
A School-Based Progressive Muscle Relaxation Program for Female Adolescents: Development and the Effectiveness on Physiological and Psychological Evidence


Abstract
1. Introduction
2. Materials and Methods
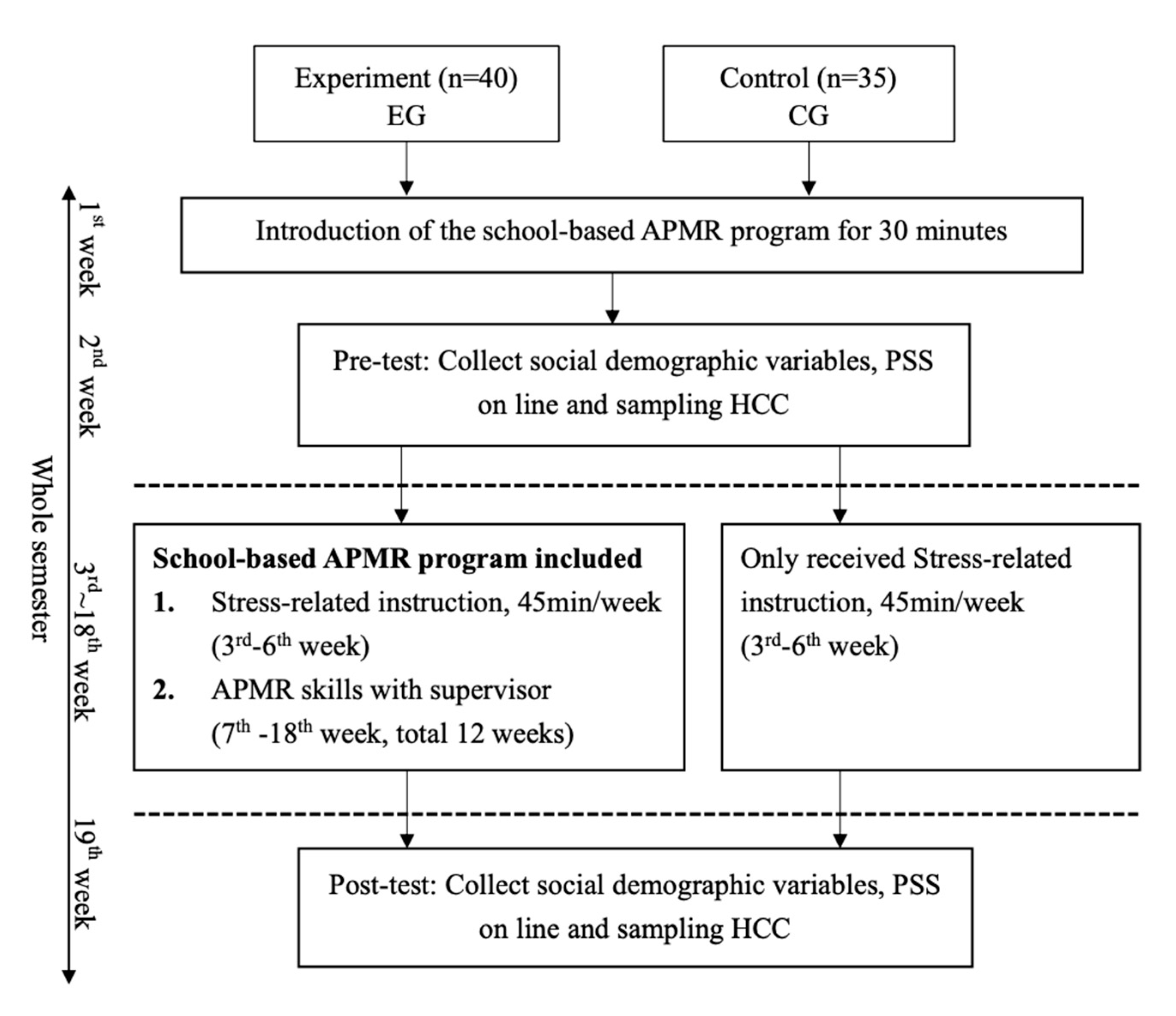
2.1. Design
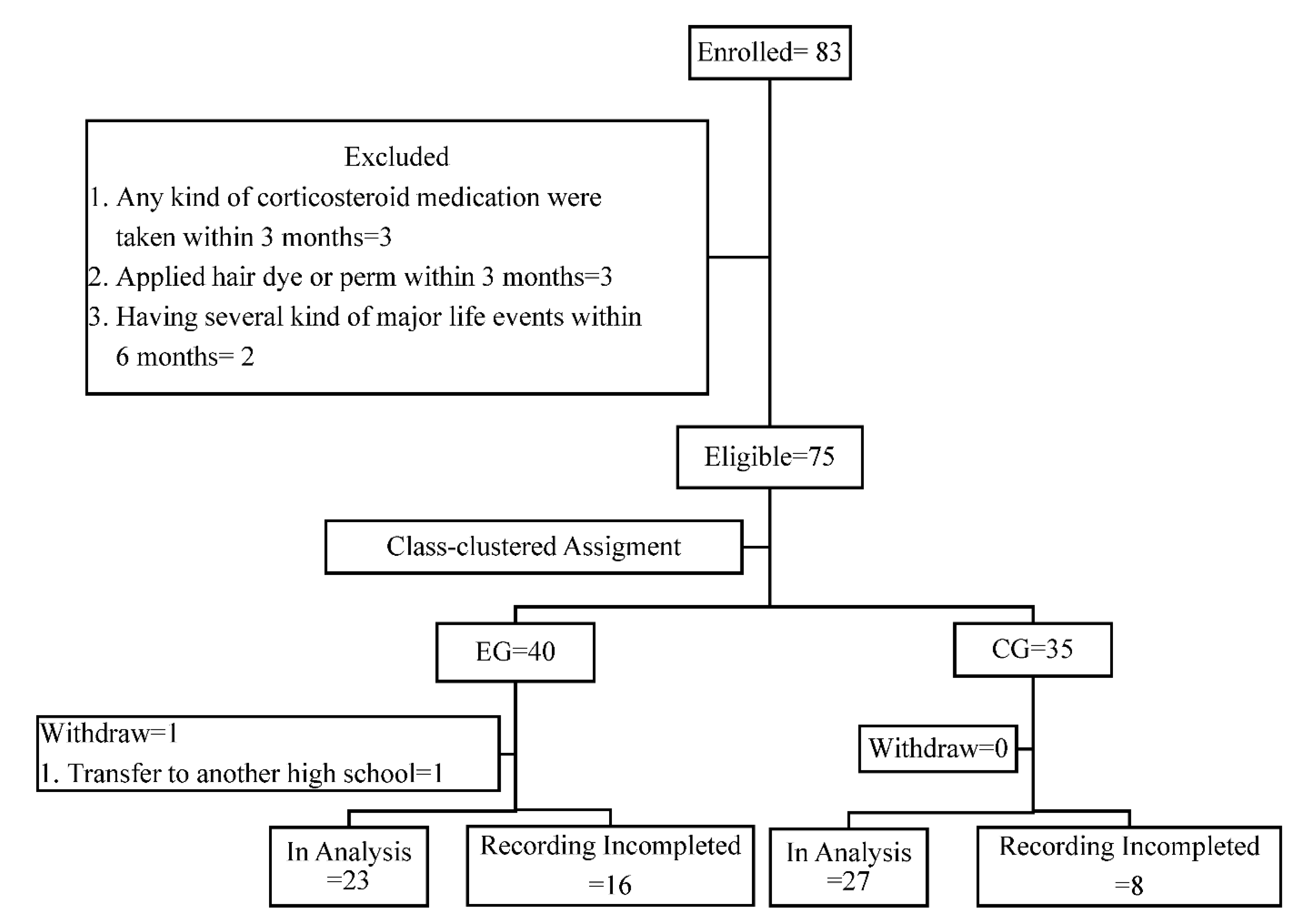
2.2. Setting and Sample
2.3. Ethical Considerations
2.4. Partnership Team for Program Development
2.5. The School-Based APMR Program
2.5.1. Stress-Related Knowledge Education
2.5.2. Techniques for APMR Practice
2.6. Evaluation of Program Feasibility
2.7. Evaluation of APMR Effects
2.7.1. Perceived Stress Scale
2.7.2. Visual Analog Scales of Relaxation Rating
2.7.3. Hair Cortisol Sample Collection and Analysis
2.8. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ali, N.M.; Nowshad, N.A.; Mansoor, K.M.; Ibnouf, R.A.; Albehiery, R.M.; Carrick, F.R.; Abdulrahman, M. Perceived academic and psychological stress among adolescents in United Arab Emirates: Role of gender, age, depression, and high expectation of parents. Psychiatr. Danub. 2019, 31, 331–337. [Google Scholar] [PubMed]
- Oduwaiye, R.O.; Yahaya, L.A.; Amadi, E.C.; Tiamiyu, K.A. Stress level and academic performance of university students in Kwara State, Nigeria. Mak. J. High Educ. 2017, 9, 103–112. [Google Scholar] [CrossRef]
- Park, S.U.; Kim, M.K. Effects of campus life stress, stress coping type, self-esteem, and maladjustment perfectionism on suicide ideation among college students. Korean J. Clin. Lab. Sci. 2018, 50, 63–70. [Google Scholar] [CrossRef][Green Version]
- Steptoe, A.; Kivimäki, M. Stress and cardiovascular disease: An update on current knowledge. Annu. Rev. Public Health 2013, 34, 337–354. [Google Scholar] [CrossRef]
- King, K.M.; Molina, B.S.; Chassin, L. Prospective relations between growth in drinking and familial stressors across adolescence. J. Abnorm. Psychol. 2009, 118, 610. [Google Scholar] [CrossRef]
- Roemmich, J.N.; Lambiase, M.J.; Balantekin, K.N.; Feda, D.M.; Dorn, J. Stress, behavior, and biology: Risk factors for cardiovascular diseases in youth. Exerc. Sport Sci. Rev. 2014, 42, 145–152. [Google Scholar] [CrossRef]
- Karatoreos, I.N.; McEwen, B.S. Annual research review: The neurobiology and physiology of resilience and adaptation across the life course. J. Child Psychol. Psychiatry 2013, 54, 337–347. [Google Scholar] [CrossRef] [PubMed]
