Outpatient Waiting Time at Vietnam Health Facilities: Policy Implications for Medical Examination Procedure


 , ,
, ,
Abstract
1. Introduction
2. Methods
2.1. Data Source
2.2. Study Subjects
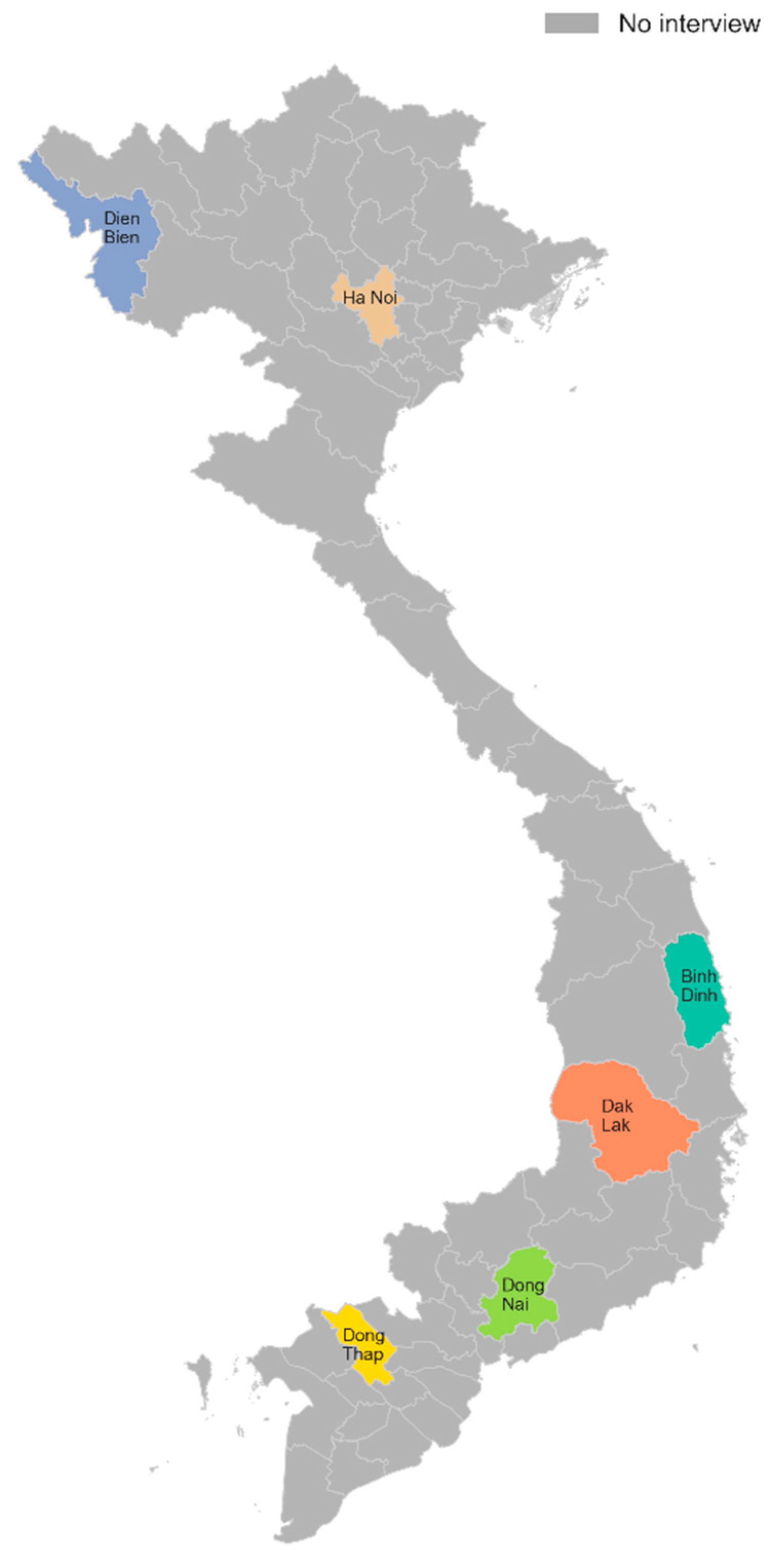
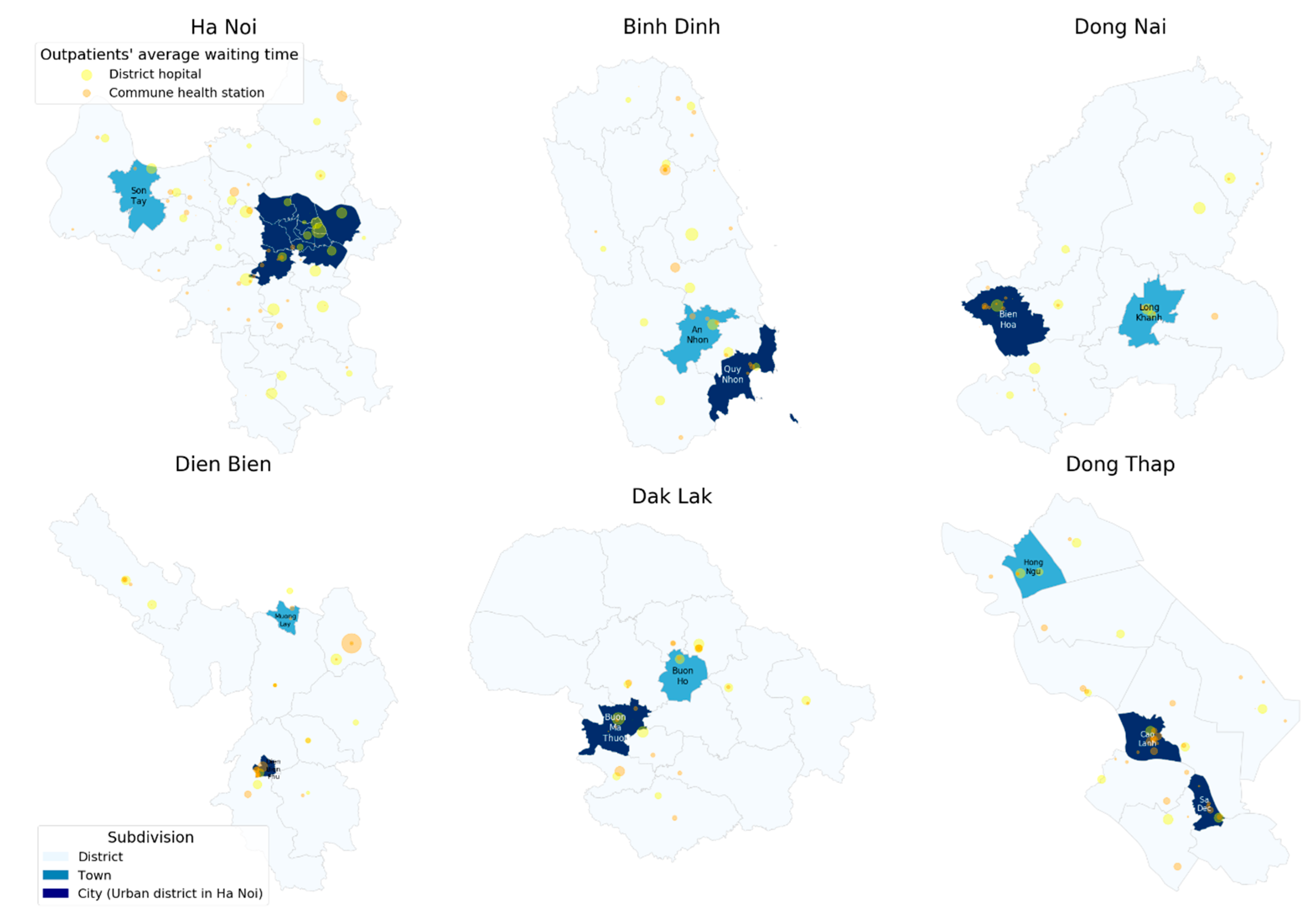
2.3. Sampling Design
2.4. Variables
2.4.1. Outcome Variable
2.4.2. Socioeconomic Variables
2.5. Measurement of Socioeconomic Status
2.6. Data Analysis
2.7. Research Ethics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Levesque, J.; Bogoch, E.R.; Cooney, B.; Johnston, B.; Wright, J.G. Improving patient satisfaction with time spent in an orthopedic outpatient clinic. Can. J. Surg. 2000, 43, 431–436. [Google Scholar] [PubMed]
- Mehra, P. Outpatient clinic waiting time, provider communication styles and satisfaction with healthcare in India. Int. J. Health Care Qual. Assur. 2016, 29, 759–777. [Google Scholar] [CrossRef] [PubMed]
- Bar-dayan, Y.; Leiba, A.; Weiss, Y.; Carroll, J.S.; Benedek, P. Waiting time is a major predictor of patient satisfaction in a primary military clinic. Mil. Med. 2002, 167, 842–845. [Google Scholar] [PubMed]
- Sibbel, R.; Urban, C. Agent-based modeling and simulation for hospital management. In Cooperative Agents; Springer: Berlin, Germany, 2001; pp. 183–202. [Google Scholar]
- Thompson, D.A.; Yarnold, P.R.; Williams, D.R.; Adams, S.L. Effects of actual waiting time, perceived waiting time, information delivery, and expressive quality on patient satisfaction in the emergency department. Ann. Emerg. Med. 1996, 28, 657–665. [Google Scholar] [CrossRef]
