
Effectiveness of Telephone Monitoring in Primary Care to Detect Pneumonia and Associated Risk Factors in Patients with SARS-CoV-2

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. SARS-CoV-2 Diagnosis and Follow-Up
2.3. Variables Collected
2.4. Statistical Analysis
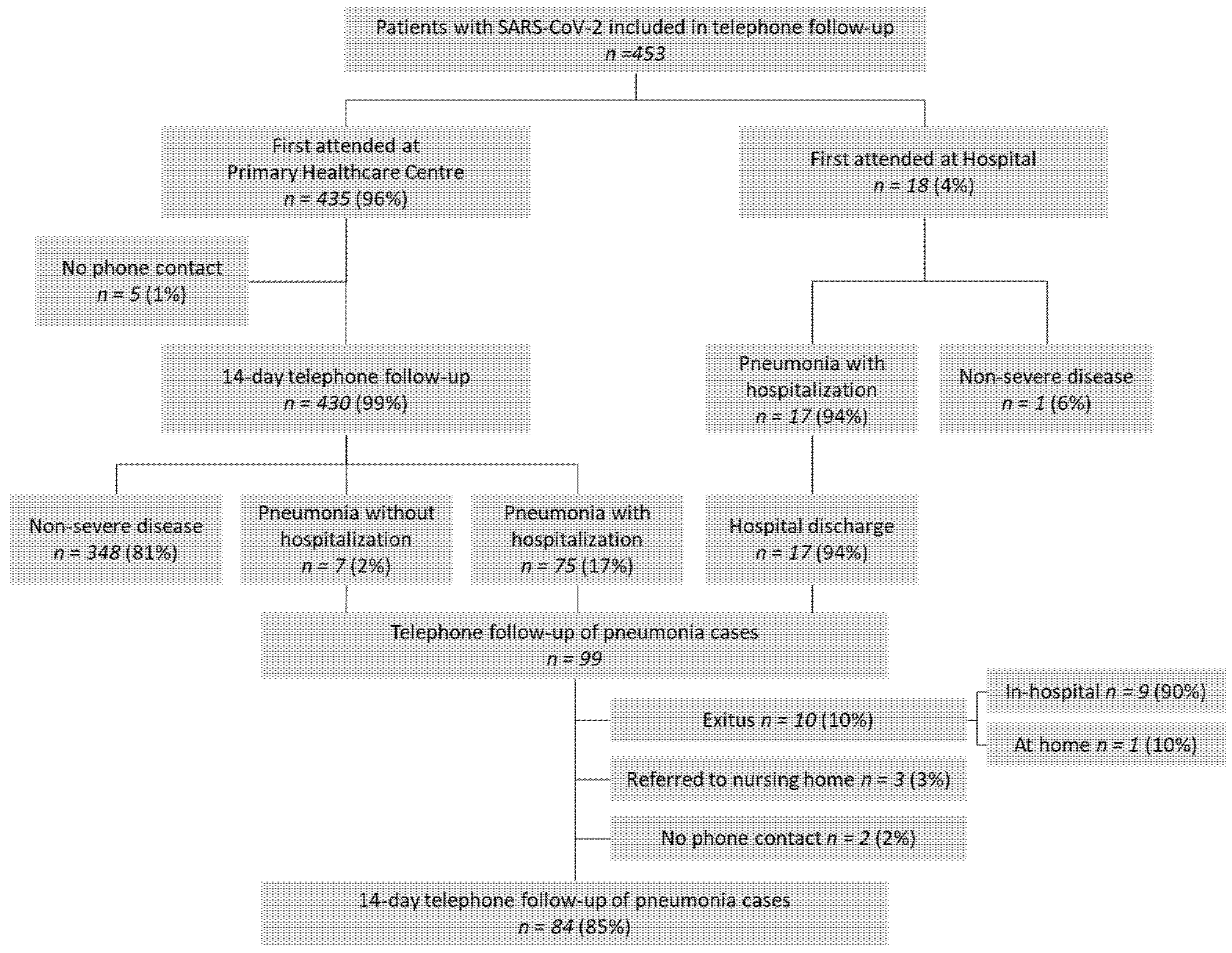
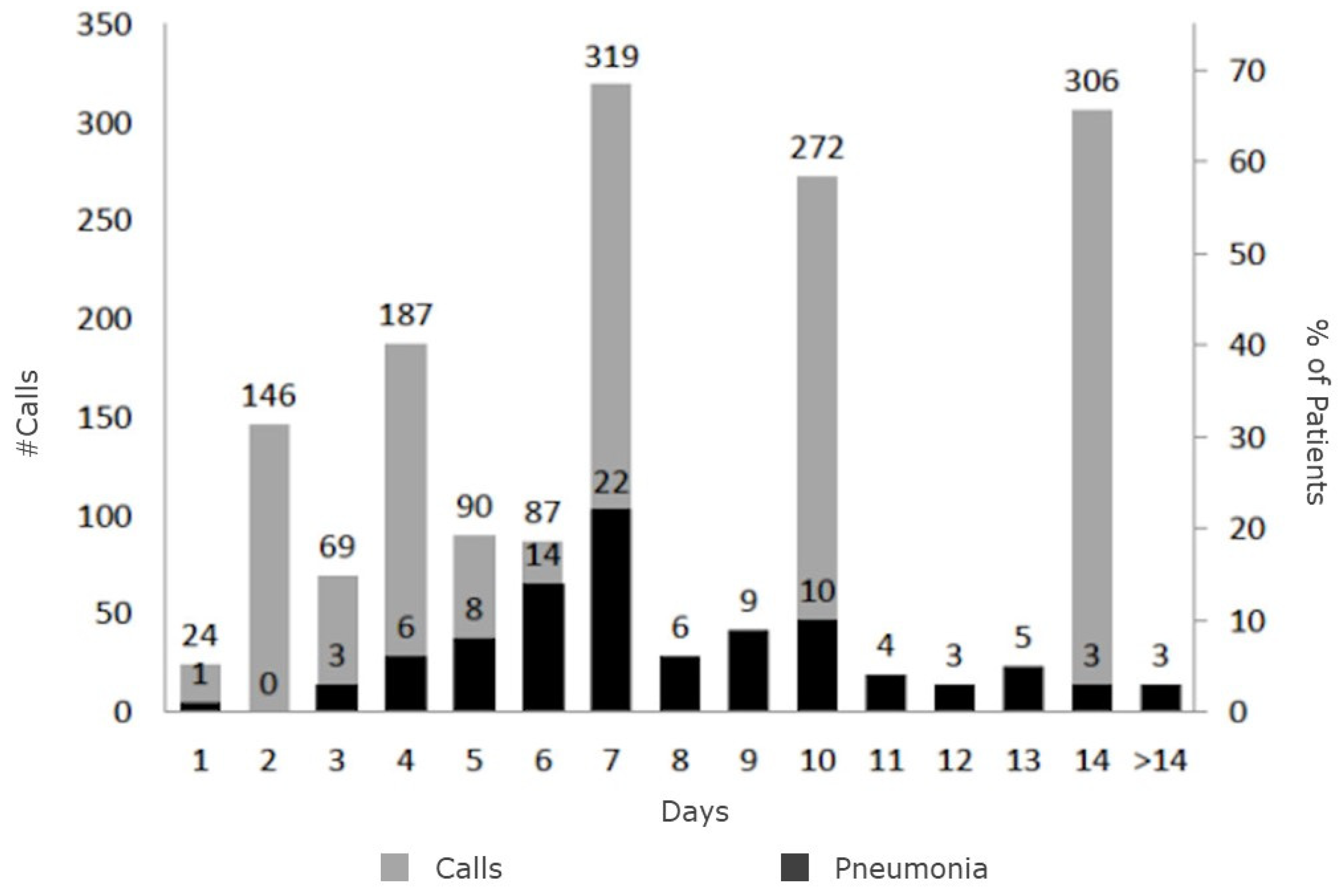
3. Results
4. Discussion
4.1. The Natural History of SARS-CoV-2
4.2. The Pandemic Accelerates the Digitalization of Healthcare
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Peckham, R. COVID-19 and the anti-lessons of history. Lancet 2020, 395, 850–852. [Google Scholar] [CrossRef] [Green Version]
- Johns Hopkins Coronavirus Resource Center. Available online: https://coronavirus.jhu.edu/map.html (accessed on 10 February 2021).
