
Comparison of Activity in Scapular Stabilizing Muscles during Knee Push-Up Plus and Modified Vojta’s 3-Point Support Exercises

Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Electromyographic Recording and Data Analysis
2.3. Procedures
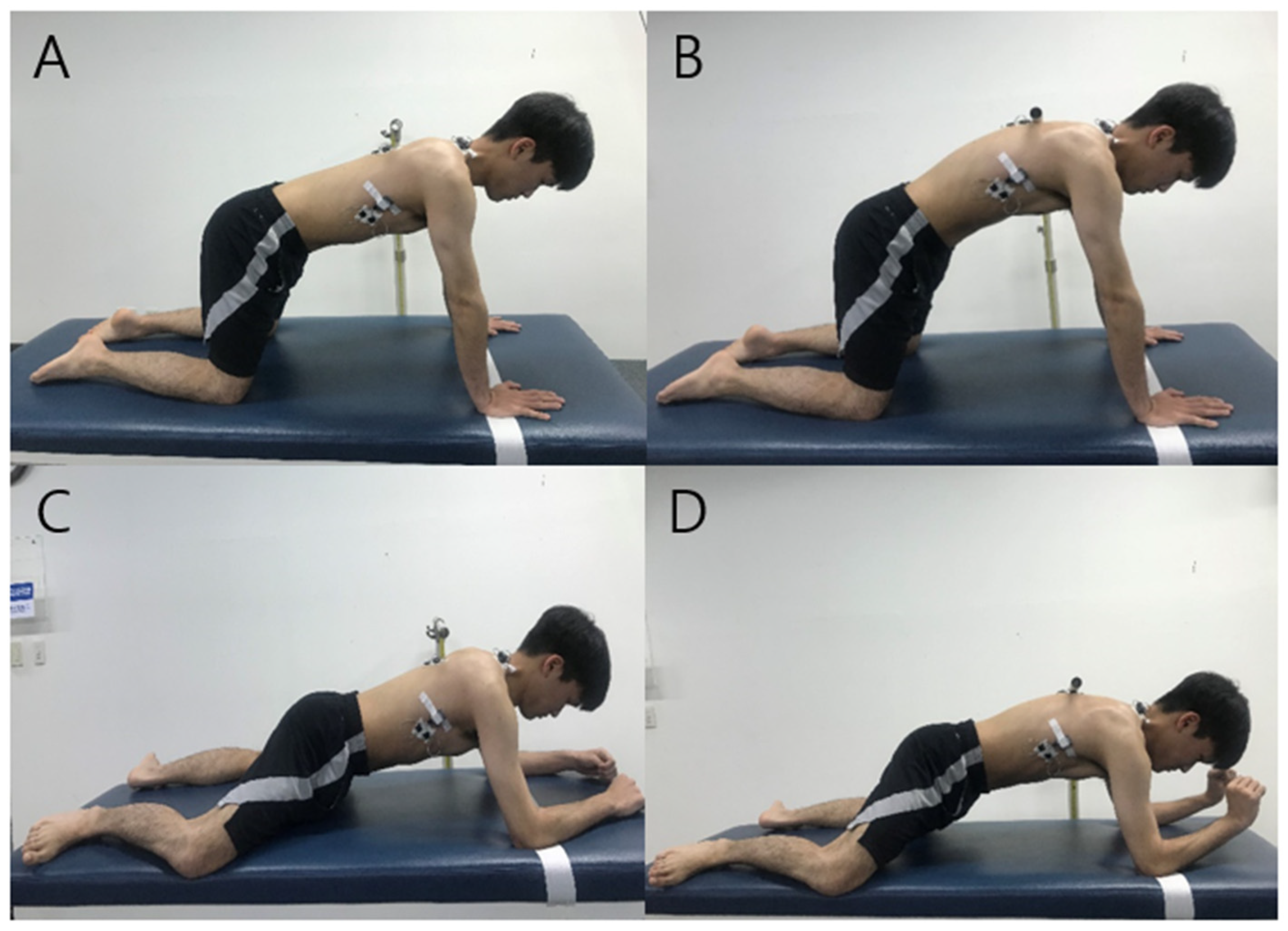
2.3.1. Knee Push-Up Plus
2.3.2. Modified Vojta’s 3-Point Support
2.4. Statistical Analysis
3. Results
3.1. General Characteristics of the Subjects
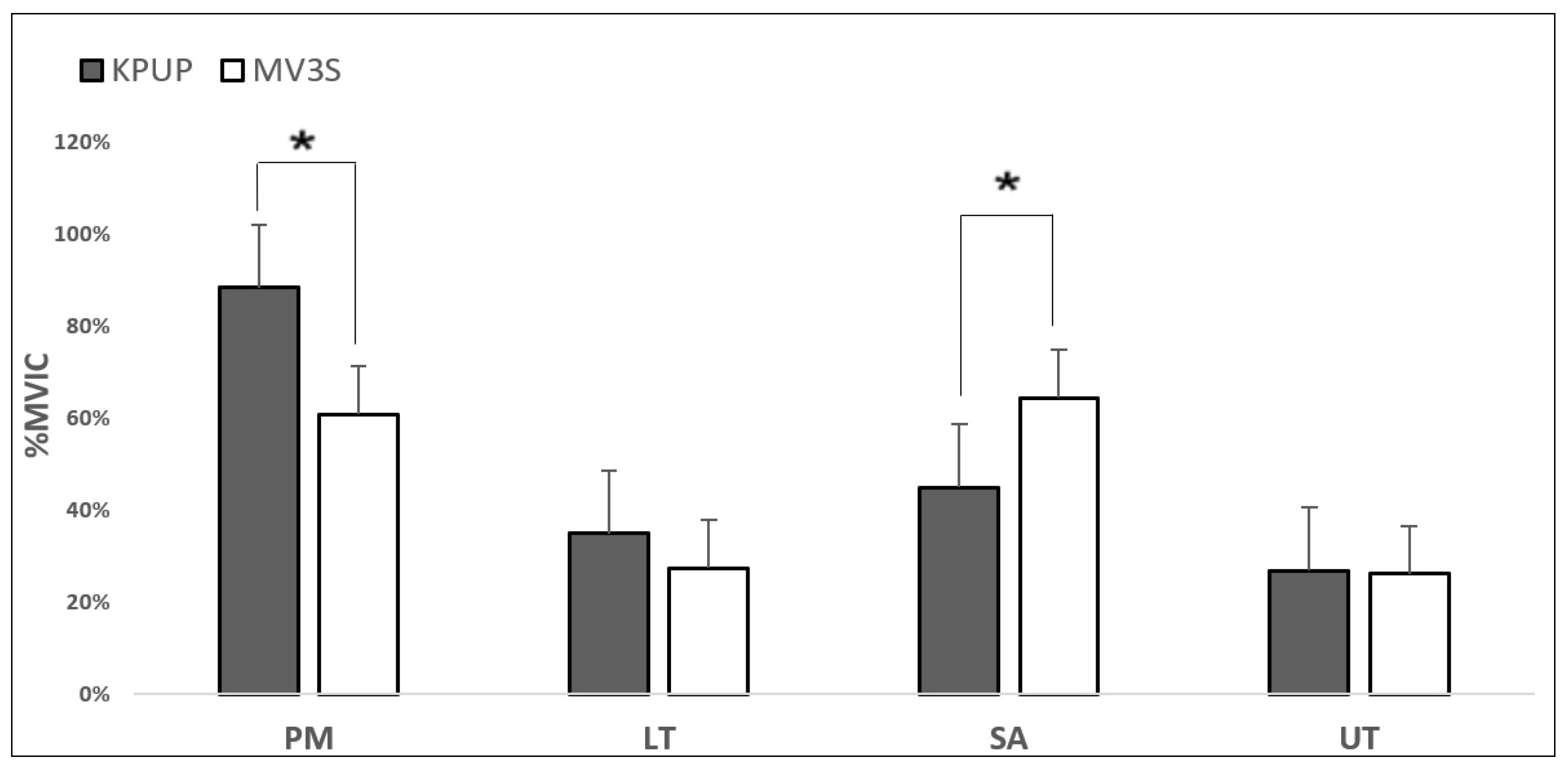
3.2. Comparison of Muscle Activity between Scapular Stabilizers during KPUP and MV3PS
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Curl, L.; Warren, R.F. Glenohumeral joint stability. Selective cutting studies on the static capsular restraints. Clin. Orthop. Relat. Res. 1996, 1996, 54–65. [Google Scholar] [CrossRef]
- De Mey, K.; Danneels, L.; Cagnie, B.; Borms, D.; T’Jonck, Z.; Van Damme, E.; Cools, A.M. Shoulder Muscle Activation Levels During Four Closed Kinetic Chain Exercises With and Without Redcord Slings. J. Strength Cond. Res. 2014, 28, 1626–1635. [Google Scholar] [CrossRef] [PubMed]
- Chester, R.; Smith, T.; Hooper, L.; Dixon, J. The impact of subacromial impingement syndrome on muscle activity patterns of the shoulder complex: A systematic review of electromyographic studies. BMC Musculoskelet. Disord. 2010, 11, 45. [Google Scholar] [CrossRef] [PubMed]
- Ludewig, P.M.; Braman, J.P. Shoulder impingement: Biomechanical considerations in rehabilitation. Man. Ther. 2011, 16, 33–39. [Google Scholar] [CrossRef]
- Phadke, V.; Camargo, P.; Ludewig, P. Scapular and rotator cuff muscle activity during arm elevation: A review of normal function and alterations with shoulder impingement. Braz. J. Phys. Ther. 2009, 13, 1–9. [Google Scholar] [CrossRef]
- Ludewig, P.M.; Reynolds, J.F. The association of scapular kinematics and glenohumeral joint pathologies. J. Orthop. Sports Phys. Ther. 2009, 39, 90–104. [Google Scholar] [CrossRef]
- Escamilla, R.F.; Yamashiro, K.; Paulos, L.; Andrews, J.R. Shoulder Muscle Activity and Function in Common Shoulder Rehabilitation Exercises. Sports Med. 2009, 39, 663–685. [Google Scholar] [CrossRef] [PubMed]
