Perspectives of Stakeholders on Technology Use in the Care of Community-Living Older Adults with Dementia: A Systematic Literature Review

 ,
,
Abstract
1. Introduction
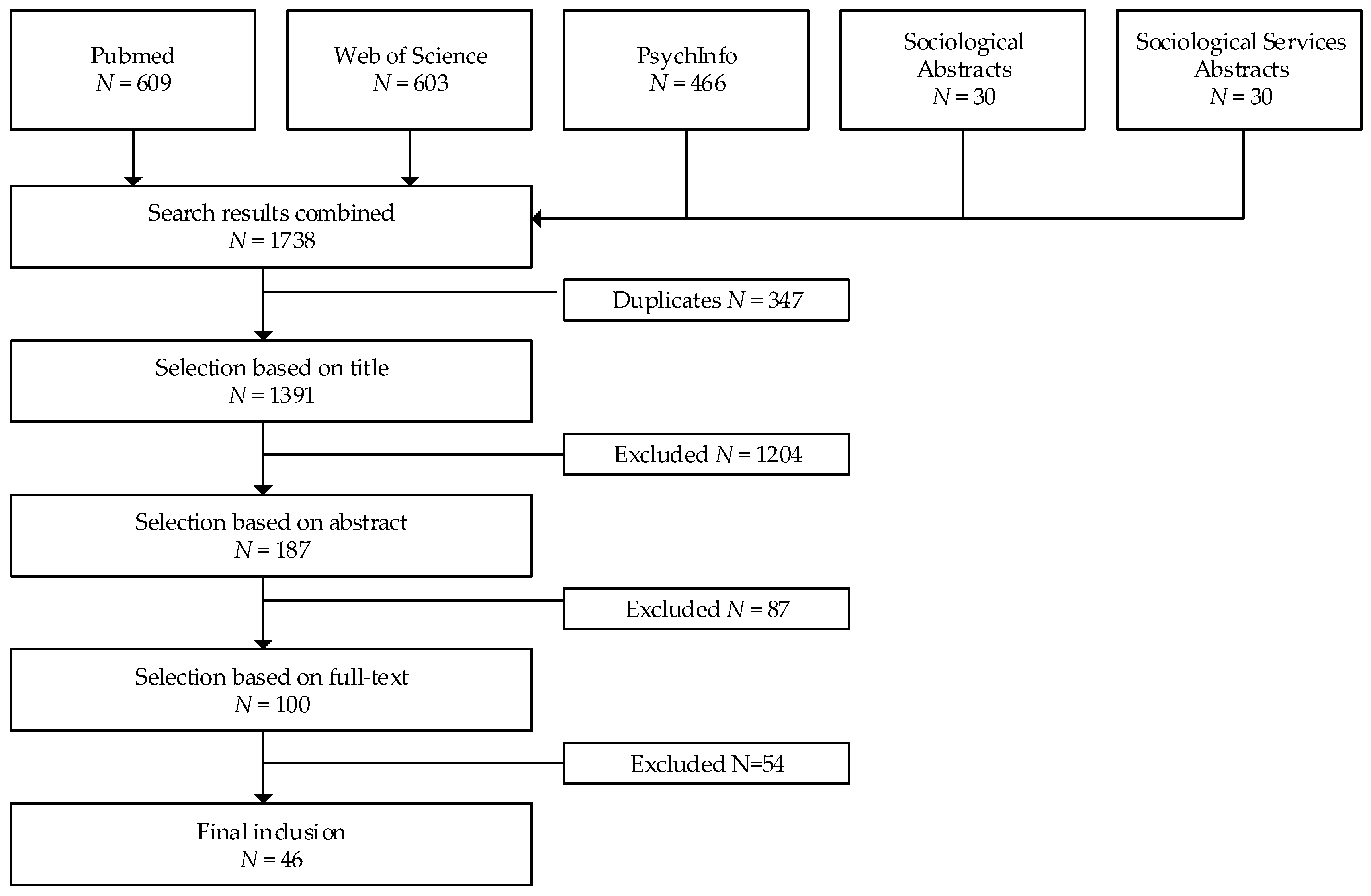
2. Materials and Methods
3. Results
3.1. General Findings
3.2. Shared Perspectives on Technology use Among all Stakeholders
3.3. Perspectives on Technology Use among Persons with Dementia
3.4. Perspectives on Technology Use among Informal Caregivers
3.5. Perspectives on Technology Use among Formal Caregivers
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Boldy, D.; Grenade, L.; Lewin, G.; Karol, E.; Burton, E. Older people’s decisions regarding ’ageing in place’: A Western Australian case study. Australas J. Ageing 2011, 30, 136–142. [Google Scholar] [CrossRef] [PubMed]
- Eckert, J.K.; Morgan, L.A.; Swamy, N. Preferences for receipt of care among community-dwelling adults. J. Aging Soc. Policy 2004, 16, 49–65. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Age-friendly Cities: A Guide.; World Health Organization: Geneva, Schwitzerland, 2007. [Google Scholar]
- Fausset, C.B.; Kelly, A.J.; Rogers, W.A.; Fisk, A.D. Challenges to Aging in Place: Understanding Home Maintenance Difficulties. J. Housing Elderly 2011, 25, 125–141. [Google Scholar] [CrossRef]
- Peek, S.T.M.; Aarts, S.; Wouters, E. Can smart home technolog deliver on the promise of independent living? A critical reflection based on the perspecties of older adults. In Handbook of Smart Homes, Health Care and Well-being; van Hoof, J., Demiris, G., Eds.; Springer international Publishing: Cham, Schwitzerland, 2017; pp. 203–214. [Google Scholar]
- Reeder, B.; Meyer, E.; Lazar, A.; Chaudhuri, S.; Thompson, H.J.; Demiris, G. Framing the evidence for health smart homes and home-based consumer health technologies as a public health intervention for independent aging: A systematic review. Int. J. Med. Inform. 2013, 82, 565–579. [Google Scholar] [CrossRef]
- Frisardi, V.; Imbimbo, B.P. Gerontechnology for demented patients: smart homes for smart aging. J. Alzheimer’s Disease JAD 2011, 23, 143–146. [Google Scholar] [CrossRef]
- Nijhof, N.; van Gemert-Pijnen, L.J.; Sixsmith, A.; Seydel, E.R. User evaluation of ADLife technology to improve wellbeing and to save cost for people with dementia. Gerontechnology 2012, 11, 256. [Google Scholar] [CrossRef]
- Nijhof, N.; van Gemert-Pijnen, L.J.; Woolrych, R.; Sixsmith, A. An evaluation of preventive sensor technology for dementia care. J. Telemed. Telecare 19, 95–100. [CrossRef] [PubMed]
- Lauriks, S.; Reinersmann, A.; Van der Roest, H.G.; Meiland, F.J.; Davies, R.J.; Moelaert, F.; Mulvenna, M.D.; Nugent, C.D.; Droes, R.M. Review of ICT-based services for identified unmet needs in people with dementia. Ageing Res. Rev. 2007, 6, 223–246. [Google Scholar] [CrossRef]
- Maresova, P.; Klimova, B. Supporting Technologies for Old People with Dementia: A Review. IFAC-PapersOnLine 2015, 48, 129–134. [Google Scholar] [CrossRef]
