
Risk Factors for Early Return Visits to the Emergency Department in Patients Presenting with Nonspecific Abdominal Pain and the Use of Computed Tomography Scan

 , ,
, ,
Abstract
:1. Introduction
2. Method
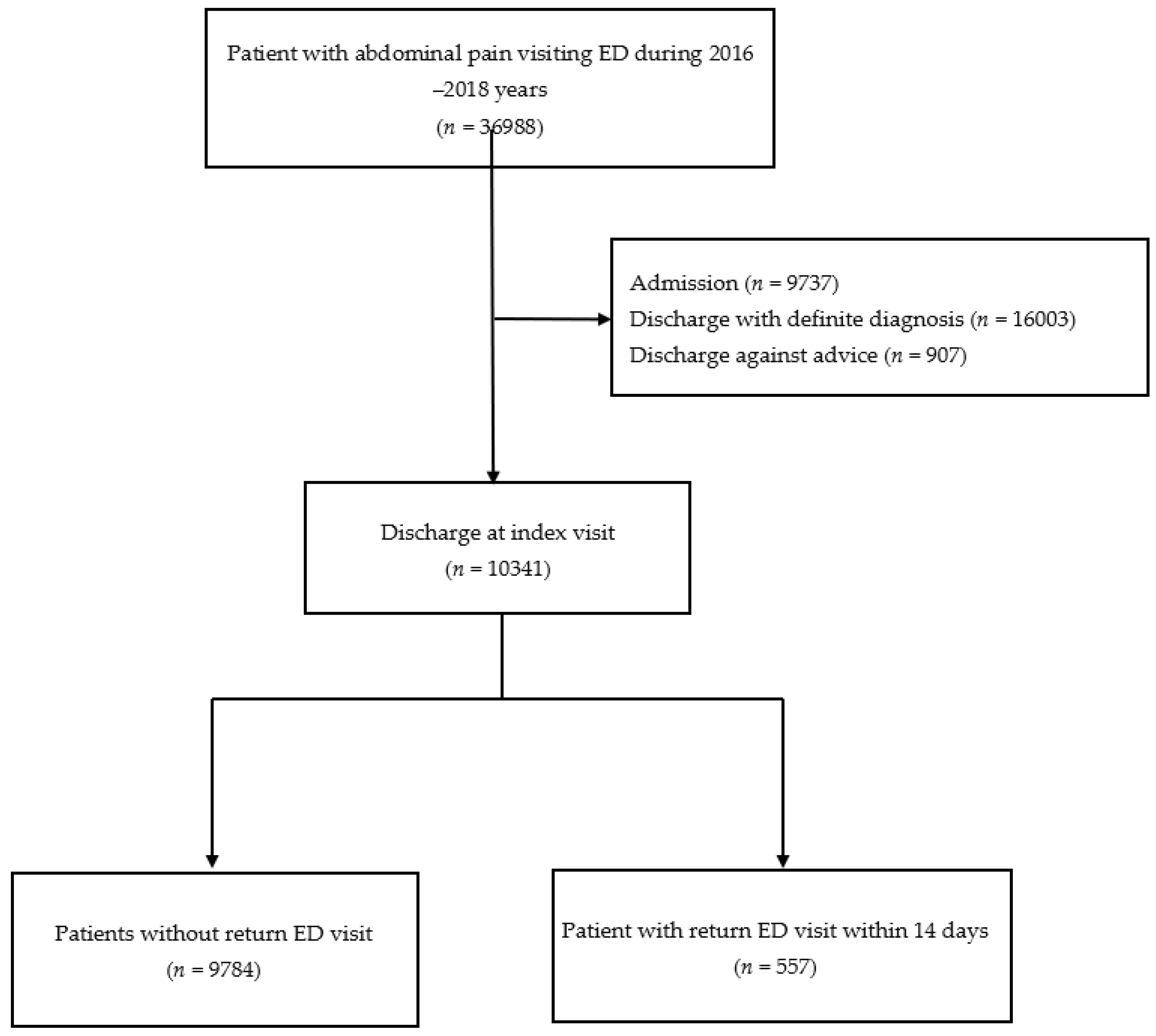
2.1. Study Setting and Patient Population
2.2. Outcome Measurement
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Powers, R.D.; Guertler, A.T. Abdominal pain in the ED: Stability and change over 20 years. Am. J. Emerg. Med. 1995, 13, 301–303. [Google Scholar] [CrossRef]
- Pitts, S.R.; Niska, R.W.; Xu, J.; Burt, C.W. National Hospital Ambulatory Medical Care Survey: 2006 emergency department summary. Natl. Health Stat. Reports 2008, 7, 1–38. [Google Scholar]
- Hastings, R.S.; Powers, R.D. Abdominal pain in the ED: A 35 year retrospective. Am. J. Emerg. Med. 2011, 29, 711–716. [Google Scholar] [CrossRef]
- Lukens, T.W.; Emerman, C.; Effron, D. The natural history and clinical findings in undifferentiated abdominal pain. Ann. Emerg. Med. 1993, 22, 690–696. [Google Scholar] [CrossRef]
- Cervellin, G.; Mora, R.; Ticinesi, A.; Meschi, T.; Comelli, I.; Catena, F.; Lippi, G. Epidemiology and outcomes of acute abdominal pain in a large urban Emergency Department: Retrospective analysis of 5340 cases. Ann. Transl. Med. 2016, 4, 362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ryan, J.; Hendler, J.; Bennett, K.P. Understanding Emergency Department 72-Hour Revisits Among Medicaid Patients Using Electronic Healthcare Records. Big Data 2015, 3, 238–248. [Google Scholar] [CrossRef] [PubMed]
- Truong, M.; Meckler, G.; Doan, Q.H. Emergency Department Return Visits Within a Large Geographic Area. J. Emerg. Med. 2017, 52, 801–808. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.L.; Wang, F.T.; Chiang, Y.C.; Chiu, Y.F.; Lin, T.G.; Fu, L.F.; Tsai, T.L. Unplanned emergency department revisits within 72 hours to a secondary teaching referral hospital in Taiwan. J. Emerg. Med. 2010, 38, 512–517. [Google Scholar] [CrossRef] [PubMed]
- Foran, A.; Wuerth-Sarvis, B.; Milne, W.K. Bounce-back visits in a rural emergency department. Can. J. Rural. Med. 2010, 15, 108–112. [Google Scholar] [PubMed]
