
Should We Be Screening for and Treating Periodontal Disease in Individuals Who Are at Risk of Rheumatoid Arthritis?


{kind=link}
Abstract
:1. Introduction
2. The Association between Rheumatoid Arthritis and Periodontitis
3. Why Should We Identify Individuals at Risk of Rheumatoid Arthritis?
4. How Can We Identify Individuals at Risk of Rheumatoid Arthritis?
5. How Should We Screen At-Risk Individuals for Periodontitis?
6. How Should We Treat PD in Individuals at Risk of RA
7. Where Should the Periodontal Screening/Treatment Take Place
8. How Should We Measure the Outcome of Treatment?
9. The Acceptability of Identifying and Modifying Risk Factors in Individuals at Risk of RA
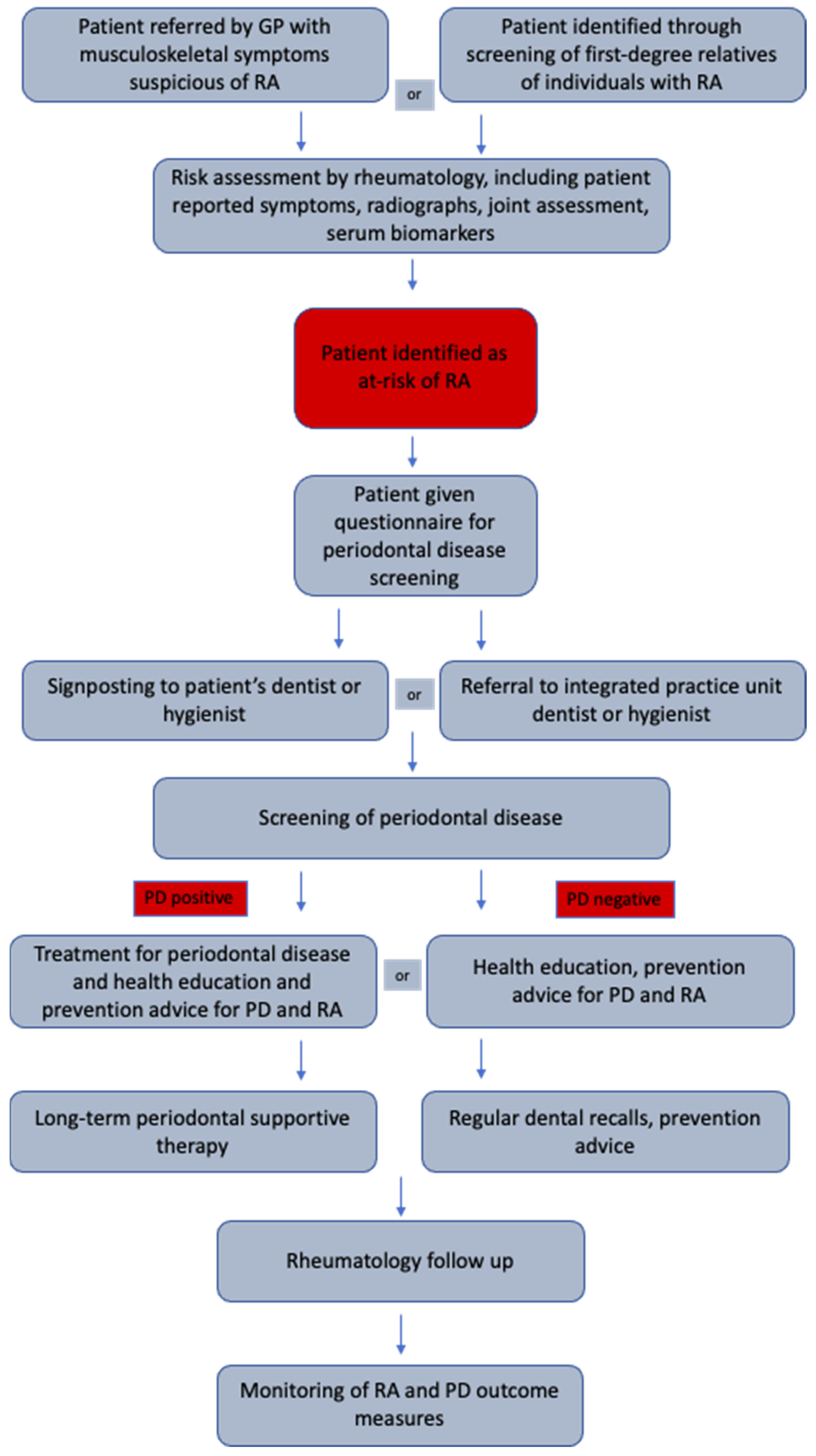
10. A Model for Treating PD in the At-Risk Population
11. Research Agenda
12. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hajishengallis, G.; Darveau, R.P.; Curtis, M.A. The keystone-pathogen hypothesis. Nat. Rev. Microbiol. 2012, 10, 717–725. [Google Scholar] [CrossRef]
- Hajishengallis, G.; Liang, S.; Payne, M.A.; Hashim, A.; Jotwani, R.; Eskan, M.A.; McIntosh, M.L. Low-abundance biofilm species orchestrates inflammatory periodontal disease through the commensal microbiota and complement. Cell Host Microbe 2011, 10, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Botelho, J.; Proenca, L.; Leira, Y.; Chambrone, L.; Mendes, J.J.; Machado, V. Economic Burden of Periodontal Disease in Europe and the United States of America-An updated forecast. medRxiv 2021. Online Ahead of Print. [Google Scholar] [CrossRef]
- Silman, J.A.; Pearson, J.E. Epidemiology and genetics of rheumatoid arthritis. Arthritis Res. Ther. 2002, 4, 1–8. [Google Scholar]
- Guo, Q.; Wang, Y.; Xu, D.; Nossent, J.; Pavlos, N.J.; Xu, J. Rheumatoid arthritis: Pathological mechanisms and modern pharmacologic therapies. Bone Res. 2018, 6, 1–14. [Google Scholar] [CrossRef]
- Verstappen, S.M.M.; Jacobs, J.W.G.; van der Veen, M.J.; Heurkens, A.H.M.; Schenk, Y.; Borg, E.J.T.; Blaauw, A.A.M.; Bijlsma, J.W.J.; The Utrecht Rheumatoid Arthritis Cohort Study Group. Intensive treatment with methotrexate in early rheumatoid arthritis: Aiming for remission. Computer Assisted Management in Early Rheumatoid Arthritis (CAMERA, an open-label strategy trial). Ann. Rheum. Dis. 2007, 66, 1443–1449. [Google Scholar] [CrossRef] [Green Version]
- Van der Linden, M.P.M.; Cessie, S.L.; Raza, K.; Woude, D.V.D.; Knevel, R.; Huizinga, T.W.J.; Van der Helm-van Mil, A.H.M. Long-term impact of delay in assessment of patients with early arthritis. Arthritis Rheum. 2010, 62, 3537–3546. [Google Scholar] [CrossRef]
