Impacts of Anthropometric, Biochemical, Socio-Demographic, and Dietary Habits Factors on the Health Status of Urban Corporate People in a Developing Country



Abstract
1. Introduction
- How much does each factor contribute to the health status among urban corporate people in Bangladesh?
- What is the most significant factor for influencing the health status among urban corporate people in Bangladesh?
2. Materials and Methods
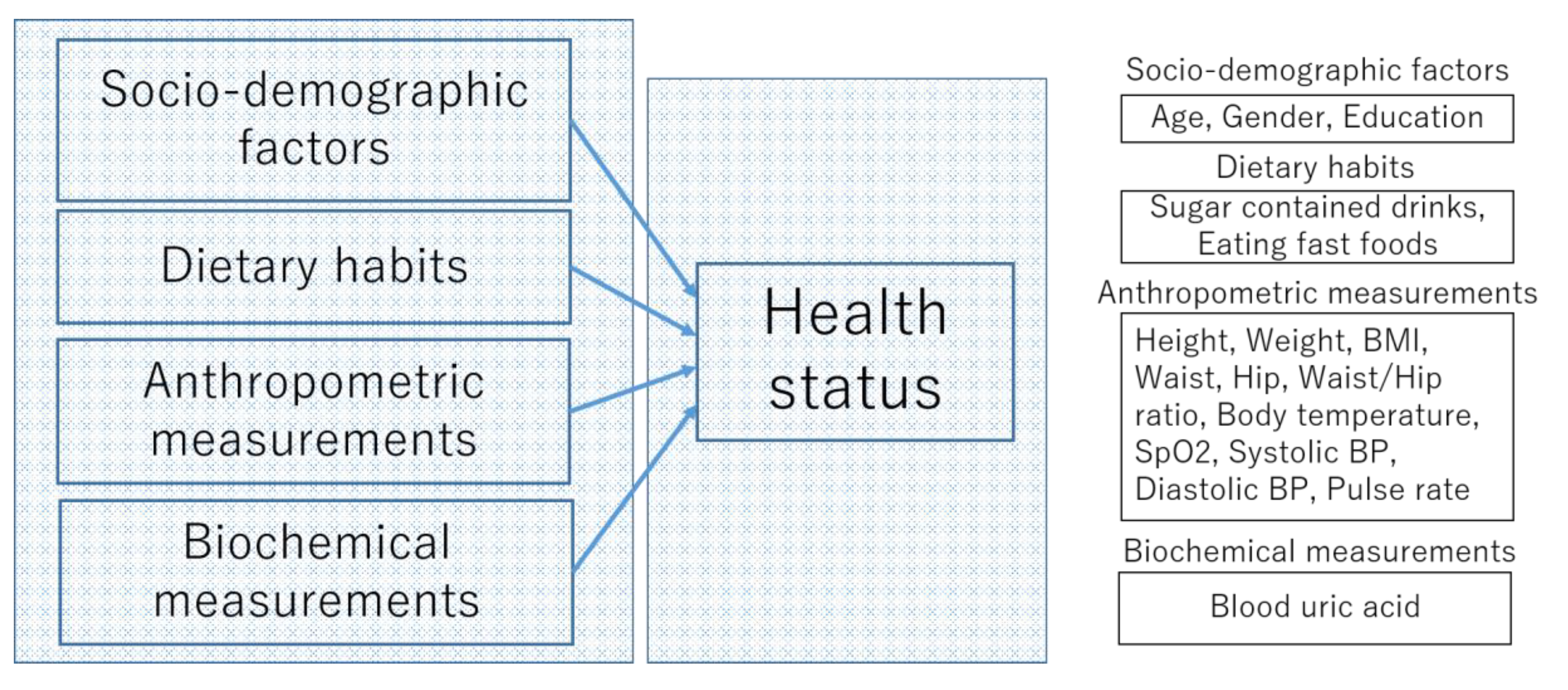
2.1. Hypotheses Development
2.1.1. Socio-Demographic Characteristics
2.1.2. Dietary Habits
2.1.3. Anthropometric Measurements
2.1.4. Biochemical Measurements
2.2. Study Place
2.3. Portable Health Clinic (PHC) System
2.4. Data Collection
2.5. Health Status
2.6. Data Analysis Technique
2.7. Ethical Approval
3. Results
3.1. Descriptive Statistics
3.2. Multinomial Logistic Regression Estimation
3.2.1. Relative Risk Ratio
3.2.2. Multicollinearity Check
3.2.3. Parameter Estimation
3.2.4. Interpretation of the MLR Results
4. Discussion
5. Limitations of the Study
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Sánchez-García, S.; García-Peñ, C.; Duque-López, M.X.; Juárez-Cedillo, T.; Cortés-Núñez, A.R.; Reyes-Beaman, S. Anthropometric Measures and Nutritional Status in a Healthy Elderly Population. BMC Public Health 2007, 7. [Google Scholar] [CrossRef] [PubMed]
- Nohara, Y.; Kai, E.; Ghosh, P.P.; Islam, R.; Ahmed, A.; Kuroda, M.; Inoue, S.; Hiramatsu, T.; Kimura, M.; Shimizu, S.; et al. Health Checkup and Telemedical Intervention Program for Preventive Medicine in Developing Countries: Verification Study. J. Med. Internet Res. 2015, 17. [Google Scholar] [CrossRef]
- Zaman, M.M.; Rahman, M.M.; Rahman, M.R.; Bhuiyan, M.R.; Karim, M.N.; Chowdhury, M.A.J. Prevalence of Risk Factors for Non-Communicable Diseases in Bangladesh: Results from STEPS Survey 2010. Indian J. Public Health 2016, 60, 17–25. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Noncommunicable Diseases. Available online: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed on 12 May 2020).
- Hoque, M.E.; Khokan, M.R.; Bari, W. Impact of stature on non-communicable diseases: Evidence based on bangladesh demographic and health survey, 2011 data. BMC Public Health 2014, 14. [Google Scholar] [CrossRef]
- Biswas, R.K.; Kabir, E. Influence of distance between residence and health facilities on non-communicable diseases: An assessment over hypertension and diabetes in Bangladesh. PLoS ONE 2017, 12, e0177027. [Google Scholar] [CrossRef] [PubMed]
