
Vietnamese Version of the General Medication Adherence Scale (GMAS): Translation, Adaptation, and Validation


 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Study Design
2.2.1. Stage I—Initial Translation
2.2.2. Stage II—Synthesis of Two Translations
2.2.3. Stage III—Back Translation
2.2.4. Stage IV—Expert Committee Review
- Step 4.1.
- Assessing the GMAS: The expert committee evaluated the equivalence of each question in the translations compared to the original independently. The researcher designed the assessment form, including all versions of the GMAS and the content that needed adjustment. The evaluation criteria included semantic equivalence, idiomatic equivalence, experiential equivalence, and conceptual equivalence—rating scale: 1 point if there is equivalent and 0 points if there is no equivalent.
- Step 4.2.
- Adjustment of questions that did not gain equivalent score: The questions did not achieve absolute equivalence (10/10) for four criteria, and suggestions for adjusting the content of the scale (proposed by members of the committee in Step 4.1) were synthesized by the researcher. They were sent to the members of the committee, who reviewed and adjusted them.
- Step 4.3.
- Assessing the GMAS after adjustment: The questions after adjusting were evaluated for the second equivalence by the expert committee as the four criteria and scale in Step 4.1. After this step, the pre-final version of the GMAS was generated and used for pilot testing.
2.2.5. Stage V—The Pilot Testing
2.3. Materials
- Option one: medication adherence is divided into two levels, including adherence (≥27 points) and non-adherence (<27 points).
- Option two: medication adherence is divided into five levels, including high adherence (30–33 points), good adherence (27–29 points), partial adherence (17–26 points), low adherence (11–16 points), and poor adherence (0–10 points).
2.4. Psychometric Validation of the GMAS
2.4.1. Sample Size
2.4.2. Psychometric Validation
2.5. Statistical Analysis
2.6. Ethical Approval
3. Results
3.1. Translation and Cross-Cultural Adaptation of the GMAS
3.2. Psychometric Validation of the GMAS
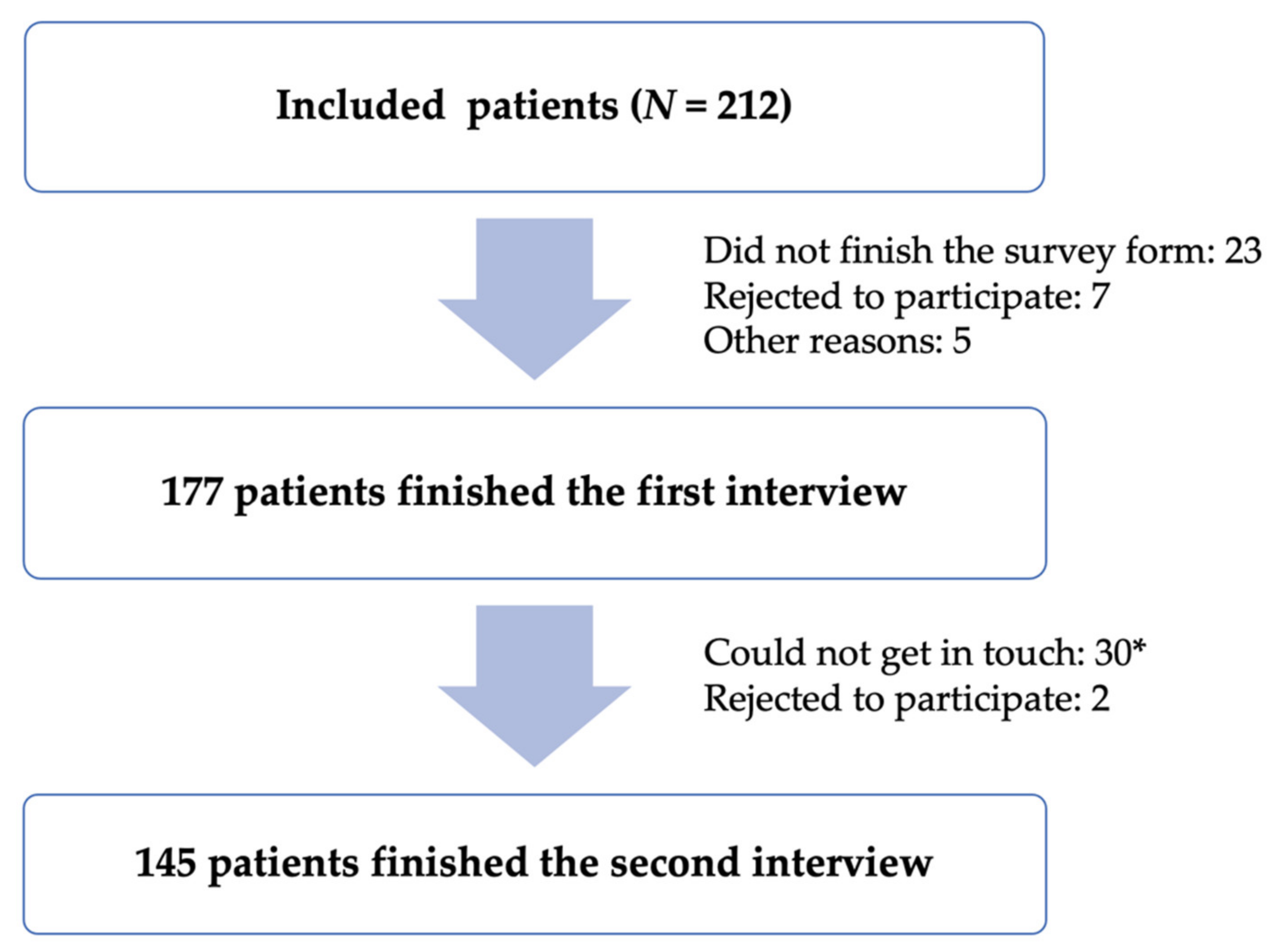
3.2.1. Patients’ Demographic Characteristics
3.2.2. Internal Consistency
3.2.3. Test–Retest Reliability
3.2.4. Content Validity
3.2.5. Construct Validity
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Question | Semantic Equivalence | Idiomatic Equivalence | Experiential Equivalence | Conceptual Equivalence |
|---|---|---|---|---|
| 1 | 10/10 | 10/10 | 10/10 | 10/10 |
| 2 | 10/10 | 10/10 | 10/10 | 10/10 |
| 3 | 10/10 | 10/10 | 10/10 | 10/10 |
| 4 | 10/10 | 10/10 | 10/10 | 10/10 |
| 5 | 10/10 | 10/10 | 10/10 | 10/10 |
| 6 | 9/10 | 10/10 | 10/10 | 10/10 |