- Greenhalgh, T.; Wherton, J.; Papoutsi, C.; Lynch, J.; Hughes, G.; A’Court, C.; Hinder, S.; Fahy, N.; Procter, R.; Shaw, S. Beyond Adoption: A New Framework for Theorizing and Evaluating Nonadoption, Abandonment, and Challenges to the Scale-Up, Spread, and Sustainability of Health and Care Technologies. J. Med. Internet Res. 2017, 19, e367. [Google Scholar] [CrossRef]
- Liu, L.; Stroulia, E.; Nikolaidis, I.; Miguel-Cruz, A.; Rios Rincon, A. Smart homes and home health monitoring technologies for older adults: A systematic review. Int. J. Med. Inform. 2016, 91, 44–59. [Google Scholar] [CrossRef]
- Murray, E.; May, C.; Mair, F. Development and formative evaluation of the e-Health Implementation Toolkit (e-HIT). BMC Med. Inform. Decis. Mak. 2010, 10, 61. [Google Scholar] [CrossRef]
- Levine, D.M.; Lipsitz, S.R.; Linder, J.A. Trends in Seniors’ Use of Digital Health Technology in the United States, 2011-2014 Trends in Seniors’ Use of Digital Health Technology in the United States, 2011–2014Letters. Jama 2016, 316, 538–540. [Google Scholar] [CrossRef]
- Cook, E.; Randhawa, G.; Guppy, A.; Sharp, C.; Barton, G.; Bateman, A.; Crawford-White, J. Exploring factors that impact the decision to use assistive telecare: Perspectives of family care-givers of older people in the United Kingdom. Ageing Soc. 2018, 38, 1912–1932. [Google Scholar] [CrossRef]
- Sponselee, A.; Schouten, B.; Bouwhuis, D.; Willems, C. Smart Home Technology for the Elderly: Perceptions of Multidisciplinary Stakeholders. In Constructing Ambient Intelligence; Mühlhäuser, M., Ferscha, A., Aitenbichler, E., Eds.; Springer: Berlin, Germanypp, 2007; volume 11, pp. 314–326. [Google Scholar]
- McCreadie, C.; Tinker, A. The acceptability of assistive technology to older people. Ageing Soc. 2005, 25, 91–110. [Google Scholar] [CrossRef]
- Peek, S.T.; Wouters, E.J.; Luijkx, K.G.; Vrijhoef, H.J. What it Takes to Successfully Implement Technology for Aging in Place: Focus Groups With Stakeholders. J. Med. Internet Res. 2016, 18, e98. [Google Scholar] [CrossRef]
- Verkerk, M.J. The Triple I model: A translation of Dooyeweerdian Philosophical concepts for Engineers. In Social change in our technology-based world. Proceedings of the 19th annual working conference of the IIDE.; Rathbone, M., von Scheele, F., Strijbos, S., Eds.; Rozenberg: Amsterdam, The Netherlands, 2014. [Google Scholar]
- Verkerk, M.J.; Holtkamp, F.C.; Wouters, E.; van Hoof, J. Professional Practices and User Practices: An Explorative Study in Health Care. Philos. Reformatica 2017, 82, 1–25. [Google Scholar] [CrossRef]
- Pace, R.; Pluye, P.; Bartlett, G.; Macaulay, A.C.; Salsberg, J.; Jagosh, J.; Seller, R. Testing the reliability and efficiency of the pilot Mixed Methods Appraisal Tool (MMAT) for systematic mixed studies review. Int. J. Nurs. Stud. 2012, 49, 47–53. [Google Scholar] [CrossRef]
