- OLVG. Ons Verhaal | OLVG. Available online: https://www.olvg.nl/ons-verhaal (accessed on 8 March 2019).
- OLVG. Jaarverantwoording 2017 Maatschappelijk Verslag en Jaarrekening. 2018. Available online: www.jaarverslagenzorg.nl (accessed on 5 April 2019).
- OLVG. Kerngegevens | OLVG. Available online: https://www.olvg.nl/kerngegevens (accessed on 5 April 2019).
- Lluch, M. Healthcare professionals’ organisational barriers to health information technologies—A literature review. Int. J. Med. Inform. 2011, 80, 849–862. [Google Scholar] [CrossRef]
- Mechanic, D.; Schlesinger, M. The impact of managed care on patients’ trust in medical care and their physicians. JAMA 1996, 275, 1693. [Google Scholar] [CrossRef] [PubMed]
- Hall, M.A.; Dugan, E.; Zheng, B.; Mishra, A.K. Trust in physicians and medical institutions: What is it, can it be measured, and does it matter? Milbank Q. 2001, 79, 613–639. [Google Scholar] [CrossRef]
- Mayer, R.C.; Davis, J.H.; Schoorman, D.F. An Integrative Model of Organizational Trust. 1995. Available online: https://static1.squarespace.com/static/577cee432e69cf8918495759/t/57bec79d46c3c412eb298a00/1472120738550/1995_MAYER+ET+AL_1995_Organizational+Trust.pdf (accessed on 17 April 2019).
- Nooteboom, B. Vertrouwen en Innovatie. 2006. Available online: http://www.seijner.nl/nooteboom-vertrouwen-en-innovatie.pdf (accessed on 19 February 2019).
- Ring, P.S.; Nooteboom, B. Trust: Forms, foundations, functions, failures and figures. Adm. Sci. Q. 2003, 48, 720. [Google Scholar] [CrossRef]
- Nooteboom, B. Vormen en bronnen van vertrouwen. Maandbl. Voor Account. en Bedrijfsecon. 2006, 80, 8–16. [Google Scholar] [CrossRef][Green Version]
- Dubois, A. UNIVERSITEIT GENT Faculteit Geneeskunde en Gezondheidswetenschappen. 2011. Available online: https://lib.ugent.be/fulltxt/RUG01/001/893/115/RUG01-001893115_2012_0001_AC.pdf (accessed on 8 March 2019).
- Hupcey, J.E.; Penrod, E.; Morse, J.M. et ProQuest Nursing & Allied Health Source pg. 2000. Available online: https://www.researchgate.net/profile/Judith_Hupcey/publication/12176796_Establishing_and_maintaining_trust_during_acute_care_hospitalizations/links/565f7afd08aefe619b28a52b.pdf (accessed on 13 March 2019).