- Baena-Díez, J.M.; Barroso, M.; Cordeiro-Coelho, S.I.; Díaz, J.L.; Grau, M. Impact of COVID-19 outbreak by income: Hitting hardest the most deprived. J. Public Health 2020, 42, 698–703. [Google Scholar] [CrossRef]
- Krist, A.H.; DeVoe, J.E.; Cheng, A.; Ehrlich, T.; Jones, S.M. Redesigning Primary Care to Address the COVID-19 Pandemic in the Midst of the Pandemic. Ann. Fam. Med. 2020, 18, 349–354. [Google Scholar] [CrossRef]
- Struyf, T.; Deeks, J.J.; Dinnes, J.; Takwoingi, Y.; Davenport, C.; Leeflang, M.M.; Spijker, R.; Hooft, L.; Emperador, D.; Dittrich, S.; et al. Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19 disease. Cochrane Database Syst. Rev. 2020, 7, CD013665. [Google Scholar] [PubMed]
- Shigekawa, E.; Fix, M.; Corbett, G.; Roby, D.H.; Coffman, J. The Current State Of Telehealth Evidence: A Rapid Review. Health Aff. 2018, 37, 1975–1982. [Google Scholar] [CrossRef] [PubMed]
- Downes, M.J.; Mervin, M.C.; Byrnes, J.M.; Scuffham, P.A. Telephone consultations for general practice: A systematic review. Syst. Rev. 2017, 6, 128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, M.; Wang, M.; Liu, J.; Holbrook, A. Do telehealth interventions improve oral anticoagulation management? A systematic review and meta-analysis. J. Thromb. Thrombolysis 2018, 45, 325–336. [Google Scholar] [CrossRef] [PubMed]
- Marx, W.; Kelly, J.T.; Crichton, M.; Craven, D.; Collins, J.; Mackay, H.; Isenring, E.; Marshall, S. Is telehealth effective in managing malnutrition in community-dwelling older adults? A systematic review and meta-analysis. Maturitas 2018, 111, 31–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, Y.; Liu, R.; Zhou, Q.; Wang, X.; Huang, L.; Shi, Q.; Wang, Z.; Lu, S.; Li, W.; Ma, Y.; et al. Application of telemedicine during the coronavirus disease epidemics: A rapid review and meta-analysis. Ann. Transl. Med. 2020, 8, 626. [Google Scholar] [CrossRef]
- World Health Organization. WHO Announces COVID-19 Outbreak a Pandemic. Available online: https://www.euro.who.int/en/health-topics/health-emergencies/coronavirus-covid-19/news/news/2020/3/who-announces-covid-19-outbreak-a-pandemic (accessed on 26 October 2021).
- Aillament Domiciliari per a Posibles Casos de Coronavirus SARS-CoV-2. Generalitat de Catalunya. Available online: https://scientiasalut.gencat.cat/bitstream/handle/11351/4715/aillament_domiciliari_possibles_casos_coronavirus_sars_cov2_2020_ca.pdf (accessed on 11 February 2021).
