
Usability of Telemedicine Mobile Applications during COVID-19 in Saudi Arabia: A Heuristic Evaluation of Patient User Interfaces


Abstract
:1. Introduction
2. Materials and Methods
2.1. Phase I. Telemedicine Apps Selection
Apps Description
2.2. Phase II. Evaluation Procedure
2.3. Phase III. Data Analysis
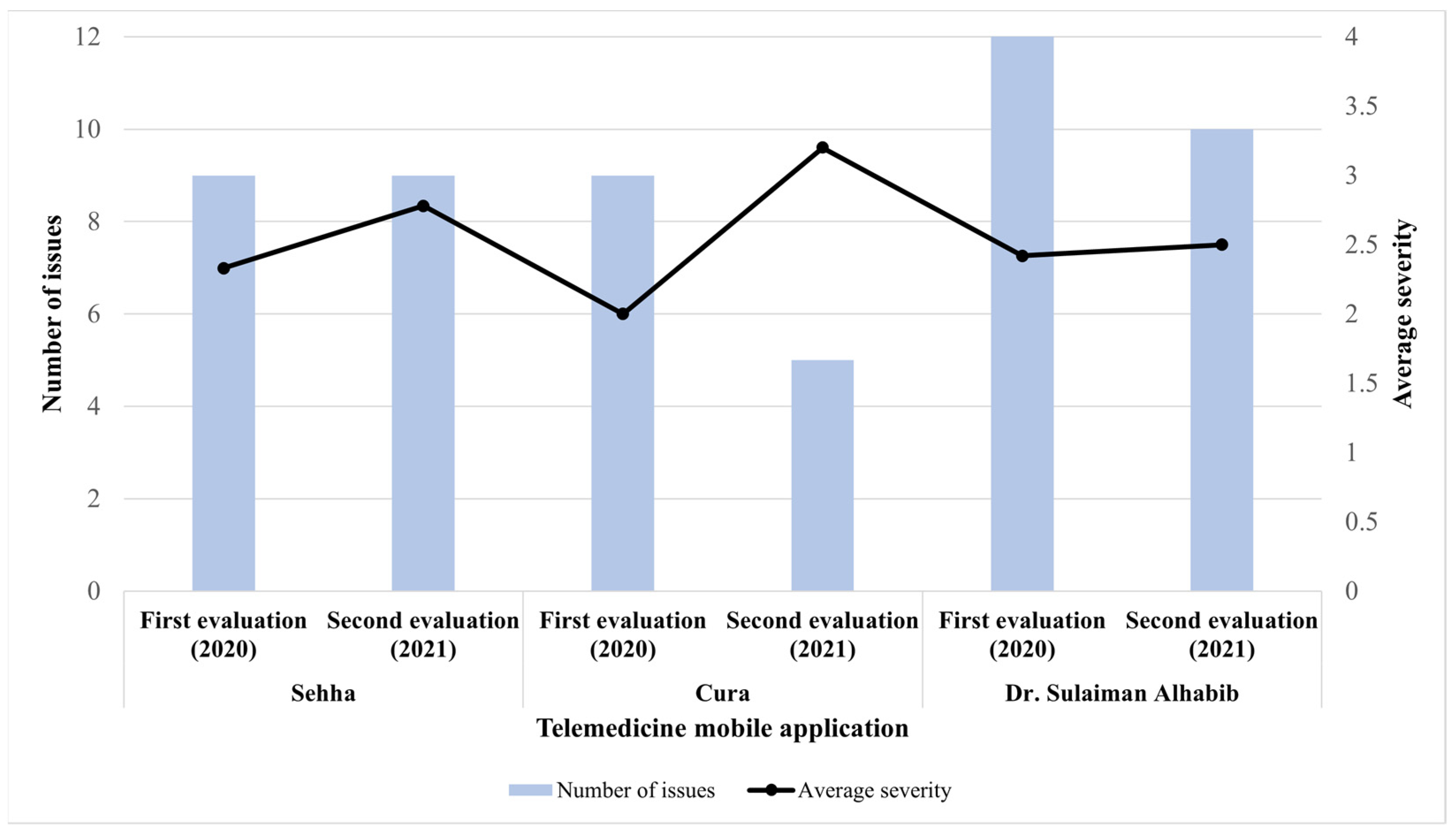
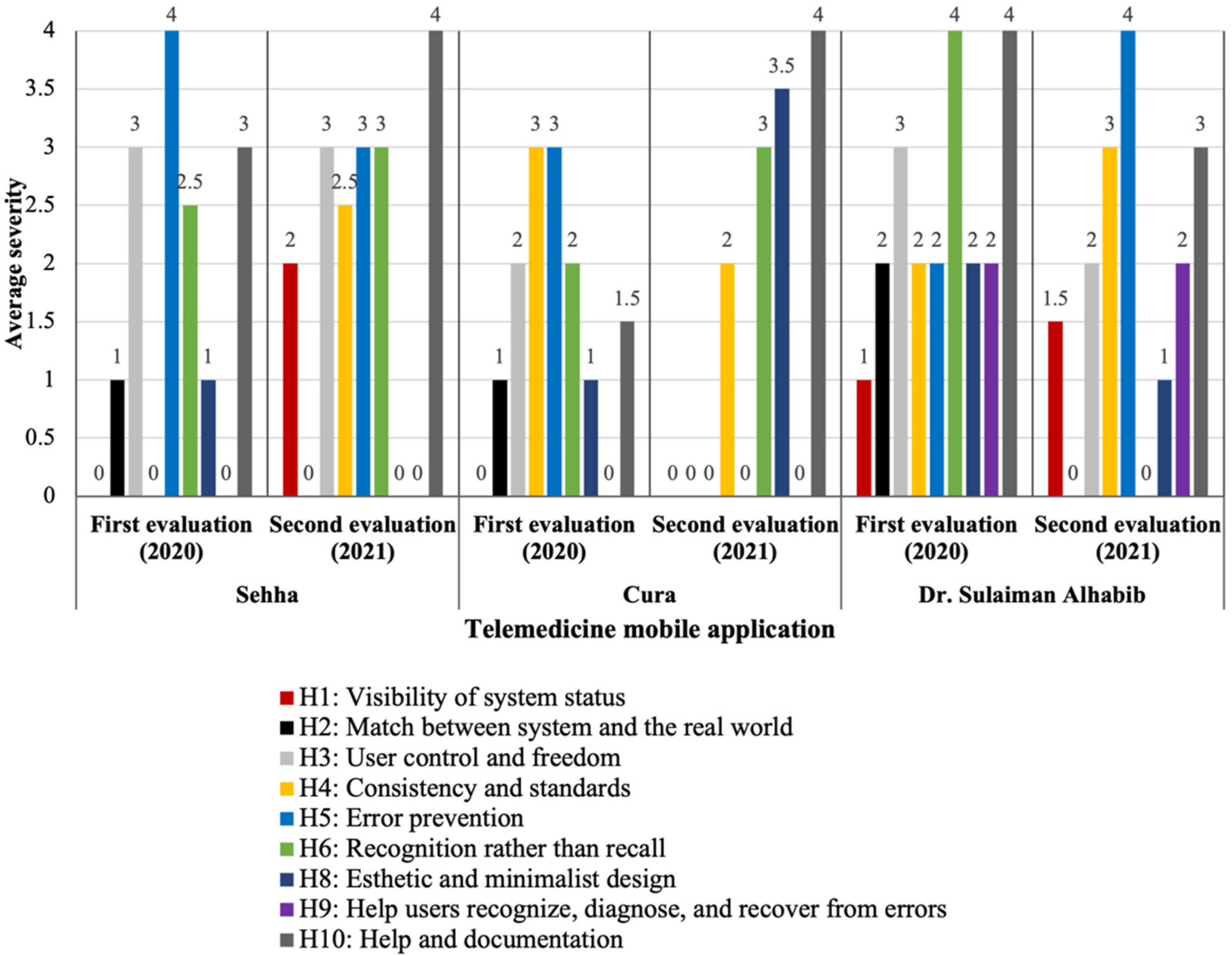
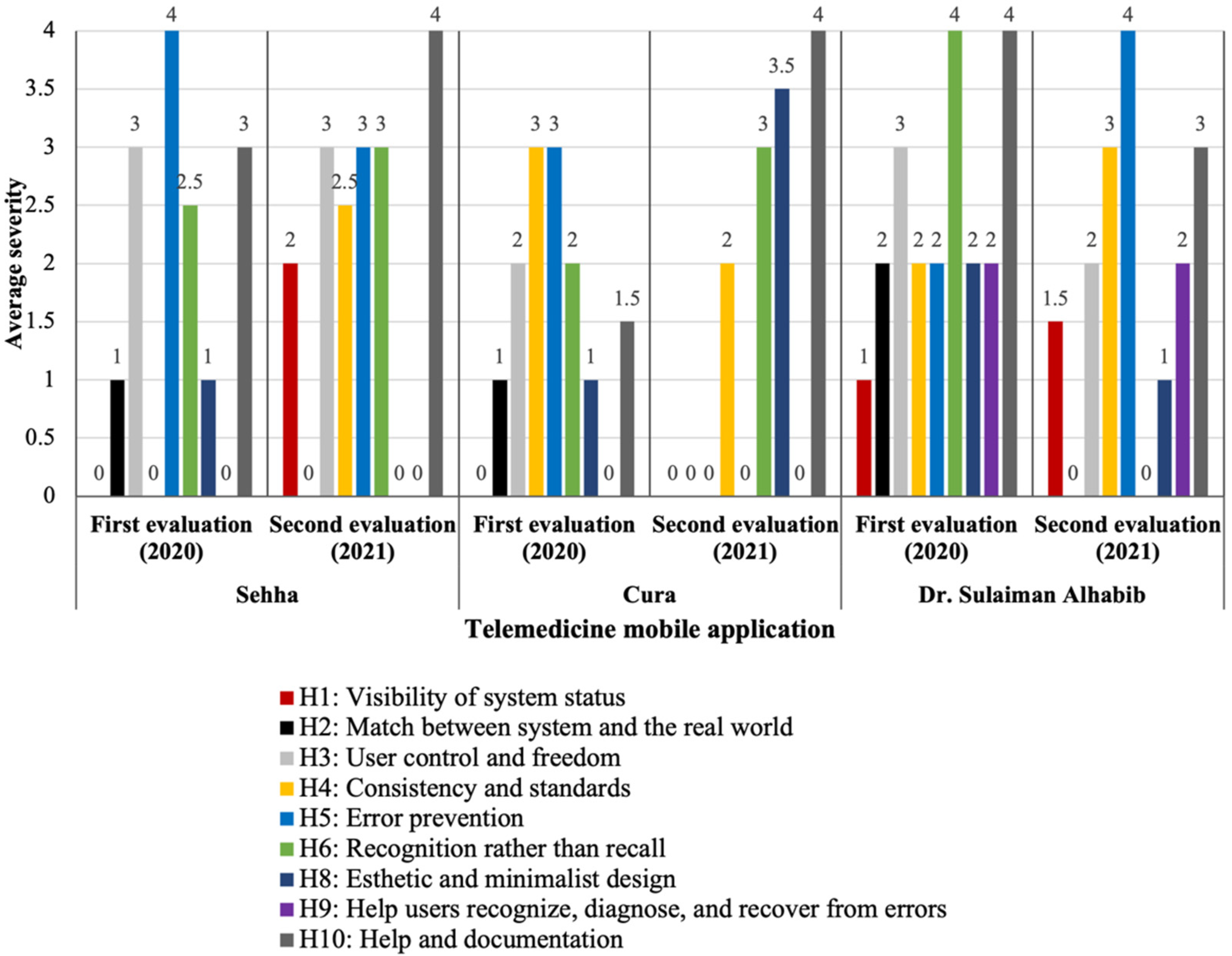
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| No. | mHealth App | App Summary Description |
|---|---|---|
| 1 | Seha | Developed by the Ministry of Health (MOH) providing health and preventive care through audio-video medical consultations by MOH’s specialists, and through artificial intelligence technologies. |
| 2 | Mawid | Developed by the Ministry of Health (MOH), to enable patient to book their appointments across primary health care centers and manage them by canceling or rescheduling. As well as managing their referral appointments. |
| 3 | Asefni | Developed by the Saudi Red Crescent Authority providing ambulance emergency services in Saudi Arabia |
| 4 | Dr. Suliman Alhabib | Developed by Dr. Sulaiman Al Habib Medical Services Group providing access to patient portal services (such as managing medical records, checking lab results and radiology reports, booking appointments, checking prescriptions) and telemedicine care. |
| 5 | Cura | Developed by Ubieva providing healthcare services 24/7 from a distance. |
| 6 | Kingdom Hospital | Developed by the Kingdom Hospital providing patient portal services (such as managing medical records, checking lab results and radiology reports, booking appointments, checking prescriptions). |
| 7 | Web Teb | Developed by Web Teb proving health and medical news and accurate health information for consumers. |
| 8 | Nahdi | Developed by Al Nahdi Medical Company as a pharmacy app delivering pharmaceutical needs to customers. |
| 9 | Al dawaa Pharmacies | Developed by Al-Dawaa Medical Services Co as a pharmacy app delivering pharmaceutical needs to customers. |
| 10 | Mouwasat Medical Services | Developed by Mouwasat Medical Services providing services, which allow patients to book appointments, choose nearest hospital and required medical specialty. |
Appendix B
- Seha
- Dr. Suliman Alhabib
- Cura
- Private
- Governmental
- Yes
- No
- COVID-19 screening information
- COVID-19 self-assessment tool
- Ability to choose a certain physician
- Ability to see physician details
- Text messaging
- Voice messaging
- Video call
- Ability to attach and send files
- Ability to schedule a tele-consultation
- Ability to receive on demand consultation
- Prescription
- Link to patient medical record
- Ability to view past consultation
- Satisfaction survey
| 0—May Not Be a Problem | 1—Cosmetic Problem Only | 2—Minor Usability Problem | 3—Major Usability Problem | 4—Usability Catastrophe | |
| Visibility of system status | |||||
| Match between system and the real world | |||||
| User control and freedom | |||||
| Consistency and standards | |||||
| Error prevention | |||||
| Recognition rather than recall | |||||
| Flexibility and efficiency of use | |||||
| Esthetic and minimalist design | |||||
| Help users recognize, diagnose, and recover from errors | |||||
| Help and documentation |
Appendix C
| # | Heuristic Item | Evaluation Period | Usability Issue Description | Location | Rating | Redesign Recommendation |
|---|---|---|---|---|---|---|
| 1 | Visibility of system status | First (2020) | No identified | |||
| Second (2021) | The timer in the consultation room: unclear what it reflects. Does it reflect the user consultation time limit or the waiting time to see the physician? | During consultation | 3 | Add description of timer, i.e., waiting time to see physician or consultation duration. | ||
| It took a while to load the consultation page to start consultation with physician. | Waiting for physician | 1 | Add a message indicating “loading”. | |||