- Taylor, P.C.; Moore, A.; Vasilescu, R.; Alvir, J.; Tarallo, M. A structured literature review of the burden of illness and unmet needs in patients with rheumatoid arthritis: A current perspective. Rheumatol. Int. 2016, 36, 685–695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burgers, L.E.; Raza, K.; Van Der Helm-Van, A.H. Window of opportunity in rheumatoid arthritis—Definitions and supporting evidence: From old to new perspectives. RMD Open 2019, 5, e000870. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cooper, N.J. Economic burden of rheumatoid arthritis: A systematic review. Rheumatology 2000, 39, 28–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ceccarelli, F.; Saccucci, M.; Di Carlo, G.; Lucchetti, R.; Pilloni, A.; Pranno, N.; Luzzi, V.; Valesini, G.; Polimeni, A. Periodontitis and Rheumatoid Arthritis: The Same Inflammatory Mediators? Mediat. Inflamm. 2019, 2019, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Herrera, M.; Silvestre-Rangil, J.; Silvestre, F.J. Association between obesity and periodontal disease. A systematic review of epidemiological studies and controlled clinical trials. Med. Oral Patol. Oral Y Cir. Bucal 2017, 22, e708. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira Ferreira, R.; de Brito Silva, R.; Magno, M.B.; Carvalho Almeida, A.P.C.P.S.; Fagundes, N.C.F.; Maia, L.C.; Lima, R.R. Does periodontitis represent a risk factor for rheumatoid arthritis? A systematic review and meta-analysis. Ther. Adv. Musculoskelet. Dis. 2019, 11, 1759720X19858514. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.; Liu, Z.; Shu, D.; Xiong, Y.; He, M.; Xu, S.; Guo, B. Association of periodontitis with rheumatoid arthritis and the effect of non-surgical periodontal treatment on disease activity in patients with rheumatoid arthritis. Med. Sci. Monit. 2018, 24, 5802. [Google Scholar] [CrossRef]
- Bıyıkoğlu, B.; Buduneli, N.; Aksu, K.; Nalbantsoy, A.; Lappin, D.F.; Evrenosoğlu, E.; Kinane, D.F. Periodontal therapy in chronic periodontitis lowers gingival crevicular fluid interleukin-1beta and DAS28 in rheumatoid arthritis patients. Rheumatol. Int. 2013, 33, 2607–2616. [Google Scholar] [CrossRef]
- Moura, M.F.; Cota, L.O.M.; Silva, T.A.; Cortelli, S.C.; Ferreira, G.A.; López, M.M.; Cortelli, J.R.; Costa, F.O. Clinical and microbiological effects of non-surgical periodontal treatment in individuals with rheumatoid arthritis: A controlled clinical trial. Odontology 2021, 109, 484–493. [Google Scholar] [CrossRef]
- Mankia, K.; Cheng, Z.; Do, T.; Hunt, L.; Meade, J.; Kang, J.; Clerehugh, V.; Speirs, A.; Tugnait, A.; Hensor, E.M.A.; et al. Prevalence of Periodontal Disease and Periodontopathic Bacteria in Anti–Cyclic Citrullinated Protein Antibody–Positive At-Risk Adults Without Arthritis. JAMA Netw. Open 2019, 2, e195394. [Google Scholar] [CrossRef]
- Loutan, L.; Alpizar-Rodriguez, D.; Courvoisier, D.S.; Finckh, A.; Mombelli, A.; Giannopoulou, C. Periodontal status correlates with anti-citrullinated protein antibodies in first-degree relatives of individuals with rheumatoid arthritis. J. Clin. Periodontol. 2019, 46, 690–698. [Google Scholar] [CrossRef]
- Harvey, G.P.; Fitzsimmons, T.R.; Dhamarpatni, A.A.S.S.K.; Marchant, C.; Haynes, D.R.; Bartold, P.M. Expression of peptidylarginine deiminase-2 and -4, citrullinated proteins and anti-citrullinated protein antibodies in human gingiva. J. Periodontal Res. 2013, 48, 252–261. [Google Scholar] [CrossRef]
