On How Chronic Conditions Affect the Patient-AI Interaction: A Literature Review


Abstract
1. Introduction
- The transition from a patriarchic to a collaborative way of managing the disease: The classic standard of care relies on a model where the physician has full authority and power over the treatment of the patient. Hence, the patients do not participate in curating the parameters of their treatment at all. The new operational shift provides more control and personalization for patients in terms of the way they manage their condition.
- The transition from an episodic to a continuous monitoring cycle for the patients’ health indicators. This aspect refers to the number of times a follow-up with the physician is held. Unlike for acute diseases, where follow-ups are rarely held, chronic conditions require a continuous monitoring process. Thanks to the advent of artificial intelligence and thanks to the affordability of sensors, patients’ indicators are measured around the clock for an efficient health and wellbeing management.
- The transition from prioritizing volume to prioritizing value for the healthcare provided: The focus for healthcare management has shifted from treating acute illnesses in a massive way, to more time allocated to understanding the patient. Value is added to the patients’ experience of managing their chronic disease through the use of connected health, tele-medicine, and tele-presence robotics [11,12,13,14]. This is achieved thanks to the availability and use of artificial intelligent systems that analyze patient’s data being collected through medical sensors. The end goal of using these technologies is to increase in the wellbeing of patients, and make the management process effective and seamless.
2. Aim and Motivation
- What is the influence of different types of chronic diseases on the design choices for AI-based health coaching systems for patients?
3. Materials and Methods
3.1. Search Strategy
3.1.1. Search Sources
3.1.2. Search Terms
3.2. Study Eligibility Criteria
3.3. Study Selection
3.4. Data Extraction
3.5. Study Quality Assessment
3.6. Data Synthesis
4. Results
4.1. Search Results
4.2. Description of the Included Studies
4.3. Axial Coding of the Elements Leading Towards an Innovative HCS
4.4. Description of the Health Coaching Systems
5. Analysis
5.1. Roles for Artificial Intelligence-Based Health Coaching Systems
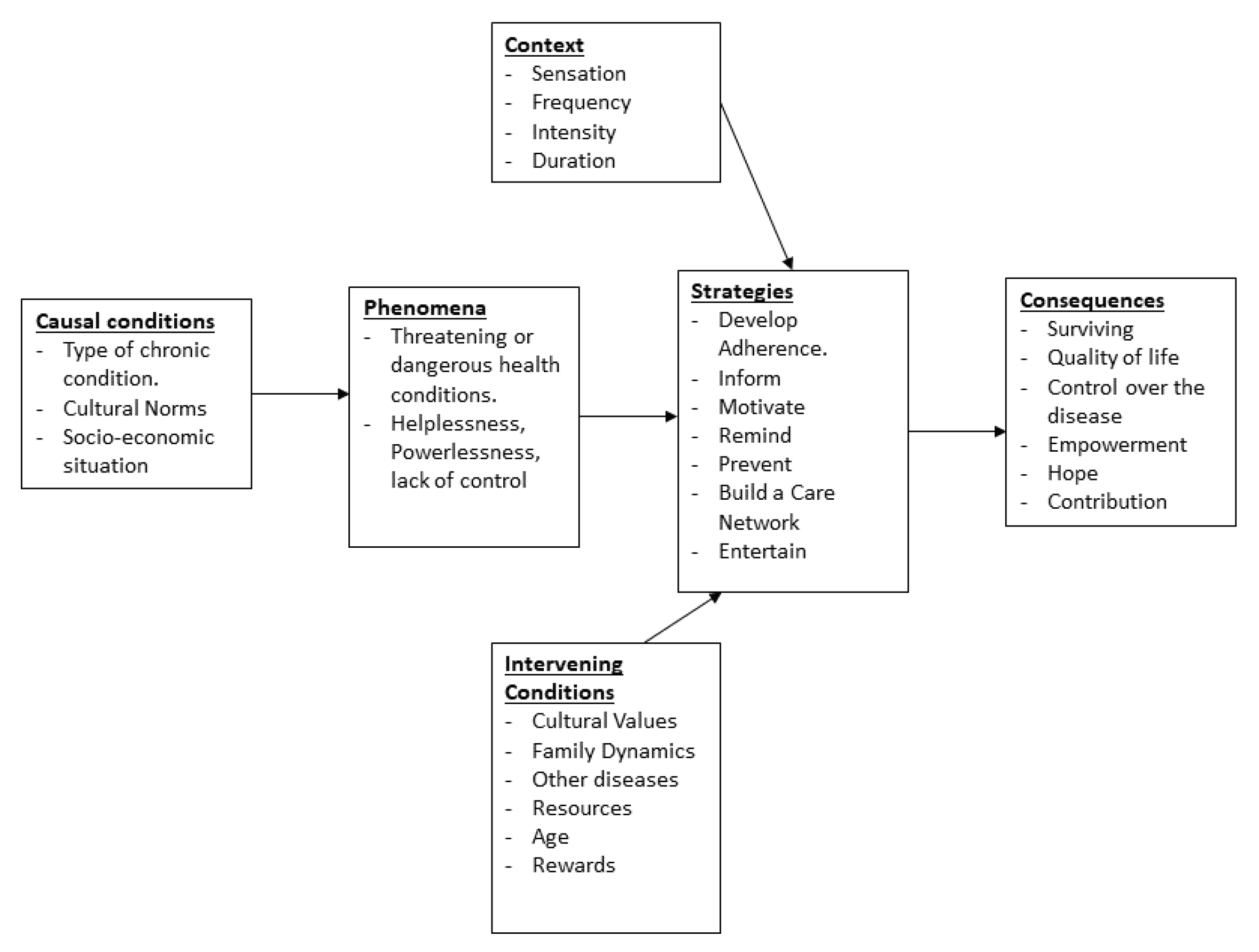
- Develop Adherence: the aim of this role is for the health coaching system to train the patients adhere to their care program. This is achieved by coaching them especially throughout the first months of the treatment. Usually, the system achieves this role by setting a goal to the user. It also provides the user with the possible methodologies to achieve the goal set by the system [20]. Throughout the duration of the care program, the patient’s adherence to the care program is developed with the help of the system directing the user towards the right habits to practice.