- Khalequzzaman, M.; Chiang, C.; Choudhury, S.R.; Yatsuya, H.; Al-Mamun, M.A.; Al-Shoaibi, A.A.A.; Hirakawa, Y.; Hoque, B.A.; Islam, S.S.; Matsuyama, A.; et al. Prevalence of non-communicable disease risk factors among poor shantytown residents in Dhaka, Bangladesh: A community-based cross-sectional survey. BMJ Open 2017, 7. [Google Scholar] [CrossRef] [PubMed]
- Chan, D.M. Global Status Report on Noncommunicable Diseases 2010; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Sampa, M.B.; Hossain, M.N.; Hoque, M.R.; Islam, R.; Yokota, F.; Nishikitani, M.; Fukuda, A.; Ahmed, A. Influence of factors on the adoption and use of ICT-based eHealth technology by urban corporate people. J. Serv. Sci. Manag. 2020, 13, 1–19. [Google Scholar] [CrossRef]
- Maimela, E.; Alberts, M.; Modjadji, S.E.P.; Choma, S.S.R.; Dikotope, S.A.; Ntuli, T.S.; Van Geertruyden, J.P. The prevalence and determinants of chronic non-communicable disease risk factors amongst adults in the Dikgale health demographic and surveillance system (HDSS) site, Limpopo Province of South Africa. PLoS ONE 2016, 11, e0147926. [Google Scholar] [CrossRef] [PubMed]
- Alikhani, S.; Delavari, A.; Alaedini, F.; Kelishadi, R.; Rohbani, S.; Safaei, A. A province-based surveillance system for the risk factors of non-communicable diseases: A prototype for integration of risk factor surveillance into primary healthcare systems of developing countries. Public Health 2009, 123, 358–364. [Google Scholar] [CrossRef] [PubMed]
- Msyamboza, K.P.; Ngwira, B.; Dzowela, T.; Mvula, C.; Kathyola, D.; Harries, A.D.; Bowie, C. The burden of selected chronic non-communicable diseases and their risk factors in Malawi: Nationwide steps survey. PLoS ONE 2011, 6, e0020316. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Preventing Chronic Diseases: A Vital Investment; World Health Organization: Geneva, Switzerland, 2005. [Google Scholar]
- Wu, S.; Wang, R.; Zhao, Y.; Ma, X.; Wu, M.; Yan, X.; He, J. The relationship between self-rated health and objective health status: A population-based study. BMC Public Health 2013, 13, 320. [Google Scholar] [CrossRef] [PubMed]
- Oh, S.M.; Stefani, K.M.; Kim, H.C. Development and application of chronic disease risk prediction models. Yonsei Med. J. 2014, 55, 853–860. [Google Scholar] [CrossRef] [PubMed]
- Hunter, D.J.; Reddy, K.S. Non-communicable diseases. N. Engl. J. Med. 2013, 369, 1336–1343. [Google Scholar] [CrossRef]