- Donald, A.N. Kinesiology of the Musculoskeletal System; Mosby: Maryland Heights, MO, USA, 2002. [Google Scholar]
- Ludewig, P.M.; Hoff, M.S.; Osowski, E.E.; Meschke, S.A.; Rundquist, P.J. Relative Balance of Serratus Anterior and Upper Trapezius Muscle Activity during Push-Up Exercises. Am. J. Sports Med. 2004, 32, 484–493. [Google Scholar] [CrossRef] [PubMed]
- Lukasiewicz, A.C.; McClure, P.; Michener, L.; Pratt, N.; Sennett, B.; Ludewig, P. Comparison of 3-Dimensional Scapular Position and Orientation Between Subjects With and Without Shoulder Impingement. J. Orthop. Sports Phys. Ther. 1999, 29, 574–586. [Google Scholar] [CrossRef]
- Castelein, B.; Cagnie, B.; Parlevliet, T.; Cools, A. Serratus anterior or pectoralis minor: Which muscle has the upper hand during protraction exercises? Man. Ther. 2016, 22, 158–164. [Google Scholar] [CrossRef]
- Decker, M.J.; Hintermeister, R.A.; Faber, K.J.; Hawkins, R.J. Serratus Anterior Muscle Activity During Selected Rehabilitation Exercises. Am. J. Sports Med. 1999, 27, 784–791. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.; Gong, W.; Lee, S.-Y. The Effect of Push-up Plus Exercise with Visual Biofeedback on The Activity of Shoulder Stabilizer Muscles for Winged Scapula. J. Phys. Ther. Sci. 2010, 22, 355–358. [Google Scholar] [CrossRef][Green Version]
- Konrad, G.G.; Jolly, J.T.; Labriola, J.E.; McMahon, P.J.; Debski, R.E. Thoracohumeral muscle activity alters glenohumeral joint biomechanics during active abduction. J. Orthop. Res. 2006, 24, 748–756. [Google Scholar] [CrossRef]
- Labriola, J.E.; Lee, T.Q.; Debski, R.E.; McMahon, P.J. Stability and instability of the glenohumeral joint: The role of shoulder muscles. J. Shoulder Elb. Surg. 2005, 14, S32–S38. [Google Scholar] [CrossRef]
- McMahon, P.J.; Chow, S.; Sciaroni, L.; Yang, B.Y.; Lee, T.Q. A novel cadaveric model for anterior-inferior shoulder dislocation using forcible apprehension positioning. J. Rehabilitation Res. Dev. 2014, 40, 349–359. [Google Scholar] [CrossRef]
- Vojta, V.; Peters, A. Das Vojta-Prinzip: Muskelspiele in Reflexfortbewegung und Motorischer Ontogenese; Springer: Berlin/Heidelberg, Germany, 2007. [Google Scholar]