| 2 | Match between system and the real world | First (2020) | User may not understand the meaning of “artificial intelligence” feature named “Smart Seha” | Log in | 1 | Add a definition of “Smart Seha” for the user in lay terms such as an “electronic tool that helps you understand your symptoms and recommends some actions”. |
| Second (2021) | None identified | |||||
| 3 | User control and freedom | First (2020) | On the “consult physician” screen- when the user enters information, chooses “live session”, then chooses to cancel after seeing the waiting time, the app doesn’t go back to the previous screen “consult physician”, the app takes the user to the home screen. | Consultation initiation | 3 | Allow the app to take the user to the previous screen and not the home screen. |
| † If the user screen goes static, the app does not give a notification to the user that a physician is present in the session and the app automatically ends the consultation without the option of going back to the session. | Waiting for physician | 3 | Allow the app to send a notification with sound to alert the user when a physician is present in the session and reply to the user. | |||
| Second (2021) | The “back” icon in the consultation room takes the user to the home screen and not to the previous page (page where the user entered the consultation details). This happens without giving a notification where the back icon will take the user. | Consultation initiation | 3 | Change the icon of the icon to show a “home” icon rather than an arrow indication “back”—or program the app to go to the previous page instead of the home. | ||
| The “back” icon and “end consultation” icon have the same functionality. | End of consultation | 3 | Differentiate between both icons by creating pages that reflect the functionality of the standard icon. | |||
| 4 | Consistency and adherence to standards | First (2020) | None identified | |||
| Second (2021) | Both “Smart Seha” and “health check” are artificial intelligence functionalities and it is unclear what the differences between these services are. | Log in | 2 | Add a description for each functionality in the home page. | ||
| The term “health check” may also reflect a tele-consultation with a physician. | Log in | 3 | Add a description for each functionality in the home page. | |||
| 5 | Error prevention | First (2020) | † No notification indicating that if the user screen is static, the consultation will end and will be counted towards the user’s monthly consultation limit. | Waiting for physician | 4 | Create a notification for the user upon entering the chat room, which indicates that the consultation session will end if no response comes from the user. |
| Second (2021) | When the user clicks on consultation by mistake, the app does not send a confirmation message to the user to start the consultation. This then counts as a consultation limit if the user decides to leave without seeing the physician. | Consultationinitiation | 3 | Allow the app to count active sessions (interaction between the physician and user)—as part of the monthly consultation limit and provide a follow-up on the experience of the consultation. | ||
| 6 | Recognition rather than recall | First (2020) | † Waiting time is only displayed before entering the consultation session room reflecting the time the user gets access to the room. When the user is in the room, waiting time for the physician to start the session is not displayed. | Waiting for physician | 2 | Provide a countdown timer within the consultation session screen showing the estimated waiting time for the physician to join. |
| After the user leaves the open consultation session, the icon for reentering the consultation is not clear for the user. | During consultation | 3 | Add “open consultation” icon with visible instructions in every page. | |||
| Second (2021) | When the user goes out of the consultation room by mistake, the app does not show a notification that “ you are in consultation”. | During consultation | 3 | Show a notification to user “you are in consultation”. | ||
