
Safety Performance in Acute Medical Care: A Qualitative, Explorative Study on the Perspectives of Healthcare Professionals

 , , , , and
, , , , and 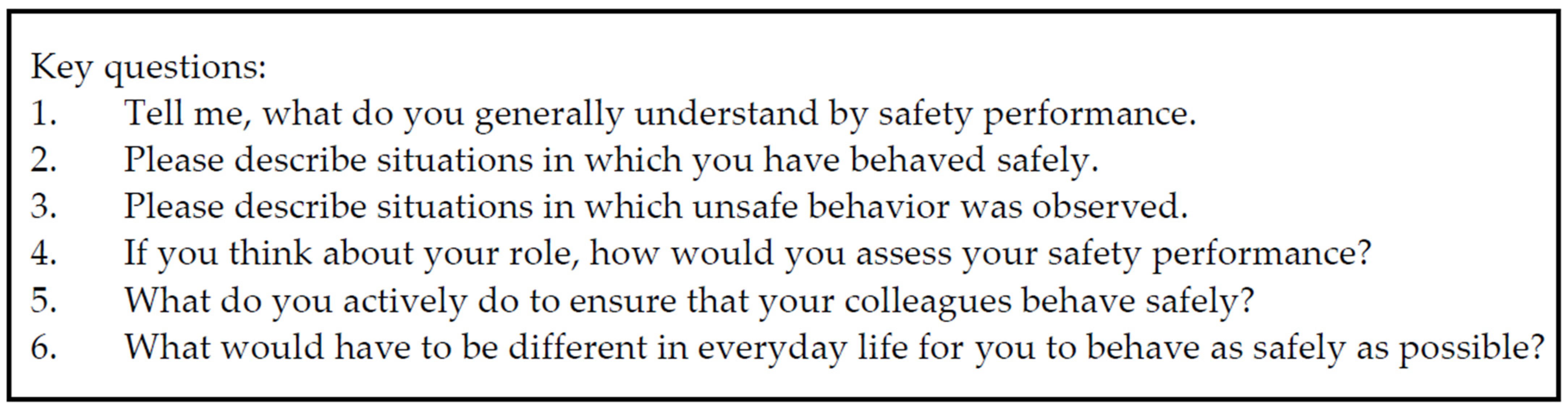{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Sample and Study Setting
2.3. Data Collection
2.4. Data Analysis
2.5. Trustworthiness of the Study
3. Results
3.1. Sample Characteristics
3.2. Aspects of Safety Performance
Well, no idea, that there are no power cables on the floor that you can trip over.(IP01)
Well, for example, that you, when you’ve moved a patient from one room to another, that you then lower the bed again, that you, I don’t know, also explain to the patient how the nurse call button works, adjust the lights, that, if it’s dark, you might also turn on the light and explain to the patient how to turn on the light.(IP05)
It’s also about sharps disposal, correct waste disposal, avoiding situations that are potentially dangerous for patients, right?(IP08)
Well, let’s start with patient safety; so, there, I would say that, for example, when the floor is mopped, that some sign is placed stating that like/that the floor is wet.(IP14)
We had a construction site here a little while ago. So we had to be careful, too; there was scaffolding here on the patio, so we locked the patio door to make sure that patients do not go there and possibly climb up.(IP19)
3.3. Aspects of Safety Performance—Organizational/Managerial
I believe at our facility, it’s that our director and deputy director are both people who pay very close attention to that. And if any mistakes are made, they communicate that. And they have very high quality standards for our team. And that as a result, I believe, a lot is actually achieved/that, well, people do act properly because we know that this is kind of demanded and required from us.(IP10)
I believe, that is really because the people all receive really good initial training, a good briefing, and continued education. So, it’s not like someone just says: “Come on, let me show you the emergency kit really quickly”, but there is an actual continued education event where you sit down for two hours and where each drug is discussed, too, what its indication is and when to use it.(IP07)
3.4. Aspects of Safety Performance—Team
That is, you then also have to take a second step and not only inform people but to somehow also enable them to act accordingly. And typically, this is best done by, well, by showing them how to do it.(IP11)
That is, if we had a reanimation here last time, then the medical team was brought in, then I asked that we reflect again on what we did, how we did it, how everyone experienced it, how everyone felt in the process, and we try to reflect on that again on the larger scale and simply do better in the future to simply ensure patient safety that way as well.(IP06)
And we actually train our physicians a little bit in this way because: “Well, do this, do that”, no physician order. Now, we don’t do anything without a physician order. And sometimes, many physicians actually then try to verbally delegate things somehow, but we just don’t do it. And then they got used to it.(IP03)
3.5. Aspects of Safety Performance—Individual Worker
And most of it, well, it’s very important that personal protection, that it is always paramount. Because, if I’m down sick, I can no longer help others. That’s why I always start with myself.(IP17)
And especially the last case, it just showed me that even I, with twenty years of job experience, still need to always reflect. Work on myself. And that gave me a little more security, to still feel that. If I had gone in there indifferently and came out indifferently, I would have been rather worried, or actually, probably not.(IP17)
And that you, as I said, participate in continued education, if you learn something from the continued education, that you just pass that on in the team, too.(IP15)
3.6. Aspects of Safety Performance—Work Environment