- Schubert, K.O.; Clark, S.R.; Van, L.K.; Collinson, J.L.; Baune, B.T. Depressive symptom trajectories in late adolescence and early adulthood: A systematic review. Aust. N. Z. J. Psychiatry 2017, 51, 477–499. [Google Scholar] [CrossRef]
- Manjushambika, R.; Prasanna, B.; Vijayaraghavan, R.; Sushama, B. Effectiveness of Jacobson’s Progressive Muscle Relaxation (JPMR) on educational stress among school going adolescents. Int. J. Nurs. Educ. 2017, 9, 110–115. [Google Scholar] [CrossRef]
- Fredrickson, B.L.; Boulton, A.J.; Firestine, A.M.; Van Cappellen, P.; Algoe, S.B.; Brantley, M.M.; Kim, S.L.; Brantley, J.; Salzberg, S. Positive emotion correlates of meditation practice: A comparison of mindfulness meditation and loving-kindness meditation. Mindfulness 2017, 8, 1623–1633. [Google Scholar] [CrossRef]
- Yang, J.; Tang, S.; Zhou, W. Effect of mindfulness-based stress reduction therapy on work stress and mental health of psychiatric nurses. Psychiatr. Danub. 2018, 30, 189–196. [Google Scholar] [CrossRef]
- Conley, C.S.; Durlak, J.A.; Kirsch, A.C. A meta-analysis of universal mental health prevention programs for higher education students. Prev. Sci. 2015, 16, 487–507. [Google Scholar] [CrossRef]
- Baer, R.; Crane, C.; Miller, E.; Kuyken, W. Doing no harm in mindfulness-based programs: Conceptual issues and empirical findings. Clin. Psychol. Rev. 2019, 71, 101–114. [Google Scholar] [CrossRef]
- Jacobson, E. Progressive relaxation. Am. J. Psychol. 1987, 100, 522–537. [Google Scholar] [CrossRef]
- Sharifah Maimunah, S.M.P.; Hashim, H.A. Differential effects of 7 and 16 groups of muscle relaxation training following repeated submaximal intensity exercise in young football players. Percept. Mot. Ski. 2016, 122, 227–237. [Google Scholar] [CrossRef] [PubMed]
- Conley, C.S.; Shapiro, J.B.; Kirsch, A.C.; Durlak, J.A. A meta-analysis of indicated mental health prevention programs for at-risk higher education students. J. Couns. Psychol. 2017, 64, 121. [Google Scholar] [CrossRef]
- Chellew, K.; Evans, P.; Fornes-Vives, J.; Perez, G.; Garcia-Banda, G. The effect of progressive muscle relaxation on daily cortisol secretion. Stress 2015, 18, 538–544. [Google Scholar] [CrossRef]
- Pawlow, L.A.; Jones, G.E. The impact of abbreviated progressive muscle relaxation on salivary cortisol and salivary immunoglobulin A (sIgA). Appl. Psychophysiol. Biofeedback 2005, 30, 375–387. [Google Scholar] [CrossRef] [PubMed]