- Ellenbecker, T.S.; Davies, G.J. Closed Kinetic Chain Exercise: A Comprehensive Guide to Multiple Joint Exercise; Human Kinetics: Champaign, IL, USA, 2001. [Google Scholar]
- Hok, P.; Opavský, J.; Kutín, M.; Tüdös, Z.; Kaňovský, P.; Hluštík, P. Modulation of the sensorimotor system by sustained manual pressure stimulation. Neuroscience 2017, 348, 11–22. [Google Scholar] [CrossRef] [PubMed]
- Sanz-Esteban, I.; Calvo-Lobo, C.; Ríos-Lago, M.; Álvarez-Linera, J.; Muñoz-García, D.; Rodríguez-Sanz, D. Mapping the human brain during a specific Vojta’s tactile input: The ipsilateral putamen’s role. Medcine 2018, 97, e0253. [Google Scholar] [CrossRef]
- Hok, P.; Opavský, J.; Labounek, R.; Kutín, M.; Šlachtová, M.; Tüdös, Z.; Kaňovský, P.; Hluštík, P. Differential Effects of Sustained Manual Pressure Stimulation According to Site of Action. Front. Neurosci. 2019, 13, 722. [Google Scholar] [CrossRef] [PubMed]
- Sanz-Esteban, I.; Cano-De-La-Cuerda, R.; San-Martín-Gómez, A.; Jiménez-Antona, C.; Monge-Pereira, E.; Estrada-Barranco, C.; Serrano, J.I. Cortical activity during sensorial tactile stimulation in healthy adults through Vojta therapy. A randomized pilot controlled trial. J. Neuroeng. Rehabil. 2021, 18, 1–13. [Google Scholar] [CrossRef]
- Sung, Y.-H.; Ha, S.-Y. The Vojta approach changes thicknesses of abdominal muscles and gait in children with spastic cerebral palsy: A randomized controlled trial, pilot study. Technol. Health Care 2020, 28, 293–301. [Google Scholar] [CrossRef]
- Horsak, B.; Kiener, M.; Pötzelsberger, A.; Siragy, T. Serratus anterior and trapezius muscle activity during knee push-up plus and knee-plus exercises performed on a stable, an unstable surface and during sling-suspension. Phys. Ther. Sport 2017, 23, 86–92. [Google Scholar] [CrossRef]
- Baechle, T.R.; Earle, R.W. Essentials of Strength Training and Conditioning; Human Kinetics: Champaign, IL, USA, 2008. [Google Scholar]
- Maeo, S.; Chou, T.; Yamamoto, M.; Kanehisa, H. Muscular activities during sling- and ground-based push-up exercise. BMC Res. Notes 2014, 7, 192. [Google Scholar] [CrossRef]
