Effects of Food Art Therapy on the Self-Esteem, Self-Expression, and Social Skills of Persons with Mental Illness in Community Rehabilitation Facilities



Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
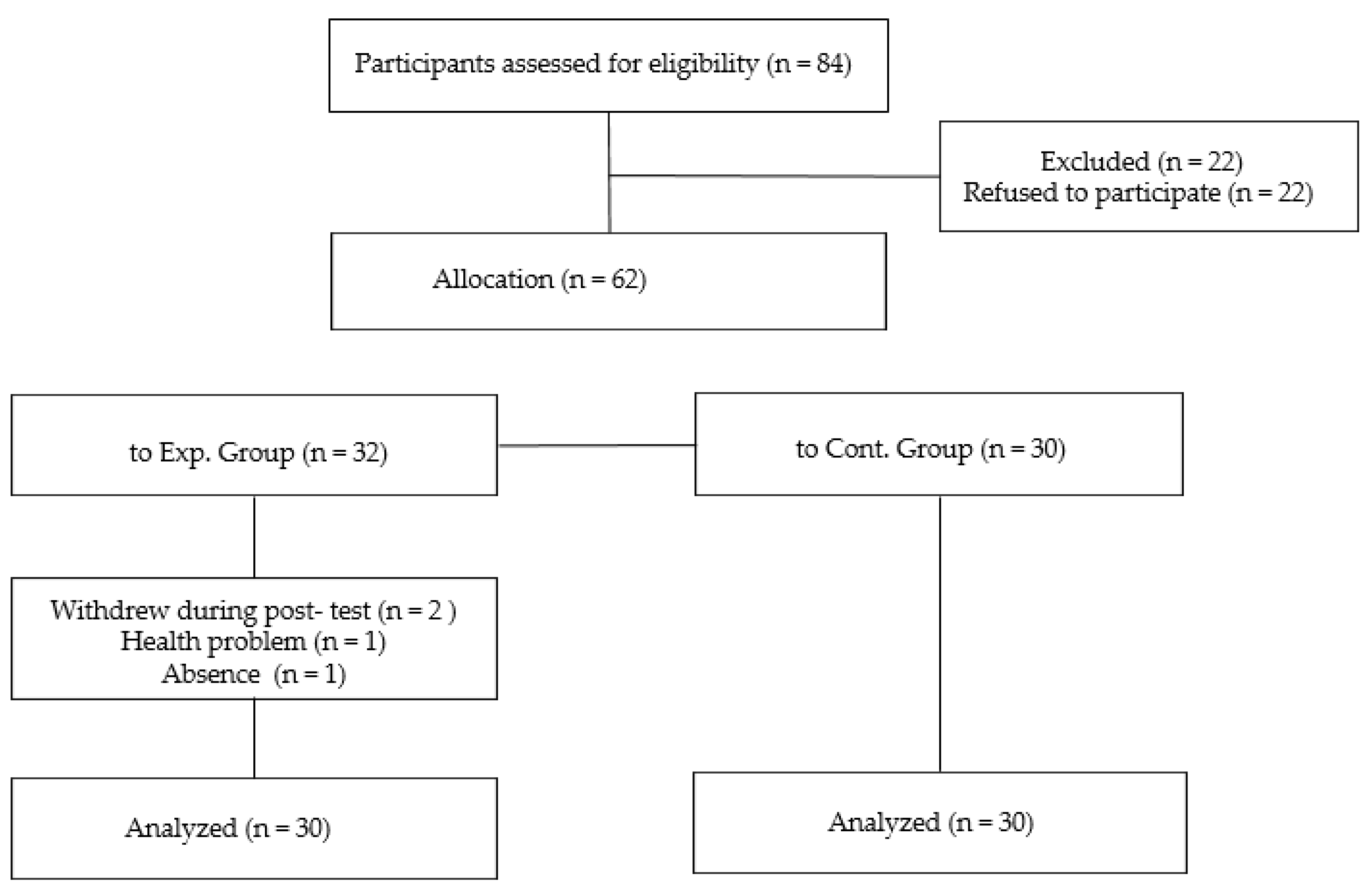
2.2. Participants
2.3. Measures
2.3.1. Rosenberg Self-Esteem Scale
2.3.2. Self-Expression Scale
2.3.3. Social Skill Rating System
2.4. Data Collection
2.4.1. Food Art Therapy Program
2.4.2. Implementing a Food Art Therapy Program
2.5. Data Analysis
3. Results
3.1. Homogeneity of Demographic Characteristics between the Groups
3.2. Homogeneity of Self-Esteem, Self-Expression, and Social Skills between the Groups
3.3. Comparison of Self-Esteem, Self-Expression, and Social Skills between the Groups
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Farmer, N.; Touchton-Leonard, K.; Ross, A. Psychosocial benefits of cooking interventions: A systematic review. Health Educ. Behav. 2018, 45, 167–180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Black, K.; Thomson, C.; Chryssidis, T.; Finigan, R.; Hann, C.; Jackson, R.; Robinson, C.; Toldi, O.; Skidmore, P. Pilot testing of an intensive cooking course for New Zealand adolescents: The create-our-own Kai study. Nutrients 2018, 10, 556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, R.C.Y.; Lee, M.S.; Chang, Y.H.; Wahlqvist, M.L. Cooking frequency may enhance survival in Taiwaness elderly. Public Health Nutr. 2012, 15, 1142–1149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barak-Nahum, A.; Haim, L.B.; Ginzburg, K. When