| 7 | 10/10 | 10/10 | 10/10 | 10/10 |
| 8 | 10/10 | 10/10 | 10/10 | 10/10 |
| 9 | 10/10 | 10/10 | 10/10 | 10/10 |
| 10 | 10/10 | 10/10 | 10/10 | 10/10 |
| 11 | 10/10 | 10/10 | 10/10 | 10/10 |
| Average score | 109/110 (0.99) | 110/110 (1.00) | 110/110 (1.00) | 110/110 (1.00) |
Appendix B
| Question | Score (Mean ± SD) |
|---|---|
| I (instruction) | 9.98 ± 0.15 |
| 1a | 9.95 ± 0.22 |
| 1b | 9.95 ± 0.22 |
| 2 | 10.00 ± 0.00 |
| 3 | 10.00 ± 0.00 |
| 4a | 10.00 ± 0.00 |
| 4b | 10.00 ± 0.00 |
| 5 | 10.00 ± 0.00 |
| 6a | 10.00 ± 0.00 |
| 6b | 8.93 ± 0.75 |
| 7 | 10.00 ± 0.00 |
| 8 | 9.88 ± 0.33 |
| 9 | 9.95 ± 0.22 |
| 10 | 9.98 ± 0.15 |
| 11 | 9.98 ± 0.15 |
| Overall score (6a) | 9.98 ± 0.06 |
| Overall score (6b) | 9.91 ± 0.09 |
Appendix C
| Dưới đây là những câu hỏi liên quan đến việc dùng thuốc điều trị đái tháo đường của ông (bà). Ở mỗi câu hỏi, ông (bà) vui lòng cho biết “mức độ” ứng với tình trạng dùng thuốc thực sự của ông (bà). | |||
|---|---|---|---|
| Câu hỏi | Nội dung | ||
| 1 | Ông (bà) có gặp khó khăn trong việc nhớ dùng thuốc không? | ||
| 2 | Ông (bà) có quên dùng thuốc do lịch trình bận rộn như du lịch, hội họp, đám tiệc, đám cưới, đi nhà thờ/chùa… không? | ||
| 3 | Khi cảm thấy khỏe, ông (bà) có ngưng dùng thuốc không? | ||
| 4 | Ông (bà) có ngưng dùng thuốc khi gặp các tác dụng không mong muốn như khó chịu ở dạ dày… không? | ||
| 5 | Ông (bà) có ngưng dùng thuốc mà không báo cho bác sĩ biết không? | ||
| 6 | Ông (bà) có ngưng dùng thuốc (điều trị đái tháo đường) do phải dùng thêm các thuốc cho bệnh khác không? | ||
| 7 | Ông (bà) có thấy bất tiện để nhớ dùng thuốc vì chế độ thuốc phức tạp không? | ||
| 8 | Trong tháng qua, có khi nào ông (bà) quên dùng thuốc vì bệnh nặng hơn và cần dùng thêm thuốc mới không? | ||
| 9 | Ông (bà) có tự ý thay đổi chế độ thuốc như liều, số lần dùng thuốc trong ngày không? | ||
| 10 | Ông (bà) có ngưng dùng thuốc vì (các) thuốc này không đáng với số tiền bỏ ra không? | ||
| 11 | Ông (bà) có gặp khó khăn để mua (các) thuốc vì chúng đắt tiền không? | ||
| Mỗi câu hỏi có 4 mức lựa chọn: luôn luôn (0 điểm), thường xuyên (1 điểm), thỉnh thoảng/đôi khi (2 điểm), không bao giờ (3 điểm). | |||
| Tổng điểm tuân thủ tích lũy (cách tính điểm cũ): | |||
| Tuân thủ cao | 30–33 điểm | Tuân thủ tốt | 27–29 điểm |
| Tuân thủ 1 phần | 17–26 điểm | Tuân thủ thấp | 11–16 điểm |
| Tuân thủ kém | 0–10 điểm | ||
| Tổng điểm tuân thủ tích lũy theo (cách tính mới): | |||
| Tuân thủ | ≥27 điểm | ||
| Không tuân thủ | <27 điểm | ||
Appendix D
| Characteristics | p-Value a | |
|---|---|---|
| Age group (year) | <45 | 0.599 |
| 45–64 | ||
| ≥65 | ||
| Gender | Female | 0.510 |
| Male | ||
| Occupation | Not working | 0.042 |
| Officer | ||
| Trader | ||
| Unskilled labor | ||