- Alwin, J.; Persson, J.; Krevers, B. Perception and significance of an assistive technology intervention—The perspectives of relatives of persons with dementia. Disabil. Rehabil. 2013, 35, 1519–1526. [Google Scholar] [CrossRef]
- Arntzen, C.; Holthe, T.; Jentoft, R. Tracing the successful incorporation of assistive technology into everyday life for younger people with dementia and family carers. Dement. Int. J. Soc. Res. Pract. 2016, 15, 646–662. [Google Scholar] [CrossRef]
- Azad, N.; Amos, S.; Milne, K.; Power, B. Telemedicine in a rural memory disorder clinic-remote management of patients with dementia. Can. Geriatr. J. 2012, 15, 96–100. [Google Scholar] [CrossRef]
- Burstein, A.A.; DaDalt, O.; Kramer, B.; D’Ambrosio, L.A.; Coughlin, J.F. Dementia caregivers and technology acceptance: Interest outstrips awareness. Gerontechnology 2015, 14, 45–56. [Google Scholar] [CrossRef]
- Chiu, T.M.; Eysenbach, G. Theorizing the health service usage behavior of family caregivers: A qualitative study of an internet-based intervention. Int. J. Med. Inform. 2011, 80, 754–764. [Google Scholar] [CrossRef]
- Chou, H.K.; Yan, S.H.; Lin, I.C.; Tsai, M.T.; Chen, C.C.; Woung, L.C. A Pilot Study of the Telecare Medical Support System as an Intervention in Dementia Care: The Views and Experiences of Primary Caregivers. J. Nurs. Res. 2012, 20, 169–180. [Google Scholar] [CrossRef]
- Cristancho-Lacroix, V.; Wrobel, J.; Cantegreil-Kallen, I.; Dub, T.; Rouquette, A.; Rigaud, A.S. A Web-Based Psychoeducational Program for Informal Caregivers of Patients With Alzheimer’s Disease: A Pilot Randomized Controlled Trial. J. Med. Internet Res. 2015, 17, 14. [Google Scholar] [CrossRef]
- Czarnuch, S.; Mihailidis, A. The design of intelligent in-home assistive technologies: Assessing the needs of older adults with dementia and their caregivers. Gerontechnology 2011, 10, 169–182. [Google Scholar] [CrossRef]
- Dal Bello-Haas, V.P.M.; O’Connell, M.E.; Morgan, D.G.; Crossley, M. Lessons learned: Feasibility and acceptability of a telehealth-delivered exercise intervention for rurald-welling individuals with dementia and their caregivers. Rural Remote Health 2014, 14, 11. [Google Scholar]
- Ekstrom, A.; Ferm, U.; Samuelsson, C. Digital communication support and Alzheimer’s disease. Dementia (London, England) 2015. [Google Scholar] [CrossRef]
- Faucounau, V.; Riguet, M.; Orvoen, G.; Lacombe, A.; Rialle, V.; Extra, J.; Rigaud, A.S. Electronic tracking system and wandering in Alzheimer’s disease: a case study. Ann. Phys. Rehabil. Med. 2009, 52, 579–587. [Google Scholar] [CrossRef]
- Gibson, G.; Dickinson, C.; Brittain, K.; Robinson, L. The everyday use of assistive technology by people with dementia and their family carers: A qualitative study. BMC Geriatr. 2015, 15, 10. [Google Scholar] [CrossRef]
- Hastall, M.R.; Eiermann, N.D.; Ritterfeld, U. Formal and informal carers’ views on ICT in dementia care: Insights from two qualitative studies. Gerontechnology 2014, 13, 53–58. [Google Scholar] [CrossRef]