- Ekstrom, R.A.; Soderberg, G.L.; Donatelli, R.A. Normalization procedures using maximum voluntary isometric contractions for the serratus anterior and trapezius muscles during surface EMG analysis. J. Electromyogr. Kinesiol. 2005, 15, 418–428. [Google Scholar] [CrossRef] [PubMed]
- Park, K.-M.; Cynn, H.-S.; Kwon, O.; Yi, C.-H.; Yoon, T.-L.; Lee, J.-H. Comparison of Pectoralis Major and Serratus Anterior Muscle Activities During Different Push-Up Plus Exercises in Subjects With and Without Scapular Winging. J. Strength Cond. Res. 2014, 28, 2546–2551. [Google Scholar] [CrossRef] [PubMed]
- Seo, S.-H.; Jeon, I.-H.; Cho, Y.-H.; Lee, H.-G.; Hwang, Y.-T.; Jang, J.-H. Surface EMG during the Push-up plus Exercise on a Stable Support or Swiss Ball: Scapular Stabilizer Muscle Exercise. J. Phys. Ther. Sci. 2013, 25, 833–837. [Google Scholar] [CrossRef] [PubMed]
- Uhl, T.L.; Carver, T.J.; Mattacola, C.G.; Mair, S.D.; Nitz, A.J. Shoulder Musculature Activation During Upper Extremity Weight-Bearing Exercise. J. Orthop. Sports Phys. Ther. 2003, 33, 109–117. [Google Scholar] [CrossRef] [PubMed]
- Contreras, B.; Schoenfeld, B.; Mike, J.; Tiryaki-Sonmez, G.; Cronin, J.; Vaino, E. The biomechanics of the push-up: Implications for resistance training programs. Strength Cond. J. 2012, 34, 41–46. [Google Scholar] [CrossRef]
- Gajewska, E.; Huber, J.; Kulczyk, A.; Lipiec, J.; Sobieska, M. An attempt to explain the Vojta therapy mechanism of action using the surface polyelectromyography in healthy subjects: A pilot study. J. Bodyw. Mov. Ther. 2018, 22, 287–292. [Google Scholar] [CrossRef]
- Ebben, W.P.; Wurm, B.; VanderZanden, T.L.; Spadavecchia, M.L.; Durocher, J.J.; Bickham, C.T.; Petushek, E. Kinetic Analysis of Several Variations of Push-Ups. J. Strength Cond. Res. 2011, 25, 2891–2894. [Google Scholar] [CrossRef]
- Hintermeister, R.A.; Lange, G.W.; Schultheis, J.M.; Bey, M.J.; Hawkins, R.J. Electromyographic Activity and Applied Load During Shoulder Rehabilitation Exercises Using Elastic Resistance. Am. J. Sports Med. 1998, 26, 210–220. [Google Scholar] [CrossRef]
- De Luca, C.J.; Basmajian, J.V. Muscles Alive: Their Functions Revealed by Electromyography; Wiliams & Wilkins: Philadelphia, PA, USA, 1985. [Google Scholar]