| 7 | Flexibility and efficiency of use | No accelerators or ability to tailor frequent actions based on inexperienced and experienced users were found. | ||||
| 8 | Esthetic and minimalist design | First (2020) | Irrelative and unclear icons shown at the end after the “consultations page” to view the history of consultations indicating “closed”. This icon is “action required”. | End of consultation | 1 | Remove the “action required” icon from the closed consultations. |
| There are two icons that lead to the same function “starting the telemedicine consultation”. One accessed in the home screen “consultations” and the other in consultations “new”, which brings the user back to the home screen. | Consultation initiation | 1 | Remove the “new” tab from the consultations screen. Main dashboard might provide a summary of the features offered on a high-level. | |||
| Second (2021) | None identified | |||||
| 9 | Recognition diagnosis, and recovery from errors | First (2020) | None identified | |||
| Second (2021) | None identified | |||||
| 10 | Help and documentation | First (2020) | Quick start guide is only displayed to the users when the app is opened for the first time. | Log in | 3 | Provide users with ongoing access to help through an icon or tab placed in the chat room and/or in the home screen as user instructions. |
| Second (2021) | The app does not provide clear directions on how to use the app, and what each icon or label means. | Orientation | 4 | Provide any extra information that would be useful to users, along with the label. | ||
| Total Issues identified from the two evaluations: 18 | ||||||
| # | Heuristic Item | Evaluation Period | Usability Issue Description | Location | Rating | Redesign Recommendation |
|---|---|---|---|---|---|---|
| 1 | Visibility of system status | First (2020) | None identified | |||
| Second (2021) | None identified | |||||
| 2 | Match between system and the real world | First (2020) | User may not comprehend the meaning of “instant consultation” vs. “specialized consultation” and “find a doctor” vs. “instant consultation” vs. “specialized consultation” in a tele-consultation setting. | Consultation initiation | 1 | Help the user decide and select the option that fits their needs. For example, users start with “instant consultation” and from there they can be referred to a specialist if needed. |
| Second (2021) | None identified | |||||
| 3 | User control and freedom | First (2020) | † No exit icon or skip from the instructions page when the user clicks the icon (i). The user must go through all the instructions. | Orientation | 2 | Provide a skip icon to end the help instructions. |
| Second (2021) | None identified | |||||
| 4 | Consistency and adherence to standards | First (2020) | The search for “find a doctor” is not clear if the user is searching for the “specialized consultation” or the “instant consultation”. | Consultation initiation | 3 | Create separate search lists based on the user’s choice. |
| On the technical support page, the license number of some staff indicates “000” or other numbers. This is unclear to the user if it is not applicable, or the license number is not updated. | Orientation | 3 | Avoid using “000” and clearly indicate if the license number does not apply to certain staff. | |||
| Second (2021) | There are some pages displaying “instant consultation” and others displaying “specialized consultation”. | Consultationinitiation | 2 | Standardize the terms or add a description under each term to indicate the difference in service. | ||
| 5 | Error prevention | First (2020) | “Short brief about your case” indicates between brackets as (optional) when in fact it is mandatory to proceed to session payment. | Consultation initiation | 3 | Remove the word “optional”. |
| Second (2021) | None identified | |||||
| 6 | Recognition rather than recall | First (2020) | † On the “search for doctor” screen” the user may not recall what each doctor specialty icon on the left panel represents and the user may need to click on each icon to read the labels presented on the right panel. | Consultation initiation | 2 | Help users select the doctor specialty based on symptoms or area of body in the main page instead of browsing all doctor specialties. |