- Whitehead, M. Inequaiities in Health: The Black Report and The Health Divide; Penguin: Harmondsworth, UK, 1988. [Google Scholar]
- Burkert, N.T.; Muckenhuber, J.; Großscha, F.; Rasky, E.; Freidl, W. Nutrition and health—The association between eating behavior and various health parameters: A matched sample study. PLoS ONE 2014, 9, e0088278. [Google Scholar] [CrossRef]
- Faruk, M.O.; Akhter, M.Z. Presence of coliforms and fecal coliforms in fast food items of local restaurants and fast food outlets of dhaka city. Bangladesh J. Microbiol. 2011, 28, 49–51. [Google Scholar] [CrossRef]
- Engchuan, W.; Dimopoulos, A.C.; Tyrovolas, S.; Caballero, F.F.; Sanchez-Niubo, A.; Arndt, H.; Ayuso-Mateos, J.L.; Haro, J.M.; Chatterji, S.; Panagiotakos, D.B. Sociodemographic indicators of health status using a machine learning approach and data from the English longitudinal study of aging (ELSA). Med. Sci. Monit. 2019, 25, 1994–2001. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Report of a WHO Expert Committee. Physical Status: The Use and Interpretation of Anthropometry; World Health Organization: Geneva, Switzerland, 1995. [Google Scholar]
- World Health Organization. Waist Circumference and Waist-Hip Ratio Report of a WHO Expert Consultation; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar] [CrossRef]
- Lee, S.; Choe, E.; Park, B. Exploration of machine learning for hyperuricemia prediction models based on basic health checkup tests. J. Clin. Med. 2019, 8, 172. [Google Scholar] [CrossRef] [PubMed]
- Sampa, M.B.; Hossain, N.; Hoque, R.; Islam, R.; Hossain, M.N.; Hoque, R.; Islam, R.; Yokota, F.; Nishikitani, M.; Fukuda, A.; et al. A framework of longitudinal study to understand determinants of actual use of the portable health clinic system. In HCI International; Streitz, N., Konomi, S., Eds.; Springer: Cham, Switzerland, 2019; Volume 11587, pp. 323–332. [Google Scholar] [CrossRef]
- Starkweather, J.; Moske, A.K. Multinomial Logistic Regression. Available online: https://it.unt.edu/sites/default/files/mlr_jds_aug2011.pdf (accessed on 10 May 2020).
- World Medical Association Declaration of Helsinki. Ethical Principles for Medical Research Involving Human Subjects; World Medical Association Declaration of Helsinki: Helsinki, Finland, 2013. [Google Scholar] [CrossRef]
- The Free Dictionary. Available online: https://medical-dictionary.thefreedictionary.com/health+status (accessed on 5 March 2020).