life gives you lemons: The effectiveness of culinary group intervention among cancer patients. Soc. Sci. Med. 2016, 166, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Lee, J. Food art therapy, 1st ed.; Shinjeong: Seoul, Korea, 2009. [Google Scholar]
- Lee, S.; Kim, H. The effects of food art therapy program on the self-expression and sociality of children from low-income families. J. Arts Psychother. 2019, 15, 287–315. [Google Scholar]
- Suh, G.; Hyun, H.; Lee, H. Effects of food art therapy program on the improvement of self-esteem of female college students. Food Art Ther. 2017, 6, 21–33. [Google Scholar]
- Thomas, E.C.; Muralidharan, A.; Medoff, D.; Drapalski, A.L. Self-efficacy as a mediator of the relationship between social support and recovery in serious mental illness. Psychiat. Rehabil. J. 2016, 39, 352–360. [Google Scholar]
- The Wall Street Journal. Available online: https://www.wsj.com/articles/a-road-to-mental-health-through-the-kitchen-1418059204 (accessed on 4 November 2019).
- Kunikata, H.; Yoshinaga, N.; Nakajima, K. Effect of cognitive behavioral group therapy for recovery of self-esteem on community-living individuals with mental illness: Non-randomized controlled trial. Psychiatry Clin. Neurosci. 2016, 70, 4457–4468. [Google Scholar] [CrossRef] [Green Version]
- Funk, H.E. A Quantitative Evaluation of Cooking Classes Taught to College Students with Autism Spectrum Disorder. unpublished; manuscript in preparation.