- György, B.; Tóth, E.; Tarcsa, E.; Falus, A.; Buzás, E.I. Citrullination: A posttranslational modification in health and disease. Int. J. Biochem. Cell Biol. 2006, 38, 1662–1677. [Google Scholar] [CrossRef] [PubMed]
- Gabarrini, G.; De Smit, M.; Westra, J.; Brouwer, E.; Vissink, A.; Zhou, K.; Rossen, J.; Stobernack, T.; Van Dijl, J.M.; Van Winkelhoff, A.J. The peptidylarginine deiminase gene is a conserved feature of Porphyromonas gingivalis. Sci. Rep. 2015, 5, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Rahajoe, P.S.; De Smit, M.; Schuurmans, G.; Raveling-Eelsing, E.; Kertia, N.; Vissink, A.; Westra, J. Increased IgA anti-citrullinated protein antibodies in the periodontal inflammatory exudate of healthy individuals compared to rheumatoid arthritis patients. J. Clin. Periodontol. 2020, 47, 552–560. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Bañuelos, E.; Mukherjee, A.; Darrah, E.; Andrade, F. Rheumatoid Arthritis-Associated Mechanisms of Porphyromonas gingivalis and Aggregatibacter actinomycetemcomitans. J. Clin. Med. 2019, 8, 1309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Konig, M.F.; Abusleme, L.; Reinholdt, J.; Palmer, R.J.; Teles, R.P.; Sampson, K.; Rosen, A.; Nigrovic, P.A.; Sokolove, J.; Giles, J.T.; et al. Aggregatibacter actinomycetemcomitans-induced hypercitrullination links periodontal infection to autoimmunity in rheumatoid arthritis. Sci. Transl. Med. 2016, 8, ra176–ra369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Katma, M.K.; Bissada, N.F.; Bordeaux, J.M.; Sue, J.; Askari, A.D. Control of Periodontal Infection Reduces the Severity of Active Rheumatoid Arthritis. JCR J. Clin. Rheumatol. 2007, 13, 134–137. [Google Scholar] [CrossRef] [PubMed]
- Ortiz, P.; Bissada, N.; Palomo, L.; Han, Y.; Al-Zahrani, M.; Panneerselvam, A.; Askari, A. Periodontal Therapy Reduces the Severity of Active Rheumatoid Arthritis in Patients Treated With or Without Tumor Necrosis Factor Inhibitors. J. Periodontol. 2009, 80, 535–540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okada, M.; Kobayashi, T.; Ito, S.; Yokoyama, T.; Abe, A.; Murasawa, A.; Yoshie, H. Periodontal treatment decreases levels of antibodies to Porphyromonas gingivalis and citrulline in patients with rheumatoid arthritis and periodontitis. J. Periodontol. 2013, 84, e74–e84. [Google Scholar] [CrossRef] [PubMed]
- Białowąs, K.; Radwan-Oczko, M.; Duś-Ilnicka, I.; Korman, L.; Świerkot, J. Periodontal disease and influence of periodontal treatment on disease activity in patients with rheumatoid arthritis and spondyloarthritis. Rheumatol. Int. 2020, 40, 455–463. [Google Scholar] [CrossRef] [Green Version]
- Silva, D.S.; Costa, F.; Baptista, I.P.; Santiago, T.; Lund, H.; Tarp, S.; Silva, J.A.; Christensen, R. Evidence-based research on effectiveness of periodontal treatment in rheumatoid arthritis patients: A systematic review and meta-analysis. Arthritis Rheum. 2021. Online Ahead of Print. [Google Scholar] [CrossRef]