| Education level | Elementary school | 0.540 |
| High school | ||
| College/university/higher | ||
| Monthly income (million VND) | 3–5 | 0.001 |
| 5–10 | ||
| >10 | ||
| Duration of diabetes (year) | <5 | 0.335 |
| 5–10 | ||
| >10 | ||
| Chronic comorbidity | Yes | 0.059 |
| No | ||
| Treatment with insulin | Yes | 0.519 |
| No | ||
| BMQ–V (mean ± SD) | Specific-Necessity | <0.001 |
| Specific-Concerns | 0.915 | |
References
- Viswanathan, M.; Golin, C.E.; Jones, C.D.; Ashok, M.; Blalock, S.; Wines, R.C.M.; Coker-Schwimmer, E.J.L.; Grodensky, C.A.; Rosen, D.L.; Yuen, A.; et al. Closing the quality gap: Revisiting the state of the science (vol. 4: Medication adherence interventions: Comparative effectiveness). Evid. Rep. Technol. Assess. 2012, 1, 1–685. [Google Scholar]
- Saeedi, P.; Petersohn, I.; Salpea, P.; Malanda, B.; Karuranga, S.; Unwin, N.; Colagiuri, S.; Guariguata, L.; Motala, A.A.; Ogurtsova, K.; et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas. Diabetes Res. Clin. Pract. 2019, 157, 107843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Association, A.D. Glycemic Targets: Standards of Medical Care in Diabetes—2020. Diabetes Care 2020, 43 (Suppl. 1), S66–S76. [Google Scholar] [CrossRef] [PubMed]
- Bayisa, B.; Bekele, M. Glycemic control and associated factors among type, I.I.; diabetic patients on chronic follow up at Southwest Ethiopia. J. Med. Health Sci. 2017, 6, 341–349. [Google Scholar]
- Yue, J.; Mao, X.; Xu, K.; Lü, L.; Liu, S.; Chen, F.; Wang, J. Prevalence, awareness, treatment and control of diabetes mellitus in a Chinese population. PLoS ONE 2016, 11, e0153791. [Google Scholar] [CrossRef] [PubMed]
- Omar, S.M.; Musa, I.E.; ElSouli, A.; Adam, I. Prevalence, risk factors, and glycaemic control of type 2 diabetes mellitus in eastern Sudan: A community-based study. Ther. Adv. Endocrinol. Metab. 2019, 10, 2042018819860071. [Google Scholar] [CrossRef] [PubMed]
- Borgharkar, S.S.; Das, S.S. Real-world evidence of glycemic control among patients with type 2 diabetes mellitus in India: The TIGHT study. BMJ Open Diabetes Res. Care 2019, 7, e000654. [Google Scholar] [CrossRef] [Green Version]
- Osterberg, L.; Blaschke, T. Adherence to medication. N. Engl. J. Med. 2005, 353, 487–497. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, T.; Cao, H.T.K.; Quach, D.N.; Le, K.K.; Au, S.X.; Pham, S.T.; Nguyen, T.H.; Pham, T.T.; Taxis, K. Translation and cross-cultural adaptation of the brief illness perception questionnaire, the beliefs about medicines questionnaire and the Morisky Medication Adherence Scale into Vietnamese. Pharmacoepidemiol. Drug Saf. 2015, 24, 159–160. [Google Scholar]
- Beaton, D.E.; Bombardier, C.; Guillemin, F.; Ferraz, M.B. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine 2000, 25, 3186–3191. [Google Scholar] [CrossRef] [Green Version]