- Nickel, C.; Lahmann, C.; Tritt, K.; Loew, T.H.; Rother, W.K.; Nickel, M.K. Stressed aggressive adolescents benefit from progressive muscle relaxation: A random, prospective, controlled trial. Stress Health 2005, 21, 169–175. [Google Scholar] [CrossRef]
- Oken, B.S.; Chamine, I.; Wakeland, W. A systems approach to stress, stressors and resilience in humans. Behav. Brain Res. 2015, 282, 144–154. [Google Scholar] [CrossRef]
- Gjerstad, J.K.; Lightman, S.L.; Spiga, F. Role of glucocorticoid negative feedback in the regulation of HPA axis pulsatility. Stress 2018, 21, 403–416. [Google Scholar] [CrossRef]
- Lupien, S.J.; McEwen, B.S.; Gunnar, M.R.; Heim, C. Effects of stress throughout the lifespan on the brain, behaviour and cognition. Nat. Rev. Neurol. 2009, 10, 434–445. [Google Scholar] [CrossRef]
- Shirtcliff, E.A.; Essex, M.J. Concurrent and longitudinal associations of basal and diurnal cortisol with mental health symptoms in early adolescence. Dev. Psychobiol. 2008, 50, 690–703. [Google Scholar] [CrossRef]
- Stalder, T.; Steudte-Schmiedgen, S.; Alexander, N.; Klucken, T.; Vater, A.; Wichmann, S.; Kirschbaum, C.; Miller, R. Stress-related and basic determinants of hair cortisol in humans: A meta-analysis. Psychoneuroendocrino 2017, 77, 261–274. [Google Scholar] [CrossRef] [PubMed]
- Iglesias, S.L.; Jacobsen, D.; Gonzalez, D.; Azzara, S.; Repetto, E.M.; Jamardo, J.; Gómez, S.G.; Mesch, V.; Berg, G.; Fabre, B. Hair cortisol: A new tool for evaluating stress in programs of stress management. Life Sci. 2015, 141, 188–192. [Google Scholar] [CrossRef]
- Wosu, A.C.; Valdimarsdóttir, U.; Shields, A.E.; Williams, D.R.; Williams, M.A. Correlates of cortisol in human hair: Implications for epidemiologic studies on health effects of chronic stress. Ann. Epidemiol. 2013, 23, 797–811. [Google Scholar] [CrossRef] [PubMed]
- Gerber, M.; Kalak, N.; Lemola, S.; Clough, P.J.; Perry, J.L.; Pühse, U.; Elliot, C.; Holsboer-Trachsler, E.; Brand, S. Are adolescents with high mental toughness levels more resilient against stress? Stress Health 2013, 29, 164–171. [Google Scholar] [CrossRef] [PubMed]
- Dajani, R.; Hadfield, K.; van Uum, S.; Greff, M.; Panter-Brick, C. Hair cortisol concentrations in war-affected adolescents: A prospective intervention trial. Psychoneuroendocrinology 2018, 89, 138–146. [Google Scholar] [CrossRef] [PubMed]