- Gray, D.E. Doing Research in the Real World, 2nd ed; SAGE Publications Ltd: Thousend Oakes, CA, USA, 2014. [Google Scholar]
- Bryman, A. Social Research Methods, 4th ed.; Oxford University Press Inc.: New York, NY, USA, 2012. [Google Scholar]
- Shoemaker, K.; Smith, C.P. The impact of patient-physician alliance on trust following an adverse event. Patient Educ. Couns. 2019, 102, 1342–1349. [Google Scholar] [CrossRef] [PubMed]
- Oates, K. The new clinical leader. J. Paediatr. Child Health 2012, 48, 472–475. [Google Scholar] [CrossRef]
- Kennedy, D.M.; Anastos, C.T.; Genau, M.C. Improving healthcare service quality through performance management. Leadersh. Health Serv. 2019, 32, 477–492. [Google Scholar] [CrossRef]
- Li, A.N.; Tan, H.H. What happens when you trust your supervisor? Mediators of individual performance in trust relationships. J. Organ. Behav. 2012, 34, 407–425. [Google Scholar] [CrossRef]
- Ramani, S.; Könings, K.D.; Mann, K.V.; Pisarski, E.E.; Van Der Vleuten, C.P. About politeness, face, and feedback. Acad. Med. 2018, 93, 1348–1358. [Google Scholar] [CrossRef]
- Strandås, M.; Bondas, T. The nurse-patient relationship as a story of health enhancement in community care: A meta-ethnography. J. Adv. Nurs. 2017, 74, 11–22. [Google Scholar] [CrossRef]
- Vanhaecht, K. In search of Mangomoments. Lancet Oncol. 2018, 19, 165. [Google Scholar] [CrossRef]
- Brown, A.E.; Benoit, D.; Azoulay, E.; Butler, T.P.; Folcarelli, P.; Geller, G.; Rozenblum, R.; Sands, K.; Sokol-Hessner, L.; Talmor, D.; et al. The practice of respect in the ICU. Am. J. Respir. Crit. Care. Med. 2018, 197, 1389–1395. [Google Scholar] [CrossRef]
- Hillen, M.A.; De Haes, H.C.J.M.; Smets, E.M.A. Cancer patients’ trust in their physician-a review. Psycho-Oncology 2011, 20, 227–241. [Google Scholar] [CrossRef]
- Bäck, E.; Wikblad, K. Privacy in hospital. J. Adv. Nurs. 1998, 27, 940–945. [Google Scholar] [CrossRef]
- Oztürk, H.; Sayligil, O.; Musmul, A.; Acar, N.E. The perception of privacy in the emergency department: Medical faculty hospital as a case in point. Konuralp Tıp Derg. 2018, 10, 26–33. [Google Scholar] [CrossRef]
- Rojas, M. Respect to the Privacy in ICU. By María Rojas–Proyecto HU-CI. 2016. Available online: https://humanizandoloscuidadosintensivos.com/en/respect-to-privacy-in-icu-by-maria-rojas/ (accessed on 4 July 2019).
- Halpern, N.A. Innovative designs for the smart ICU. Chest 2014, 145, 646–658. [Google Scholar] [CrossRef]
- Vincent, J. The Hospital of Tomorrow: An ICU Perspective. International Hospital. 2019. Available online: https://www.interhospi.com/detail/international-hospital/the-hospital-of-tomorrow-an-icu-perspective/ (accessed on 4 July 2019).
- Watson, N.; Gibson, C.; Nowatzke, R.; Monsma, N. 1175: Bedside rounds or table rounds in the ICU? Crit. Care Med. 2018, 46, 571. [Google Scholar] [CrossRef]
- Hei, C.H.; Ismail, A.; Choy, H.H. Indicators for medical mistrust in healthcare–A review and standpoint from southeast asia. Malays. J. Med Sci. 2017, 24, 5–20. [Google Scholar] [CrossRef]
- Ågård, A.S.; Hofhuis, J.G.; Koopmans, M.; Gerritsen, R.T.; Spronk, P.E.; Engelberg, R.A.; Curtis, J.R.; Zijlstra, J.G.; Jensen, H.I. Identifying improvement opportunities for patient- and family-centered care in the ICU: Using qualitative methods to understand family perspectives. J. Crit. Care 2019, 49, 33–37. [Google Scholar] [CrossRef]
- Belseck, N. The reality of palliation. Med. Chronical 2019, 5, 4–7. [Google Scholar]
- Brasel, K.; Condron, M. End of life issues. In Surgical Ethics; Springer International Publishing: Heidelberg, Germany, 2019; pp. 239–248. [Google Scholar]
- Cheraghi, M.A.; Bahramnezhad, F.; Mehrdad, N. Review of ordering don’t resuscitate in Iranian dying patients. J. Relig. Health 2017, 57, 951–959. [Google Scholar] [CrossRef]
- Höglund, A.T.; Falkenström, E. The status of ethics in Swedish health care management: A qualitative study. BMC Health Serv. Res. 2018, 18, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Henderson, S.; Horne, M.; Hills, R.; Kendall, E. Cultural competence in healthcare in the community: A concept analysis. Health Soc. Care Community 2018, 26, 590–603. [Google Scholar] [CrossRef]