An example is, well, if a patient is infectious and isolated, you have to put on specific protective clothing if you perform activities near the patient so that you then leave the microbes in the room when you take off the protective clothing.(IP11)
Another topic is the administration of medications; for example, infusions, when I administer them. Or injections that I administer. There as well, it’s important that I make sure, for instance, to disinfect the puncture site, or disinfect the connectors to which the infusion is hooked up to ensure that I do not expose the patient to microbes through the injections or infusions.(IP11)
3.7. Aspects of Safety Performance—Patient
For instance, storage, repositioning, patient admission, to ensure that data are appropriately collected, documented, and that this is a continuous cycle. The patient, for example, which side is operated on, is it the right patient, is the name correct, the information, etc.? Is the patient placed on the correct table? Have we brought up the correct X-rays? It runs through all of that. Well, those are the patient-relevant data that, I think, do play a major role. Because mix-ups have been described over and over. And of course, they should be avoided if at all possible.(IP22)
So, of course, as I already mentioned, with regard to hazardous objects, escape routes, that patients have been informed, too, for instance, what to do in case of fire. Because something like that can happen at any time even without external influences.(IP13)
My staff knows exactly, if I’m not well, that I simply know I can always address that. And to give the patient this psychological, well, safety; I do think that is part of patient safety as well.(IP06)
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- de Vries, E.N.; Ramrattan, M.A.; Smorenburg, S.M.; Gouma, D.J.; Boermeester, M.A. The incidence and nature of in-hospital adverse events: A systematic review. Qual. Saf. Health Care 2008, 17, 216–223. [Google Scholar] [CrossRef]
- Baethge, A.; Müller, A.; Rigotti, T. Nursing performance under high workload: A diary study on the moderating role of selection, optimization and compensation strategies. J. Adv. Nurs. 2016, 72, 545–557. [Google Scholar] [CrossRef]
- Aiken, L.H.; Sermeus, W.; van den Heede, K.; Sloane, D.M.; Busse, R.; McKee, M.; Bruyneel, L.; Rafferty, A.M.; Griffiths, P.; Moreno-Casbas, M.T.; et al. Patient safety, satisfaction, and quality of hospital care: Cross sectional surveys of nurses and patients in 12 countries in Europe and the United States. BMJ 2012, 344, e1717. [Google Scholar] [CrossRef] [PubMed]
- Aiken, L.H.; Sloane, D.M.; Barnes, H.; Cimiotti, J.P.; Jarrín, O.F.; McHugh, M.D. Nurses’ And Patients’ Appraisals Show Patient Safety In Hospitals Remains A Concern. Health Aff. 2018, 37, 1744–1751. [Google Scholar] [CrossRef]
- Arnetz, J.E.; Neufcourt, L.; Sudan, S.; Arnetz, B.B.; Maiti, T.; Viens, F. Nurse-Reported Bullying and Documented Adverse Patient Events: An Exploratory Study in a US Hospital. J. Nurs. Care Qual. 2020, 35, 206–212. [Google Scholar] [CrossRef]
- Stone, P.W.; Mooney-Kane, C.; Larson, E.L.; Horan, T.; Glance, L.G.; Zwanziger, J.; Dick, A.W. Nurse Working Conditions and Patient Safety Outcomes. Med. Care 2007, 45, 571–578. [Google Scholar] [CrossRef]
- Aiken, L.H.; Clarke, S.P.; Sloane, D.M.; Lake, E.T.; Cheney, T. Effects of hospital care environment on patient mortality and nurse outcomes. J. Nurs. Adm. 2008, 38, 223–229. [Google Scholar] [CrossRef]
- Brunetto, Y.; Xerri, M.; Farr-Wharton, B.; Shacklock, K.; Farr-Wharton, R.; Trinchero, E. Nurse safety outcomes: Old problem, new solution—The differentiating roles of nurses’ psychological capital and managerial support. J. Adv. Nurs. 2016, 72, 2794–2805. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine (US) Committee on the Work Environment for Nurses and Patient Safety. Keeping Patients Safe: Transforming the Work Environment of Nurses; Page, A., Ed.; National Academies Press (US): Washington, DC, USA, 2004.