- Xie, Y.; Wang, Z.; Liao, H.; Marley, G.; Wu, D.; Tang, W. Epidemiologic, clinical, and laboratory findings of the COVID-19 in the current pandemic: Systematic review and meta-analysis. BMC Infect. Dis. 2020, 20, 640. [Google Scholar] [CrossRef]
- Zheng, Z.; Peng, F.; Xu, B.; Zhao, J.; Liu, H.; Peng, J.; Li, Q.; Jiang, C.; Zhou, Y.; Liu, S.; et al. Risk factors of critical & mortal COVID-19 cases: A systematic literature review and meta-analysis. J. Infect. 2020, 81, e16–e25. [Google Scholar] [PubMed]
- Petrilli, C.M.; Jones, S.A.; Yang, J.; Rajagopalan, H.; O’Donnell, L.; Chernyak, Y.; Tobin, K.A.; Cerfolio, R.J.; Francois, F.; Horwitz, L.I. Factors associated with hospital admission and critical illness among 5279 people with coronavirus disease 2019 in New York City: Prospective cohort study. BMJ 2020, 369, m1966. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Huang, D.Q.; Zou, B.; Yang, H.; Hui, W.Z.; Rui, F.; Yee, N.; Liu, C.; Nerurkar, S.N.; Kai, J.; et al. Epidemiology of COVID-19: A systematic review and meta-analysis of clinical characteristics, risk factors, and outcomes. J. Med. Virol. 2021, 93, 1449–1458. [Google Scholar] [CrossRef] [PubMed]
- Temesgen, Z.M.; DeSimone, D.C.; Mahmood, M.; Libertin, C.R.; Varatharaj Palraj, B.R.; Berbari, E.F. Health Care after the COVID-19 Pandemic and the Influence of Telemedicine. Mayo Clin. Proc. 2020, 95, S66–S68. [Google Scholar] [CrossRef] [PubMed]
- Joy, M.; McGagh, D.; Jones, N.; Liyanage, H.; Sherlock, J.; Parimalanathan, V.; Akinyemi, O.; van Vlymen, J.; Howsam, G.; Marshall, M.; et al. Reorganisation of primary care for older adults during COVID-19: A cross-sectional database study in the UK. Br. J. Gen. Pract. 2020, 70, e540–e547. [Google Scholar] [CrossRef]
- Pérez Sust, P.; Solans, O.; Fajardo, J.C.; Medina Peralta, M.; Rodenas, P.; Gabaldà, J.; Garcia Eroles, L.; Comella, A.; Velasco Muñoz, C.; Sallent Ribes, J.; et al. Turning the Crisis into an Opportunity: Digital Health Strategies Deployed during the COVID-19 Outbreak. JMIR Public Health Surveill. 2020, 6, e19106. [Google Scholar] [CrossRef] [PubMed]
- Vidal-Alaball, J.; Acosta-Roja, R.; Pastor Hernández, N.; Sanchez Luque, U.; Morrison, D.; Narejos Pérez, S.; Perez-Llano, J.; Salvador Vèrges, A.; López Seguí, F. Telemedicine in the face of the COVID-19 pandemic. Aten. Primaria 2020, 52, 418–422. [Google Scholar] [CrossRef] [PubMed]
- Khairat, S.; Meng, C.; Xu, Y.; Edson, B.; Gianforcaro, R. Interpreting COVID-19 and Virtual Care Trends: Cohort Study. JMIR Public Health Surveill. 2020, 6, e18811. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chu, D.K.; Akl, E.A.; Duda, S.; Solo, K.; Yaacoub, S.; Schünemann, H.J.; COVID-19 Systematic Urgent Review Group Effort (SURGE) Study Authors. Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and COVID-19: A systematic review and meta-analysis. Lancet 2020, 395, 1973–1987. [Google Scholar] [CrossRef]
- Gilbert, A.W.; Billany, J.; Adam, R.; Martin, L.; Tobin, R.; Bagdai, S.; Galvin, N.; Farr, I.; Allain, A.; Davies, L.; et al. Rapid implementation of virtual clinics due to COVID-19: Report and early evaluation of a quality improvement initiative. BMJ Open Qual. 2020, 9, e000985. [Google Scholar] [CrossRef]
