Predictors of Health-Related Quality of Life among Healthcare Workers in the Context of Health System Strengthening in Kenya


Abstract
1. Introduction
- What is the average overall self-assessed health status of the healthcare workers?
- Is there a statistically significant difference between healthcare workers’ overall self-assessed health status and hospital ownership?
- What is the statistically significant relationship between healthcare workers’ overall self-assessed health status and personal, job-related, and work environment characteristics?
2. Materials and Methods
2.1. Study Design
2.2. Study Setting
2.3. Study Population and Sample
2.4. Data Collection
2.4.1. Sample Characteristics
2.4.2. The EQ-5D-5L
2.4.3. Statistical Analysis
2.5. Ethical Considerations
3. Results
3.1. Sample Characteristics
3.2. Work Environment Characteristics
3.3. EQ-5D-5L Health Profile, Index Value and EQ-VAS
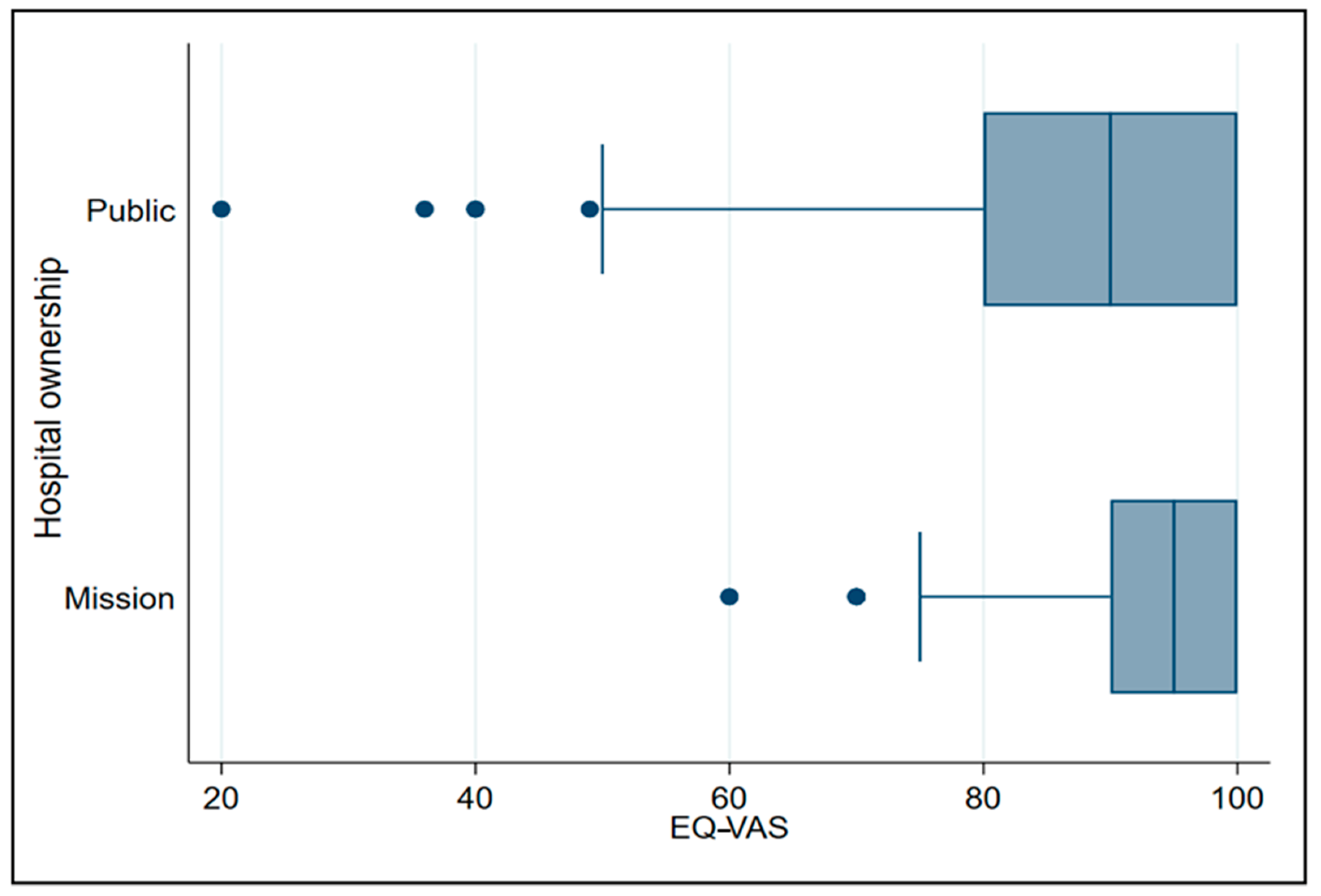
3.4. Overall Self-Reported Health Status by Hospital Ownership
3.5. Predictors of Overall Health Status
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- United Nations. Transforming Our World: The 2030 Agenda for Sustainable Development; A/RES/70/1; UN: New York, NY, USA, 2015. [Google Scholar]
- World Health Assembly. Global Strategy on Human Resources for Health: Workforce 2030; WHA69.19; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- World Health Organization. A Universal Truth: No Health Without a Workforce; WHO: Geneva, Switzerland, 2013. [Google Scholar]