- Lopez-Olivo, M.A.; Kakpovbia-Eshareturi, V.; des Bordes, J.K.; Barbo, A.; Christensen, R.; Suarez-Almazor, M.E. Treating Early Undifferentiated Arthritis: A Systematic Review and Meta-Analysis of Direct and Indirect Trial Evidence. Arthritis Care Res. 2018, 70, 1355–1365. [Google Scholar] [CrossRef] [Green Version]
- Van der Helm-vanMil, A.H.; le Cessie, S.; van Dongen, H.; Breedveld, F.C.; Toes, R.E.; Huizinga, T.W. A prediction rule for disease outcome in patients with recent-onset undifferentiated arthritis: How to guide individual treatment decisions. Arthritis Rheum. 2007, 56, 433–440. [Google Scholar] [CrossRef]
- McNally, E.; Keogh, C.; Galvin, R.; Fahey, T. Diagnostic accuracy of a clinical prediction rule (CPR) for identifying patients with recent-onset undifferentiated arthritis who are at a high risk of developing rheumatoid arthritis: A systematic review and meta-analysis. Semin. Arthritis Rheum. 2014, 43, 498–507. [Google Scholar] [CrossRef]
- Bos, W.H.; Ursum, J.; de Vries, N.; Bartelds, G.M.; Wolbink, G.J.; Nurmohamed, M.T.; Van Der Horst-Bruinsma, I.E.; Van De Stadt, R.J.; Crusius, J.B.A.; Tak, P.P.; et al. The role of the shared epitope in arthralgia with anti-cyclic citrullinated peptide antibodies (anti-CCP), and its effect on anti-CCP levels. Ann. Rheum. Dis. 2008, 67, 1347–1350. [Google Scholar] [CrossRef] [PubMed]
- Rantapää-Dahlqvist, S.; De Jong, B.A.W.; Berglin, E.; Hallmans, G.; Wadell, G.; Stenlund, H.; Sundin, U.; Van Venrooij, W.J. Antibodies against cyclic citrullinated peptide and IgA rheumatoid factor predict the development of rheumatoid arthritis. Arthritis Rheum. 2003, 48, 2741–2749. [Google Scholar] [CrossRef]
- Frisell, T.; Holmqvist, M.; Källberg, H.; Klareskog, L.; Alfredsson, L.; Askling, J. Familial Risks and Heritability of Rheumatoid Arthritis: Role of Rheumatoid Factor/Anti-Citrullinated Protein Antibody Status, Number and Type of Affected Relatives, Sex, and Age. Arthritis Rheum. 2013, 65, 2773–2782. [Google Scholar] [CrossRef]
- Bos, W.H.; Wolbink, G.J.; Boers, M.; Tijhuis, G.J.; de Vries, N.; Van Der Horst-Bruinsma, I.E.; Tak, P.P.; Van De Stadt, R.J.; Van Der Laken, C.J.; Dijkmans, B.A.C.; et al. Arthritis development in patients with arthralgia is strongly associated with anti-citrullinated protein antibody status: A prospective cohort study. Ann. Rheum. Dis. 2009, 69, 490–494. [Google Scholar] [CrossRef]
- Rakieh, C.; Nam, J.L.; Hunt, L.; Hensor, E.; Das, S.; Bissell, L.-A.; Villeneuve, E.; McGonagle, D.; Hodgson, R.; Grainger, A.; et al. Predicting the development of clinical arthritis in anti-CCP positive individuals with non-specific musculoskeletal symptoms: A prospective observational cohort study. Ann. Rheum. Dis. 2015, 74, 1659–1666. [Google Scholar] [CrossRef] [PubMed]
- Di Matteo, A.; Mankia, K.; Duquenne, L.; Cipolletta, E.; Wakefield, R.J.; Garcia-Montoya, L.; Nam, J.L.; Emery, P. Ultrasound erosions in the feet best predict progression to inflammatory arthritis in anti-CCP positive at-risk individuals without clinical synovitis. Ann. Rheum. Dis. 2020, 79, 901–907. [Google Scholar] [CrossRef]