- Inform: the inform role consists of providing medical information about a chronic disease. This information is communicated to the user in a variety of ways to support patients’ education. This leads the users to understand the cause and effect of specific actions on their chronic condition. The aim is to support the patients understand their conditions and, hence, adhere to the care program provided.
- Motivate: this role comes into action when users are in moments of set back or depression. This is due to the mental exhaustion their disease is putting on them. Although patients, who have already developed adherence, are informed about the benefits of the care program on their health and wellness, they may often become less motivated. In such a situation, they decide to discontinue the care program. Thus, an immediate intervention from the health coaching system to motivate them is needed. The motivate role shows the patients their past achievement in managing their condition. This is usually done by providing the users with the baseline measurements that were taken at the very beginning of the care program, and showing them how far they came ever since. The progress shown is often motivating to the patients [20,43].
- Remind: this role relies on notifying the users on the right time in case they forget to accomplish a task towards their care program. The remind functionalities involve the users less in terms of time spent interacting with the health coaching system as compared to the other previously described functionality roles [43].
- Prevent: this role relies on observing the user’s chronic condition health indicators in order to prevent accordingly a health crisis in which the patients find themselves unprepared for [41,46]. In this role, systems monitor the indicators’ thresholds or use machine learning to predict when will the next health crisis occur [40,41,46]. Thus, this methodology minimizes the risk for an unexpected crisis [40].
- Build a Care Network: for this role, systems rely on establishing a social bond among the patient and other users of the system. A bond is also established among stakeholders that are not involved in using the system, but are invested in the patient’s management plan. These stakeholders help the patients in coping with their chronic disease. Building a care network aims at bridging the gap between the patient and the health coaches involved in the care process of the patient. Such health coaching systems are designed to allow clinicians, caregivers, families, and friends of the patients to have access to specific parts of the patients’ data [22,47,48].
- Entertain: this role refers to the idea that for certain users, the chronic condition they face is managed easier in a fun interactive way. Some applications use serious games [37,38], while other rely on gamifying their platforms to engage the users and gain their time and attention [21,28]. In such systems, rewards, scores, and other engaging methods are adopted [21,28,37,38].
5.2. Role Combinations for Artificial Intelligence-Based Health Coaching Systems
- The Full Multilateral HCS combination category: is characterized by the combination of all the HCS roles in the same system. The HCSs for cardio-vascular diseases, chronic obstructive pulmonary disease, and multiple sclerosis all fall under this category.
- The Unilateral HCS category: is a configuration focused on a system implementing only one role. Chronic musculo-skeletal pain, Parkinson, and rare chronic diseases fall under this category.
- The Opposing Bilateral HCS combination category: refers to different HCS roles, if combined together might undo the progress that each role has contributed to. An example of that would be the inform and entertain functionality. In the majority of cases, developing digital games is mainly intended for entertainment. Therefore, it is rare to find a video game with the intention to inform and educate. However, combining these two functionalities is possible, as it is the case for the diabetes HCSs for adolescents [37,38].
- The complementing Bilateral HCS combination category: complementing bilateral HCS roles refer to the roles that complement each other. The way these roles complement one another is by one role contributing to the development of the other. The end goal is to achieve better chronic disease management. Examples of this configuration is the “remind” and “prevent”. The roles in the HCS that remind patients with chronic migraine to take medications also contribute in preventing a migraine crisis from happening [40,41]. Another example are the motivate and develop adherence roles. Incorporating those roles simultaneously in the system motivates patients to maintain their chronic disease management schedule. The maintenance of a well managed chronic condition care schedule encourages patients to adhere to their care programs.
- The one-role-missing combination category: is characterized by a HCS incorporating all the roles except one. The case of arthritis and obesity falls under this category.
- The blurred roles combination category: is characterized by some roles not being incorporated fully or accurately. The case of serious mental illness falls under this category.
6. Discussion
6.1. Multilateral Combination Category
6.2. Unilateral Combination Category
6.3. The Opposing Bilateral Combination Category
6.4. Complementing Bilateral Combination Category
6.5. The One-Role-Missing Combination Category
6.6. The Blurred Roles Category
7. Conclusions
7.1. Concluding Remarks
- The study measured outcome: Table 2 and Table 3 revealed the measured outcome of each primary study. Throughout our analysis, we sorted these outcomes across four categories; the acceptability of the system by the participants, its effectiveness on their self-management of the disease, its usability, and finally the adoption of the participants for the system post the experiment phase. It is noteworthy that studies often do not explicitly declare their intended outcome. Therefore, the classification made across Table 2 and Table 3 is subjective to the understanding of the authors of this work. In the unlikely event when the authors of the primary studies declare the measured outcome at the end of the experiment phase, objective metrics to measure it are set before the start of the experiment. These metrics are usually represented by a question with a binary answer (e.g., Did the participant adopt the system past the experiment phase or not?). This is observed in the four studies that measure the adoption of the system post the experiment phase [22,32,36,48]. At the opposite end of the spectrum, the majority of the studies that do not specify the measured outcome metrics, as illustrated by the studies that measure the effectiveness of the system (refer to the full list of the 17 studies that fall under this category in Table 3), find the task of providing a trenchant decision with regards to the outcome of the study difficult. This may be due to different causes. Among these causes are: the sample of participants involved in the study, as well as its setting. These two causes are developed in the two points below.