- Beaton, D.; Bombardier, C.; Guillemin, F.; Ferraz, M.B. Recommendations for the cross-cultural adaptation of the DASH & QuickDASH outcome measures. Inst. Work Health 2007, 1, 1–45. [Google Scholar]
- Naqvi, A.A.; Hassali, M.A.; Rizvi, M.; Zehra, A.; Iffat, W.; Haseeb, A.; Jamshed, S. Development and validation of a novel General Medication Adherence Scale (GMAS) for chronic illness patients in Pakistan. Front. Pharmacol. 2018, 9, 1124. [Google Scholar] [CrossRef] [Green Version]
- Naqvi, A.A.; Hassali, M.A.; Jahangir, A.; Nadir, M.N.; Kachela, B. Translation and validation of the English version of the general medication adherence scale (GMAS) in patients with chronic illnesses. J. Drug Assess. 2019, 8, 36–42. [Google Scholar] [CrossRef] [Green Version]
- Tsang, S.; Royse, C.F.; Terkawi, A.S. Guidelines for developing, translating, and validating a questionnaire in perioperative and pain medicine. Saudi J. Anaesth. 2017, 11 (Suppl. 1), S80. [Google Scholar] [CrossRef]
- Nunnally, J.C. Psychometric Theory, 3rd ed.; Tata McGraw-Hill Education: New York, NY, USA, 1994. [Google Scholar]
- Comrey, A.; Lee, H. A First Course in Factor Analysis; Lawrence Eribaum Associates, Inc. Publishers: Hillsdale, NJ, USA, 1992. [Google Scholar]
- Terwee, C.B.; Bot, S.D.; de Boer, M.R.; van der Windt, D.A.; Knol, D.L.; Dekker, J.; Bouter, L.M.; de Vet, H.C. Quality criteria were proposed for measurement properties of health status questionnaires. J. Clin. Epidemiol. 2007, 60, 34–42. [Google Scholar] [CrossRef] [Green Version]
- Kimberlin, C.L.; Winterstein, A.G. Validity and reliability of measurement instruments used in research. Am. J. Health-Syst. Pharmacy 2008, 65, 2276–2284. [Google Scholar] [CrossRef]
- Devon, H.A.; Block, M.E.; Moyle-Wright, P.; Ernst, D.M.; Hayden, S.J.; Lazzara, D.J.; Savoy, S.M.; Kostas-Polston, E. A psychometric toolbox for testing validity and reliability. J. Nurs. Scholarsh. 2007, 39, 155–164. [Google Scholar] [CrossRef]
- Huynh, Q.N.P.; Nguyen, T.; Truong, T.T.A.; Huynh, M.N.H.; Nguyen, T.H.; Ghisi, G.L.D.M.; Taxis, K. Vietnamese version of the coronary artery disease education questionnaire—Short version: Translation, adaptation and validation. J. Clin. Pharm. Ther. 2020, 45, 691–697. [Google Scholar] [CrossRef]
- Taber, K.S. The use of Cronbach’s alpha when developing and reporting research instruments in science education. Res. Sci. Educ. 2018, 48, 1273–1296. [Google Scholar] [CrossRef]
- Naqvi, A.A.; Hassali, M.A.; Rizvi, M.; Zehra, A.; Nisa, Z.-U.; Islam, A.; Iqbal, M.S.; Farooqui, M.; Imam, M.T.; Hossain, M.A.; et al. Validation of the General Medication Adherence Scale in Pakistani patients with rheumatoid arthritis. Front. Pharmacol. 2020, 11, 1039. [Google Scholar] [CrossRef]