- Groeneveld, M.G.; Savas, M.; van Rossum, E.F.; Vermeer, H.J. Children’s hair cortisol as a biomarker of stress at school: A follow-up study. Stress 2020, 23, 590–596. [Google Scholar] [CrossRef]
- Garcia, C.; Pintor, J.K.; Lindgren, S. Feasibility and acceptability of a school-based coping intervention for Latina adolescents. J. Sch. Nurs. 2010, 26, 42–52. [Google Scholar] [CrossRef]
- Karlén, J.; Ludvigsson, J.; Frostell, A.; Theodorsson, E.; Faresjö, T. Cortisol in hair measured in young adults—A biomarker of major life stressors? BMC Clin. Pathol. 2011, 11, 12. [Google Scholar] [CrossRef]
- Kuyken, W.; Weare, K.; Ukoumunne, O.C.; Vicary, R.; Motton, N.; Burnett, R. Effectiveness of the Mindfulness in Schools Programme: Non-randomised controlled feasibility study. Br. J. Psychiatry 2013, 203, 126–131. [Google Scholar] [CrossRef] [PubMed]
- Neil-Sztramko, S.; Gotay, C.; Sabiston, C.; Demers, P.; Campbell, K. Feasibility of a telephone and web-based physical activity intervention for women shift workers. Transl. Behav. Med. 2017, 7, 268–276. [Google Scholar] [CrossRef]
- Thabane, L.; Ma, J.; Chu, R.; Cheng, J.; Ismaila, A.; Rios, L.P.; Robson, R.; Thabane, M.; Giangregorio, L.; Goldsmith, C.H. A tutorial on pilot studies: The what, why and how. BMC Med. Res. Methodol. 2010, 10, 1. [Google Scholar] [CrossRef] [PubMed]
- Leung, D.Y.; Lam, T.H.; Chan, S.C. Three versions of perceived stress scale: Validation in a sample of Chinese cardiac patients who smoke. BMC Public Health 2015, 10, 513–519. [Google Scholar] [CrossRef]
- Bijur, P.E.; Silver, W.; Gallagher, E.J. Reliability of the visual analog scale for measurement of acute pain. Acad Emerg. Med. 2001, 8, 1153–1157. [Google Scholar] [CrossRef] [PubMed]
- Nagata, C.; Ido, M.; Shimizu, H.; Misao, A.; Matsuura, H. Choice of response scale for health measurement: Comparison of 4, 5, and 7-point scales and visual analog scale. J Epidemiol. 1996, 6, 192–197. [Google Scholar] [CrossRef]
- Davenport, M.D.; Tiefenbacher, S.; Lutz, C.K.; Novak, M.A.; Meyer, J.S. Analysis of endogenous cortisol concentrations in the hair of rhesus macaques. Gen. Comp. Endocrinol. 2006, 147, 255–261. [Google Scholar] [CrossRef]
- Dettenborn, L.; Tietze, A.; Bruckner, F.; Kirschbaum, C. Higher cortisol content in hair among long-term unemployed individuals compared to controls. Psychoneuroendocrino 2010, 35, 1404–1409. [Google Scholar] [CrossRef]