| Second (2021) | There is no specific icon that represents “help”. Help videos are displayed with other information under “find doctor” tab. | Orientation | 3 | Add an icon representing “help” where users can easily recall. | ||
| 7 | Flexibility and efficiency of use | No accelerators or ability to tailor frequent actions based on inexperienced and experienced users were found. | ||||
| 8 | Esthetic and minimalist design | First (2020) | The main “search for doctor” screen displays too much information in one screen i.e., name of doctor, picture, title, specialty, and rating. | Consultation initiation | 1 | The name of specialty may be removed since it is indicated under the main screen heading. Rating can also be removed as it is shown when the user clicks on a specific doctor. |
| Second (2021) | There is a tab to “find a doctor” and there is also the same tab under “clinic”. “Find doctor” tab includes several irrelevant information | Consultation initiation Consultation initiation | 3 4 | Remove the additional tab which is under the clinic. Only include information relevant to “find doctor” | ||
| 9 | Recognition diagnosis, and recovery from errors | First (2020) | None identified | |||
| Second (2021) | None identified | |||||
| 10 | Help and documentation | First (2020) | The location of where the support and help are displayed in the app (part of the doctor list) may confuse the user. † The icon (i) representing help may be confused with general information about the app. | Orientation Orientation | 1 2 | It should be under a separate help icon. Change the icon (i) to “help” |
| Second (2021) | Difficult to retrieve the help page when a consultation with the physician is ongoing. | During consultation | 4 | Add a clear separate page with a help icon, which can be accessible. | ||
| Total Issues identified from the two evaluations: 14 | ||||||
| # | Heuristic Item | Evaluation Period | Usability Issue Description | Location | Rating | Redesign Recommendation |
|---|---|---|---|---|---|---|
| 1 | Visibility of system status | First (2020) | The app does not provide enough feedback after pressing the start consultation button. | Consultation initiation | 1 | Provide constructive feedback describing what the system is doing. |
| Second (2021) | Loading time was long. Does not indicate what the app is doing from one page to another, just shows the hospital logo. | Consultation initiation Orientation | 1 2 | Add a message indicating “loading”. Provide constructive feedback describing what the system is doing. | ||
| 2 | Match between system and the real world | First (2020) | When registering as a new patient, the app mandates the name in English. | Registration | 2 | Allow the user to choose the name in Arabic or English. |
| Second (2021) | None identified | |||||
| 3 | User control and freedom | First (2020) | In the payment screen, when user wants to change method of payment, the back icon takes the user to the home screen to start over and not back to the payment method options. † The session starts a video directly without the patient’s consent. | Consultation initiation During consultation | 2 4 | Allow the user to go back to the previous payment method screen instead of the home screen. Notify the patient that the session will start in video or start with a voice call and then with video after patient approval. |
| Second (2021) | The app allows the users to search the schedules of physicians before logging in. After the user has chosen a time, the app displays a message to the user to logs in. When the user login, the app returns the user to the home screen to search again. | Consultation initiation | 2 | Ask the user to log in before searching the schedules of physicians or prevent the app from going back to the first step (home screen) after the user logs in. | ||