- Hu, M.; Nohara, Y.; Wakata, Y.; Ahmed, A.; Nakashima, N.; Nakamura, M. Machine learning based prediction of non-communicable diseases to improving intervention program in Bangladesh. Eur. J. Biomed. Inform. 2018, 14. [Google Scholar] [CrossRef]
- Alberti, G.; Zimmet, P.; Shaw, J.; Grundy, S.M. The IDF consensus worldwide definition of the metabolic syndrome. Bruss. Int. Diabetes Fed. 2006, 23, 469–480. [Google Scholar]
- Monyai, S.; Lesaoana, M.; Darikwa, T.; Nyamugure, P. Application of multinomial logistic regression to educational factors of the 2009 general household survey in South Africa. J. Appl. Stat. 2016, 43, 128–139. [Google Scholar] [CrossRef]
- Multinomial Logistic Regression Using R: Data Science Beginners. Available online: https://datasciencebeginners.com/2018/12/20/multinomial-logistic-regression-using-r/ (accessed on 11 March 2020).
- Multinomial logIstic Regression: Stata Data Analysis. Available online: https://stats.idre.ucla.edu/other/mult-pkg/faq/general/faq-how-do-i-cite-web-pages-and-programs-from-the-ucla-statistical-consulting-group/ (accessed on 10 March 2020).
- Kim, S.; Chang, Y.; Yun, K.E.; Jung, H.S.; Lee, S.J.; Shin, H.; Ryu, S. Development of nephrolithiasis in asymptomatic hyperuricemia: A cohort study. Am. J. Kidney Dis. 2017, 70, 173–181. [Google Scholar] [CrossRef] [PubMed]
- Madhu, B.; Ashok, N.C.; Balasubramanian, S. A multinomial logistic regression analysis to study the influence of residence and socio-economic status on breast cancer incidences in southern Karnataka. Int. J. Math. Stat. Invent. 2014, 2, 1–8. [Google Scholar]
- Poda, G.G.; Hsu, C.; Rau, H.; Chao, J.C. Impact of socio-demographic factors, lifestyle and health status on nutritional status among the elderly in Taiwan. Nutr. Res. Pract. 2019, 13, 222–229. [Google Scholar] [CrossRef] [PubMed]
- Jong, V.; Eijkemans, M.; Calster, B.; Timmerman, D.; Moons, K. Sample size considerations and predictive performance of multinomial logistic prediction models. Stat. Med. 2019, 38, 1601–1619. [Google Scholar] [CrossRef] [PubMed]
- Multinomial Logistic Regression R Data Analysis Examples. Available online: https://stats.idre.ucla.edu/r/dae/multinomial-logistic-regression/ (accessed on 3 February 2020).
- Nakanishi, N.; Yoshida, H.; Nakamura, K.; Suzuki, K.; Tatara, K. Predictors for development of hyperuricemia: An 8-year longitudinal study in middle-aged Japanese men. Metabolism 2001, 50, 621–626. [Google Scholar] [CrossRef]
- Rl, W. Gout and hyperuricemia. Curr. Opin. Rheumatol. 2002, 14, 281–286. [Google Scholar] [CrossRef]
- Ogura, T.; Matsuura, Y.; Mimura, Y.; Kishida, M.; Otsuka, F.; Tobe, K. Recent trends of hyperuricemia and obesity in Japanese male adolescents, 1991 through 2002. Metabolism 2004, 53, 448–453. [Google Scholar] [CrossRef]
- Ali, N.; Perveen, R.; Rahman, S.; Mahmood, S.; Rahman, S.; Islam, S.; Haque, T.; Sumon, A.H.; Kathak, R.R.; Molla, N.H.; et al. Prevalence of hyperuricemia and the relationship between serum uric acid and obesity: A study on bangladeshi adults. PLoS ONE 2018, 13, e0206850. [Google Scholar] [CrossRef]