- Sample of participants. The sample size across the primary studies ranged between five up to 375 participants [28,35]. This is a significant difference among studies that measure the outcome of systems with multiple similarities. This difference in the number of participants involved in each experiment changes the dynamics of measuring the outcome out of the study. For the study with only five participants [28], it is logistically, and technically easier to measure whether the patients adopted the system past the experimentation phase. However, when the number of participant is 55 folds larger, with a number of participants of 275 [35], finding the objectivity in measuring the effectiveness of the system on the participants is supposedly significantly difficult. The number of participants involved in the study may not be the only factor hindering an objective measurement outcome of the health coaching system. The following point discusses another factor that may be involved in this predicament.
- Setting of the study. The setting where the study is conducted may also be a factor in hindering an objective measurement for the effectiveness of the health coaching system. Table 2 shows that the setting of the primary studies varied between a clinical, a community, as well as an academic setting. These settings, depending on the health coaching system, may either involve favoritism, impartiality, or dis-favoritism to the approval of the participant for the system. Allowing the freedom for the participants to experiment with the system in their home setting is less stressing when compared to testing the system in an academic or a medical setting.
7.2. Limitations
7.2.1. Limitations at the Level of the Conducted Studies
7.2.2. Limitations at the Level of the Literature Review
- The methodology followed to perform the literature review: the authors follow a grounded theory literature review methodology. This methodology is more common in the social sciences compared to computer sciences [15]. This is because it allows the construction of theories through methodical gathering and analysis of data. It also uses inductive reasoning, in contrast to the deductive model based on hypothesis of the scientific method. Given the fields that are involved in this review (HCI, AI-based HCSs, chronic diseases), it is also appropriate to follow the systematic review methodology. However, the authors referred to GTLR to enable the identification of the different features that characterize artificial intelligence based health coaching systems used by patients with chronic diseases. This approach treats the content of the primary studies as empirical data. This led to different codes to emerge. The process also involved revising these codes, and grouping them into themes. This subsequently led to grounding the roles that the artificial intelligence health coaching systems play, as well as grounding the the combination of the roles that form the design of AI-based HCSs for different chronic conditions.
- The search and selection process: while there exists some commonalities among the search and selection strategies of both the systematic review and the GTLR methodologies. These commonalities are summarized in a systematic approach to searching, analysing, and reporting a set of literature (e.g., The screening steps, the clarification of what items are included in each step, two independent reviewers screening, a third solving inter-rater disagreements etc.) [15]. The systematic review methodology is characterized by unique and distinct guidelines to accurately present each step before reaching to the set of included primary studies. Among these guidelines that are not performed in this review: The PRISMA-style flowchart, the formal assessment of each study’s quality before including it in the set the primary studies, and the meta-analysis assessing the statistical heterogeneity among included studies.
7.3. Future Works
Author Contributions
Funding
Conflicts of Interest
Appendix A
- Pubmed: (artificial intelligence OR machine learning) AND (chronic disease OR chronic condition) AND (health care OR health coaching OR health management)
- IEEE Xplore: (artificial intelligence OR machine learning) AND (chronic disease OR chronic condition) AND (health care OR health coaching OR health management)
- ACM Digital Library: (artificial intelligence OR machine learning) AND (chronic disease OR chronic condition) AND (“health coaching” OR “health management”)
References
- Raghupathi, W.; Raghupathi, V. An Empirical Study of Chronic Diseases in the United States: A Visual Analytics Approach to Public Health. Int. J. Environ. Res. Public Health 2018, 15, 431. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. The Top 10 Causes of Death. 2018. Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 31 August 2020).
- Centers for Disease Control and Prevention. Chronic Disease at a Glance Reports. 2018. Available online: https://www.cdc.gov/nccdphp/publications/ (accessed on 31 August 2020).
- Sqalli, M.T.; Al-Thani, D. Towards an Integrated Health and Wellness Program Using Human-IoT Interaction. In Proceedings of the 2020 IEEE International Conference on Informatics, IoT, and Enabling Technologies (ICIoT), Doha, Qatar, 2–5 February 2020; IEEE: Piscataway, NJ, USA, 2020. [Google Scholar] [CrossRef]
- Wahab, O.A.; Hachami, M.O.; Zaffari, A.; Vivas, M.; Dagher, G.G. DARM. In Proceedings of the 18th International Database Engineering & Applications Symposium on—IDEAS ’14, Porto, Portugal, 7–9 July 2014; ACM Press: New York, NY, USA, 2014. [Google Scholar] [CrossRef]