- Gunnarsson, O.S.; Birgisson, G.; Oddsdottir, M.; Gudbjartsson, T. One year follow-up of patients discharged from the emergency department with non-specific abdominal pain. Laeknabladid 2011, 97, 231–236. [Google Scholar]
- Verelst, S.; Pierloot, S.; Desruelles, D.; Gillet, J.B.; Bergs, J. Short-term unscheduled return visits of adult patients to the emergency department. J. Emerg. Med. 2014, 47, 131–139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duseja, R.; Bardach, N.S.; Lin, G.A.; Yazdany, J.; Dean, M.L.; Clay, T.H.; Boscardin, W.J.; Dudley, R.A. Revisit rates and associated costs after an emergency department encounter: A multistate analysis. Ann. Intern. Med. 2015, 162, 750–756. [Google Scholar] [CrossRef] [PubMed]
- Hu, K.W.; Lu, Y.H.; Lin, H.J.; Guo, H.R.; Foo, N.P. Unscheduled return visits with and without admission post emergency department discharge. J. Emerg. Med. 2012, 43, 1110–1118. [Google Scholar] [CrossRef]
- Meldon, S.W.; Mion, L.C.; Palmer, R.M.; Drew, B.L.; Connor, J.T.; Lewicki, L.J.; Bass, D.M.; Emerman, C.L. A brief risk-stratification tool to predict repeat emergency department visits and hospitalizations in older patients discharged from the emergency department. Acad. Emerg. Med. 2003, 10, 224–232. [Google Scholar] [CrossRef]
- Martin-Gill, C.; Reiser, R.C. Risk factors for 72-hour admission to the ED. Am. J. Emerg. Med. 2004, 22, 448–453. [Google Scholar] [CrossRef] [PubMed]
- Lerman, B.; Kobernick, M.S. Return visits to the emergency department. J. Emerg. Med. 1987, 5, 359–362. [Google Scholar] [CrossRef] [Green Version]
- Chiang, C.Y.; Cheng, F.J.; Huang, Y.S.; Chen, Y.L.; Wu, K.H.; Chiu, I.M. ICU admission following an unscheduled return visit to the pediatric emergency department within 72 hours. BMC Pediatr. 2019, 19, 268. [Google Scholar] [CrossRef] [PubMed]
- LaMantia, M.A.; Platts-Mills, T.F.; Biese, K.; Khandelwal, C.; Forbach, C.; Cairns, C.B.; Busby-Whitehead, J.; Kizer, J.S. Predicting hospital admission and returns to the emergency department for elderly patients. Acad. Emerg. Med. 2010, 17, 252–259. [Google Scholar] [CrossRef] [PubMed]
- Chiang, C.Y.; Chen, Y.L.; Lin, Y.R.; Cheng, F.J.; Wu, K.H.; Chiu, I.M. Characteristics of Febrile Children Admitted to the ICU Following an Unscheduled ED Revisit Within 72 h, a Case-Control Study. Front. Pediatr. 2020, 8, 411. [Google Scholar] [CrossRef] [PubMed]