- Lakey, C.E.; Hirsch, J.K.; Nelson, L.A.; Nasmenang, S.A. Effects of contingent self-esteem on depressive symptoms and suicidal behavior. Death Stud. 2014, 38, 563–570. [Google Scholar] [CrossRef]
- Stadelmann, S.; Grunewald, M.; Gibbels, C.; Jaeger, S.; Matuschek, T.; Weis, S.; Klein, A.M.; Hiemisch, A.; Klitzing, K.; Dohnert, M. Self-esteem of 8–14-year-old children with psychiatric disorders: Disorder-and gender-specific effects. Child. Psychiatry Hum. Dev. 2017, 48, 40–52. [Google Scholar] [CrossRef]
- Jordan, C.H.; Logel, C.; Spencer, S.J.; Zanna, M.P.; Wood, J.V.; Holmes, J.G. Responsive low self-esteem: Low explicit self-esteem, implicit self-esteem, and reactions to performance outcomes. J. Soc. Clin. Psychol. 2013, 32, 703–732. [Google Scholar] [CrossRef]
- Lee, J. Food art therapy for children and adolescents. J. Living Sci. Res. 2017, 43, 65–77. [Google Scholar]
- Vagos, P.; Pereira, A. A cognitive perspective for understanding and training assertiveness. Eur. Psychol. 2016, 21, 109–121. [Google Scholar] [CrossRef]
- Hill, K.H.; O’Brien, K.A.; Yurt, R.W. Therapeutic efficacy of a therapeutic cooking group from the patients’ perspective. J. Burn Care Res. 2007, 28, 324–327. [Google Scholar] [CrossRef]
- Bae, H.N.; Choi, S.W.; Yu, J.C.; Lee, J.S. Reliability and validity of the Korean version of the Rosenberg Self-Esteem Scale (K-RSES) in adult. Mood Emot. 2014, 12, 43–49. [Google Scholar]
- Kim, S.H. The effects of assertiveness training on assertiveness behavior of high school students. Master’s Thesis, Kyungpook National University, Daegu, Korea, 1982. [Google Scholar]
- Gresham, F.M.; Elliott, S.N. Social Skills Rating System: Manual; American Guidance Service: Circle Pines, MN, USA, 1990. [Google Scholar]
- Kim, H. A study on the validation of Social Skills Rating System (SSRS). J. Spec. Educ. 1996, 17, 121–135. [Google Scholar]
- Kim, S.; Kim, H.; Cheon, S. The effect of food art therapy for self-efficacy, emotional expression and resilience of elementary school students in multi-cultural family. J. Arts Psychother. 2019, 15, 257–285. [Google Scholar] [CrossRef]
- Park, A.; Lee, B.; Park, K. The study on the trends of activities cooking to follow cooking therapy program: With the study on the theses from 2000 to 2015. Int. J. Tour. Hosp. Res. 2015, 29, 195–208. [Google Scholar]
- Fitzsimmons, S.; Buettner, L.L. A therapeutic cooking program for older adults with dementia: Effects on agitation and apathy. Am. J. Recreat. 2003, 2, 23–33. [Google Scholar]
- Nordentoft, M.; Rasmussen, J.; Melau, M.; Hhorthoj, C.R.; Thorup, A.E. How successful are first episode programs? A review of the evidence for specialized assertive early intervention. Curr. Opin. Psychiatry 2014, 27, 167–172. [Google Scholar] [CrossRef]
- Engler-Stringer, R.; Berenbaum, S. Exploring social support through collective kitchen participation in three Canadian cities. Can. J. Community Ment. Health 2007, 26, 91–105. [Google Scholar] [CrossRef]
- Yuhi, T.; Ise, K.; Iwashina, K.; Terao, N.; Yoshioka, S.; Shomura, K.; Maehara, T.; Yazaki, A.; Koichi, K.; Furuhara, K.; et al. Sex differences in salivary oxytocin and cortisol concentration changes during cooking in a small group. Behav. Sci. (Basel.) 2018, 8, 101. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