- Naqvi, A.A.; Al-Shayban, D.M.; Ghori, S.A.; Mahmoud, M.A.; Haseeb, A.; Faidah, H.S.; Hassali, M.A. Validation of the General Medication Adherence Scale (GMAS) in Saudi patients with chronic disease. Front. Pharmacol. 2019, 10, 633. [Google Scholar] [CrossRef] [Green Version]
- Nonogaki, A.; Heang, H.; Yi, S.; Van Pelt, M.; Yamashina, H.; Taniguchi, C.; Nishida, T.; Sakakibara, H. Factors associated with medication adherence among people with diabetes mellitus in poor urban areas of Cambodia: A cross-sectional study. PLoS ONE 2019, 14, e0225000. [Google Scholar] [CrossRef] [Green Version]
- Mallah, Z.; Hammoud, Y.; Awada, S.; Rachidi, S.; Zein, S.; Ballout, H.; Al-Hajje, A. Validation of diabetes medication adherence scale in the Lebanese population. Diabetes Res. Clin. Pract. 2019, 156, 107837. [Google Scholar] [CrossRef]
| Characteristics | Number (n = 177) | Percentage |
|---|---|---|
| Age | ||
| Mean ± SD | 59.40 ± 8.67 | |
| <45 | 11 | 6.2 |
| 45–64 | 120 | 67.8 |
| ≥65 | 46 | 26.0 |
| Gender | ||
| Female | 120 | 67.8 |
| Male | 57 | 32.2 |
| Occupation | ||
| Not working | 122 | 68.9 |
| Officer | 24 | 13.6 |
| Trader | 16 | 9.0 |
| Unskilled labor | 15 | 8.5 |
| Education level | ||
| Elementary school | 17 | 9.6 |
| High school | 103 | 58.2 |
| College/university/higher | 57 | 32.2 |
| Monthly income (million VND) | ||
| 3–5 | 13 | 7.3 |
| 5–10 | 125 | 70.6 |
| >10 | 39 | 22.1 |
| Duration of diabetes (years) | ||
| <5 | 76 | 43.0 |
| 5–10 | 45 | 25.4 |
| >10 | 56 | 31.6 |
| Chronic comorbidity | ||
| Yes | 146 | 82.5 |
| No | 31 | 17.5 |
| Type of comorbidity | ||
| Hypertension | 99 | 67.8 |
| Dyslipidemia | 82 | 56.2 |
| Ischemic heart disease | 26 | 17.8 |
| Treatment with insulin | ||
| Yes | 45 | 25.4 |
| No | 132 | 74.6 |
| BMQ–V (mean ± SD) | ||
| Specific necessity | 19.99 ± 4.48 | |
| Specific concerns | 12.97 ± 2.11 | |
| Domains/Subscale | Item | Corrected Item-Total Correlation | Cronbach’s Alpha If Item Deleted | Cronbach’s Alpha for Each Domain | Cronbach’s Alpha for the Total Scale |
|---|---|---|---|---|---|
| Non-adherence due to patient behavior (intentional and unintentional) | 1 | 0.579 | 0.793 | 0.731 | 0.817 |
| 2 | 0.385 | 0.811 | |||
| 3 | 0.481 | 0.803 | |||
| 4 | 0.352 | 0.813 | |||
| 5 | 0.765 | 0.771 | |||
| Non-adherence due to additional disease and pill burden and | 6 | 0.570 | 0.794 | 0.686 | |
| 7 | 0.516 | 0.800 | |||
| 8 | 0.507 | 0.802 | |||
| 9 | 0.430 | 0.808 | |||
| Non-adherence due to financial constraints | 10 | 0.362 | 0.813 | 0.700 | |
| 11 | 0.351 | 0.814 |
| Item | Spearman’s Correlation Coefficient | p-Value |
|---|---|---|
| 1 | 0.887 | <0.001 |
| 2 | 0.883 | <0.001 |