- Jorgensen, S.; Zurayk, M.; Yeung, S.; Terry, J.; Dunn, M.; Nieberg, P.; Wong-Beringer, A. Risk factors for early return visits to the emergency department in patients with urinary tract infection. Am. J. Emerg. Med. 2018, 36, 12–17. [Google Scholar] [CrossRef]
- To, T.; Zhu, J.; Ryckman, K.; Gershon, A. Risk Factors for Return to the Emergency Department for Asthma: A Population-Based Study. J. Allergy. Clin. Immunol. Pract. 2018, 6, 1907–1913. [Google Scholar] [CrossRef] [PubMed]
- McCusker, J.; Healey, E.; Bellavance, F.; Connolly, B. Predictors of repeat emergency department visits by elders. Acad. Emerg. Med. 1997, 4, 581–588. [Google Scholar] [CrossRef] [Green Version]
- Poh, X.E.; Wu, K.H.; Chen, C.C.; Huang, J.B.; Cheng, F.J.; Chiu, I.M. Outcomes for Patients with Urinary Tract Infection After an Initial Intravenous Antibiotics Dose Before Emergency Department Discharge. Infect. Dis. Ther. 2021, 10, 1479–1489. [Google Scholar] [CrossRef]
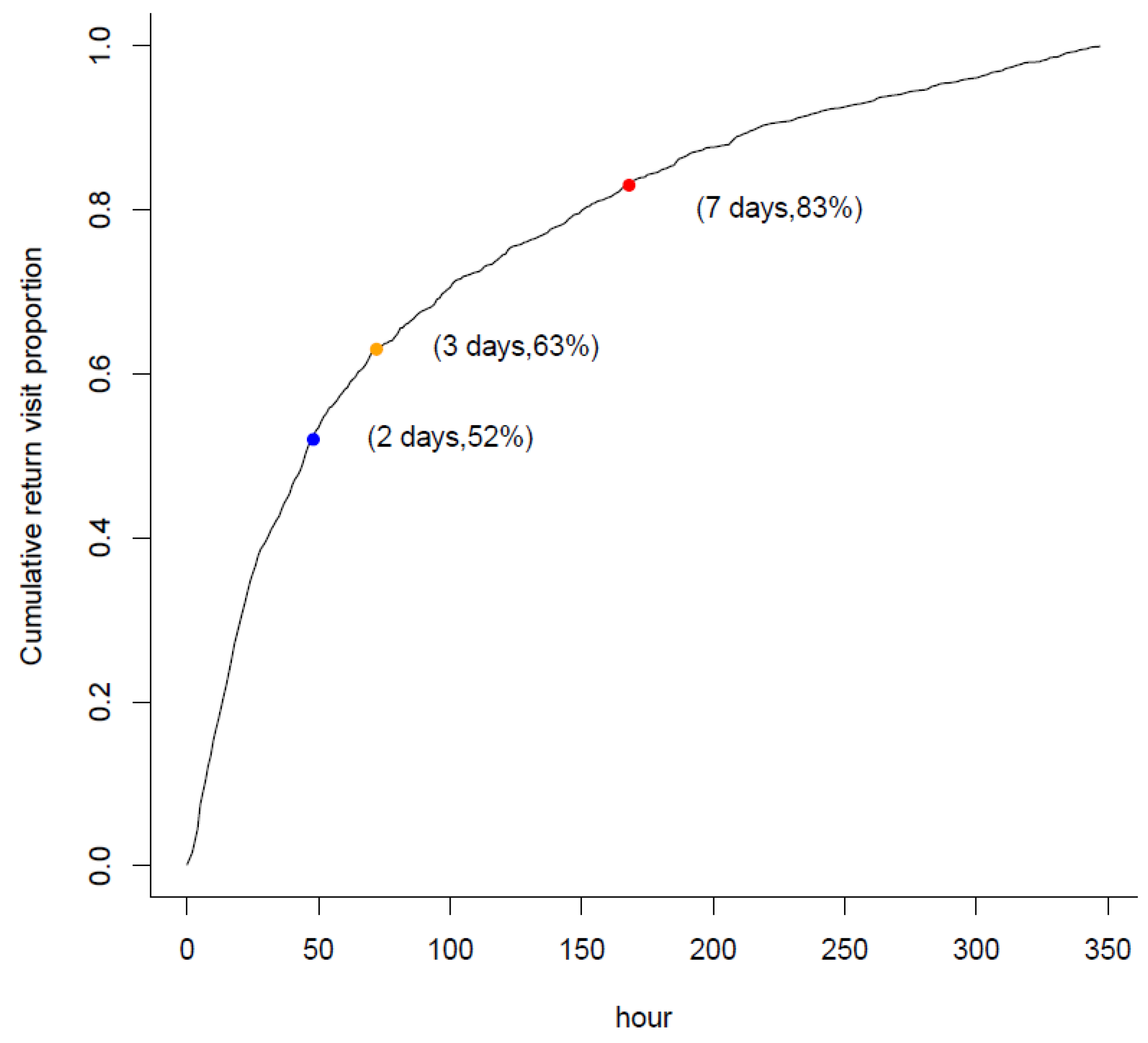
- Rising, K.L.; Victor, T.W.; Hollander, J.E.; Carr, B.G. Patient returns to the emergency department: The time-to-return curve. Acad. Emerg. Med. 2014, 21, 864–871. [Google Scholar] [CrossRef] [PubMed]
- Onur, O.E.; Guneysel, O.; Unluer, E.E.; Akoglu, H.; Cingi, A.; Onur, E.; Denizbasi, A. “Outpatient follow-up” or “Active clinical observation” in patients with nonspecific abdominal pain in the Emergency Department. A randomized clinical trial. Minerva. Chir. 2008, 63, 9–15. [Google Scholar] [PubMed]
- Gerhardt, R.T.; Nelson, B.K.; Keenan, S.; Kernan, L.; MacKersie, A.; Lane, M.S. Derivation of a clinical guideline for the assessment of nonspecific abdominal pain: The Guideline for Abdominal Pain in the ED Setting (GAPEDS) Phase 1 Study. Am. J. Emerg. Med. 2005, 23, 709–717. [Google Scholar] [CrossRef]
- Ravn-Christensen, C.; Qvist, N.; Bay-Nielsen, M.; Bisgaard, T. Pathology is common in subsequent visits after admission for non-specific abdominal pain. Dan. Med. J. 2019, 66, A5549. [Google Scholar] [PubMed]
- Koyuncu, N.; Karcioglu, O.; Sener, S. Nonspecific abdominal pain: A follow-up survey. Niger. J. Clin. Pract. 2018, 21, 332–336. [Google Scholar] [PubMed]