- World Health Organization. Working Together for Health; The World Health Report 2006: Policy Briefs; WHO: Geneva, Switzerland, 2006. [Google Scholar]
- World Health Organization. World Health Statistics 2019: Monitoring Health for the Sustainable Development Goals; WHO: Geneva, Switzerland, 2019. [Google Scholar]
- Mumbo, H.M.; Were, S.O.; Murianki, C.A.; Mutuku, M.P.; Mutwiwa, S.N. The implication of the shortage of health workforce specialist on universal health coverage in Kenya. Hum. Resour. Health 2017, 15, 80. [Google Scholar] [CrossRef]
- Hongoro, C.; McPake, B. How to bridge the gap in human resources for health. Lancet 2004, 364, 1451–1456. [Google Scholar] [CrossRef]
- Kirigia, J.; Gbary, A.; Nyoni, J.; Seddoh, A.; Muthuri, L. The cost of health-related brain drain to the WHO African Region. Afr. J. Health Sci. 2008, 13. [Google Scholar] [CrossRef]
- World Health Organization Regional Committee for Africa. Migration of Health Personnel: Code of Practice for International Recruitment of Health Workers; AFR/RC59/R6; World Health Organization Regional Committee for Africa: Brazzaville, Congo, 2009. [Google Scholar]
- Ministry of Health. Kenya Health Policy 2014–2030; Government of Kenya: Nairobi, Kenya, 2014.
- Ministry of Health. Kenya Health Workforce Report: The Status of Healthcare Professionals in Kenya, 2015; Ministry of Health, Government of Kenya: Nairobi, Kenya, 2015.