- Nazir, S.; Khan, S.; Khan, H.U.; Ali, S.; Garcia-Magarino, I.; Atan, R.B.; Nawaz, M. A Comprehensive Analysis of Healthcare Big Data Management, Analytics and Scientific Programming. IEEE Access 2020, 8, 95714–95733. [Google Scholar] [CrossRef]
- Rjoub, G.; Bentahar, J.; Wahab, O.A. BigTrustScheduling: Trust-aware big data task scheduling approach in cloud computing environments. Future Gener. Comput. Syst. 2020, 110, 1079–1097. [Google Scholar] [CrossRef]
- Sqalli, M.T.; Al-Thani, D. AI-supported Health Coaching Model for Patients with Chronic Diseases. In Proceedings of the 2019 16th International Symposium on Wireless Communication Systems (ISWCS), Oulu, Finland, 27–30 August 2019; IEEE: Piscataway, NJ, USA, 2019. [Google Scholar] [CrossRef]
- Jones, D.S.; Podolsky, S.H.; Greene, J.A. The Burden of Disease and the Changing Task of Medicine. N. Engl. J. Med. 2012, 366, 2333–2338. [Google Scholar] [CrossRef] [PubMed]
- Moore, J.O. Technology-Supported Apprenticeship in the Management of Chronic Disease. Ph.D. Thesis, Harvard University, Cambridge, MA, USA, 2014. [Google Scholar]
- Yamashita, K.; Kato, Y.; Kurabe, K.; Koike, M.; Jinno, K.; Kito, K.; Tatsuno, K.; Sqalli, M.T. Remote operation of a robot for maintaining electric power distribution system using a joystick and a master arm as a Human Robot Interface medium. In Proceedings of the 2016 International Symposium on Micro-NanoMechatronics and Human Science (MHS), Nagoya, Japan, 28–30 November 2016; IEEE: Piscataway, NJ, USA, 2016. [Google Scholar] [CrossRef]
- Kurabe, K.; Kato, Y.; Koike, M.; Jinno, K.; Yamashita, K.; Kito, K.; Sqalli, M.T.; Tatsuno, K. A robot controller for power distribution line maintenance robot working by task-level command. In Proceedings of the 2016 IEEE/SICE International Symposium on System Integration (SII), Sapporo, Japan, 13–15 December 2016; IEEE: Piscataway, NJ, USA, 2016. [Google Scholar] [CrossRef]
- Sqalli, M.T.; Tatsuno, K.; Kurabe, K.; Ando, H.; Obitsu, H.; Itakura, R.; Aoto, T.; Yoshino, K. Improvement of a tele-presence robot autonomous navigation Using SLAM algorithm. In Proceedings of the 2016 International Symposium on Micro-NanoMechatronics and Human Science (MHS), Nagoya, Japan, 28–30 November 2016; IEEE: Piscataway, NJ, USA, 2016. [Google Scholar] [CrossRef]
- Koutentakis, D.; Pilozzi, A.; Huang, X. Designing Socially Assistive Robots for Alzheimer’s Disease and Related Dementia Patients and Their Caregivers: Where We Are and Where We Are Headed. Healthcare 2020, 8, 73. [Google Scholar] [CrossRef] [PubMed]
- Wolfswinkel, J.F.; Furtmueller, E.; Wilderom, C.P.M. Using grounded theory as a method for rigorously reviewing literature. Eur. J. Inf. Syst. 2013, 22, 45–55. [Google Scholar] [CrossRef]
- Khan, M.B.; Yang, X.; Ren, A.; Al-Hababi, M.A.M.; Zhao, N.; Guan, L.; Fan, D.; Shah, S.A. Design of Software Defined Radios Based Platform for Activity Recognition. IEEE Access 2019, 7, 31083–31088. [Google Scholar] [CrossRef]
- Nunes, F.; Verdezoto, N.; Fitzpatrick, G.; Kyng, M.; Grönvall, E.; Storni, C. Self-Care Technologies in HCI: Trends, Tensions, and Opportunities. ACM Trans. Computer-Hum. Interact. 2015, 22, 1–45. [Google Scholar] [CrossRef]
- Amershi, S.; Inkpen, K.; Teevan, J.; Kikin-Gil, R.; Horvitz, E.; Weld, D.; Vorvoreanu, M.; Fourney, A.; Nushi, B.; Collisson, P.; et al. Guidelines for Human-AI Interaction. In Proceedings of the 2019 CHI Conference on Human Factors in Computing Systems-CHI ’19, Glasgow, UK, 4–9 May 2019; ACM Press: New York, NY, USA, 2019. [Google Scholar] [CrossRef]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Med. (Zagreb) 2012, 22, 276–282. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Heng, T.; Shaw, C.; Li, L.; Feehan, L. Towards developing an e-coach to support arthritis patients in maintaining a physically active lifestyle. In Proceedings of the 12th EAI International Conference on Pervasive Computing Technologies for Healthcare-PervasiveHealth ’18, New York, NY, USA, 21–24 May 2018; ACM Press: New York, NY, USA, 2018. [Google Scholar] [CrossRef]
- Vera-Munoz, C.; Arredondo, M.T.; Ottaviano, M.; Salvi, D.; Stut, W. HeartCycle: User interaction and patient education. In Proceedings of the 2013 35th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Osaka, Japan, 3–7 July 2013; IEEE: Piscataway, NJ, USA, 2013. [Google Scholar] [CrossRef]
- Sideris, C.; Alshurafa, N.; Kalantarian, H.; Sarrafzadeh, M.; Eastwood, J.A. Effects of coaching on adherence in remote health monitoring systems. In Proceedings of the Conference on Wireless Health-WH ’15, Bethesda, MD, USA, 14–16 October 2015; ACM Press: New York, NY, USA, 2015. [Google Scholar] [CrossRef]
- Barrett, M.; Boyne, J.; Brandts, J.; Rocca, H.P.B.L.; Maesschalck, L.D.; Wit, K.D.; Dixon, L.; Eurlings, C.; Fitzsimons, D.; Golubnitschaja, O.; et al. Artificial intelligence supported patient self-care in chronic heart failure: A paradigm shift from reactive to predictive, preventive and personalised care. EPMA J. 2019, 10, 445–464. [Google Scholar] [CrossRef] [PubMed]
- Jeon, T.; Kim, B.; Jeon, M.; Lee, B.G. Implementation of a portable device for real-time ECG signal analysis. BioMed. Eng. OnLine 2014, 13, 160. [Google Scholar] [CrossRef] [PubMed]
- Klein, M.; Mogles, N.; van Wissen, A. An Intelligent Coaching System for Therapy Adherence. IEEE Pervasive Comput. 2013, 12, 22–30. [Google Scholar] [CrossRef]