- Jentoft, R.; Holthe, T.; Arntzen, C. The use of assistive technology in the everyday lives of young people living with dementia and their caregivers. Can a simple remote control make a difference? Int. Psychogeriatr. 2014, 26, 2011–2021. [Google Scholar] [CrossRef]
- Kearns, W.D.; Rosenberg, D.; West, L.; Applegarth, S. Attitudes and expectations of technologies to manage wandering behavior in persons with dementia. Gerontechnology 2007, 6, 89–101. [Google Scholar] [CrossRef]
- Kerssens, C.; Kumar, R.; Adams, A.E.; Knott, C.C.; Matalenas, L.; Sanford, J.A.; Rogers, W.A. Personalized Technology to Support Older Adults With and Without Cognitive Impairment Living at Home. Am. J. Alzheimers Dis. Other Dement. 2015, 30, 85–97. [Google Scholar] [CrossRef]
- Kim, H. Understanding Internet Use Among Dementia Caregivers: Results of Secondary Data Analysis Using the US Caregiver Survey Data. Interact. J. Med. Res. 2015, 4, 27–38. [Google Scholar] [CrossRef]
- Landau, R.; Auslander, G.K.; Werner, S.; Shoval, N.; Heinik, J. Families’ and Professional Caregivers’ Views of Using Advanced Technology to Track People With Dementia. Qual. Health Res. 2010, 20, 409–419. [Google Scholar] [CrossRef]
- Landau, R.; Auslander, G.K.; Werner, S.; Shoval, N.; Heinik, J. Who should make the decision on the use of GPS for people with dementia? Aging Ment. Health 2011, 15, 78–84. [Google Scholar] [CrossRef]
- Landau, R.; Werner, S.; Auslander, G.K.; Shoval, N.; Heinik, J. Attitudes of Family and Professional Care-Givers towards the Use of GPS for Tracking Patients with Dementia: An Exploratory Study. Br. J. Soc. Work 2009, 39, 670–692. [Google Scholar] [CrossRef]
- Lindqvist, E.; Nygard, L.; Borell, L. Significant junctures on the way towards becoming a user of assistive technology in Alzheimer’s disease. Scand. J. Occup. Ther. 2013, 20, 386–396. [Google Scholar] [CrossRef]
- Lundberg, S. The results from a two-year case study of an information and communication technology support system for family caregivers. Disabil. Rehabil. Assist. Technol. 2014, 9, 353–358. [Google Scholar] [CrossRef]
- Mao, H.F.; Chang, L.H.; Yao, G.; Chen, W.Y.; Huang, W.N.W. Indicators of perceived useful dementia care assistive technology: Caregivers’ perspectives. Geriatr. Gerontol. Int. 2015, 15, 1049–1057. [Google Scholar] [CrossRef]
- McCabe, L.; Innes, A. Supporting safe walking for people with dementia: User participation in the development of new technology. Gerontechnology 2013, 12, 4–15. [Google Scholar] [CrossRef]
- Mehrabian, S.; Extra, J.; Wu, Y.H.; Pino, M.; Traykov, L.; Rigaud, A.S. The perceptions of cognitively impaired patients and their caregivers of a home telecare system. J. Med. Device. 2015, 8, 21–29. [Google Scholar] [CrossRef]