- Pumerantz, A.S.; Bissett, S.M.; Dong, F.; Ochoa, C.; Wassall, R.R.; Davila, H.; Barbee, M.; Nguyen, J.; Vila, P.; Preshaw, P.M. Standardized screening for periodontitis as an integral part of multidisciplinary management of adults with type 2 diabetes: An observational cross-sectional study of cohorts in the USA and UK. BMJ Open Diabetes Res. Care 2017, 5, e000413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carra, M.C.; Gueguen, A.; Thomas, F.; Pannier, B.; Caligiuri, G.; Steg, P.G.; Zins, M.; Bouchard, P. Self-report assessment of severe periodontitis: Periodontal screening score development. J. Clin. Periodontol. 2018, 45, 818–831. [Google Scholar] [CrossRef]
- Buhlin, K.; Gustafsson, A.; Andersson, K.; Håkansson, J.; Klinge, B. Validity and limitations of self-reported periodontal health. Community Dent. Oral Epidemiol. 2002, 30, 431–437. [Google Scholar] [CrossRef] [PubMed]
- Joshipura, K.J.; Douglass, C.W.; Garcia, R.I.; Valachovic, R.; Willett, W.C. Validity of self-reported periodontal measures. J. Public Health Dent. 1996, 56, 212. [Google Scholar] [CrossRef] [Green Version]
- Page, L.A.F.; Thomson, W.M.; Broadbent, J. Validity of self-reported periodontal questions in a New Zealand cohort. Clin. Oral Investig. 2016, 20, 563–569. [Google Scholar] [CrossRef]
- Abbood, H.M.; Hinz, J.; Cherukara, G.; Macfarlane, T.V. Validity of Self-Reported Periodontal Disease: A Systematic Review and Meta-Analysis. J. Periodontol. 2016, 87, 1474–1483. [Google Scholar] [CrossRef] [PubMed]
- Van Der Weijden, G.A.; Timmerman, M.F. A systematic review on the clinical efficacy of subgingival debridement in the treatment of chronic periodontitis. J. Clin. Periodontol. 2002, 29, 55–71. [Google Scholar] [CrossRef]
- Leite, F.R.M.; Nascimento, G.G.; Baake, S.; Pedersen, L.D.; Scheutz, F.; López, R. Impact of Smoking Cessation on Periodontitis: A Systematic Review and Meta-analysis of Prospective Longitudinal Observational and Interventional Studies. Nicotine Tob. Res. 2019, 21, 1600–1608. [Google Scholar] [CrossRef] [PubMed]
- Deane, K.D.; Demoruelle, M.K.; Kelmenson, L.B.; Kuhn, K.A.; Norris, J.M.; Holers, V.M. Genetic and environmental risk factors for rheumatoid arthritis. Best Pract. Res. Clin. Rheumatol. 2017, 31, 3–18. [Google Scholar] [CrossRef]
- Porter, M.E. A Strategy for Health Care Reform — Toward a Value-Based System. N. Engl. J. Med. 2009, 361, 109–112. [Google Scholar] [CrossRef] [Green Version]
- Anusha, D.; Chaly, P.E.; Junaid, M.; Nijesh, J.; Shivashankar, K.; Sivasamy, S. Efficacy of a mouthwash containing essential oils and curcumin as an adjunct to nonsurgical periodontal therapy among rheumatoid arthritis patients with chronic periodontitis: A randomized controlled trial. Indian J. Dent. Res. 2019, 30, 506. [Google Scholar] [CrossRef]
- Kaushal, S.; Singh, A.K.; Lal, N.; Das, S.K.; Mahdi, A.A. Effect of periodontal therapy on disease activity in patients of rheumatoid arthritis with chronic periodontitis. J. Oral Biol. Craniofacial Res. 2019, 9, 128–132. [Google Scholar] [CrossRef]