- Raynor, J.; Cervellione, K.; Curiel-Duran, L.; Ullah, T.; Patel, M. Resident Cultural Competence in the ICU. Am. J. Respir. Crit. Care Med. 2019, 199, A1370. [Google Scholar] [CrossRef]
- Brown, E.M.A.; Gabe, J. From patient deference towards negotiated and precarious informality: An Eliasian analysis of English general practitioners’ understandings of changing patient relations. Soc. Sci. Med. 2015, 146, 164–172. [Google Scholar] [CrossRef]
- Althubaiti, A. Information bias in health research: Definition, pitfalls, and adjustment methods. J. Multidiscip. Health 2016, 9, 211–217. [Google Scholar] [CrossRef]
- Poncet, M.C.; Toullic, P.; Papazian, L.; Kentish-Barnes, N.; Timsit, J.-F.; Pochard, F.; Chevret, S.; Schlemmer, B.; Azoulay, É. Burnout syndrome in critical care nursing staff. Am. J. Respir. Crit. Care Med. 2007, 175, 698–704. [Google Scholar] [CrossRef]
- Embriaco, N.; Azoulay, E.; Barrau, K.; Kentish, N.; Pochard, F.; Loundou, A.; Papazian, L. High level of burnout in intensivists. Am. J. Respir. Crit. Care Med. 2007, 175, 686–692. [Google Scholar] [CrossRef]
- Allen, I.E.; Seaman, C.A. Statistics roundtable: Likert scales and data analyses. Qual. Prog. 2007, 40, 64–65. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Mayer & Davis [26] | Hall et al. [25] | Nooteboom [28,29] | |
|---|---|---|---|
| Ability | The group of skills, competencies, and characteristics that enable a party to have influence within some specific domain | - | - |
| Benevolence | The extent to which a trustee is believed to want to do good to the trustor, aside from an egocentric profit motive | - | - |
| Competence | - | Producing the best achievable results and avoiding mistakes | Including but not exclusively, skills and knowledge concerning production of goods or services, employing technology or building and maintaining relations with other people |
| Confidentiality | - | Proper use of data and privacy | - |
| Fidelity | - | Acting in the best interest of the patient and not taking advantage of their vulnerability | - |
| Global trust | - | - A collective concept for concerns which have a strong connection with some areas but do not fit in one | - |
| - A more holistic aspect of trust, as it is reasonable to expect that trust has a significant component which is not divisible | |||
| Honesty | - | Telling the truth and evasion of intentional lies | Trust in the truthfulness of an actor, this actor often is the only information source |
| Integrity | The relationship between integrity and trust involves the trustor’s perception that the trustee adheres to a set of principles that the trustor finds acceptable | - | - |
| Intention | - | - | The expectation that the partner will not behave opportunistically |
| Outcome | The outcome of the trusting behavior (favorable or unfavorable) will influence trust indirectly through the perceptions of ability, benevolence, and integrity at the next interaction | - | - |
| Perceived risk | Involves the risks that are identified by trustee and trustor | - | - |
| Risk-taking in relations | differentiates the outcomes of trust from general risk-taking behaviors because it can occur only in the context of a specific, identifiable relationship with another party | - | - |
| Concept | Dimensions | Operational Definition |
|---|---|---|
| Competence | Communication competence | The perception of the respondent regarding the ability of the HCP build and maintain relations with other people as well as being able to make themselves understood, and understand others. |
| Other types of competence | The perception of the respondent regarding skills and knowledge concerning production of goods or services, employing technology Intention. | |
| Intention | Opportunism | The perception of respondents regarding endangerment of the relationship by the HCP. |