- Kordestani, H.; Mojarad, R.; Chibani, A.; Osmani, A.; Amirat, Y.; Barkaoui, K.; Zahran, W. Hapicare: A Healthcare Monitoring System with Self-Adaptive Coaching using Probabilistic Reasoning. In Proceedings of the 2019 IEEE/ACS 16th International Conference on Computer Systems and Applications (AICCSA), Abu Dhabi, UAE, 3–7 November 2019; IEEE: Piscataway, NJ, USA, 2019. [Google Scholar] [CrossRef]
- Hermens, H.; op den Akker, H.; Tabak, M.; Wijsman, J.; Vollenbroek, M. Personalized Coaching Systems to support healthy behavior in people with chronic conditions. J. Electromyogr. Kinesiol. 2014, 24, 815–826. [Google Scholar] [CrossRef] [PubMed]
- Mateevitsi, V.; Reda, K.; Leigh, J.; Johnson, A. The health bar: A Persuasive Ambient Display to improve the office worker’s well being. In Proceedings of the 5th Augmented Human International Conference on-AH ’14, Kobe, Japan, 7–9 March 2014; ACM Press: New York, NY, USA, 2014. [Google Scholar] [CrossRef]
- Swann-Sternberg, T.; Singh, A.; Bianchi-Berthouze, N.; Williams, A. User needs for technology supporting physical activity in chronic pain. In Proceedings of the 2012 ACM Annual Conference Extended Abstracts on Human Factors in Computing Systems Extended Abstracts-CHI EA ’12, Austin, TX, USA, 5–10 May 2012. [Google Scholar] [CrossRef]
- Ghods, A.; Caffrey, K.; Lin, B.; Fraga, K.; Fritz, R.; Schmitter-Edgecombe, M.; Hundhausen, C.; Cook, D.J. Iterative Design of Visual Analytics for a Clinician-in-the-Loop Smart Home. IEEE J. Biomed. Health Inform. 2019, 23, 1742–1748. [Google Scholar] [CrossRef] [PubMed]
- Beattie, M.; Zheng, H.; Nugent, C.; McCullagh, P. Self-management of COPD. In Proceedings of the 8th International Conference on Ubiquitous Information Management and Communication-ICUIMC ’14, Siem Reap Cambodia, Cambodia, 9–11 January 2014; ACM Press: New York, NY, USA, 2014. [Google Scholar] [CrossRef]
- Bartlett, Y.K.; Webb, T.L.; Hawley, M.S. Using Persuasive Technology to Increase Physical Activity in People with Chronic Obstructive Pulmonary Disease by Encouraging Regular Walking: A Mixed-Methods Study Exploring Opinions and Preferences. J. Med. Internet Res. 2017, 19, e124. [Google Scholar] [CrossRef] [PubMed]
- Brunschwiler, T.; Straessle, R.; Weiss, J.; Michel, B.; Kessel, T.V.; Ko, B.J.; Wood, D.; Nordmann, Y.; Muehlner, U. CAir: Mobile-health intervention for COPD patients. In Proceedings of the 2017 IEEE 19th International Conference on e-Health Networking, Applications and Services (Healthcom), Dalian, China, 12–15 October 2017; IEEE: Piscataway, NJ, USA, 2017. [Google Scholar] [CrossRef]
- Burgess, E.R. Collaborative Self-management of Depression. In Conference Companion Publication of the 2019 on Computer Supported Cooperative Work and Social Computing; ACM: New York, NY, USA, 2019. [Google Scholar] [CrossRef]
- Fadhil, A.; Wang, Y.; Reiterer, H. Assistive Conversational Agent for Health Coaching: A Validation Study. Methods Inf. Med. 2019, 58, 9–23. [Google Scholar] [CrossRef] [PubMed]
- Tseng, J.C.; Lin, B.H.; Lin, Y.F.; Tseng, V.S.; Day, M.L.; Wang, S.C.; Lo, K.R.; Yang, Y.C. An interactive healthcare system with personalized diet and exercise guideline recommendation. In Proceedings of the 2015 Conference on Technologies and Applications of Artificial Intelligence (TAAI), Tainan, Taiwan, 20–22 November 2015; IEEE: Piscataway, NJ, USA, 2015. [Google Scholar] [CrossRef]
- Harris, A.; Durresi, A.; Tuceryan, M.; Hannon, T.S. Integrated and Personalized Diabetes Coach for Children. In Proceedings of the 2015 IEEE 29th International Conference on Advanced Information Networking and Applications Workshops, Gwangju, Korea, 25–27 March 2015; IEEE: Piscataway, NJ, USA, 2015. [Google Scholar] [CrossRef]
- den Akker, R.; Klaassen, R.; Bul, K.; Kato, P.M.; van der Burg, G.J.; di Bitonto, P. Let them play. In Proceedings of the 11th EAI International Conference on Pervasive Computing Technologies for Healthcare-PervasiveHealth ’17, Barcelona, Spain, 23–26 May 2017; ACM Press: New York, NY, USA, 2017. [Google Scholar] [CrossRef]
- Desai, P.M.; Levine, M.E.; Albers, D.J.; Mamykina, L. Pictures Worth a Thousand Words: Reflections on Visualizing Personal Blood Glucose Forecasts for Individuals with Type 2 Diabetes. In Proceedings of the 2018 CHI Conference on Human Factors in Computing Systems-CHI18, Montréal, QC, Canada, 21–26 April 2018; ACM Press: New York, NY, USA, 2018. [Google Scholar] [CrossRef]
- Park, S.Y.; Chen, Y. Individual and Social Recognition: Challenges and Opportunities in Migraine Management. In Proceedings of the 18th ACM Conference on Computer Supported Cooperative Work & Social Computing-CSCW ’15, Vancouver, DC, Canada, 14–18 March 2015; ACM Press: New York, NY, USA, 2015. [Google Scholar] [CrossRef]
- Schroeder, J.; Chung, C.F.; Epstein, D.A.; Karkar, R.; Parsons, A.; Murinova, N.; Fogarty, J.; Munson, S.A. Examining Self-Tracking by People with Migraine. In Proceedings of the 2018 on Designing Interactive Systems Conference 2018-DIS ’18, Hong Kong, China, 9–13 June 2018; ACM Press: New York, NY, USA, 2018. [Google Scholar] [CrossRef]
- Ayobi, A.; Marshall, P.; Cox, A.L.; Chen, Y. Quantifying the Body and Caring for the Mind. In Proceedings of the 2017 CHI Conference on Human Factors in Computing Systems-CHI ’17, Denver, CO, USA, 6–11 May 2017; ACM Press: New York, NY, USA, 2017. [Google Scholar] [CrossRef]