- Martins, J.; Tucci, H.T.; Andrade, R.; Araújo, R.C.; Bevilaqua-Grossi, D.; Oliveira, A.S. Electromyographic Amplitude Ratio of Serratus Anterior and Upper Trapezius Muscles During Modified Push-Ups and Bench Press Exercises. J. Strength Cond. Res. 2008, 22, 477–484. [Google Scholar] [CrossRef] [PubMed]
- Ha, S.-M.; Kwon, O.-Y.; Cynn, H.-S.; Lee, W.-H.; Park, K.-N.; Kim, S.-H.; Jung, D.-Y. Comparison of electromyographic activity of the lower trapezius and serratus anterior muscle in different arm-lifting scapular posterior tilt exercises. Phys. Ther. Sport 2012, 13, 227–232. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Gender | Number of Subjects | Age (Years) | Height (cm) | Weight (kg) |
|---|---|---|---|---|
| Male | 19 | 20.86 ± 2.31 | 168.00 ± 7.13 | 63.9 ± 11.50 |
| Female | 21 | 21.02 ± 2.24 | 167.80 ± 7.21 | 62.6 ± 10.50 |
| Muscle | KPUP | MV3PS | p | Effect Size |
|---|---|---|---|---|
| Mean ± SD | Mean ± SD | |||
| PM | 88.28 ± 11.40 | 60.76 ± 9.76 | <0.001 * | 0.720 |
| LT | 34.91 ± 6.95 | 27.43 ± 3.25 | 0.276 | 0.175 |
| SA | 44.88 ± 3.69 | 64.36 ± 6.04 | <0.001 * | 0.678 |
| UT | 26.86 ± 5.44 | 26.10 ± 4.29 | 0.880 | 0.024 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lim, H. Comparison of Activity in Scapular Stabilizing Muscles during Knee Push-Up Plus and Modified Vojta’s 3-Point Support Exercises. Healthcare 2021, 9, 1636. https://doi.org/10.3390/healthcare9121636
Lim H. Comparison of Activity in Scapular Stabilizing Muscles during Knee Push-Up Plus and Modified Vojta’s 3-Point Support Exercises. Healthcare. 2021; 9(12):1636. https://doi.org/10.3390/healthcare9121636
Chicago/Turabian StyleLim, Hyoungwon. 2021. "Comparison of Activity in Scapular Stabilizing Muscles during Knee Push-Up Plus and Modified Vojta’s 3-Point Support Exercises" Healthcare 9, no. 12: 1636. https://doi.org/10.3390/healthcare9121636
APA StyleLim, H. (2021). Comparison of Activity in Scapular Stabilizing Muscles during Knee Push-Up Plus and Modified Vojta’s 3-Point Support Exercises. Healthcare, 9(12), 1636. https://doi.org/10.3390/healthcare9121636