| 4 | Consistency and adherence to standards | First (2020) | † How to access the telemedicine service from the home page is unclear to the user, i.e., what is the difference between the live care icon and the request appointment icon. | Consultation initiation | 2 | Make the live care icon more visible to the user by creating an option to choose from a list of consultation types, e.g., telemedicine-live, or physical visit by appointment |
| Second (2021) | After selecting” live care’’, there are two tabs: “consultation” and “name of the doctor”, which confuse the user. | Consultation initiation | 3 | Add a description under each tab | ||
| 5 | Error prevention | First (2020) | When registering as a new patient, the app does not indicate the name in English as a requirement. † No confirmation message for the user to end the session. | Registration End of consultation | 2 2 | Inform the user or provide an early error message when Arabic letters are written. Show a confirmation message before ending the session. |
| Second (2021) | The app did not provide an error prevention message during log in stage. In general, the app did not provide any error prevention messages. | Log in Registration | 4 4 | Add notification messages throughout the app, indicating and error will occur if the user proceeds or clicks a certain tab or icon. | ||
| 6 | Recognition rather than recall | First (2020) | † No instructions on how to use the app. | During consultation | 4 | Provide the user with clear instruction before the start of the live care session. |
| Second (2021) | None identified | |||||
| 7 | Flexibility and efficiency of use | No accelerators or ability to tailor frequent actions based on inexperienced and experienced users were found. | ||||
| 8 | Esthetic and minimalist design | First (2020) | The home page dashboard has so many displayed icons, which may confuse the user. The live session screen has icons placed in the bottom panel that may not be needed during the live consultation session such as “book appointment” and “actions”. | Registration Consultation initiation | 2 1 | Design a more minimalist and esthetic home screen. Remove “book appointment” and “actions” icons from the live session screen. |
| Second (2021) | “My Medical File” tab has many icons, which may confuse the user, when accessing records. | Registration | 1 | Minimize the icons and information displayed, by allowing the patient to personalize the page. | ||
| 9 | Recognition diagnosis, and recovery from errors | First (2020) | The error presented to the user because of choosing an unavailable clinic does not show a recovery message that the clinic has ended. The user must close the application and start over. | Consultation initiation | 1 | Add real-time updates indicating the available clinics (currently online) vs. unavailable clinics (offline) and provide a message to the user indicating what to do in case he/she chooses an unavailable clinic. |
| Second (2021) | The error presented to the user was not clear and did not explain the error and the solution. | Consultation initiation | 2 | Add clear error messages associated with clear instructions on how to resolve the error | ||
| 10 | Help and documentation | First (2020) | Instructions on how to use the “live care” feature are not presented to the user with no technical support contact information in case the user needs assistance. | Orientation | 4 | Provide users with easy access to instructions on how to use the app and on the home screen as user instructions. Provide contacts for help and support or live chat for technical issues. |
| Second (2021) | Instructions on how to access the help giving instructions on how to use the “live care” feature are not clear to the user. Voice recognition help is not appropriately working. | Orientation during consultation | 2 4 | Add a clear separate page with a help icon, explaining how the app is used. Improve or remove the feature. | ||
| Total Issues identified from the two evaluations: 22 | ||||||
References
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 27 September 2021).