- Kiambati, H.; Kiio, C.; Toweett, J. Understanding the Labour Market and Productivity of Human Resources for Health: Country Report Kenya; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Waithaka, D.; Kagwanja, N.; Nzinga, J.; Tsofa, B.; Leli, H.; Mataza, C.; Nyaguara, A.; Bejon, P.; Gilson, L.; Barasa, E.W.; et al. Prolonged health worker strikes in Kenya—Perspectives and experiences of frontline health managers and local communities in Kilifi County. Int. J. Equity Health 2020, 19, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Irimu, G.; Ogero, M.; Mbevi, G.; Kariuki, C.; Gathara, D.; Akech, S.; Barasa, E.; Tsofa, B.; English, M. Tackling health professionals’ strikes: An essential part of health system strengthening in Kenya. BMJ Glob. Health 2018, 3, e001136. [Google Scholar] [CrossRef] [PubMed]
- Njuguna, J. Impact of Health Workers’ Strike in August 2014 on Health Services in Mombasa County Referral Hospital, Kenya. J. Health Care Poor Underserved 2015, 26, 1200–1206. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Regional Committee for Africa. Road Map for Scaling Up the Human Resources for Health for Improved Health Service Delivery in the African Region 2012–2025; World Health Organization Regional Committee for Africa: Luanda, Angola, 2012. [Google Scholar]
- World Health Organization. Global Strategy on Human Resources for Health: Workforce 2030; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- World Health Assembly. Follow-Up of the Recife Political Declaration on Human Resources for Health: Renewed Commitments towards Universal Health Coverage; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Government of Kenya. The Constitution of Kenya; Government of Kenya: Nairobi, Kenya, 2010. [Google Scholar]
- EuroQol Group. EuroQol—A new facility for the measurement of health-related quality of life. Health Policy 1990, 16, 199–208. [Google Scholar] [CrossRef]
- World Health Organization. Everybody’s Business: Strengthening Health Systems to Improve Health Outcomes; WHO: Geneva, Switzerland, 2007. [Google Scholar]
- World Health Organization. Constitution of the World Health Organization; WHO: Geneva, Switzerland, 2006. [Google Scholar]
- Kirigia, J. Health impacts of epidemiological environment change: Measurement issues. Environ. Dev. Econ. 1996, 1, 359–367. [Google Scholar] [CrossRef]
- Karimi, M.; Brazier, J. Health, Health-Related Quality of Life, and Quality of Life: What is the Difference? PharmacoEconomics 2016, 34, 645–649. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, C.M.; Benatti, M.C.C.; Rodrigues, R.C.M. Occupational accidents and health-related quality of life: A study in three hospitals. Rev. Lat. Am. Enferm. 2009, 17, 101–107. [Google Scholar] [CrossRef][Green Version]
- Wu, S.-Y.; Li, H.-Y.; Tian, J.; Zhu, W.; Li, J.; Wang, X.-R. Health-related Quality of Life and Its Main Related Factors among Nurses in China. Ind. Health 2011, 49, 158–165. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, M. Health-related quality of life among healthcare providers in Pakistan. J. Pharm. Bioallied Sci. 2020. [Google Scholar] [CrossRef]
- Munguti, N.D.; Kirigia, J.M. Human resources health related quality of life: A case study of Groot Schuur Hospital in South Africa. Afr. J. Health Sci. 2007, 5, 185–189. [Google Scholar]
- Tountas, Y.; Demakakos, P.; Yfantopoulos, Y.; Aga, J.; Houliara, L.; Pavi, E. The health related quality of life of the employees in the Greek hospitals: Assessing how healthy are the health workers. Health Qual. Life Outcomes 2003, 1, 61. [Google Scholar] [CrossRef]
- Terer, C.C.; Bustinduy, A.L.; Magtanong, R.V.; Muhoho, N.; Mungai, P.L.; Muchiri, E.M.; Kitron, U.; King, C.H.; Mutuku, F.M. Evaluation of the Health-related Quality of Life of Children in Schistosoma haematobium-endemic Communities in Kenya: A Cross-sectional Study. PLoS Negl. Trop. Dis. 2013, 7, e2106. [Google Scholar] [CrossRef]