- Thompson, D.A.; Yarnold, P.R. Relating patient satisfaction to waiting time perceptions and expectations: The disconfirmation paradigm. Acad. Emerg. Med. 1995, 2, 1057–1062. [Google Scholar] [CrossRef] [PubMed]
- Mohebbifar, R.; Sokhanvar, M.; Khosravizadeh, O.; Mousavi Isfahani, H. Outpatient waiting time in health services and teaching hospitals: A case study in Iran. Glob. J. Health Sci. 2013, 6, 172–180. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, B.A.; Khairatul, K.; Farnaza, A. An assessment of patient waiting and consultation time in a primary healthcare clinic. Malays. Fam. Physician 2017, 12, 14–21. [Google Scholar] [PubMed]
- Dos Santos, L.M.; Stewart, G.; Rosenberg, N.M. Pediatric emergency department walk-outs. Pediatr. Emerg. Care 1994, 10, 76–78. [Google Scholar] [CrossRef] [PubMed]
- Oche, M.; Adamu, H. Determinants of patient waiting time in the general outpatient department of a tertiary health institution in north Western Nigeria. Ann. Med. Health Sci. Res. 2013, 3, 588–592. [Google Scholar] [PubMed]
- Vietnam Ministry of Health. Joint Annual Health Review 2015: Strengthening Primary Health Care at the Grassroots Towards Universal Health Coverage; Vietnam Ministry of Health Hanoi: Hanoi, Vietnam, 2016.
- Khue, L.N. Find Solutions to Reduce Waiting Time for Medical Examination and Treatment and Improve Hospital Hygiene; Agency of Health Examination and Treatment: Hanoi, Vietnam, 2018. [Google Scholar]
- The World Bank. District and Commune Health Facility Survey; The World Bank: Washington, DC, USA, 2015. [Google Scholar]