- Monaghesh, E.; Hajizadeh, A. The role of telehealth during COVID-19 outbreak: A systematic review based on current evidence. BMC Public Health 2020, 20, 1193. [Google Scholar] [CrossRef]
- John Leon Singh, H.; Couch, D.; Yap, K. Mobile Health Apps That Help With COVID-19 Management: Scoping Review. JMIR Nurs. 2020, 3, e20596. [Google Scholar] [CrossRef]
- Zhai, Y.; Wang, Y.; Zhang, M.; Gittell, J.H.; Jiang, S.; Chen, B.; Cui, F.; He, X.; Zhao, J.; Wang, X. From isolation to coordination: How can telemedicine help combat the COVID-19 outbreak? MedRxiv 2020. [Google Scholar] [CrossRef]
- Rabuñal, R.; Suarez-Gil, R.; Golpe, R.; Martínez-García, M.; Gómez-Méndez, R.; Romay-Lema, E.; Pérez-López, A.; Rodríguez-Álvarez, A.; Bal-Alvaredo, M. Usefulness of a Telemedicine Tool TELEA in the Management of the COVID-19 Pandemic. Telemed e-Health. 2020, 26, 1332–1335. [Google Scholar] [CrossRef]
- Hassounah, M.; Raheel, H.; Alhefzi, M. Digital response during the COVID-19 pandemic in Saudi Arabia. J. Med. Internet Res. 2020, 22, e19338. [Google Scholar] [CrossRef]
- Ministry of Health. Sehha. Available online: https://www.moh.gov.sa/en/Support/Pages/MobileApp.aspx (accessed on 27 September 2021).
- Narasimha, S.; Madathil, K.C.; Agnisarman, S.; Rogers, H.; Welch, B.; Ashok, A.; Nair, A.; McElligott, J. Designing Telemedicine Systems for Geriatric Patients: A Review of the Usability Studies. Telemed. e-Health 2017, 23, 459–472. [Google Scholar] [CrossRef] [PubMed]
- Abelson, J.; Li, K.; Wilson, G.; Shields, K.; Schneider, C.; Boesveld, S. Supporting quality public and patient engagement in health system organizations: Development and usability testing of the Public and Patient Engagement Evaluation Tool. Health Expect. 2016, 19, 817–827. [Google Scholar] [CrossRef] [PubMed]
- Bestsennyy, O.; Gilbert, G.; Harris, A. Rost. Telehealth: A Quarter-Trillion-Dollar Post-COVID-19 Reality? Available online: https://www.mckinsey.com/industries/healthcare-systems-and-services/our-insights/telehealth-a-quarter-trillion-dollar-post-covid-19-reality (accessed on 17 November 2021).
- International Organization for Standardization. Usability of Consumer Products and Products for Public Use—Part 2: Summative Test Method. Iso.org. Available online: https://www.iso.org/obp/ui/#iso:std:iso:ts:20282:-2:ed-2:v1:en (accessed on 2 November 2021).
- Zapata, B.C.; Fernández-Alemán, J.L.; Idri, A.; Toval, A. Empirical Studies on Usability of mHealth Apps: A Systematic Literature Review. J. Med. Syst. 2015, 39, 1. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, J.; Molich, R. Heuristic evaluation of user interfaces. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems Empowering People—CHI’90, Seattle, WA, USA, 1–5 April 1990; ACM Press: New York, NY, USA, 1990; pp. 249–256. [Google Scholar] [CrossRef]
- Agnisarman, S.; Narasimha, S.; Madathil, K.C.; Welch, B.; Brinda, F.; Ashok, A.; McElligott, J.; Alhuwail, D.; Chaudry, B. Toward a More Usable Home-Based Video Telemedicine System: A Heuristic Evaluation of the Clinician User Interfaces of Home-Based Video Telemedicine Systems. JMIR Hum. Factors 2017, 4, e11. [Google Scholar] [CrossRef] [PubMed]
- Lilholt, P.H.; Jensen, M.H.; Hejlesen, O.K. Heuristic evaluation of a telehealth system from the Danish TeleCare North Trial. Int. J. Med. Inform. 2015, 84, 319–326. [Google Scholar] [CrossRef]
- Tang, Z.; Johnson, T.; Tindall, R.; Zhang, J. Applying Heuristic Evaluation to Improve the Usability of a Telemedicine System. Telemed. e-Health 2006, 12, 24–34. [Google Scholar] [CrossRef] [PubMed]
- Ligons, F.M.; Romagnoli, K.M.; Browell, S.; Hochheiser, H.S.; Handler, S.M. Assessing the usability of a telemedicine-based Medication Delivery Unit for older adults through inspection methods. AMIA Annu. Symp. Proc. 2011, 2011, 795–804. [Google Scholar]
- Dourado, M.A.; Canedo, E.D. Usability Heuristics for Mobile Applications—A Systematic Review. In Proceedings of the International Conference on Enterprise Information Systems (ICEIS), Madeira, Portugal, 21–24 March 2018. [Google Scholar]
- Virzi, R.A. Refining the Test Phase of Usability Evaluation: How Many Subjects Is Enough? Hum. Factors J. Hum. Factors Ergon. Soc. 1992, 34, 457–468. [Google Scholar] [CrossRef]
- Nielsen, J.; Landauer, T.K. A mathematical model of the finding of usability problems. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems—CHI’93, New York, NY, USA, 22–27 April 2006; ACM Press: New York, NY, USA, 1993; pp. 206–213. [Google Scholar] [CrossRef]
- National Transformation Program|Saudi Vision 2030. Available online: https://www.vision2030.gov.sa/v2030/vrps/ntp/ (accessed on 27 September 2021).