- Porter, S.; McConnell, T.; McLaughlin, K.; Lynn, F.; Cardwell, C.; Braiden, H.-J.; Boylan, J.; Holmes, V. Music therapy for children and adolescents with behavioural and emotional problems: A randomised controlled trial. J. Child Psychol. Psychiatry 2017, 58, 586–594. [Google Scholar] [CrossRef]
- Sauvé, B.; Koren, G.; Walsh, G.; Tokmakejian, S.; Van Uum, S.H. Measurement of cortisol in human hair as a biomarker of systemic exposure. Clin. Invest. Med. 2007, 30, E183–E191. [Google Scholar] [CrossRef]
- Dimou, P.; Bacopoulou, F.; Darviri, C.; Chrousos, G. Stress management and sexual health of young adults: A pilot randomised controlled trial. Andrologia 2014, 46, 1022–1031. [Google Scholar] [CrossRef]
- Sivo, S.A.; Saunders, C.; Chang, Q.; Jiang, J.J. How low should you go? Low response rates and the validity of inference in is questionnaire research. J. Assoc. Inf. Syst. 2006, 7, 351–414. [Google Scholar] [CrossRef]
- Short, S.J.; Stalder, T.; Marceau, K.; Entringer, S.; Moog, N.K.; Shirtcliff, E.A. Correspondence between hair cortisol concentrations and 30-day integrated daily salivary and weekly urinary cortisol measures. Psychoneuroendocrinology 2016, 71, 12–18. [Google Scholar] [CrossRef]
- Agorastos, A.; Pervanidou, P.; Chrousos, G.P.; Kolaitis, G. Early life stress and trauma: Developmental neuroendocrine aspects of prolonged stress system dysregulation. Hormones 2018, 17, 507–520. [Google Scholar] [CrossRef] [PubMed]
- Chrousos, G.P. Stress and disorders of the stress system. Nat. Rev. Endocrinol. 2009, 5, 374. [Google Scholar] [CrossRef] [PubMed]
- Herman, J.P.; McKlveen, J.M.; Ghosal, S.; Kopp, B.; Wulsin, A.; Makinson, R.; Scheimann, J.; Myers, B. Regulation of the hypothalamic-pituitary-adrenocortical stress response. Compr. Physiol. 2011, 6, 603–621. [Google Scholar] [CrossRef]
- Joseph, D.N.; Whirledge, S. Stress and the HPA axis: Balancing homeostasis and fertility. Int. J. Mol. Sci. 2017, 18, 2224. [Google Scholar] [CrossRef] [PubMed]
- Burford, N.G.; Webster, N.A.; Cruz-Topete, D. Hypothalamic-pituitary-adrenal axis modulation of glucocorticoids in the cardiovascular system. Int. J. Mol. Sci. 2017, 18, 2150. [Google Scholar] [CrossRef]