| Lack of dedication or care | The perception of the respondent regarding the effort and attention shown by the HCP. | |
| Good intentions | The perception of the respondent regarding the loyalty, caring, respect, advocacy or avoiding conflicts of interest by HCP. | |
| Integrity | Honesty | The perception of the respondent regarding if the HCP tells the truth and avoids lies. |
| Dishonesty | The perception of the respondent regarding if HCP lie, or tell half-truths, even if they are confronted with their lies/deceptions. | |
| Lack of honesty or incomplete honesty | The perception of the respondent regarding if HCP lie or tell half-truths. | |
| Global trust | Collective concept | The perception of the respondent regarding concerns which have a strong connection with some areas but do not fit in one. |
| Holistic aspect of trust | The perception of the respondent regarding the expectation that trust has a significant component which is not divisible. | |
| Risk | The perception of the respondent regarding the risks they have undergone in the trust relationship. | |
| Outcome | Above expectations | The perception of the respondent regarding the exceeding of the expectations. |
| In line with expectations | The perception of the respondent regarding if the expectations have been met. | |
| Below expectations | The perception of the respondent regarding the failing of expectations. |
| Respondent | Patient/Partner | Male/Female (Patient) | Age (Patient) | LOS (on the ICU)/Time of Employance |
|---|---|---|---|---|
| Intensivist/Nurse | ||||
| Patient 1 | Patient + partner | F | 38 | 28 days |
| Patient 2 | Patient | M | 67 | 8 days |
| Patient 3 | Partner | M | 64 | 6 days |
| Patient 4 | Partner | F | 30 | 1 day |
| Patient 5 | Partner | M | 51 | 10 days |
| Patient 6 | Partner | M | 62 | 9 weeks |
| Patient 7 | Partner | M | 37 | 5 weeks |
| Patient 8 | Patient | F | 68 | 2 days |
| HCP 1 | Nurse | F | - | - |
| HCP 2 | Nurse | M | - | 31 years |
| HCP 3 | Intensivist | M | - | 2 years |
| HCP 4 | Intensivist | F | - | 16 years |
| HCP 5 | Nurse | F | - | 15 years |
| HCP 6 | Intensivist | M | - | 2.5 years |
| HCP 7 | Intensivist | M | - | 10 years |
| HCP 8 | Intensivist | F | - | 14 years |
| Communication Competence | Attributes | Total (P/F; HCP) |
|---|---|---|
| Explaining | Should be clear, fitting to the patients/partners preferences and intelligence, and have a confirmatory element | 15 (7:8) |
| Personal contact | The behavior and courtesy of HCPs | 11 (6:5) |
| Medical contact/information | The clarity regarding where or with whom patients/family should receive medical information | 8 (6:2) |
| Coordination | Alignments between HCPs regarding patient communication | 6 (5:1) |
| Listening | Hear what the patient and/or family explain | 7 (3:4) |
| Relevance of communication | Understanding of the power of communication | 8 (2:6) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lemmers, A.L.; van der Voort, P.H.J. Trust in Intensive Care Patients, Family, and Healthcare Professionals: The Development of a Conceptual Framework Followed by a Case Study. Healthcare 2021, 9, 208. https://doi.org/10.3390/healthcare9020208
Lemmers AL, van der Voort PHJ. Trust in Intensive Care Patients, Family, and Healthcare Professionals: The Development of a Conceptual Framework Followed by a Case Study. Healthcare. 2021; 9(2):208. https://doi.org/10.3390/healthcare9020208
Chicago/Turabian StyleLemmers, Anne Lotte, and Peter H. J. van der Voort. 2021. "Trust in Intensive Care Patients, Family, and Healthcare Professionals: The Development of a Conceptual Framework Followed by a Case Study" Healthcare 9, no. 2: 208. https://doi.org/10.3390/healthcare9020208
APA StyleLemmers, A. L., & van der Voort, P. H. J. (2021). Trust in Intensive Care Patients, Family, and Healthcare Professionals: The Development of a Conceptual Framework Followed by a Case Study. Healthcare, 9(2), 208. https://doi.org/10.3390/healthcare9020208