- Kirigia, J.M. Economic evaluation in schistosomiasis: Valuation of health states preferences: A research note. Health Econ. 1998, 7, 551–556. [Google Scholar] [CrossRef]
- Winter, S.; Obara, L.M.; Barchi, F. Environmental Correlates of Health-Related Quality of Life among Women Living in Informal Settlements in Kenya. Int. J. Environ. Res. Public Health 2019, 16, 3948. [Google Scholar] [CrossRef]
- Nyongesa, M.K.; Mwangi, P.; Wanjala, S.W.; Mutua, A.M.; Koot, H.M.; Cuijpers, P.; Newton, C.R.J.C.; Abubakar, A. Correlates of health-related quality of life among adults receiving combination antiretroviral therapy in coastal Kenya. Heal. Qual. Life Outcomes 2020, 18, 169. [Google Scholar] [CrossRef]
- Van Der Kop, M.L.; Muhula, S.; Patel, A.; Thabane, L.; Awiti, P.; Kyomuhangi, L.; Abunah, B.; Nagide, P.I.; Smillie, K.; Ojakaa, D.I.; et al. Gender differences in health-related quality of life at the time of a positive HIV test—A cross-sectional study in a resource-poor, high prevalence setting in Nairobi, Kenya. AIDS Care 2017, 30, 493–499. [Google Scholar] [CrossRef]
- Mûnene, E.; Ekman, B. Does duration on antiretroviral therapy determine health-related quality of life in people living with HIV? A cross-sectional study in a regional referral hospital in Kenya. Glob. Health Action 2014, 7, 23554. [Google Scholar] [CrossRef]
- Kamau, E.; Kayima, J.; Otieno, C.F. The determinants of health related quality of life of patients on maintenance hae-modialysis at Kenyatta National Hospital, Kenya. East Afr. Med. J. 2014, 91, 368–374. [Google Scholar] [PubMed]
- Polack, S.; Eusebio, C.; Mathenge, W.; Wadud, Z.; Mamunur, A.; Fletcher, A.; Foster, A.; Kuper, H. The Impact of Cataract Surgery on Health Related Quality of Life in Kenya, the Philippines, and Bangladesh. Ophthalmic Epidemiol. 2010, 17, 387–399. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health. COVID-19 Outbreak in Kenya: Daily Situation Report—132; Ministry of Health, Government of Kenya: Nairobi, Kenya, 2020.
- Ng, Q.X.; De Deyn, M.L.Z.Q.; Lim, D.Y.; Chan, H.W.; Yeo, W.S. The wounded healer: A narrative review of the mental health effects of the COVID-19 pandemic on healthcare workers. Asian J. Psychiatry 2020, 54, 102258. [Google Scholar] [CrossRef] [PubMed]
- The County Government of Meru. Meru County Integrated Development Plan 2018–2022; The County Government of Meru: Meru, Kenya, 2018; p. 337.
- World Health Organization. Transforming and Scaling Up Health Professionals’ Education and Training; World Health Organization Guidelines 2013; WHO: Geneva, Switzerland, 2013. [Google Scholar]
- The Survey System. Sample Size Calculator. Available online: https://www.surveysystem.com/sscalc.htm (accessed on 18 June 2019).
- EuroQol Research Foundation. EQ-5D-5L User Guide; EuroQol Research Foundation: Rotterdam, The Netherlands, 2019. [Google Scholar]
- Studenmund, A.H.; Cassidy, H.J. Using Econometrics: A Practical Guide; Harper Collins Publishers: New York, NY, USA, 1992. [Google Scholar]
- Cho, S.; Lee, H.; Oh, E.G.; Kim, G.S.; Kim, Y.-C.; Park, C. Health-related quality of life among migrant workers: The impact of health-promoting behaviors. Nurs. Health Sci. 2019, 22, 318–327. [Google Scholar] [CrossRef]
- United Nations Economic Commission for Europe. Commitment 5 of the UNECE Strategy on Ageing: To Enable Labour Markets to Respond to the Economic and Social Consequences of Population Ageing; United Nations Economic Commission for Europe (UNECE): Geneva, Switzerland, 2011. [Google Scholar]
- Marmot, M. The Influence of Income on Health: Views of an Epidemiologist. Health Aff. 2002, 21, 31–46. [Google Scholar] [CrossRef]
- World Bank. World Development Indicators. Available online: https://data.worldbank.org/indicator/SP.POP.DPND?locations=KE (accessed on 2 November 2020).