- Meiland, F.J.M.; Bouman, A.I.E.; Sävenstedt, S.; Bentvelzen, S.; Davies, R.J.; Mulvenna, M.D.; Nugent, C.D.; Moelaert, F.; Hettinga, M.E.; Bengtsson, J.E.; et al. Usability of a new electronic assistive device for community-dwelling persons with mild dementia. Aging Ment. Health 2012, 16, 584–591. [Google Scholar] [CrossRef]
- Mulvenna, M.; Hutton, A.; Coates, V.; Martin, S.; Todd, S.; Bond, R.; Moorhead, A. Views of caregivers on the ethics of assistive technology used for home surveillance of people living with dementia. Neuroethics 2017. [Google Scholar] [CrossRef]
- Nauha, L.; Keranen, N.S.; Kangas, M.; Jamsa, T.; Reponen, J. Assistive technologies at home for people with a memory disorder. Dementia 2016. [Google Scholar] [CrossRef]
- Newton, L.; Dickinson, C.; Gibson, G.; Brittain, K.; Robinson, L. Exploring the views of GPs, people with dementia and their carers on assistive technology: A qualitative study. BMJ Open 2016, 6, 7. [Google Scholar] [CrossRef]
- Nijhof, N.; van Gemert-Pijnen, J.E.W.C.; Burns, C.M.; Seydel, E.R. A personal assistant for dementia to stay at home safe at reduced cost. Gerontechnology 2013a, 11, 469–479. [Google Scholar] [CrossRef]
- Olsson, A.; Skovdahl, K.; Engstrom, M. Using diffusion of innovation theory to describe perceptions of a passive positioning alarm among persons with mild dementia: A repeated interview study. BMC Geriatr. 2016, 16, 6. [Google Scholar] [CrossRef]
- Pakrasi, S.; Burmeister, O.K.; Coppola, J.F.; McCallum, T.J.; Loeb, G. Ethical telehealth design for users with dementia. Gerontechnology 2015, 13, 383–387. [Google Scholar] [CrossRef][Green Version]
- Pilotto, A.; D’Onofrio, G.; Benelli, E.; Zanesco, A.; Cabello, A.; Margeli, M.C.; Wanche-Politis, S.; Seferis, K.; Sancarlo, D.; Kilias, D.; et al. Information and Communication Technology Systems to Improve Quality of Life and Safety of Alzheimer’s Disease Patients: A Multicenter International Survey. J. Alzheimers Dis. 2011, 23, 131–141. [Google Scholar] [CrossRef]
- Pino, M.; Boulay, M.; Jouen, F.; Rigaud, A.S. “Are we ready for robots that care for us?” Attitudes and opinions of older adults toward socially assistive robots. Front. Aging Neurosci. 2015, 7, 15. [Google Scholar] [CrossRef]
- Pot, A.M.; Blom, M.M.; Willemse, B.M. Acceptability of a guided self-help Internet intervention for family caregivers: Mastery over dementia. Int. Psychogeriatr. 2015, 27, 1343–1354. [Google Scholar] [CrossRef]
- Pot, A.M.; Willemse, B.M.; Horjus, S. A pilot study on the use of tracking technology: Feasibility, acceptability, and benefits for people in early stages of dementia and their informal caregivers. Aging & mental health 2012, 16, 127–134. [Google Scholar] [CrossRef]
- Powell, J.; Gunn, L.; Lowe, P.; Sheehan, B.; Griffiths, F.; Clarke, A. New networked technologies and carers of people with dementia: An interview study. Ageing Soc. 2010, 30, 1073–1088. [Google Scholar] [CrossRef]
- Riikonen, M.; Mäkelä, K.; Perälä, S. Safety and monitoring technologies for the homes of people with dementia. Gerontechnology 2010, 9, 32–45. [Google Scholar] [CrossRef]