| Sessions | Topics | Contents | Examples of Work |
|---|---|---|---|
| 1 | Self-introduction egg sandwich | 1. Greeting 2. Pre-test using questionnaires 3. Introduce topic and activities of the day 4. Cooperate with others to make egg sandwiches and express the meaning of their works 5. Wrap-up: eating, clearing | (During the first session, the authors were nervous and forgot to take pictures.) |
| 2 | My garden (sweet potato mousse salad) | 1. Greeting 2. Introduce topic and activities of the day 3. Make sweet potato mousse together using ingredients to shape ‘my garden’ (non-verbal self-expression) and express the meaning of their works 4. Wrap-up: eating, clearing |  |
| 3 | The word that I want to hear the most (decorating a pancake) | 1. Greeting 2. Introduce topic and activities of the day 3. Decorate a pancake using a chocolate pen and fruits and express the meaning of their works 4. Wrap-up: eating, clearing |  |
| 4 | My own cupcake | 1. Greeting 2. Introduce topic and activities of the day 3. Think about the things that are most valuable and interested in them 4. Express one’s interests using the ingredients provided 5. Wrap-up: eating, clearing |  |
| 5 | Making important people (making rice balls) | 1. Greeting 2. Introduce topic and activities of the day 3. Enjoy happy feelings while thinking about important people 4. Create and introduce important people using rice balls 5. Wrap-up: eating, clearing |  |
| 6 | My face (my face tortilla) | 1. Greeting 2. Introduce topic and activities of the day 3. Consider and introduce one’s strengths 4. Using tortillas, create one’s face and reveal current emotional state and perspective on oneself 5. Wrap-up: eating, clearing |  |
| 7 | A friend’s face (friend face tortilla) | 1. Greeting 2. Introduce topic and activities of the day 3. Using tortillas, create the face of a friend and express the friend’s advantages 4. Wrap-up: eating, clearing |  |
| 8 | Create your own rainbow (fruit skewer) | 1. Greeting 2. Introduce topic and activities of the day 3. Have a positive image of the future and introduce one’s dream by making fruit skewers using various fruits 4. Wrap-up: eating, clearing post-test |  |
| Demographic Characteristics | Experimental Group (n = 30) | Control Group (n = 30) | Chi-Square | ||
|---|---|---|---|---|---|
| t-Test | p | ||||
| Sex | Male | 18 (60.0%) | 16 (53.3%) | 0.27 | 0.602 |
| Female | 12 (40.0%) | 14 (46.7%) | |||
| Marital status | Single | 27 (90.0%) | 25 (83.3%) | 1.21 | 0.706 |
| Married | 0 (0%) | 1 (3.3%) | |||
| Others | 3 (10.0%) | 4 (13.3%) | |||
| Age (years) | 18–29 | 6 (20.0%) | 3 (10.0%) | 1.74 | 0.627 |
| 30–39 | 12 (40.0%) | 11 (36.7%) | |||
| 40–49 | 9 (30.0%) | 11 (36.7%) | |||
| 50 and over | 3 (10.0%) | 5 (16.7%) | |||
| Educational level | Middle school or lower | 1 (3.3%) | 1 (3.3%) | 0.31 a | 1.000 |
| High school | 25 (83.3%) | 25 (83.3%) | |||
| Bachelor’s degree or higher | 4 (13.3%) | 4 (13.3%) | |||
| Degree of disability | 1 | 2 (6.7%) | 3 (10.0%) | 0.48 | 0.924 |
| 2 | 1 (3.3%) | 1 (3.3%) | |||
| 3 | 18 (60.0%) | 19 (63.3%) | |||