- Council of Cooperative Health Insurance. Available online: https://www.cchi.gov.sa/en/Pages/default.aspx (accessed on 27 September 2021).
- Ekeland, A.G.; Bowes, A.; Flottorp, S. Effectiveness of telemedicine: A systematic review of reviews. Int. J. Med. Inform. 2010, 79, 736–771. [Google Scholar] [CrossRef] [Green Version]
- Alshareef, M.; Alsaleh, S.; Albaharna, H.; Alghulikah, A.; Aloulah, M.; Alroqi, A.; Alromaih, S.; Alanazy, F.H.; Al-Dousary, S. Utilization of telemedicine in rhinologic practice during COVID-19 pandemic. Am. J. Otolaryngol. 2021, 42, 102929. [Google Scholar] [CrossRef]
- Al-Sofiani, M.E.; Alyusuf, E.Y.; Alharthi, S.; Alguwaihes, A.M.; Al-Khalifah, R.; Alfadda, A. Rapid Implementation of a Diabetes Telemedicine Clinic During the Coronavirus Disease 2019 Outbreak: Our Protocol, Experience, and Satisfaction Reports in Saudi Arabia. J. Diabetes Sci. Technol. 2021, 15, 329–338. [Google Scholar] [CrossRef] [PubMed]
- Tourkmani, A.M.; Alharbi, T.J.; Bin Rsheed, A.M.; Alrasheedy, A.; Almadani, W.; Aljuraisi, F.; Al Otaibi, A.F.; Al Harbi, M.; Al Abood, A.F.; Ibn Alshaikh, A. The impact of telemedicine on patients with uncontrolled type 2 diabetes mellitus during the COVID-19 pandemic in Saudi Arabia: Findings and implications. J. Telemed. Telecare 2021. [Google Scholar] [CrossRef]
- Mubaraki, A.A.; Alrabie, A.D.; Sibyani, A.K.; Aljuaid, R.S.; Bajaber, A.S.; Mubaraki, M.A. Advantages and disadvantages of telemedicine during the COVID-19 pandemic era among physicians in Taif, Saudi Arabia. Saudi Med. J. 2021, 42, 110–115. [Google Scholar] [CrossRef]
- Ministry of Health. MOH Reports First Case of Coronavirus Infection. Available online: https://www.moh.gov.sa/en/Ministry/MediaCenter/News/Pages/News-2020-03-02-002.aspx (accessed on 27 September 2021).
- National Digital Transformation Unit. National Digital Transformation Unit. Available online: https://www.my.gov.sa/wps/portal/snp/aboutksa/digitaltransformation (accessed on 7 November 2021).
- National Health Information Center. The Governing Rules of Telehealth (Telemedicine) in Saudi Arabia. Available online: https://nhic.gov.sa/en/Initiatives/Documents/TheGoverningRulesOfTelehealthEnglishEstablishingRules.pdf (accessed on 27 September 2021).
- Cura Healthcare. Cura App. Available online: https://cura.healthcare/en/ (accessed on 27 September 2021).
- Dr. Suliman Alhabib. HMG History. Available online: https://hmg.com/en/About-us/History/Pages/projects.aspx (accessed on 27 September 2021).
- Nielsen, J. Usability inspection methods. In Proceedings of the Conference Companion on Human Factors in Computing Systems, Boston, MA, USA, 24–28 April 1994; pp. 413–414. [Google Scholar]
- Google. Google Form. Available online: https://www.google.com/intl/en-GB/forms/about/ (accessed on 27 September 2021).
- Nielsen, J. Finding usability problems through heuristic evaluation. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems—CHI’92, Monterey, CA, USA, 3–7 May 1992; ACM Press: New York, NY, USA, 1992; pp. 373–380. [Google Scholar] [CrossRef]
- McDonagh, M.; Peterson, K.; Raina, P.; Chang, S.; Shekelle, P. Avoiding Bias in Selecting Studies. In Methods Guide for Effectiveness and Comparative Effectiveness Reviews [Internet]; Agency for Healthcare Research and Quality (US): Rockville, MD, USA, 2008. Available online: https://www.ncbi.nlm.nih.gov/books/NBK126701/ (accessed on 17 November 2021).
- Ministry of Health. Healthcare Licensing Services. Available online: https://www.moh.gov.sa/en/eServices/Licences/Pages/default.aspx (accessed on 27 September 2021).
- Communications, Commission IT. Communications and Information Technology Commission. Available online: https://www.citc.gov.sa/ar/Pages/default.aspx (accessed on 27 September 2021).