- Omboni, S. Telemedicine during the COVID-19 in Italy: A Missed Opportunity? Telemed. J. E-Health 2020, 26, 973–975. [Google Scholar] [CrossRef] [Green Version]
- Muflih, S.M.; Al-Azzam, S.; Abuhammad, S.; Jaradat, S.K.; Karasneh, R.; Shawaqfeh, M.S. Pharmacists’ experience, competence and perception of telepharmacy technology in response to COVID-19. Int. J. Clin. Pract. 2021, 75, e14209. [Google Scholar] [CrossRef] [PubMed]
- Wosik, J.; Fudim, M.; Cameron, B.; Gellad, Z.F.; Cho, A.; Phinney, D.; Curtis, S.; Roman, M.; Poon, E.G.; Ferranti, J.; et al. Telehealth transformation: COVID-19 and the rise of virtual care. J. Am. Med. Inform. Assoc. 2020, 27, 957–962. [Google Scholar] [CrossRef]
- Jiménez-Rodríguez, D.; Santillán García, A.; Montoro Robles, J.; Rodríguez Salvador, M.; Muñoz Ronda, F.J.; Arrogante, O. Increase in Video Consultations During the COVID-19 Pandemic: Healthcare Professionals’ Perceptions about Their Implementation and Adequate Management. Int. J. Environ. Res. Public Health 2020, 17, 5112. [Google Scholar] [CrossRef]
- Faezipour, M.; Abuzneid, A. Smartphone-Based Self-Testing of COVID-19 Using Breathing Sounds. Telemed. J. E-Health 2020, 26, 1202–1205. [Google Scholar] [CrossRef]
- Wong, C.K.; Ho, D.; Tam, A.R.; Zhou, M.; Lau, Y.M.; Tang, M.; Tong, R.; Rajput, K.S.; Chen, G.; Chan, S.C.; et al. Artificial intelligence mobile health platform for early detection of COVID-19 in quarantine subjects using a wearable biosensor: Protocol for a randomised controlled trial. BMJ Open 2020, 10, e038555. [Google Scholar] [CrossRef]
- Hong, Y.R.; Lawrence, J.; Williams, D., Jr.; Mainous, A., III. Population-Level Interest and Telehealth Capacity of US Hospitals in Response to COVID-19: Cross-Sectional Analysis of Google Search and National Hospital Survey Data. JMIR Public Health Surveill. 2020, 6, e18961. [Google Scholar] [CrossRef]
- Pianese, T.; Belfiore, P. Exploring the Social Networks’ Use in the Health-Care Industry: A Multi-Level Analysis. Int. J. Environ. Res. Public Health 2021, 18, 7295. [Google Scholar] [CrossRef]
- Thackeray, R.; Neiger, B.L.; Smith, A.K.; Van Wagenen, S.B. Adoption and use of social media among public health departments. BMC Public Health 2012, 12, 242. [Google Scholar] [CrossRef] [Green Version]
- Lam, P.W.; Sehgal, P.; Andany, N.; Mubareka, S.; Simor, A.E.; Ozaldin, O.; Leis, J.A.; Daneman, N.; Chan, A.K. A virtual care program for outpatients diagnosed with COVID-19: A feasibility study. CMAJ Open 2020, 8, E407–E413. [Google Scholar] [CrossRef]
- Xu, H.; Huang, S.; Qiu, C.; Liu, S.; Deng, J.; Jiao, B.; Tan, X.; Ai, L.; Xiao, Y.; Belliato, M.; et al. Monitoring and Management of Home-Quarantined Patients with COVID-19 Using a WeChat-Based Telemedicine System: Retrospective Cohort Study. J. Med. Internet Res. 2020, 22, e19514. [Google Scholar] [CrossRef] [PubMed]
- Cheng, A.; Caruso, D.; McDougall, C. Outpatient Management of COVID-19: Rapid Evidence Review. Am. Fam. Phys. 2020, 102, 478–486. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All (n = 453) | SARS-CoV-2 Non-Severe Disease (n = 354) | SARS-CoV-2 Pneumonia (n = 99) | p-Value | |