- Cullis, J.G.; Jones, P.R.; Propper, C. Waiting lists and medical treatment: Analysis and policies. In Handbook of Health Economics; Elsevier: Amsterdam, The Netherlands, 2000; Volume 1, pp. 1201–1249. [Google Scholar]
- Martin, S.; Smith, P.C. Rationing by waiting lists: An empirical investigation. J. Public Econ. 1999, 71, 141–164. [Google Scholar] [CrossRef]
- Tran, T.D.; Nguyen, U.V.; Tran, B.X. Patient waiting time in the outpatient clinic at a central surgical hospital of Vietnam: Implications for resource allocation. F1000Research 2017, 6, 454. [Google Scholar] [CrossRef] [PubMed]
- Le, C.T.; Huynh, T.T.; Do, T.C. Procedures of medical examination in outpatient clinic, Trung Vuong Emergency Hospital. Med. J. Ho Chi Minh City 2012, 4, 16. [Google Scholar]
- United Nations Population Fund in Vietnam. Factsheet: The Age and Sex Structure of Vietnam’s Population: Evidence from the 2009 Census; United Nations Population Fund: Hanoi, Vietnam, 2009. [Google Scholar]
- Nguyen, S.T.T.; Yamamoto, E.; Nguyen, M.T.N.; Le, H.B.; Kariya, T.; Saw, Y.M.; Nguyen, C.D.; Hamajima, N. Waiting time in the outpatient clinic at a national hospital in Vietnam. Nagoya J. Med. Sci. 2018, 80, 227. [Google Scholar]
- Idler, E.L.; Benyamini, Y. Self-rated health and mortality: A review of twenty-seven community studies. J. Health Soc. Behav. 1997, 38, 21–37. [Google Scholar] [CrossRef] [PubMed]
- McCallum, J.; Shadbolt, B.; Wang, D. Self-rated health and survival: A 7-year follow-up study of Australian elderly. Am. J. Public Health 1994, 84, 1100–1105. [Google Scholar] [CrossRef] [PubMed]
- Giang, T.L.; Pfau, W.D. The Elderly Population in Vietnam during Economic Transformation: An Overview; MPRA Paper: Munich, Germany, 2007. [Google Scholar]