- Cosgarea, R.; Tristiu, R.; Dumitru, R.B.; Arweiler, N.B.; Rednic, S.; Sirbu, C.I.; Eick, S. Effects of non-surgical periodontal therapy on periodontal laboratory and clinical data as well as on disease activity in patients with rheumatoid arthritis. Clin. Oral Investig. 2019, 23, 141–151. [Google Scholar] [CrossRef] [PubMed]
- Pinho, M.D.N.; Oliveira, R.D.R.; Novaes, A.B., Jr.; Voltarelli, J.C. Relationship between periodontitis and rheumatoid arthritis and the effect of non-surgical periodontal treatment. Braz. Dent. J. 2009, 20, 355–364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kurgan, Ş.; Fentoglu, O.; Önder, C.; A Serdar, M.; Eser, F.; Tatakis, D.N.; Gunhan, M. The effects of periodontal therapy on gingival crevicular fluid matrix metalloproteinase-8, interleukin-6 and prostaglandin E2 levels in patients with rheumatoid arthritis. J. Periodontal Res. 2016, 51, 586–595. [Google Scholar] [CrossRef] [PubMed]
- Monsarrat, P.; de Grado, G.F.; Constantin, A.; Willmann, C.; Nabet, C.; Sixou, M.; Cantagrel, A.; Barnetche, T.; Mehsen-Cetre, N.; Schaeverbeke, T.; et al. The effect of periodontal treatment on patients with rheumatoid arthritis: The ESPERA randomised controlled trial. Jt. Bone Spine 2019, 86, 600–609. [Google Scholar] [CrossRef]
- Salliot, C.; Van Der Heijde, D. Long-term safety of methotrexate monotherapy in patients with rheumatoid arthritis: A systematic literature research. Ann. Rheum. Dis. 2008, 68, 1100–1104. [Google Scholar] [CrossRef] [Green Version]
- Mazaud, C.; Fardet, L. Relative risk of and determinants for adverse events of methotrexate prescribed at a low dose: A systematic review and meta-analysis of randomized placebo-controlled trials. Br. J. Dermatol. 2017, 177, 978–986. [Google Scholar] [CrossRef] [PubMed]
- Mosor, E.; Stoffer-Marx, M.; Steiner, G.; Raza, K.; Stack, R.J.; Simons, G.; Falahee, M.; Skingle, D.; Dobrin, M.; Schett, G.; et al. I Would Never Take Preventive Medication! Perspectives and Information Needs of People Who Underwent Predictive Tests for Rheumatoid Arthritis. Arthritis Rheum. 2020, 72, 360–368. [Google Scholar] [CrossRef] [Green Version]
- Sparks, J.A.; Iversen, M.D.; Yu, Z.; Triedman, N.A.; Prado, M.G.; Kroouze, R.M.; Kalia, S.S.; Atkinson, M.L.; Mody, E.A.; Helfgott, S.M.; et al. Disclosure of Personalized Rheumatoid Arthritis Risk Using Genetics, Biomarkers, and Lifestyle Factors to Motivate Health Behavior Improvements: A Randomized Controlled Trial. Arthritis Rheum. 2018, 70, 823–833. [Google Scholar] [CrossRef]
- Serban, S.; Dietrich, T.; Lopez-Oliva, I.; De Pablo, P.; Raza, K.; Filer, A.; Chapple, I.; Hill, K. Attitudes towards Oral Health in Patients with Rheumatoid Arthritis: A Qualitative Study Nested within a Randomized Controlled Trial. JDR Clin. Transl. Res. 2019, 4, 360–370. [Google Scholar] [CrossRef] [PubMed]