- Ernstmann, N.; Ommen, O.; Driller, E.; Kowalski, C.; Neumann, M.; Bartholomeyczik, S.; Pfaff, H. Social capital and risk management in nursing. J. Nurs. Care Qual. 2009, 24, 340–347. [Google Scholar] [CrossRef]
- Danielsson, M.; Nilsen, P.; Rutberg, H.; Fock, J.; Carlfjord, S. Patient safety subcultures among registered nurses and nurse assistants in Swedish hospital care: A qualitative study. BMC Nurs. 2014, 13, 39. [Google Scholar] [CrossRef] [PubMed]
- World Health Organzation. Human Factors in Patient Safety. Review of Topics and Tools: Report for Methods and Measures Working Group of WHO Patient Safety. 2009. Available online: https://www.who.int/patientsafety/research/methods_measures/human_factors/human_factors_review.pdf (accessed on 16 July 2020).
- Carayon, P.; Wetterneck, T.B.; Rivera-Rodriguez, A.J.; Hundt, A.S.; Hoonakker, P.; Holden, R.; Gurses, A.P. Human factors systems approach to healthcare quality and patient safety. Appl. Ergon. 2014, 45, 14–25. [Google Scholar] [CrossRef]
- Pronovost, P.J.; Weisfeldt, M.L. Science-Based Training in Patient Safety and Quality. Ann. Intern. Med. 2012, 157, 141–144. [Google Scholar] [CrossRef]
- Health and Safety Executive. HSG48 Reducing Error and Influencing Behaviour: Examines Human Factors and How They Can Affect Workplace Health and Safety; The Stationery Office Ltd.: Norwich, UK, 1999.
- Brasaitė, I.; Kaunonen, M.; Martinkėnas, A.; Mockienė, V.; Suominen, T. Health care professionals’ skills regarding patient safety. Medicina 2016, 52, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Griffin, M.A.; Neal, A. Perceptions of Safety at Work: A Framework for Linking Safety Climate to Safety Performance, Knowledge, and Motivation. J. Occup. Health Psychol. 2000, 5, 347–358. [Google Scholar] [CrossRef] [PubMed]
- Neal, A.; Griffin, M.A.; Hart, P.M. The impact of organizational climate on safety climate and individual behavior. Saf. Sci. 2000, 34, 99–109. [Google Scholar] [CrossRef]
- Dieckmann, P.; Patterson, M.; Lahlou, S.; Mesman, J.; Nyström, P.; Krage, R. Variation and adaptation: Learning from success in patient safety-oriented simulation training. Adv. Simul. 2017, 2, 21. [Google Scholar] [CrossRef] [PubMed]
- Hughes, L.J.; Mitchell, M.; Johnston, A.N.B. ‘Failure to fail’ in nursing—A catch phrase or a real issue? A systematic integrative literature review. Nurse Educ. Pract. 2016, 20, 54–63. [Google Scholar] [CrossRef]
- Kang, J.-H.; Kim, C.-W.; Lee, S.-Y. Nurse-Perceived Patient Adverse Events depend on Nursing Workload. Osong Public Health Res. Perspect. 2016, 7, 56–62. [Google Scholar] [CrossRef]
- Shin, S.; Park, J.-H.; Bae, S.-H. Nurse staffing and nurse outcomes: A systematic review and meta-analysis. Nurs. Outlook 2018, 66, 273–282. [Google Scholar] [CrossRef]
- Wynendaele, H.; Willems, R.; Trybou, J. Systematic review: Association between the patient-nurse ratio and nurse outcomes in acute care hospitals. J. Nurs. Manag. 2019, 27, 896–917. [Google Scholar] [CrossRef]