|---|---|---|---|---|
| Age, mean (SD) | 50 (16) | 47 (15) | 60 (15) | <0.001 |
| Sex (male), n (%) | 189 (41.7) | 143 (40.4) | 46 (46.5) | 0.333 |
| SARS-CoV-2 risk factors | ||||
| Age ≥65 years | 74 (16.3) | 37 (10.5) | 37 (37.4) | <0.001 |
| Cardiopathy | 30 (6.6) | 17 (4.8) | 13 (13.1) | 0.007 |
| Type 2 diabetes mellitus | 37 (8.2) | 22 (6.2) | 15 (15.2) | 0.008 |
| Hypertension | 97 (21.4) | 58 (16.4) | 39 (39.4) | <0.001 |
| Immunosuppression | 18 (4.0) | 9 (2.5) | 9 (9.1) | 0.007 |
| Chronic obstructive pulmonary disease | 13 (2.9) | 6 (1.7) | 7 (7.1) | 0.010 |
| Unadjusted HR (95% CI) | p-Value | Adjusted HR * (95% CI) | p-Value | |
|---|---|---|---|---|
| Age ≥ 65 years | 3.31 (2.16; 5.08) | <0.001 | -- | -- |
| Cardiopathy | 1.90 (0.99; 3.65) | 0.055 | 0.93 (0.48; 1.82) | 0.841 |
| Type 2 diabetes mellitus | 1.79 (0.98; 3.28) | 0.058 | 0.94 (0.50; 1.77) | 0.858 |
| Hypertension | 2.40 (1.58; 3.66) | <0.001 | 1.21 (0.74; 1.98) | 0.446 |
| Chronic obstructive pulmonary | 3.20 (1.61; 6.37) | 0.001 | 1.23 (0.57; 2.62) | 0.597 |
| Immunosuppression | 3.03 (1.40; 6.54) | 0.005 | 2.35 (1.08; 5.09) | 0.030 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baena-Díez, J.M.; Gonzalez-Casafont, I.; Cordeiro-Coelho, S.; Fernández-González, S.; Rodríguez-Jorge, M.; Pérez-Torres, C.U.F.; Larrañaga-Cabrera, A.; García-Lareo, M.; de la Arada-Acebes, A.; Martín-Jiménez, E.; et al. Effectiveness of Telephone Monitoring in Primary Care to Detect Pneumonia and Associated Risk Factors in Patients with SARS-CoV-2. Healthcare 2021, 9, 1548. https://doi.org/10.3390/healthcare9111548
Baena-Díez JM, Gonzalez-Casafont I, Cordeiro-Coelho S, Fernández-González S, Rodríguez-Jorge M, Pérez-Torres CUF, Larrañaga-Cabrera A, García-Lareo M, de la Arada-Acebes A, Martín-Jiménez E, et al. Effectiveness of Telephone Monitoring in Primary Care to Detect Pneumonia and Associated Risk Factors in Patients with SARS-CoV-2. Healthcare. 2021; 9(11):1548. https://doi.org/10.3390/healthcare9111548
Chicago/Turabian StyleBaena-Díez, Jose Miguel, Isabel Gonzalez-Casafont, Sara Cordeiro-Coelho, Soledad Fernández-González, Migdalia Rodríguez-Jorge, Clara Uxía Fernández Pérez-Torres, Andrea Larrañaga-Cabrera, Manel García-Lareo, Ana de la Arada-Acebes, Esther Martín-Jiménez, and et al. 2021. "Effectiveness of Telephone Monitoring in Primary Care to Detect Pneumonia and Associated Risk Factors in Patients with SARS-CoV-2" Healthcare 9, no. 11: 1548. https://doi.org/10.3390/healthcare9111548
APA StyleBaena-Díez, J. M., Gonzalez-Casafont, I., Cordeiro-Coelho, S., Fernández-González, S., Rodríguez-Jorge, M., Pérez-Torres, C. U. F., Larrañaga-Cabrera, A., García-Lareo, M., de la Arada-Acebes, A., Martín-Jiménez, E., Pérez-Orcero, A., Hernández-Ibáñez, R., Gonzalo-Voltas, A., Bermúdez-Chillida, N., Simón-Muela, C., del Carlo, G., Bayona-Faro, C., Rey-Reñones, C., Aguilar-Palacio, I., & Grau, M. (2021). Effectiveness of Telephone Monitoring in Primary Care to Detect Pneumonia and Associated Risk Factors in Patients with SARS-CoV-2. Healthcare, 9(11), 1548. https://doi.org/10.3390/healthcare9111548