- Gabayan, G.Z.; Asch, S.M.; Hsia, R.Y.; Zingmond, D.; Liang, L.J.; Han, W.; McCreath, H.; Weiss, R.E.; Sun, B.C. Factors associated with short-term bounce-back admissions after emergency department discharge. Ann. Emerg. Med. 2013, 62, 136–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayward, J.; Hagtvedt, R.; Ma, W.; Gauri, A.; Vester, M.; Holroyd, B.R. Predictors of Admission in Adult Unscheduled Return Visits to the Emergency Department. West. J. Emerg. Med. 2018, 19, 912–918. [Google Scholar] [CrossRef] [PubMed]
- Rupp, T.; Delaney, K.A. Inadequate analgesia in emergency medicine. Ann. Emerg. Med. 2004, 43, 494–503. [Google Scholar] [CrossRef] [PubMed]
- Stalnikowicz, R.; Mahamid, R.; Kaspi, S.; Brezis, M. Undertreatment of acute pain in the emergency department: A challenge. Int. J. Qual. Health Care 2005, 17, 173–176. [Google Scholar] [CrossRef] [Green Version]
- Gardner, C.S.; Jaffe, T.A.; Nelson, R.C. Impact of CT in elderly patients presenting to the emergency department with acute abdominal pain. Abdom. Imaging 2015, 40, 2877–2882. [Google Scholar] [CrossRef] [PubMed]
- Hustey, F.M.; Meldon, S.W.; Banet, G.A.; Gerson, L.W.; Blanda, M.; Lewis, L.M. The use of abdominal computed tomography in older ED patients with acute abdominal pain. Am. J. Emerg. Med. 2005, 23, 259–265. [Google Scholar] [CrossRef] [PubMed]
- You, H.; Sweeny, A.; Cooper, M.L.; Von Papen, M.; Innes, J. The management of diverticulitis: A review of the guidelines. Med. J. Aust. 2019, 211, 421–427. [Google Scholar] [CrossRef] [PubMed]
- Rami Reddy, S.R.; Cappell, M.S. A Systematic Review of the Clinical Presentation, Diagnosis, and Treatment of Small Bowel Obstruction. Curr. Gastroenterol. Rep. 2017, 19, 28. [Google Scholar] [CrossRef] [PubMed]
- Goodman, T.R.; Amurao, M. Medical imaging radiation safety for the female patient: Rationale and implementation. Radiographics 2012, 32, 1829–1837. [Google Scholar] [CrossRef] [PubMed]
- Balthazar, E.J.; Birnbaum, B.A.; Yee, J.; Megibow, A.J.; Roshkow, J.; Gray, C. Acute appendicitis: CT and US correlation in 100 patients. Radiology 1994, 190, 31–35. [Google Scholar] [CrossRef]