- Schlesinger, N. Dietary factors and hyperuricaemia. Curr. Pharm. Des. 2005, 11, 4133–4138. [Google Scholar] [CrossRef]
- Miao, Z.; Yan, S.; Wang, J.; Wang, B.; Li, Y.; Xing, X.; Yuan, Y.; Meng, D.; Wang, L.; Gu, J.; et al. Insulin resistance acts as an independent risk factor exacerbating high-purine diet induced renal injury and knee joint gouty lesions. Inflamm. Res. 2009, 58, 659–668. [Google Scholar] [CrossRef]
- Lapidus, L.; Bengtsson, C.; Larsson, B.; Pennert, K.; Rybo, E.; Sjöström, L. Distribution of adipose tissue and risk of cardiovascular disease and death: A 12 year follow up of participants in the population study of women in Gothenburg, Sweden. Br. Med. J. 1984, 289, 1257–1261. [Google Scholar] [CrossRef] [PubMed]
- Beaglehole, R.; Bonita, R.; Horton, R.; Adams, C.; Alleyne, G.; Asaria, P.; Baugh, V.; Bekedam, H.; Billo, N.; Casswell, S.; et al. Priority actions for the non-communicable disease crisis. Lancet 2011, 377, 1438–1447. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Number | Independent Variables | Description | n |
|---|---|---|---|
| Clinical factors | |||
| 1 | Height (cm) | Height of the participant | 271 |
| 2 | Weight (kg) | Weight of the participant | 271 |
| 3 | BMI (kg/m2) | Weight divided by the square of the height | 271 |
| 4 | Waist (cm) | Waist circumference | 271 |
| 5 | Hip (cm) | Hip circumference | 271 |
| 6 | Waist/hip ratio | Waist to hip ratio | 271 |
| 7 | Body temperature (°F) | Body temperature | 271 |
| 8 | SpO2 | Oxygenation of blood (%) | 271 |
| 9 | Systolic BP (mmHg) | Systolic blood pressure | 271 |
| 10 | Diastolic BP (mmHg) | Diastolic blood pressure | 271 |
| 11 | Pulse rate (bpm) | Pulse rate | 271 |
| 12 | Blood uric acid (mg/dL) | Blood uric acid | 271 |
| Socio-demographic factors | |||
| 1 | Gender | Gender of the participant | 271 |
| 2 | Age | Age of the participant | 271 |
| 3 | Education | Education completed by the participant | 271 |
| Dietary information factors | |||
| 1 | Drinks | Drinking sugar-containing drinks (Coke, Fanta, soda, fruit juice, other sweet/sugar-containing drinks) three or more times a week | 271 |
| 2 | Eating fast foods | Eating fast foods such as pizzas, hamburgers, deep-fried foods (e.g., singara, samosa, Mughlai paratha, etc.) outside three or more times a week | 271 |
| Parameter (Independent Variables) | Healthy | Caution | Affected | Emergent | |
|---|---|---|---|---|---|
| Height (cm) | |||||
| Weight (kg) | |||||
| BMI | <25 | ≥25, <30 | ≥30, <35 | ≥35 | |
| Waist (cm) | Male | <90.0 | ≥90.0 | NA | NA |
| Female | <80.0 | ≥80.0 | NA | NA | |
| Hip (cm) | |||||
| Waist/hip ratio | Male | <0.90 | ≥0.90 | NA | NA |
| Female | <0.85 | ≥0.85 | NA | NA | |
| Body temperature (°F) | <98.6 | ≥98.6, <99.5 | ≥99.5 | NA | |
| Oxygenation of blood (%) | ≥96 | ≥93, <96 | ≥90, <93 | <90 | |