- Subramanian, S.V. Income Inequality and Health: What Have We Learned So Far? Epidemiol. Rev. 2004, 26, 78–91. [Google Scholar] [CrossRef]
- World Bank. Kenya Economic Update, April 2020: Turbulent Times for Growth in Kenya—Policy Options during the COVID-19 Pandemic; World Bank: Washington, DC, USA, 2020. [Google Scholar]
- Guler, N.; Kuzu, F. The Health-Related Quality of Life of the Health Professionals Working in the Primary Healthcare Centers and Its Correlation with Selected Sociodemographic Factors in Sivas, a Central Anatolian City. Sci. Res. Essays 2009, 4, 1547–1552. [Google Scholar]
- Kheiraoui, F.; Gualano, M.R.; Mannocci, A.; Boccia, A.; La Torre, G. Quality of life among healthcare workers: A multicentre cross-sectional study in Italy. Public Health 2012, 126, 624–629. [Google Scholar] [CrossRef]
- World Haalth Organization. Universal Health Coverage and Ageing. Available online: https://www.who.int/ageing/health-systems/uhc-ageing/en/ (accessed on 21 December 2020).
- Dieleman, M.; Harnmeijer, J.W. Improving Health Worker Performance: In Search of Promising Practices; WHO: Geneva, Switzerland, 2006. [Google Scholar]
- Weinberg, D.B.; Avgar, A.C.; Sugrue, N.M.; Cooney-Miner, D. The Importance of a High-Performance Work Environment in Hospitals. Health Serv. Res. 2012, 48, 319–332. [Google Scholar] [CrossRef]
- Herzberg, F. One More Time: How Do You Motivate Employees? Harv. Bus. Rev. 2003, 81, 87–96. [Google Scholar]
- Alshmemri, M.; Shahwan-Akl, L.; Maude, P. Herzberg’s two-factor theory. Life Sci. J. 2017, 14, 12–16. [Google Scholar]


{kind=link}
| Personal and Job-Related Variables | Overall (n = 553) n (%) | Public Hospitals (n = 434) n (%) | Mission Hospitals (n = 119) n (%) |
|---|---|---|---|
| Sex | |||
| Male | 214 (38.70) | 180 (41.47) | 34 (28.57) |
| Female | 339 (61.30) | 254 (58.53) | 85 (71.43) |
| Age | |||
| ≤25 | 62 (11.21) | 52 (11.98) | 10 (8.40) |
| 26–35 | 220 (39.78) | 177 (40.78) | 43 (36.13) |
| 36–45 | 181(32.73) | 134 (30.88) | 47 (39.50) |
| 46–55 | 67 (12.12) | 57 (13.13) | 10 (8.40) |
| ≥56 | 23 (3.80) | 14(3.23) | 9 (7.56) |
| Marital status | |||
| Single | 179 (32.37) | 140 (32.26) | 39 (32.77) |
| Married | 349 (63.11) | 275 (62.67) | 74 (62.18) |
| Divorced | 12 (2.17) | 8 (1.84) | 4 (3.36) |
| Widowed | 13 (2.35) | 11 (2.53) | 2 (1.68) |
| Years of experience | |||
| <5 | 146 (26.40) | 113 (26.04) | 44 (36.97) |
| 5–10 | 197 (35.62) | 157 (36.18) | 29 (24.37) |
| 11–20 | 137 (24.77) | 103 (23.73) | 34 (28.57) |
| 21–30 | 61 (11.03) | 52 (11.98) | 9 (7.56) |
| >30 | 12 (2.17) | 9 (2.07) | 3 (2.52) |
| Income range per month in Kenyan Shilling (KES) | |||
| ≤14,999 | 25 (4.52) | 23 (5.30) | 2 (1.68) |
| 15,000–24,999 | 56 (10.13) | 40 (9.22) | 16 (13.45) |
| 25,000–44,999 | 65 (11.75) | 48 (11.06) | 17 (14.29) |
| 45,000–64,999 | 119 (21.52) | 90 (20.74) | 29 (24.37) |