- Boudiaf, M.; Soyer, P.; Terem, C.; Pelage, J.P.; Maissiat, E.; Rymer, R. CT evaluation of small bowel obstruction. Radiographics 2001, 21, 613–624. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| with Return Visit Median (IQR)/N (%) | without Return Visit Median (IQR)/N (%) | p-Value | |
|---|---|---|---|
| Total number of patients | 557 | 9784 | |
| Age, year | 50 (36–65) | 42 (31–58) | <0.001 |
| Male | 262 (47.0) | 3680 (37.6%) | <0.001 |
| Vital signs at admission | |||
| Temperature, °C | 36.5 (36.1–36.8) | 36.4 (36.1–36.6) | 0.740 |
| Heart rate, beats per minute | 80 (70–92) | 81 (72–92) | 0.110 |
| MAP, mmHg | 104 (92–117) | 100 (89–113) | <0.001 |
| Vital signs at discharge | |||
| Temperature, °C | 36.5 (36.1–36.8) | 36.3 (36.0–36.8) | 0.029 |
| Heart rate, beats per minute | 75 (67–85) | 75 (67–84) | 0.950 |
| MAP, mmHg | 95 (85–106) | 92 (82–103) | <0.001 |
| ED length of stay, hour | 1.7 (1.2–2.7) | 1.8 (1.2–3.0) | 0.190 |
| Chronic disease | |||
| Hypertension | 138 (24.8%) | 1739 (18.8%) | <0.001 |
| DM | 61 (11.0%) | 674 (6.9%) | <0.001 |
| CKD | 21 (3.8%) | 204 (2.1%) | 0.015 |
| Liver cirrhosis | 9 (1.6%) | 123 (1.3%) | 0.435 |
| Malignancy | 58 (10.4%) | 642 (6.2%) | <0.001 |
| ED examination | |||
| Computed tomography | 61 (11.0%) | 1278 (13.1%) | 0.156 |
| X-ray | 325 (58.3%) | 5822 (59.5%) | 0.595 |
| Laboratory test | 399 (71.6%) | 6678 (68.3%) | 0.102 |
| ED medication | |||
| NSAID | 308 (55.3%) | 4782 (48.9%) | 0.003 |
| Opioid | 125 (22.4%) | 1193 (12.2%) | <0.001 |
| Variable | Odds Ratio (95%CI) | p-Value |
|---|---|---|
| Age | 1.007 (1.003–1.011) | 0.004 |
| Male | 1.307 (1.036–1.650) | 0.024 |
| Vital signs | ||
| MAP at admission | 1.005 (0.997–1.012) | 0.213 |
| MAP at discharge | 1.003 (0.993–1.002) | 0.559 |
| Fever at discharge (Temperature ≥ 38 °C) | 2.129 (0.749–6.056) | 0.156 |
| ED medications | ||
| NSAID | 1.563 (1.219–2.003) | <0.001 |
| Opioid | 2.213 (1.643–2.930) | <0.001 |
| ED examinations | ||
| Computed tomography | 0.605 (0.390–0.937) | 0.021 |
| X-ray | 0.819 (0.642–1.04) | 0.106 |
| Laboratory test | 0.992 (0.763–1.290) | 0.954 |
| Chronic disease | ||
| Hypertension | 1.313 (0.905–1.791) | 0.102 |
| DM | 0.940 (0.633–1.376) | 0.759 |
| CKD | 1.174 (0.919–1.500) | 0.198 |
| Liver cirrhosis | 0.992 (0.444–2.217) | 0.984 |