- Chambrone, L.; Preshaw, P.M.; Rosa, E.F.; Heasman, P.A.; Romito, G.A.; Pannuti, C.M.; Tu, Y.-K. Effects of smoking cessation on the outcomes of non-surgical periodontal therapy: A systematic review and individual patient data meta-analysis. J. Clin. Periodontol. 2013, 40, 607–615. [Google Scholar] [CrossRef]
- Liu, X.; Tedeschi, S.K.; Barbhaiya, M.; Leatherwood, C.L.; Speyer, C.B.; Lu, B.; Costenbader, K.H.; Karlson, E.W.; Sparks, J.A. Impact and Timing of Smoking Cessation on Reducing Risk of Rheumatoid Arthritis Among Women in the Nurses’ Health Studies. Arthritis Rheum. 2019, 71, 914–924. [Google Scholar] [CrossRef] [PubMed]
- Watt, R.G.; Serban, S. Multimorbidity: A challenge and opportunity for the dental profession. Br. Dent. J. 2020, 229, 282–286. [Google Scholar] [CrossRef] [PubMed]
- D’Aiuto, F.; Gkranias, N.; Bhowruth, D.; Khan, T.; Orlandi, M.; Suvan, J.; Masi, S.; Tsakos, G.; Hurel, S.; Hingorani, A.; et al. Systemic effects of periodontitis treatment in patients with type 2 diabetes: A 12 month, single-centre, investigator-masked, randomised trial. Lancet Diabetes Endocrinol. 2018, 6, 954–965. [Google Scholar] [CrossRef]
- Commissioning Standard: Dental Care for People with Diabetes. England.Nhs.Uk. 2019. Available online: https://www.england.nhs.uk/wp-content/uploads/2019/08/commissioning-standard-dental-care-for-people.pdf (accessed on 29 September 2021).
- Mustufvi, Z.; Barraclough, O.; Hearnshaw, S.; Whiston, S.; Grant, S.; Serban, S.; Douglas, G. Flexible Commissioning: A prevention and access focused approach in Yorkshire and the Humber. BDJ Pract. 2020, 33, 20–22. [Google Scholar] [CrossRef]
- Yonel, Z.; Cerullo, E.; Kröger, A.T.; Gray, L.J. Use of dental practices for the identification of adults with undiagnosed type 2 diabetes mellitus or non-diabetic hyperglycaemia: A systematic review. Diabet. Med. 2020, 37, 1443–1453. [Google Scholar] [CrossRef]
- Dental Checks: Intervals Between Oral Health Reviews. 2004. Available online: https://www.nice.org.uk/guidanchttps://www.nice.org.uk/guidance/cg19e/cg19 (accessed on 29 September 2021).

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mustufvi, Z.; Serban, S.; Chesterman, J.; Mankia, K. Should We Be Screening for and Treating Periodontal Disease in Individuals Who Are at Risk of Rheumatoid Arthritis? Healthcare 2021, 9, 1326. https://doi.org/10.3390/healthcare9101326
Mustufvi Z, Serban S, Chesterman J, Mankia K. Should We Be Screening for and Treating Periodontal Disease in Individuals Who Are at Risk of Rheumatoid Arthritis? Healthcare. 2021; 9(10):1326. https://doi.org/10.3390/healthcare9101326
Chicago/Turabian StyleMustufvi, Zhain, Stefan Serban, James Chesterman, and Kulveer Mankia. 2021. "Should We Be Screening for and Treating Periodontal Disease in Individuals Who Are at Risk of Rheumatoid Arthritis?" Healthcare 9, no. 10: 1326. https://doi.org/10.3390/healthcare9101326
APA StyleMustufvi, Z., Serban, S., Chesterman, J., & Mankia, K. (2021). Should We Be Screening for and Treating Periodontal Disease in Individuals Who Are at Risk of Rheumatoid Arthritis? Healthcare, 9(10), 1326. https://doi.org/10.3390/healthcare9101326