| Blood pressure (mmHg) | Systolic | <130 | ≥130, <140 | ≥140, <180 | ≥180 |
| Diastolic | <85 | ≥85, <90 | ≥90, <110 | ≥110 | |
| Blood sugar (mmol/dL) | RBS | <7.78 | ≥7.78, <11.11 | ≥11.11, <16.67 | ≥16.67 |
| FBS | <5.56 | ≥5.56, <7.0 | ≥7.0, <11.11 | ≥11.11 | |
| Blood hemoglobin (g/dL) | ≥12.0 | ≥10.0, <12.0 | ≥8.0, <10.0 | <8.0 | |
| Pulse rate (bpm) | ≥60, <100 | ≥50, <60 OR ≥100, <120 | <50 OR ≥120 | NA | |
| Arrhythmia | Normal | Others | |||
| Blood cholesterol (mg/dL) | ≤200.0 | >200.0, ≤225.0 | >225.0, <240.0 | ≥240.0 | |
| Blood uric acid (mg/dL) | Male | >3.5, ≤7.0 | >7.0, <8.0 | ≥8.0 | |
| Female | >2.4, ≤6.0 | >6.0, <7.0 | ≥7.0 |
| Number | Variables | Minimum | Maximum | Mean ± Std. Deviation |
|---|---|---|---|---|
| 1 | Age | 34 | 77 | 49.61 ± 7.39 |
| 2 | Height (cm) | 140.00 | 184.00 | 163.05 ± 7.45 |
| 3 | Weight (kg) | 44.20 | 114.40 | 67.52 ± 10.06 |
| 4 | BMI (kg/m2) | 18.39 | 40.53 | 25.37 ± 3.20 |
| 5 | Waist (cm) | 63.60 | 118.00 | 90.24 ± 7.80 |
| 6 | Hip (cm) | 80.00 | 127.00 | 94.54 ± 6.29 |
| 7 | Waist/hip ratio | 0.64 | 1.11 | 0.96 ± 0.06 |
| 8 | Body temperature (°F) | 92.12 | 99.64 | 96.07 ± 1.15 |
| 9 | SpO2 | 93 | 99 | 97.67 ± 1.17 |
| 10 | Systolic BP (mmHg) | 92 | 180 | 126.68 ± 14.88 |
| 11 | Diastolic BP (mmHg) | 59 | 108 | 81.71 ± 8.43 |
| 12 | Pulse rate (bpm) | 51 | 123 | 80.27 ± 11.66 |
| 13 | Blood uric acid (mg/dL) | 3.10 | 11.00 | 6.63 ± 1.54 |
| No. | Categorical Variables | Description | Categories/Levels | Frequency | % |
|---|---|---|---|---|---|
| 1 | Gender | Gender of the participant | Male = 1; | 225 | 83.0 |
| female = 0 | 46 | 17.0 | |||
| 2 | Education | Education completed by the participant | 1 = No education (no school entered); | 10 | 3.7 |
| 2 = Primary school completed; | 30 | 11.1 | |||
| 3 = Secondary school completed; | 11 | 4.1 | |||
| 4 = High school completed; | 23 | 8.5 | |||
| 5 = Vocation school completed; | 1 | 0.4 | |||
| 6 = College/university completed; | 63 | 23.2 | |||
| 7 = Higher (master or doctor) completed | 133 | 49.1 | |||
| 3 | Drinks | Drinking sugar-containing drinks (Coke, Fanta, soda, fruit juice, other sweet/sugar-containing drinks) three or more times a week | 2 = Yes; | 26 | 9.6 |
| 1 = No | 245 | 90.4 | |||
| 4 | Eating fast foods | Eating fast foods such as pizzas, hamburgers, deep-fried foods (e.g., singara, samosa, Mughlai paratha, etc.) three or more times a week | 2 = Yes; | 49 | 18.1 |
| 1 = No | 222 | 81.9 | |||
| 5 | Health status | Overall health condition | 1 = healthy; | 2 | 0.7 |
| 2 = caution; | 80 | 29 | |||
| 3 = affected; | 122 | 45 | |||
| 4=emergent | 67 | 25 |
| Health Status | Factors Name | Estimate B | Std. Error | Z Value | Pr(>|z|) | Exp(B) |
|---|---|---|---|---|---|---|
| Affected | Intercept | 20.09 | 0.01 | 3243.46 | <2.2 × 10−16 *** | 5.26 × 108 |
| Age | 0.05 | 0.03 | 1.76 | 0.08 | 1.04 | |
| Gender | −1.60 | 0.77 | −2.09 | 0.04 * | 0.21 | |
| Education | −0.04 | 0.09 | −0.38 | 0.71 | 0.97 | |