| 3 | 0.756 | <0.001 |
| 4 | 0.807 | <0.001 |
| 5 | 0.905 | <0.001 |
| 6 | 0.898 | <0.001 |
| 7 | 0.804 | <0.001 |
| 8 | 0.826 | <0.001 |
| 9 | 0.711 | <0.001 |
| 10 | 0.696 | <0.001 |
| 11 | 0.714 | <0.001 |
| For all item | 0.879 | <0.001 |
| Characteristics | Adherence | Non-Adherence | p-Value a | ||
|---|---|---|---|---|---|
| Number | % | Number | % | ||
| Age group (year) | 0.207 | ||||
| <45 | 9 | 81.8 | 2 | 18.2 | |
| 45–64 | 81 | 67.5 | 39 | 32.5 | |
| ≥65 | 26 | 56.5 | 20 | 43.5 | |
| Gender | 0.425 | ||||
| Female | 81 | 67.5 | 39 | 32.5 | |
| Male | 35 | 61.4 | 22 | 38.6 | |
| Occupation | 0.012 | ||||
| Not-working | 78 | 63.9 | 44 | 36.1 | |
| Officer | 22 | 91.7 | 2 | 8.3 | |
| Trader | 7 | 43.8 | 9 | 56.2 | |
| Unskilled labor | 9 | 60.0 | 6 | 40.0 | |
| Education level | 0.756 | ||||
| Elementary school | 10 | 58.8 | 7 | 41.2 | |
| High school | 67 | 65.0 | 36 | 35.0 | |
| College/university/higher | 39 | 68.4 | 18 | 31.6 | |
| Monthly income (million VND) | 0.015 | ||||
| 3–5 | 4 | 30.8 | 9 | 69.2 | |
| 5–10 | 83 | 66.4 | 42 | 33.6 | |
| >10 | 29 | 74.4 | 10 | 25.6 | |
| Duration of diabetes (year) | 0.549 | ||||
| <5 | 50 | 65.8 | 26 | 34.2 | |
| 5–10 | 32 | 71.1 | 13 | 28.9 | |
| >10 | 34 | 65.5 | 22 | 34.5 | |
| Chronic comorbidity | 0.895 | ||||
| Yes | 96 | 65.8 | 50 | 34.2 | |
| No | 20 | 64.5 | 11 | 35.5 | |
| Treatment with insulin | 0.205 | ||||
| Yes | 26 | 57.8 | 19 | 42.2 | |
| No | 90 | 68.2 | 42 | 31.8 | |
| BMQ-V (mean ± SD) | |||||
| Specific-Necessity | 20.77 ± 2.70 18.51 ± 4.24 | 0.001 | |||
| Specific-Concerns | 12.91 ± 2.05 13.07 ± 2.24 | 0.612 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nguyen, T.H.; Truong, H.V.; Vi, M.T.; Taxis, K.; Nguyen, T.; Nguyen, K.T. Vietnamese Version of the General Medication Adherence Scale (GMAS): Translation, Adaptation, and Validation. Healthcare 2021, 9, 1471. https://doi.org/10.3390/healthcare9111471
Nguyen TH, Truong HV, Vi MT, Taxis K, Nguyen T, Nguyen KT. Vietnamese Version of the General Medication Adherence Scale (GMAS): Translation, Adaptation, and Validation. Healthcare. 2021; 9(11):1471. https://doi.org/10.3390/healthcare9111471
Chicago/Turabian StyleNguyen, Thao Huong, Hoa Van Truong, Mai Tuyet Vi, Katja Taxis, Thang Nguyen, and Kien Trung Nguyen. 2021. "Vietnamese Version of the General Medication Adherence Scale (GMAS): Translation, Adaptation, and Validation" Healthcare 9, no. 11: 1471. https://doi.org/10.3390/healthcare9111471
APA StyleNguyen, T. H., Truong, H. V., Vi, M. T., Taxis, K., Nguyen, T., & Nguyen, K. T. (2021). Vietnamese Version of the General Medication Adherence Scale (GMAS): Translation, Adaptation, and Validation. Healthcare, 9(11), 1471. https://doi.org/10.3390/healthcare9111471