| 65,000–74,999 | 65 (11.75) | 50 (11.52) | 15 (12.61) |
| 75,000–84,999 | 62 (11.21) | 45 (10.37) | 17 (14.29) |
| 85,000–104,999 | 83 (15.01) | 73 (16.82) | 10 (8.40) |
| ≥105,000 | 78 (14.10) | 65 (14.97) | 13 (10.92) |
| Education attained | |||
| Certificate | 28 (5.06) | 20 (4.61) | 8 (6.72) |
| Diploma | 335 (60.58) | 260 (59.91) | 75 (63.03) |
| Bachelor’s degree | 157 (28.39) | 128 (29.49) | 29 (24.37) |
| Honors degree | 1 (0.18) | 1 (0.23) | 0 (0) |
| Master’s degree | 30 (5.42) | 24 (5.53) | 6 (5.04) |
| Doctor of Philosophy (PhD) degree | 2 (0.36) | 1 (0.23) | 1 (0.84) |
| Health professional cadres | |||
| Physician or Specialist Doctor | 31 (5.61) | 18 (4.15) | 13 (10.92) |
| Nursing professional | 169 (30.56) | 134 (30.88) | 35 (29.41) |
| Pharmaceutical professional | 41 (7.41) | 30 (6.91) | 11 (9.24) |
| Dentistry professional | 52 (9.40) | 37 (8.53) | 15 (12.61) |
| Clinical officer | 100 (18.08) | 76 (17.51) | 24 (20.17) |
| Medical laboratory scientist | 54 (9.76) | 41 (9.45) | 13 (10.92) |
| Public health specialist | 40 (7.23) | 37 (8.53) | 3 (2.52) |
| Nutrition and dietetics | 17 (3.07) | 16 (3.69) | 1 (0.84) |
| Radiographer | 12 (2.17) | 10 (2.30) | 2 (1.68) |
| Health records officer | 20 (3.62) | 20 (4.61) | 0 (0) |
| Physiotherapist | 12 (2.17) | 10 (2.30) | 2 (1.68) |
| Mental health specialists | 5 (0.90) | 5 (1.15) | 0 (0) |
| Type of employment | |||
| Full-time | 517 (93.49) | 406 (93.55) | 111 (93.28) |
| Part-time | 36 (6.51) | 28 (6.45) | 8 (6.72) |
| Hours worked per week | |||
| ≤10 | 47 (8.50) | 42 (9.68) | 5 (4.20) |
| 11–20 | 5 (0.90) | 4 (0.92) | 1 (0.84) |
| 21–30 | 11 (1.99) | 10 (2.30) | 1 (0.84) |
| 31–40 | 407 (73.60) | 316 (72.81) | 91 (76.47) |
| 41–50 | 45 (8.14) | 34 (7.83) | 11 (9.24) |
| ≥51 | 38 (6.87) | 28 (6.45) | 10 (8.40) |
| Household size | |||
| 1–2 | 181 (32.73) | 127 (29.26) | 54 (45.38) |
| 3–4 | 200 (36.17) | 161 (37.10) | 39 (32.77) |
| 5–7 | 159 (28.75) | 133 (30.65) | 26 (21.85) |
| 8–0 | 13 (2.35) | 13 (3.0) | 0 (0) |
| Upgrade in-service training | |||
| Yes | 365 (66) | 283 (65.21) | 82 (68.91) |
| No | 188 (34) | 151 (34.79) | 37 (31.09) |
| Staff housing | |||
| Yes | 74 (13.38) | 39 (8.99) | 35 (29.41) |
| No | 479 (86.62) | 395 (91.01) | 84 (70.59) |
| Type of housing | |||
| Permanent housing | 64 (11.57) | 35 (8.06) | 29 (24.37) |
| Semi-permanent housing | 9 (1.63) | 3 (0.69) | 6 (5.04) |
| Temporary housing | 1 (0.18) | 1 (0.23) | 1 (0.84) |
| Work Environment Variables | Overall (n = 553) n (%) | Public Hospitals (n = 434) n (%) | Mission Hospitals (n = 119) n (%) |
|---|---|---|---|
| Constant supply of water | |||
| Yes | 459 (83) | 353 (81.33) | 106 (89.08) |
| No | 94 (17) | 81 (18.66) | 13 (10.92) |
| Occurrence of unavailable water (≥1 day) | |||
| Yes | 220 (39.78) | 161 (37.10) | 59 (49.58) |