- Heier, L.; Gambashidze, N.; Hammerschmidt, J.; Riouchi, D.; Weigl, M.; Neal, A.; Icks, A.; Brossart, P.; Geiser, F.; Ernstmann, N. Safety Performance of Healthcare Professionals: Validation and Use of the Adapted Workplace Health and Safety Instrument. Int. J. Environ. Res. Public Health 2021, 18, 7816. [Google Scholar] [CrossRef] [PubMed]
- Hu, S.H.; Wang, T.; Ramalho, N.C.; Zhou, D.; Hu, X.; Zhao, H. Relationship between patient safety culture and safety performance in nursing: The role of safety behaviour. Int. J. Nurs. Pract. 2021, 27, e12937. [Google Scholar] [CrossRef]
- Campbell, A.; Layne, D.; Scott, E. Relational Quality of Registered Nurses and Nursing Assistants: Influence on Patient Safety Culture. Healthcare 2021, 9, 189. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Francisco, D.H.; Duarte-Clíments, G.; Del Rosario-Melián, J.M.; Gómez-Salgado, J.; Romero-Martín, M.; Sánchez-Gómez, M.B. Influence of Workload on Primary Care Nurses’ Health and Burnout, Patients’ Safety, and Quality of Care: Integrative Review. Healthcare 2020, 8, 12. [Google Scholar] [CrossRef]
- Christian, M.S.; Bradley, J.C.; Wallace, J.C.; Burke, M.J. Workplace safety: A meta-analysis of the roles of person and situation factors. J. Appl. Psychol. 2009, 94, 1103–1127. [Google Scholar] [CrossRef] [PubMed]
- Neal, A.; Griffin, M.A. Safety Climate and Safety Behaviour. Aust. J. Manag. 2002, 27, 67–75. [Google Scholar] [CrossRef]
- Heier, L.; Gambashidze, N.; Hammerschmidt, J.; Riouchi, D.; Geiser, F.; Ernstmann, N. Development and testing of the situational judgment test to measure safety performance of healthcare professionals: An explorative cross-sectional study. Nurs. Open 2021. [Google Scholar] [CrossRef]
- Tannen, A.; Feuchtinger, J.; Strohbücker, B.; Kocks, A. Survey zur Einbindung von Pflegefachpersonen mit Hochschulabschlüssen an deutschen Universitätskliniken—Stand 2015. Z. Evid. Fortbild. Qual. Gesundhwes. 2017, 120, 39–46. [Google Scholar] [CrossRef]
- Helfferich, C. Die Qualität Qualitativer Daten: Manual für die Durchführung Qualitativer Interviews; 4. Auflage; VS Verlag für Sozialwissenschaften: Wiesbaden, Germany, 2011. [Google Scholar]
- Mayring, P. Qualitative Inhaltsanalyse: Grundlagen und Techniken; Beltz: Weinheim, Germany, 2015; ISBN 3407257309. [Google Scholar]
- Korstjens, I.; Moser, A. Series: Practical guidance to qualitative research. Part 4: Trustworthiness and publishing. Eur. J. Gen. Pract. 2018, 24, 120–124. [Google Scholar] [CrossRef]
- Ferorelli, D.; Giandola, T.; Laterza, M.; Solarino, B.; Pezzolla, A.; Zotti, F.; Dell’Erba, A. Handover checklist: Testing a standardization process in an Italian hospital. Risk Manag. Healthc. Policy 2017, 10, 87–93. [Google Scholar] [CrossRef]
- Ferorelli, D.; Solarino, B.; Trotta, S.; Mandarelli, G.; Tattoli, L.; Stefanizzi, P.; Bianchi, F.P.; Tafuri, S.; Zotti, F.; Dell’Erba, A. Incident Reporting System in an Italian University Hospital: A New Tool for Improving Patient Safety. Int. J. Environ. Res. Public Health 2020, 17, 6267. [Google Scholar] [CrossRef] [PubMed]