- The National Assembly of the Socialist Republic of Vietnam. Law on Medical Examination and Treatment; NASRV: Hanoi, Vietnam, 2009.
- Communist Journal. Ensuring Health Care for Ethnic Minority People in Vietnam. Vietnam. Available online: http://english.tapchicongsan.org.vn/ (accessed on 6 June 2019).
- Vietnam Ministry of Health. Decision: Issuing Guidelines for Medical Examination Process at the Hospital’s Medical Department; Vietnam Ministry of Health: Hanoi, Vietnam, 2013.
- Ministry of Health and Joint Partnership Group. Improving Quality of Medical Services. 2010; (In Vietnamese). Available online: http://jahr.org.vn/downloads/JAHR2012/JAHR2012_Eng_Full.pdf?phpMyAdmin=5b051da883f5a46f0982cec60527c597 (accessed on 1 May 2019).
- Vietnam News. Overloaded Central Hospitals in Need of Support. Available online: https://vietnamnews.vn/society/450851/overloaded-central-hospitals-in-need-of-support.html#WbjfkWP5AtWJVf30.97 (accessed on 1 June 2018).




{kind=link}
{kind=link}
{kind=link}
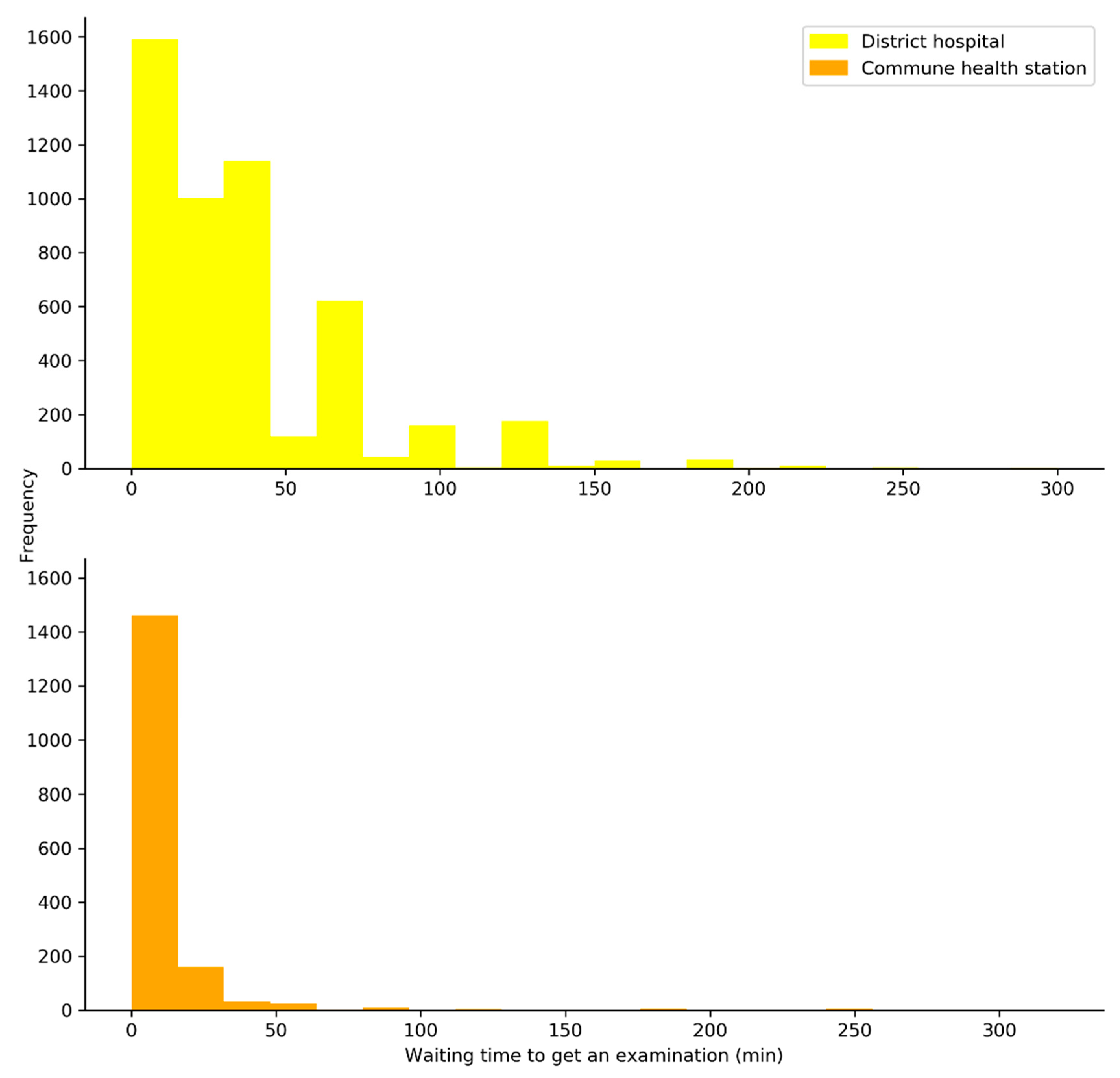
| Characteristics | District Hospital (n = 4949) | Commune Health Center (n = 1724) | ||||
|---|---|---|---|---|---|---|
| n | Outpatient’s Average Waiting Time (min) (Mean ± SD) | p-Value | n | Outpatient’s Average Waiting Time (min) (Mean ± SD) | p-Value | |
| Age group | <0.001 *** | 0.41 | ||||
| <15 | 1625 | 25.7 ± 28.5 | 438 | 10.3 ± 27.0 | ||
| 15–60 | 2081 | 34.1 ± 35.7 | 765 | 12.1 ± 34.1 | ||
| ≥60 | 1243 | 39.0 ± 40.5 | 521 | 11.8 ± 24.7 | ||
| Gender | 0.16 | 0.14 | ||||
| Male | 2217 | 31.3 ± 33.3 | 693 | 9.2 ± 21.7 | ||