- Robinson, L.; Hutchings, D.; Corner, L.; Finch, T.; Hughes, J.; Brittain, K.; Bond, J. Balancing rights and risks: Conflicting perspectives in the management of wandering in dementia. Health Risk Soc. 2007, 9, 389–406. [Google Scholar] [CrossRef]
- Rosenberg, L.; Kottorp, A.; Nygard, L. Readiness for Technology Use With People With Dementia: The Perspectives of Significant Others. J. Appl. Gerontol. 2012, 31, 510–530. [Google Scholar] [CrossRef]
- Schaller, S.; Marinova-Schmidt, V.; Setzer, M.; Kondylakis, H.; Griebel, L.; Sedlmayr, M.; Graessel, E.; Maler, J.M.; Kirn, S.; Kolominsky-Rabas, P.L. Usefulness of a Tailored eHealth Service for Informal Caregivers and Professionals in the Dementia Treatment and Care Setting: The eHealthMonitor Dementia Portal. JMIR RES. Protoc. 2016, 5, 18. [Google Scholar] [CrossRef]
- Solli, H.; Hvalvik, S.; Bjørk, I.T.; Hellesø, R. Characteristics of the relationship that develops from nurse-caregiver communication during telecare. J. Clin. Nurs. 2015, 24, 1995–2004. [Google Scholar] [CrossRef] [PubMed]
- Torkamani, M.; McDonald, L.; Saez Aguayo, I.; Kanios, C.; Katsanou, M.N.; Madeley, L.; Limousin, P.D.; Lees, A.J.; Haritou, M.; Jahanshahi, M. A randomized controlled pilot study to evaluate a technology platform for the assisted living of people with dementia and their carers. J. Alzheimers Dis. 2014, 41, 515–523. [Google Scholar] [CrossRef]
- White, E.B.; Montgomery, P. Electronic tracking for people with dementia: An exploratory study of the ethical issues experienced by carers in making decisions about usage. Dement. Int. J. Soc. Res. Pract. 2014, 13, 216–232. [Google Scholar] [CrossRef] [PubMed]
- Wilz, G.; Soellner, R. Evaluation of a short-term telephone-based cognitive behavioral intervention for dementia family caregivers. Clin. Gerontol. 2016, 39, 25–47. [Google Scholar] [CrossRef]
- Peek, S.T.M.; Luijkx, K.G.; Vrijhoef, H.J.M.; Nieboer, M.E.; Aarts, S.; van der Voort, C.S.; Rijnaard, M.D.; Wouters, E.J.M. Origins and consequences of technology acquirement by independent-living seniors: Towards an integrative model. BMC Geriatr. 2017, 17, 189. [Google Scholar] [CrossRef]
- Olsson, A.; Persson, A.C.; Bartfai, A.; Boman, I.L. Sensor technology more than a support. Scand. J. Occup. Ther. 2017. [Google Scholar] [CrossRef] [PubMed]
- Nijhof, N. eHealth for people with dementia in home-based and residential care. PhD Thesis, University of Twente, Enschede, The Netherlands, 2013. [Google Scholar]
- Nijhof, N.; van Hoof, J.; Blom, M.M.; van Gemert-Pijnen, J.E.W.C. Smart Living in Dementia Care. In Handbook of Smart Homes, Health Care and Well-Being; van Hoof, J., Demiris, G., Wouters, E.J.M., Eds.; Springer International Publishing: Cham, Schwitzerland, 2014; pp. 1–8. [Google Scholar]
- Janevic, M.R.; Connell, C.M. Racial, ethnic, and cultural differences in the dementia caregiving experience: Recent findings. Gerontologist 2001, 41, 334–347. [Google Scholar] [CrossRef]