- Barnett, J.; Harricharan, M.; Fletcher, D.; Gilchrist, B.; Coughlan, J. myPace: An Integrative Health Platform for Supporting Weight Loss and Maintenance Behaviors. IEEE J. Biomed. Health Inform. 2015, 19, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Rutjes, H.; Willemsen, M.C.; IJsselsteijn, W.A. Beyond Behavior: The Coach’s Perspective on Technology in Health Coaching. In Proceedings of the 2019 CHI Conference on Human Factors in Computing Systems-CHI ’19, Glasgow, UK, 4–9 May 2019; ACM Press: New York, NY, USA, 2019. [Google Scholar] [CrossRef]
- Mitsis, K.; Zarkogianni, K.; Bountouni, N.; Athanasiou, M.; Nikita, K.S. An Ontology-Based Serious Game Design for the Development of Nutrition and Food Literacy Skills. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; IEEE: Piscataway, NJ, USA, 2019. [Google Scholar] [CrossRef]
- Nunes, F.; Fitzpatrick, G. Understanding the Mundane Nature of Self-care: Ethnographic Accounts of People Living with Parkinson’s. In Proceedings of the 2018 CHI Conference on Human Factors in Computing Systems-CHI ’18, Montréal, QC, Canada, 21–26 April 2018; ACM Press: New York, NY, USA, 2018. [Google Scholar] [CrossRef]
- MacLeod, H.; Oakes, K.; Geisler, D.; Connelly, K.; Siek, K. Rare World: Towards Technology for Rare Diseases. In Proceedings of the 33rd Annual ACM Conference on Human Factors in Computing Systems-CHI ’15, Seoul, Korea, 18–23 April 2015; ACM Press: New York, NY, USA, 2015. [Google Scholar] [CrossRef]
- MacLeod, H.; Bastin, G.; Liu, L.S.; Siek, K.; Connelly, K. “Be Grateful You Don’t Have a Real Disease”: Understanding Rare Disease Relationships. In Proceedings of the 2017 CHI Conference on Human Factors in Computing Systems-CHI ’17, Denver, CO, USA, 6–11 May 2017; ACM Press: New York, NY, USA, 2017. [Google Scholar] [CrossRef]
- Aschbrenner, K.A.; Naslund, J.A.; Gorin, A.A.; Mueser, K.T.; Scherer, E.A.; Viron, M.; Kinney, A.; Bartels, S.J. Peer support and mobile health technology targeting obesity-related cardiovascular risk in young adults with serious mental illness: Protocol for a randomized controlled trial. Contemp. Clin. Trials 2018, 74, 97–106. [Google Scholar] [CrossRef] [PubMed]
- Fadhil, A.; Schiavo, G.; Wang, Y.; Yilma, B.A. The Effect of Emojis when interacting with Conversational Interface Assisted Health Coaching System. In Proceedings of the 12th EAI International Conference on Pervasive Computing Technologies for Healthcare, New York, NY, USA, 21–24 May 2018; ACM: New York, NY, USA, 2018. [Google Scholar] [CrossRef]
- Fadhil, A.; Matteotti, C.; Armellin, G.; Villafiorita, A.; Betti, D. CoachMe: A Platform for Promoting Healthy Lifestyle. In Proceedings of the 18th International Conference on Human-Computer Interaction with Mobile Devices and Services Adjunct-MobileHCI ’16, Florence, Italy, 6–9 September 2020; ACM Press: New York, NY, USA, 2016. [Google Scholar] [CrossRef]
- Tseng, K.C.; Wong, A.M.K.; Hsu, C.L.; Tsai, T.H.; Han, C.M.; Lee, M.R. The iFit: An Integrated Physical Fitness Testing System to Evaluate the Degree of Physical Fitness of the Elderly. IEEE Trans. Biomed. Eng. 2013, 60, 184–188. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Reference | Chronic Condition | Patient Profile | Technology | Number of Weeks | Number of Participants |
|---|---|---|---|---|---|
| [20] | Arthritis | Patients with mobility limitation who prefer to not be dependent on a caregiver | “FitViz” web application allows the patients to autonomously manage their physical activity trends by showing visualizations of their activity goals. | 4 | 20 |
| [21] | Cardio-Vascular disease | Patients with a sedentary lifestyle and difficulty in initiating the care treatment | “HeartCycle” is personal health system based on a goal oriented design and an education and coaching strategy. | 13 | 120 |
| [22] | Cardio-Vascular Disease | Patients who live an unsane lifestyle and do not contemplate changing it. This lifestyle consists of a junk food based diet, and sedentary living | Remote health monitoring system based on customized messages sent to patients. The system also uses machine learning to predict the following week’s patient adherence. | 26 | 90 |
| [23] | Cardio-Vascular Disease | Ageing population with recurrent and unpredictable heart failures | System with predictive, preventive and personalized medicine approach where patients are leading their management, supported by an easily accessible online application that takes advantage of artificial intelligence | 8 | 90 |
| [24] | Cardio-Vascular Disease | Patients with abrupt cardiac failures who need to be monitored all the time for prevention and precaution of the next crisis | Portable ECG device that provides captured ECG data and suspected waveform to identify sporadic and chronic events of heart diseases | - | - |
| [25] | Cardio-Vascular Disease | Patients who find a difficulty in maintain a good balance between work, social life, a healthy diet or a regular medicine intake | “The eMate intelligent coaching system” uses the computerized behavior intervention model to send the user tailored information to motivate behavior change and overcome the patient’s lifestyle challenges. | 12 | 40 |
| [26] | Cardio-Vascular Disease | Patients with abrupt cardiac failures who need to be monitored all the time for prevention and precaution of the next crisis | Hapicare, a system that applies ontology-based uncertain reasoning over IoT sensors data and self-assessment to prevent the patient’s heart crisis | - | - |