| None | 9 (30.0%) | 7 (23.3%) | |||
| Diagnosis | Schizophrenia | 27 (90.0%) | 28 (93.3%) | 0.22 | 0.640 |
| Depression | 3 (10.0%) | 2 (6.7%) | |||
| Variables | Experimental Group (n = 30) | Control Group (n = 30) | t | p | |
|---|---|---|---|---|---|
| M ± SD | M ± SD | ||||
| Self-esteem | 22.90 ± 5.06 | 23.30 ± 4.74 | −0.32 | 0.753 | |
| Self-expression | Contents | 22.30 ± 2.29 | 20.97 ± 3.34 | 1.80 | 0.076 |
| Verbal | 14.90 ± 4.99 | 14.33 ± 5.35 | 0.42 | 0.673 | |
| Nonverbal | 8.33 ± 2.55 | 8.17 ± 2.61 | 0.25 | 0.804 | |
| Total | 45.53 ± 8.33 | 43.47 ± 9.87 | 0.88 | 0.385 | |
| Social skills | Cooperation | 14.30 ± 2.26 | 13.93 ± 2.42 | 0.61 | 0.547 |
| Assertion | 13.63 ± 3.29 | 12.37 ± 3.83 | 1.38 | 0.174 | |
| Self-control | 14.00 ± 2.15 | 13.70 ± 2.29 | 0.52 | 0.603 | |
| Total | 41.93 ± 6.07 | 40.00 ± 6.89 | 1.15 | 0.254 | |
| Variables | Group | Pre-Test | Post-Test | Differences | t | p | |
|---|---|---|---|---|---|---|---|
| M ± SD | M ± SD | M ± SD | |||||
| Self-esteem | Experimental | 22.90 ± 5.06 | 31.00 ± 4.19 | 8.10 ± 6.47 | 6.86 | <0.001 | |
| Control | 23.30 ± 4.74 | 23.60 ± 3.98 | 0.30 ± 7.27 | ||||
| Self-expression | Contents | Experimental | 22.30 ± 2.29 | 27.07 ± 2.84 | 4.77 ± 3.31 | 7.89 | <0.001 |
| Control | 20.97 ± 3.34 | 21.23 ± 4.52 | 0.27 ± 5.84 | ||||
| Verbal | Experimental | 14.90 ± 4.99 | 21.27 ± 2.79 | 6.37 ± 5.81 | 6.00 | <0.001 | |
| Control | 14.33 ± 5.35 | 15.63 ± 5.68 | 1.30 ± 7.01 | ||||
| Nonverbal | Experimental | 8.33 ± 2.55 | 12.53 ± 1.81 | 4.20 ± 3.21 | 7.17 | <0.001 | |
| Control | 8.17 ± 2.61 | 8.83 ± 2.99 | 0.67 ± 3.63 | ||||
| Total | Experimental | 45.53 ± 8.33 | 60.87 ± 6.22 | 15.33 ± 10.34 | 8.12 | <0.001 | |
| Control | 43.47 ± 9.87 | 45.70 ± 11.76 | 2.23 ± 14.86 | ||||
| Social skills | Cooperation | Experimental | 14.30 ± 2.26 | 16.43 ± 1.94 | 2.13 ± 3.45 | 3.39 | 0.002 |
| Control | 13.93 ± 2.42 | 14.60 ± 2.96 | 0.67 ± 3.06 | ||||
| Assertion | Experimental | 13.63 ± 3.29 | 16.20 ± 2.69 | 2.57 ± 4.65 | 3.02 | 0.005 | |
| Control | 12.37 ± 3.83 | 13.77 ± 3.78 | 1.40 ± 5.38 | ||||
| Self-control | Experimental | 14.00 ± 2.15 | 16.13 ± 2.86 | 2.13 ± 3.35 | 3.49 | 0.002 | |
| Control | 13.70 ± 2.29 | 14.67 ± 2.37 | 0.97 ± 2.77 | ||||
| Total | Experimental | 41.93 ± 6.07 | 48.77 ± 6.23 | 6.83 ± 9.28 | 4.03 | <0.001 | |
| Control | 40.00 ± 6.89 | 43.03 ± 7.30 | 3.03 ± 9.48 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.-H.; Choe, K.; Lee, K. Effects of Food Art Therapy on the Self-Esteem, Self-Expression, and Social Skills of Persons with Mental Illness in Community Rehabilitation Facilities. Healthcare 2020, 8, 428. https://doi.org/10.3390/healthcare8040428
Kim J-H, Choe K, Lee K. Effects of Food Art Therapy on the Self-Esteem, Self-Expression, and Social Skills of Persons with Mental Illness in Community Rehabilitation Facilities. Healthcare. 2020; 8(4):428. https://doi.org/10.3390/healthcare8040428
Chicago/Turabian StyleKim, Ju-Hye, Kwisoon Choe, and Kyoungsook Lee. 2020. "Effects of Food Art Therapy on the Self-Esteem, Self-Expression, and Social Skills of Persons with Mental Illness in Community Rehabilitation Facilities" Healthcare 8, no. 4: 428. https://doi.org/10.3390/healthcare8040428