| No | 333 (60.22) | 273 (62.90) | 60 (50.42) |
| Safe drinking water | |||
| Yes | 413 (74.68) | 310 (71.43) | 103 (86.55) |
| No | 140 (25.32) | 124 (28.57) | 16 (13.45) |
| Acceptable main source of water | |||
| Yes | 461 (83.36) | 353 (81.34) | 108 (90.76) |
| No | 92 (16.64) | 81 (18.66) | 11 (9.24) |
| Type of toilet facility | |||
| Flush or pour flush | 420 (75.95) | 323 (74.42) | 97 (81.51) |
| Pit latrine | 133 (24.05) | 111 (25.58) | 22 (18.49) |
| Risk when using toilet facility | |||
| Yes | 141 (25.50) | 120 (27.65) | 21 (17.65) |
| No | 412 (74.50) | 314 (72.35) | 98 (82.35) |
| Type of risk | |||
| Injury | 16 (2.89) | 15 (3.46) | 1 (0.84) |
| Harassment | 15 (2.71) | 15 (3.46) | 0 (0) |
| Health (infections) | 99 (17.90) | 80 (18.43) | 19 (15.97) |
| ≥2 types of risk | 11 (1.99) | 11 (2.53) | 0 (0) |
| None | 412 (74.50) | 313 (72.12) | 99 (83.19) |
| Hospital disposal of waste | |||
| Formal collection service | 100 (18.08) | 75 (17.28) | 25 (21.01) |
| Informal collection service | 15 (2.71) | 9 (2.07) | 6 (5.04) |
| Disposal in designated area | 181 (32.73) | 144 (33.18) | 37 (31.09) |
| Disposal within the hospital compound | 138 (24.95) | 102 (23.50) | 36 (30.25) |
| Disposal elsewhere (burning, burying or other) | 52 (9.40) | 45 (10.37) | 7 (5.88) |
| Unknown | 67 (12.12) | 59 (13.59) | 8 (6.72) |
| Constant availability of handwash soap | |||
| Yes | 508 (91.86) | 396 (91.24) | 112 (94.11) |
| No | 45 (8.14) | 38 (8.76) | 7 (5.88) |
| Constant availability of water for handwashing | |||
| Yes | 468 (84.63) | 361 (83.18) | 107 (89.92) |
| No | 85 (15.37) | 73 (16.82) | 12 (10.08) |
| Appropriate distance of handwashing station from the toilet (≤5 m) | |||
| Yes | 499 (90.24) | 389 (89.63) | 110 (92.44) |
| No | 54 (9.76) | 45 (10.37) | 9 (7.56) |
| Workplace safety and health committee | |||
| Yes | 313 (56.60) | 262 (60.37) | 51 (42.86) |
| No | 240 (43.40) | 172 (39.63) | 68 (57.14) |
| Overall safety of hospital work environment | |||
| 0–2 (not safe) | 11 (1.99) | 11 (2.53) | 0 (0) |
| 3–5 (slightly safe) | 99 (17.90) | 90 (20.74) | 9 (7.56) |
| 6–8 (moderately safe) | 300 (54.25) | 229 (52.76) | 71 (59.66) |
| 9–10 (very safe) | 143 (5.86) | 104 (23.96) | 39 (32.77) |
| n | R2 | Adjusted R2 | F | Sig. F Change | |
|---|---|---|---|---|---|
| EQ-VAS | 553 | 0.0138 | 0.0120 | 7.69 | 0.0057 * |
| n | R2 | Adjusted R2 | F | Sig. F Change | |
|---|---|---|---|---|---|
| EQ-VAS | 553 | 0.1373 | 0.964 | 3.35 | 0.0001 * |
| Independent Variables | Coef. | Std. Err. | T-Value | Sig. | 95% Conf. Interval | |
|---|---|---|---|---|---|---|
| Hospital Ownership | 3.079 | 1.407 | 2.19 | 0.029 * | 0.316 | 5.843 |
| Sex | −0.072 | 1.093 | −0.07 | 0.947 | −2.220 | 2.075 |
| Age | −0.431 | 0.103 | −4.18 | 0.000 * | −0.634 | −0.229 |
| Income | 2.550 | 1.401 | 1.82 | 0.069 ** | −0.202 | 5.303 |