| Female | 2732 | 31.6 ± 36.7 | 1031 | 13.2 ± 34.1 | ||
| Ethnicity | <0.001 *** | <0.001 *** | ||||
| NonKinh | 408 | 26.7 ± 30.1 | 276 | 28.8 ± 64.2 | ||
| Kinh | 4541 | 33.0 ± 35.6 | 1448 | 8.3 ± 14.4 | ||
| Self-reported health status | <0.001 *** | 0.20 | ||||
| Bad or very bad | 2106 | 34.6 ± 38.2 | 715 | 11.4 ± 28.9 | ||
| Normal | 2709 | 31.4 ± 32.8 | 967 | 11.8 ± 30.9 | ||
| Good or very good | 134 | 24.9 ± 31.3 | 42 | 9.7 ± 16.1 | ||
| First visit | 0.38 | 0.02 * | ||||
| No | 4454 | 32.2 ± 34.8 | 1607 | 11.9 ± 30.5 | ||
| Yes | 495 | 35.7 ± 38.7 | 117 | 7.4 ± 16.2 | ||
| Health insurance | 0.43 | <0.001 *** | ||||
| Insured | 4728 | 32.4 ± 35.1 | 1593 | 12.3 ± 30.8 | ||
| Uninsured | 221 | 36.2 ± 38.4 | 131 | 2.8 ± 5.0 | ||
| Socioeconomic status | <0.001 *** | <0.001 *** | ||||
| 1st quintile (poorest) | 1017 | 34.3 ± 33.1 | 334 | 21.3 ± 50.9 | ||
| 2nd quintile | 1054 | 30.3 ± 31.2 | 388 | 13.6 ± 33.0 | ||
| 3th quintile | 928 | 33.9 ± 37.2 | 468 | 9.0 ± 15.6 | ||
| 4th quintile | 960 | 32.7 ± 35.5 | 197 | 6.5 ± 12.2 | ||
| 5th quintile (richest) | 990 | 31.8 ± 38.9 | 337 | 6.1 ± 11.9 | ||
| Provinces | <0.001 *** | <0.001 *** | ||||
| Ha Noi | 1110 | 36.0 ± 43.5 | 280 | 9.1 ± 19.8 | ||
| Dien Bien | 315 | 21.3 ± 25.9 | 217 | 35.5 ± 70.9 | ||
| Binh Dinh | 575 | 31.8 ± 33.9 | 139 | 13.3 ± 18.6 | ||
| Dak Lak | 769 | 31.0 ± 34.9 | 240 | 8.0 ± 11.5 | ||
| Dong Nai | 870 | 37.8 ± 37.1 | 317 | 2.6 ± 6.2 | ||
| Dong Thap | 1310 | 30.1 ± 26.9 | 531 | 9.6 ± 12.7 | ||
| Characteristics | Comparison | District Hospital | Commune Health Station | ||
|---|---|---|---|---|---|