| Height | −0.17 | 0.11 | −1.53 | 0.13 | 0.85 | |
| Weight | 0.19 | 0.14 | 1.39 | 0.17 | 1.21 | |
| Waist | 0.17 | 0.05 | 3.47 | 0.00 *** | 1.19 | |
| BMI | −0.43 | 0.37 | −1.15 | 0.26 | 0.66 | |
| Hip | −0.21 | 0.07 | −3.01 | 0.01 ** | 0.82 | |
| WHR | −12.42 | 0.01 | −1698.74 | <2.2 × 10−16 *** | 4.04 × 10−6 | |
| SpO2 | 0.23 | 0.14 | 1.66 | 0.09 | 1.25 | |
| Systolic BP | 0.03 | 0.02 | 1.54 | 0.13 | 1.04 | |
| Diastolic BP | 0.07 | 0.4 | 2.08 | 0.04 * | 1.08 | |
| Drinks | −0.63 | 0.58 | −1.09 | 0.28 | 0.54 | |
| Eating fast food | 0.27 | 0.49 | 0.54 | 0.60 | 1.31 | |
| Body temperature | −0.15 | 0.16 | −0.94 | 0.35 | 0.87 | |
| Pulse rate | 0.02 | 0.02 | 1.15 | 0.26 | 1.02 | |
| Blood uric acid | 0.60 | 0.15 | 3.96 | 7.35 × 10−5 *** | 1.82 | |
| Emergent | Intercept | 98.04 | 0.01 | 10298.82 | <2.2 × 10−16 *** | 3.77 × 1042 |
| Age | 0.03 | 0.04 | 0.79 | 0.44 | 1.03 | |
| Gender | −3.55 | 1.04 | −3.44 | 0.00 *** | 0.03 | |
| Education | −0.06 | 0.14 | −0.41 | 0.68 | 0.95 | |
| Height | −0.91 | 0.16 | −5.70 | 1.21 × 10−8 *** | 0.41 | |
| Weight | 1.01 | 0.19 | 5.20 | 1.92 × 10−7 *** | 2.73 | |
| Waist | −0.32 | 0.08 | −4.38 | 1.18 × 10−5 ** | 0.74 | |
| BMI | −2.77 | 0.54 | −5.17 | 2.30 × 10−7 *** | 0.07 | |
| Hip | 0.42 | 0.10 | 4.34 | 1.42 × 10−5 *** | 1.51 | |
| WHR | 42.59 | 0.02 | 4005.93 | <2.2 × 10−16 *** | 3.12 × 10−18 | |
| SpO2 | 0.07 | 0.19 | 0.34 | 0.74 | 1.08 | |
| Systolic BP | 0.07 | 0.03 | 2.48 | 0.01 * | 1.07 | |
| Diastolic BP | −0.01 | 0.05 | −0.15 | 0.89 | 0.99 | |
| Drinks | −0.52 | 0.96 | −0.54 | 0.59 | 0.60 | |
| Eating fast food | 0.29 | 0.77 | 0.36 | 0.72 | 1.33 | |
| Body temperature | −0.32 | 0.23 | −1.43 | 0.16 | 0.73 | |
| Pulse rate | 0.03 | 0.03 | 0.97 | 0.34 | 1.03 | |
| Blood uric acid | 2.40 | 0.30 | 7.99 | 1.27 × 10−15 *** | 11.02 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sampa, M.B.; Hoque, M.R.; Hossain, M.N. Impacts of Anthropometric, Biochemical, Socio-Demographic, and Dietary Habits Factors on the Health Status of Urban Corporate People in a Developing Country. Healthcare 2020, 8, 188. https://doi.org/10.3390/healthcare8030188
Sampa MB, Hoque MR, Hossain MN. Impacts of Anthropometric, Biochemical, Socio-Demographic, and Dietary Habits Factors on the Health Status of Urban Corporate People in a Developing Country. Healthcare. 2020; 8(3):188. https://doi.org/10.3390/healthcare8030188
Chicago/Turabian StyleSampa, Masuda Begum, Md. Rakibul Hoque, and Md. Nazmul Hossain. 2020. "Impacts of Anthropometric, Biochemical, Socio-Demographic, and Dietary Habits Factors on the Health Status of Urban Corporate People in a Developing Country" Healthcare 8, no. 3: 188. https://doi.org/10.3390/healthcare8030188
APA StyleSampa, M. B., Hoque, M. R., & Hossain, M. N. (2020). Impacts of Anthropometric, Biochemical, Socio-Demographic, and Dietary Habits Factors on the Health Status of Urban Corporate People in a Developing Country. Healthcare, 8(3), 188. https://doi.org/10.3390/healthcare8030188