| [27] | Chronic Neck Pain | Patients on treatment for neck or shoulder pain who need to constantly track EMG patterns of the Trapezius muscles in order to estimate their level of relaxation. | Personal Coaching Systems (PCS) that uses on-body sensing, combined with smart reasoning and context-aware feedback to support users in developing and maintaining a healthier behavior | - | - |
| [28] | Chronic Musculo-skeletal Pain (CMSP) | Patients with CMSP who are depressed and unproductive in their offices | “Healthbar” is a persuasive ambiant dislplay mounted on the office computer screens of workers to remind them to perform some in-office physical activity. | 4 | 5 |
| [29] | CMSP | Patients who associate painful memories and negative experiences related to CMSP | “PMP: Pain Management Program” system to coach patients, tailored by machine learning and physiotherapists. | 10 | 9 |
| [30] | CMSP | Old patients with CMSP who suffer from a limited ability to move | Clinician-in-the-loop (CIL) visual interface that provides clinicians with patient behavior patterns derived from smart home data. | 10 | 60 |
| [31] | Chronic Obstructive Pulmonary Disease | Patients suffering from breathlessness and fatigue. This obstacle is making physical activity challenging for them | Use of machine learning to predict the health decline of the pulmonary disease before the problem occurs. | 4 | 9 |
| [32] | Chronic Obstructive Pulmonary Disease | Breathlessness and fatigue, making physical activity challenging | Compared the use of patients for three different prototype mobile applications. Each one uses a type of persuasive technology design principles, as defined by the persuasive systems design (PSD). | 12 | 87 |
| [33] | Chronic Obstructive Pulmonary Disease | Patients who are frustrated due to impaired performance of daily living activities | System that trains a predictive algorithm to prevent exacerbations. The system also provide personalized virtual coaching to improve medication adherence and activity level. | 40 | 10 |
| [34] | Depression | Patients who are unmotivated, depressed, and antisocial | Use of a variety of technology channels to connect with others patients to express their moods. System that creates solutions and challenges to overcome depression. | 4 | 20 |
| [35] | Depression | Depressed patients who face low physical activity, harmful unhealthy diet, and high levels of stress | human–virtual agent mediated system that leverages the conversational aspect to handle menial caregiver’s works by engaging patients in a conversation. | 4 | 375 |
| [36] | Hypertension | Patients who need to maintain a continuous check of their vital signs to prevent health repercussions | “iHealth365” is an interactive system of virtual healthcare assistant to help patients easily understand their health conditions, and then well manage it for a better wellbeing. It analyzes the result of regular physical examination to evaluate the health risk and provide personalized healthcare services for patients | 30 | 10 |
| [37] | Diabetes | Adolescent patients who lack the understanding, importance and motivation to manage diabetes | Integrated Personalized mobile e-Health Coach for adolescents to support them in dealing with diabetes. | 5 | 16 |
| [38] | Diabetes | Adolescents patients who lack the understanding and motivation to manage diabetes | Platform that uses gaming and coaching for adolescent patients with type 1 diabetes | 2 | 18 |
| [39] | Diabetes | Patients who are unable to manage their diabetes by themselves | System that attempts to visualize personalized blood glucose forecasts. These forecasts promote diabetes self-management, as well as understanding key styles and visual features that resonate with patients | 4 | 13 |
| [40] | Migraine | Patients who are scared of unpredictable, intermittent breakouts in everyday life | Application to track a wide spectrum of life events across intermittent time stamps. The application therefore helps patients make sense of subjective information. | 2 | 12 |
| [41] | Migraine | Patients who have unpredictable, and poorly-understood pain, sensitivity to light, and impaired cognition. | System to track the nature of the symptoms to accommodate the uncertainty of migraine pain. | - | 279 |
| [42] | Multiple sclerosis | Patients who are Passionate about pursuing a healthy lifestyle. They are engaged in self-tracking practices of their own volition | System that adopts self-care practices with different self-tracking technologies. | - | 15 |
| [43] | Obesity | Patients with low motivation. They find a difficulty in initiating their care program. | “myPace” Obesity management system that connects dietitians to patients. It shows to the patients their regular progress updates as well as tailored advice provided by dietitians. | 1 | 10 |
| [44] | Obesity | Patients who are unconscious about their nutritional choices, or are unmotivated to change their behavior towards a sane and healthy lifestyle | e-coaching system that draws from the techniques of professional nutritional coaches | 1 | 10 |
| [45] | Obesity | Patients who suffer from unhealthy dietary habits limited nutrition literacy and food literacy skills | Serious game aiming at building nutrition literacy and food literacy skills in adolescents and young adults. | 4 | 10 |
| [46] | Parkinson | Patients living with Parkinson’s perform multiple activities in a mundane way, surprisingly different from people who do not manage this condition | Technology that adopts simple reminder methodologies to foster the mundane care for Parkinson for a better wellbeing | - | - |