| Marital status | 1.329 | 1.245 | 1.07 | 0.286 | −1.117 | 3.775 |
| Education attained | 0.006 | 1.170 | 0.01 | 0.996 | −2.293 | 2.305 |
| Years of experience | 0.181 | 0.120 | 1.51 | 0.132 | −0.055 | 0.416 |
| Health professional cadre | 0.435 | 1.208 | 0.36 | 0.719 | −1.937 | 2.807 |
| Type of employment | −0.599 | 2.226 | −0.27 | 0.788 | −4.974 | 3.773 |
| In-service training | −0.440 | 1.180 | −0.37 | 0.709 | −2.757 | 1.877 |
| Hours worked per week | 0.021 | 0.039 | 0.53 | 0.595 | −0.056 | 0.098 |
| Household size | 0.065 | 0.328 | 0.20 | 0.843 | −0.579 | 0.708 |
| Staff housing | −1.703 | 1.612 | −1.06 | 0.291 | −4.871 | 1.464 |
| Consistent supply of water | 0.602 | 1.698 | 0.35 | 0.723 | −2.733 | 3.938 |
| Occurrence of water unavailability | −0.956 | 1.148 | −0.83 | 0.405 | −3.211 | 1.299 |
| Safe drinking water | −0.177 | 1.407 | −0.13 | 0.900 | −2.941 | 2.587 |
| Acceptable main source of water | −1.020 | 1.675 | −0.61 | 0.543 | −4.310 | 2.670 |
| Type of toilet facility | −0.951 | 1.265 | −0.75 | 0.453 | −3.437 | 1.535 |
| Presence of risk when using toilet facility | −3.126 | 1.287 | −2.43 | 0.015 * | −5.654 | −0.597 |
| Hospital dispose of garbage | 0.038 | 1.373 | 0.03 | 0.978 | −2.660 | 2.736 |
| Availability of water for hand washing | 4.478 | 1.895 | 2.36 | 0.018 * | 0.756 | 8.200 |
| Constant availability of soap | 2.284 | 2.258 | 1.01 | 0.312 | −2.153 | 6.721 |
| ≤5 m of handwashing station from the toilet | −1.767 | 2.112 | −0.84 | 0.403 | −5.917 | 2.382 |
| Workplace safety and health committee | −1.238 | 1.211 | −1.02 | 0.307 | −3.617 | 1.141 |
| Overall safety of hospital work environment | 1.030 | 0.309 | 3.34 | 0.001 * | 0.423 | 1.637 |
| Constant | 90.257 | 4.630 | 19.49 | 0.000 | 81.160 | 99.354 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muthuri, R.N.D.K.; Senkubuge, F.; Hongoro, C. Predictors of Health-Related Quality of Life among Healthcare Workers in the Context of Health System Strengthening in Kenya. Healthcare 2021, 9, 18. https://doi.org/10.3390/healthcare9010018
Muthuri RNDK, Senkubuge F, Hongoro C. Predictors of Health-Related Quality of Life among Healthcare Workers in the Context of Health System Strengthening in Kenya. Healthcare. 2021; 9(1):18. https://doi.org/10.3390/healthcare9010018
Chicago/Turabian StyleMuthuri, Rose Nabi Deborah Karimi, Flavia Senkubuge, and Charles Hongoro. 2021. "Predictors of Health-Related Quality of Life among Healthcare Workers in the Context of Health System Strengthening in Kenya" Healthcare 9, no. 1: 18. https://doi.org/10.3390/healthcare9010018
APA StyleMuthuri, R. N. D. K., Senkubuge, F., & Hongoro, C. (2021). Predictors of Health-Related Quality of Life among Healthcare Workers in the Context of Health System Strengthening in Kenya. Healthcare, 9(1), 18. https://doi.org/10.3390/healthcare9010018