- Tsiouli, E.; Pavlopoulos, V.; Alexopoulos, E.C.; Chrousos, G.; Darviri, C. Short-term impact of a stress management and health promotion program on perceived stress, parental stress, health locus of control, and cortisol levels in parents of children and adolescents with diabetes type 1: A pilot randomized controlled trial. Explore 2014, 10, 88–98. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Control Group (n = 27) | Experimental Group (n = 23) |
|---|---|---|
| Mean (SD) | ||
| Body Height (cm) | 159.8 (5.7) | 162.5 (5.4) |
| Body Weight (kg) | 55.9 (11.3) | 56 (10.5) |
| Body Mass Index (kg/m2) | 21.8 (3.9) | 21.2 (3.7) |
| Measurements | ||
| Perceived Stress Scale | 29.3 (7.4) | 27.9 (6.1) |
| Log Hair Cortisol Concentration (pg/mg) | 1.9 (0.5) | 1.8 (0.5) |
| Variables | Groups | Mean (95% Confidence Interval) | Within p Value | Between p Value | Partial Eta Squared | |
|---|---|---|---|---|---|---|
| Pre-Test | Post-Test | |||||
| Perceived Stress Scale | E | 27.9 (15.9~39.8) | 25.1 (5.4~44.8) | 0.91 | 0.59 | 0.01 |
| C | 29.3 (14.7~43.9) | 27.6 (9.3~45.8) | 0.22 | |||
| Log Hair Cortisol Concentration | E | 1.9 (0.9~2.8) | 1.8 (0.9~2.7) | 0.64 | 0.02 * | 0.12 |
| C | 1.7 (0.7~2.7) | 1.4 (0.2~2.5) | 0.001 *** | |||
| Visual Analog Scales of Relaxation Rating | E | 2.1 (0.6~3.6) | 3.3 (1.5~3.3) | <0.001 *** | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsai, M.-L.; Cheng, T.-H.; Yang, Y.-K.; Wang, C.-J. A School-Based Progressive Muscle Relaxation Program for Female Adolescents: Development and the Effectiveness on Physiological and Psychological Evidence. Healthcare 2021, 9, 1319. https://doi.org/10.3390/healthcare9101319
Tsai M-L, Cheng T-H, Yang Y-K, Wang C-J. A School-Based Progressive Muscle Relaxation Program for Female Adolescents: Development and the Effectiveness on Physiological and Psychological Evidence. Healthcare. 2021; 9(10):1319. https://doi.org/10.3390/healthcare9101319
Chicago/Turabian StyleTsai, Mei-Li, Tsan-Hwang Cheng, Yen-Kuang Yang, and Chi-Jane Wang. 2021. "A School-Based Progressive Muscle Relaxation Program for Female Adolescents: Development and the Effectiveness on Physiological and Psychological Evidence" Healthcare 9, no. 10: 1319. https://doi.org/10.3390/healthcare9101319
APA StyleTsai, M.-L., Cheng, T.-H., Yang, Y.-K., & Wang, C.-J. (2021). A School-Based Progressive Muscle Relaxation Program for Female Adolescents: Development and the Effectiveness on Physiological and Psychological Evidence. Healthcare, 9(10), 1319. https://doi.org/10.3390/healthcare9101319