| Malignancy | 0.946 (0.628–1.426) | 0.791 |
| Subgroup | Number | Odds Ratio (95% CI) | p-Value | |
|---|---|---|---|---|
| Age ≤ 60 years old | 7971 | 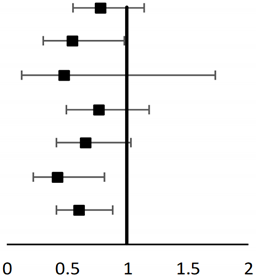 | 0.789 (0.547–1.137) | 0.204 |
| Age > 60 years old | 2370 | 0.544 (0.302–0.978) | 0.036 | |
| Age > 80 years old | 470 | 0.477 (0.132–1.730) | 0.26 | |
| Male | 3942 | 0.765 (0.496–1.180) | 0.226 | |
| Female | 6399 | 0.656 (0.419–1.026) | 0.065 | |
| Underlying disease | 2027 | 0.423 (0.221–0.812) | 0.01 | |
| Receive pain control | 6098 | 0.609 (0.419–0.884) | 0.009 | |
| Outcomes in Return Visit | Without CT Scan during Index ED Visit N = 496 | With CT Scan during Index ED Visit N = 61 | p-Value |
|---|---|---|---|
| Diagnosed with NSAP | 257 (51.8%) | 38 (74.5%) | <0.001 |
| Discharge | 337 (57.7%) | 51 (83.6%) | <0.001 |
| Admission | 158 (31.9%) | 10 (16.4%) | 0.002 |
| Surgery | 76 (15.3%) | 5 (8.2%) | 0.008 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yau, F.-F.F.; Yang, Y.; Cheng, C.-Y.; Li, C.-J.; Wang, S.-H.; Chiu, I.-M. Risk Factors for Early Return Visits to the Emergency Department in Patients Presenting with Nonspecific Abdominal Pain and the Use of Computed Tomography Scan. Healthcare 2021, 9, 1470. https://doi.org/10.3390/healthcare9111470
Yau F-FF, Yang Y, Cheng C-Y, Li C-J, Wang S-H, Chiu I-M. Risk Factors for Early Return Visits to the Emergency Department in Patients Presenting with Nonspecific Abdominal Pain and the Use of Computed Tomography Scan. Healthcare. 2021; 9(11):1470. https://doi.org/10.3390/healthcare9111470
Chicago/Turabian StyleYau, Fei-Fei Flora, Ying Yang, Chi-Yung Cheng, Chao-Jui Li, Su-Hung Wang, and I-Min Chiu. 2021. "Risk Factors for Early Return Visits to the Emergency Department in Patients Presenting with Nonspecific Abdominal Pain and the Use of Computed Tomography Scan" Healthcare 9, no. 11: 1470. https://doi.org/10.3390/healthcare9111470
APA StyleYau, F.-F. F., Yang, Y., Cheng, C.-Y., Li, C.-J., Wang, S.-H., & Chiu, I.-M. (2021). Risk Factors for Early Return Visits to the Emergency Department in Patients Presenting with Nonspecific Abdominal Pain and the Use of Computed Tomography Scan. Healthcare, 9(11), 1470. https://doi.org/10.3390/healthcare9111470