| [47] | Rare Chronic Diseases | Patients appropriate the disease to their identity | social support care network to find fellow patients with the same rare chronic disease | - | - |
| [48] | Rare Chronic Diseases | Patients who are depressed, anxious, worried about the future and lonely | Online support group and repository for updated research about the disease | 22 | 11 |
| [49] | Mental Illness | Patients with low self-esteem, and low confidence. They are mostly overweight obese as a consequence of a sedentary lifestyle | Two system models are proposed. 1. a mobile health group life-style intervention (PeerFIT) 2. one-on-one wearable supported mobile life-style coaching (BEAT) | … | 144 |
| [50] | Mental Illness | Patients are hesitant and hostile towards engaging in conversations with the social surrounding. | Conversational health coaching system with multiple interaction modalities to suit the preferences of the patient (emoji-based, written, conversational) | 1 | 58 |
| Characteristics | Number of Studies |
|---|---|
| Study Design | Quasi-Experiment: n = 14, Survey n = 13, Randomized Controlled Trial n = 4 |
| Type of publication | Conference: n = 21, Journal: n = 9, Thesis: n = 1 |
| Country | The Netherlands: n = 5, US: n = 12, UK: n = 4, Italy: n = 3, Canada n = 1, Spain: n = 1, Switzerland: n = 1, Austria: n = 1, France: n = 1, Taiwan: n = 1, Greece: n = 1 |
| Years of publication | 2019: n = 9, 2018: n = 6, 2017: n = 4, 2016: n = 1, 2015: n = 5, 2014: n = 3, 2013: n = 2, 2012: n = 1 |
| Sample size | <50: n = 19 50–100: n = 8, 100–375: n = 4 |
| Mean age | 34.6 years |
| Sample type | Non clinical: n = 21 Clinical n = 10 |
| Setting | Clinical n = 9, Community n = 17, Academic n = 5 |
| Measured outcome | Acceptability: n = 5 Effectiveness: n = 17 Usability: n = 5 Adoption: n = 4 |
| Category | Characteristics | Reference |
|---|---|---|
| Purpose | Training | [25,27,32,36,49] |
| Screening | [20,30] | |
| Self-Management | [17,21,22,23,26,31,34,42,44] | |
| Counseling | [29,35,37] | |
| Education | [28,38,39,47,48,50] | |
| Diagnosing | [24,33,40,41,43,45] | |
| Platform | Stand alone software | [20,21,23,28,29,30,32,33,35,36,37,38,39,40,42,44,45,49,50] |
| web-based | [17,22,24,25,26,27,31,33,41,43,47,48] | |
| Interaction | rule-based | [17,20,28,29,33,34,37,38,39,40,42,44,45,47,48,49] |
| artificial intelligence | [21,22,23,24,25,26,27,30,31,32,35,41,42,43,50] | |
| Chronic condition | Artritis | [20] |
| Cardio vascular diseases | [21,22,23,24,25,26] | |
| Chronic Obstructive Pulmonary Disease | [31,32,33] | |
| Chronic Muskulo Skeletal Pain | [28,29,30] | |
| Diabetes | [37,38,39] | |
| Depression | [34,35] | |
| Migraine | [40,41] | |
| Multiple Sclerosis | [42] | |
| Obesity | [43,44,45] | |
| Parkinson | [17] | |
| Rare Chronic Diseases | [47,48] | |
| Mental Illness | [49,50] | |
| Chronic Neck Pain | [27] | |
| Hypertension | [52] | |
| Measured outcome | Acceptability | [25,28,37,38,39] |
| Effectiveness | [21,23,24,26,27,29,30,31,33,34,35,42,43,44,45,46,50] | |
| Usability | [20,40,41,47,49] | |
| Adoption | [22,32,36,48] |
| Category | Chronic Condition | Reference |
|---|---|---|
| Multilateral | [21] | |
| [22] | ||
| Cardio-Vascular | [23] | |
| Diseases | [24] | |
| [26] | ||
| [25] | ||
| Chronic | [31] | |
| Obstructive | [32] | |
| Pulonary Disease | [33] | |
| Multiple Sclerosis | [42] | |
| Unilateral | Chronic Muskulo | [28] |
| Skeletal Pain | [30] | |
| [29] | ||
| Parkinson | [46] | |
| Rare Chronic | [47] | |
| Diseases | [48] | |
| Opposing Bilateral | Diabetes | [37] |
| [38] | ||
| [39] | ||
| Complementing Bilateral | Migraine | [40] |
| [41] | ||
| Chronic Neck Pain | [52] | |
| Depression | [34] | |
| [35] | ||
| One-role-missing | Arthritis | [20] |
| [43] | ||
| Obesesity | [44] | |
| [45] | ||
| Blurred Roles | Serious Mental Illness | [49] |
| Category | Chronic Condition | Reference |
|---|---|---|
| Multilateral | Cardio-Vascular | [21] |
| Diseases | [22] | |
| Multiple Sclerosis | [42] |
| Category | Chronic Condition | Reference |
|---|---|---|
| Unilateral | Parkinson | [46] |
| Rare Chronic | [47] | |
| Diseases | [48] |
| Category | Chronic Condition | Reference |
|---|---|---|
| Opposing bilateral | Diabetes | [37] |
| [38] |
| Category | Chronic Condition | Reference |
|---|---|---|
| Complementing bilateral | Migraine | [40] |
| [41] |
| Category | Chronic Condition | Reference |
|---|---|---|
| One-role-missing | Arthritis | [20] |
| Obsesity | [43] |
| Category | Chronic Condition | Reference |
|---|---|---|
| Distorted | Serious Mental Illness | [49] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tahri Sqalli, M.; Al-Thani, D. On How Chronic Conditions Affect the Patient-AI Interaction: A Literature Review. Healthcare 2020, 8, 313. https://doi.org/10.3390/healthcare8030313
Tahri Sqalli M, Al-Thani D. On How Chronic Conditions Affect the Patient-AI Interaction: A Literature Review. Healthcare. 2020; 8(3):313. https://doi.org/10.3390/healthcare8030313
Chicago/Turabian StyleTahri Sqalli, Mohammed, and Dena Al-Thani. 2020. "On How Chronic Conditions Affect the Patient-AI Interaction: A Literature Review" Healthcare 8, no. 3: 313. https://doi.org/10.3390/healthcare8030313
APA StyleTahri Sqalli, M., & Al-Thani, D. (2020). On How Chronic Conditions Affect the Patient-AI Interaction: A Literature Review. Healthcare, 8(3), 313. https://doi.org/10.3390/healthcare8030313