- Hung, C.-C.; Hsu, S.-C.; Lee, L.-L.; Huang, C.-M. The Effects of Contextual and Structural Factors on Patient Safety in Nursing Units. J. Nurs. Res. 2013, 21, 225–233. [Google Scholar] [CrossRef]
- Ko, Y.K.; Jeong, S.H.; Yu, S. Job autonomy, perceptions of organizational policy, and the safety performance of nurses. Int. J. Nurs. Pract. 2018, 24, e12696. [Google Scholar] [CrossRef]
- Weston, M.J. Defining Control Over Nursing Practice an Autonomy. J. Nurs. Adm. 2008, 38, 404–408. [Google Scholar] [CrossRef]
- Ridelberg, M.; Roback, K.; Nilsen, P. Facilitators and barriers influencing patient safety in Swedish hopsitals: A qualitatice study of nurses’ perceptions. BMC Nurs. 2014, 13, 23. [Google Scholar] [CrossRef] [PubMed]
- Aktionsbündnis Patientensicherheit (APS); Bundespflegekammer; Deutsche Gesellschaft für Pflegewissenschaft (DGP); Deutscher Pflegerat (DPR). Patient Safety/Resident Safety in Nursing Responsibility: Patientensicherheit/Bewohnersicherheit in Pflegerischer Verantwortung. 2020. Available online: https://www.aps-ev.de/wp-content/uploads/2020/11/201104_GemeinsamesPositionspapier_Patientensicherheit-in-pflegerischer-Verantwortung.pdf (accessed on 11 February 2021).
- Opitz, E.; Bösner, S.; Heinis, S.; Stibane, E.C.; Jerrentrup, A. Patientensicherheit schon im Studium vermitteln. Internist 2020, 61, 444–451. [Google Scholar] [CrossRef] [PubMed]
- Amiri, M.; Khademian, Z.; Nikandish, R. The effect of nurse empowerment educational program on patient safety culture: A randomized controlled trial. BMC Med. Educ. 2018, 18, 158. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Doody, O.; Hennessy, T. Mental health nurses experience of the introduction and practice of the Safewards model: A qualitative descriptive study. BMC Nurs. 2021, 20, 41. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heier, L.; Riouchi, D.; Hammerschmidt, J.; Gambashidze, N.; Kocks, A.; Ernstmann, N. Safety Performance in Acute Medical Care: A Qualitative, Explorative Study on the Perspectives of Healthcare Professionals. Healthcare 2021, 9, 1543. https://doi.org/10.3390/healthcare9111543
Heier L, Riouchi D, Hammerschmidt J, Gambashidze N, Kocks A, Ernstmann N. Safety Performance in Acute Medical Care: A Qualitative, Explorative Study on the Perspectives of Healthcare Professionals. Healthcare. 2021; 9(11):1543. https://doi.org/10.3390/healthcare9111543
Chicago/Turabian StyleHeier, Lina, Donia Riouchi, Judith Hammerschmidt, Nikoloz Gambashidze, Andreas Kocks, and Nicole Ernstmann. 2021. "Safety Performance in Acute Medical Care: A Qualitative, Explorative Study on the Perspectives of Healthcare Professionals" Healthcare 9, no. 11: 1543. https://doi.org/10.3390/healthcare9111543
APA StyleHeier, L., Riouchi, D., Hammerschmidt, J., Gambashidze, N., Kocks, A., & Ernstmann, N. (2021). Safety Performance in Acute Medical Care: A Qualitative, Explorative Study on the Perspectives of Healthcare Professionals. Healthcare, 9(11), 1543. https://doi.org/10.3390/healthcare9111543