- Tsekleves, E.; Bingley, A.F.; Lujan Escalante, M.A.; Gradinar, A. Engaging people with dementia in designing playful and creative practices: Co-design or co-creation? Dementia 2018. [Google Scholar] [CrossRef] [PubMed]
- Brankaert, R.G.A.B. Design for dementia: A design-driven living lab approach to involve people with dementia and their context. Ph.D Thesis, Eindhoven University of Technology, Eindhoven, The Netherlands, 2016. [Google Scholar]
- Roelofs, T.S.M.; Luijkx, K.G.; Embregts, P. A person-centered approach to study intimacy and sexuality in residential care facility (RCF) clients with dementia: Methodological considerations and a guide to study design. NeuroRehabilitation 2017, 41, 359–373. [Google Scholar] [CrossRef]


{kind=link}
| 1. Stakeholder perspective | |
| Stakeholder(s) | Organization(s) |
| General practitioner(s) | Client(s) |
| Caregiver(s) | Patient(s) |
| Care professional(s) | Elderly |
| Supplier(s) | Elderly people |
| Provider(s) | Older people |
| Management | Different perspectives |
| Manager(s) | |
| 2. Technology | |
| Ehealth/e-health | Telemedicine/tele-medicine |
| mhealth/m-health | Assistive technology |
| Robotics | Assisted living |
| Robotic technology | Technology acceptance |
| Sensor-based networks | Technology adoptation |
| Domotics | Tele-monitoring/telemonitoring |
| Smart home(s) | Electronic tracking |
| Home automation | Sensor technology |
| Care technology | Gero(n)technology |
| Telecare/tele-care | |
| 3. Dementia | |
| Dementia | Alzheimer’s disease |
| Alzheimer | Alzheimers disease |
| Inclusion Criteria |
|
| Exclusion Criteria |
|
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Boekel, L.C.; Wouters, E.J.M.; Grimberg, B.M.; van der Meer, N.J.M.; Luijkx, K.G. Perspectives of Stakeholders on Technology Use in the Care of Community-Living Older Adults with Dementia: A Systematic Literature Review. Healthcare 2019, 7, 73. https://doi.org/10.3390/healthcare7020073
van Boekel LC, Wouters EJM, Grimberg BM, van der Meer NJM, Luijkx KG. Perspectives of Stakeholders on Technology Use in the Care of Community-Living Older Adults with Dementia: A Systematic Literature Review. Healthcare. 2019; 7(2):73. https://doi.org/10.3390/healthcare7020073
Chicago/Turabian Stylevan Boekel, Leonieke C., Eveline J.M. Wouters, Bea M. Grimberg, Nardo J.M. van der Meer, and Katrien G. Luijkx. 2019. "Perspectives of Stakeholders on Technology Use in the Care of Community-Living Older Adults with Dementia: A Systematic Literature Review" Healthcare 7, no. 2: 73. https://doi.org/10.3390/healthcare7020073
APA Stylevan Boekel, L. C., Wouters, E. J. M., Grimberg, B. M., van der Meer, N. J. M., & Luijkx, K. G. (2019). Perspectives of Stakeholders on Technology Use in the Care of Community-Living Older Adults with Dementia: A Systematic Literature Review. Healthcare, 7(2), 73. https://doi.org/10.3390/healthcare7020073