| IRR | 95% CI | IRR | 95% CI | ||
| Age | 1.01 | 1.00–1.01 | 1.01 | 1.00–1.01 | |
| Gender | Female vs. Male | 1.05 | 0.99–1.12 | 1.17 | 0.96–1.40 |
| Ethnicity | Kinh vs. NonKinh | 1.19 | 1.07–1.33 | 0.28 | 0.22–0.37 |
| First visit | Yes vs. No | 1.21 | 1.09–1.34 | 0.85 | 0.59–1.25 |
| Self-reported health status | Bad or very bad vs. Normal | 1.05 | 0.99–1.12 | 1.16 | 0.971.40 |
| Good or very good vs. Normal | 0.83 | 0.67–1.00 | 1.17 | 0.76–1.98 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nguyen, D.-H.; Tran, D.-V.; Vo, H.-L.; Nguyen Si Anh, H.; Doan, T.-N.-H.; Nguyen, T.-H.-T. Outpatient Waiting Time at Vietnam Health Facilities: Policy Implications for Medical Examination Procedure. Healthcare 2020, 8, 63. https://doi.org/10.3390/healthcare8010063
Nguyen D-H, Tran D-V, Vo H-L, Nguyen Si Anh H, Doan T-N-H, Nguyen T-H-T. Outpatient Waiting Time at Vietnam Health Facilities: Policy Implications for Medical Examination Procedure. Healthcare. 2020; 8(1):63. https://doi.org/10.3390/healthcare8010063
Chicago/Turabian StyleNguyen, Dinh-Hoa, Dinh-Van Tran, Hoang-Long Vo, Hao Nguyen Si Anh, Thi-Ngoc-Ha Doan, and Thi-Huyen-Trang Nguyen. 2020. "Outpatient Waiting Time at Vietnam Health Facilities: Policy Implications for Medical Examination Procedure" Healthcare 8, no. 1: 63. https://doi.org/10.3390/healthcare8010063
APA StyleNguyen, D.-H., Tran, D.-V., Vo, H.-L., Nguyen Si Anh, H., Doan, T.-N.-H., & Nguyen, T.-H.-T. (2020). Outpatient Waiting Time at Vietnam Health Facilities: Policy Implications for Medical Examination Procedure. Healthcare, 8(1), 63. https://doi.org/10.3390/healthcare8010063