- Saudi Food and Drug Authority. SFDA. Available online: https://www.sfda.gov.sa/en (accessed on 27 September 2021).
- Saudi Data and AI Authority. SDAIA. Available online: https://sdaia.gov.sa (accessed on 27 September 2021).
- Saudi Central Board for Accreditation of Healthcare Institutions. CBAHI. Available online: https://portal.cbahi.gov.sa/english/home (accessed on 27 September 2021).
- Saudi Commission for Health Specialties. Telemedicine. Available online: https://www.scfhs.org.sa/en/eservices/Practitioners/Pages/TELE-MEDICINE.aspx (accessed on 27 September 2021).
- National Health Information Center (NHIC). Telemedicine Regulations in the Kingdom of Saudi Arabia. Available online: https://nhic.gov.sa/en/Initiatives/Documents/Saudi%20Arabia%20Telemedicine%20Policy.pdf (accessed on 27 September 2021).
- National Health Information Center. NHIC. Available online: https://nhic.gov.sa/en/Pages/default.aspx (accessed on 27 September 2021).
- Harbi, A. Health Care Expert’s readiness to implement National Unified Medical Records (NUMR) system in the United Arab Emirates: A Qualitative study. Informatica 2021, 45, 687–696. [Google Scholar] [CrossRef]
- Wu, R.; Ahn, G.; Hu, H. Secure sharing of electronic health records in clouds. In Proceedings of the 8th International Conference on Collaborative Computing: Networking, Applications and Worksharing (CollaborateCom), Pittsburgh, PA, USA, 14–17 October 2012; pp. 711–718. [Google Scholar]
- Zhang, J.; Johnson, T.R.; Patel, V.L.; Paige, D.L.; Kubose, T. Using usability heuristics to evaluate patient safety of medical devices. J. Biomed. Inform. 2003, 36, 23–30. [Google Scholar] [CrossRef] [Green Version]
- Triana, A.J.; Gusdorf, R.E.; Shah, K.P.; Horst, S.N. Technology Literacy as a Barrier to Telehealth During COVID-19. Telemed. e-Health 2020, 26, 1118–1119. [Google Scholar] [CrossRef] [PubMed]
- Wharton, C.; Rieman, J.; Lewis, C.; Polson, P. The cognitive walkthrough method: A practitioner’s guide. In Usability Inspection Methods; Nielsen Norman Group: Fremont, CA, USA, 1994; Available online: https://www.colorado.edu/ics/sites/default/files/attached-files/93-07.pdf (accessed on 17 November 2021).
- Alonso-Ríos, D.; Mosqueira-Rey, E.; Moret-Bonillo, V. A Systematic and Generalizable Approach to the Heuristic Evaluation of User Interfaces. Int. J. Hum.-Comput. Interact. 2017, 34, 1–14. [Google Scholar] [CrossRef]

| Feature | “Seha” | “Cura” | “Dr. Sulaiman Al Habib” | |||
|---|---|---|---|---|---|---|
| 2020 | 2021 | 2020 | 2021 | 2020 | 2021 | |
| Ability to access educational information on COVID-19 | √ | √ | √ | × | × | × |
| Includes COVID-19 patient self-assessment tool | √ | × | × | × | × | × |
| Limit to number of patient consultations | √ | √ | √ | × + | × + | × + |
| Patient able to choose among physician specialties | × | × | √ | √ | √ | √ |
| Patient able to see physician details | √ | √ | √ | √ | √ | √ |
| Supports video call | √ | √ | √ | √ | √ | √ |
| Supports text messaging | √ | √ | √ | √ | × | √ |
| Supports voice messaging | √ | √ | √ | √ | × | × |
| Ability to attached and send files | √ | √ | √ | √ | × | × |
| Patient able to schedule a telemedicine consultation | √ | √ | √ | √ | × | √ |
| Patient able to receive on demand consultation | √ | √ | √ | √ | √ | √ |
| Physician able to order a prescription | √ | √ | √ | √ | √ | √ |
| Linked to patient medical record | × | × | × | × | √ | √ |
| Patient able to view past consultation | √ | √ | √ | √ | √ | √ |
| End with satisfaction survey | √ | √ | √ | √ | √ | √ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aldekhyyel, R.N.; Almulhem, J.A.; Binkheder, S. Usability of Telemedicine Mobile Applications during COVID-19 in Saudi Arabia: A Heuristic Evaluation of Patient User Interfaces. Healthcare 2021, 9, 1574. https://doi.org/10.3390/healthcare9111574
Aldekhyyel RN, Almulhem JA, Binkheder S. Usability of Telemedicine Mobile Applications during COVID-19 in Saudi Arabia: A Heuristic Evaluation of Patient User Interfaces. Healthcare. 2021; 9(11):1574. https://doi.org/10.3390/healthcare9111574
Chicago/Turabian StyleAldekhyyel, Raniah N., Jwaher A. Almulhem, and Samar Binkheder. 2021. "Usability of Telemedicine Mobile Applications during COVID-19 in Saudi Arabia: A Heuristic Evaluation of Patient User Interfaces" Healthcare 9, no. 11: 1574. https://doi.org/10.3390/healthcare9111574
APA StyleAldekhyyel, R. N., Almulhem, J. A., & Binkheder, S. (2021). Usability of Telemedicine Mobile Applications during COVID-19 in Saudi Arabia: A Heuristic Evaluation of Patient User Interfaces. Healthcare, 9(11), 1574. https://doi.org/10.3390/healthcare9111574