The Role of Preference on Outcomes of People Receiving Evidence-Informed Community Wound Care in Their Home or in a Nurse-Clinic Setting: A Cohort Study (n = 230)

Abstract
:1. Introduction
2. Experimental Section
2.1. Design
2.2. Setting and Sample
2.3. Procedures
2.4. Data Collection and Management
2.5. Outcome Measurement
2.6. Analyses
3. Results
3.1. Individual’s Satisfaction with Care
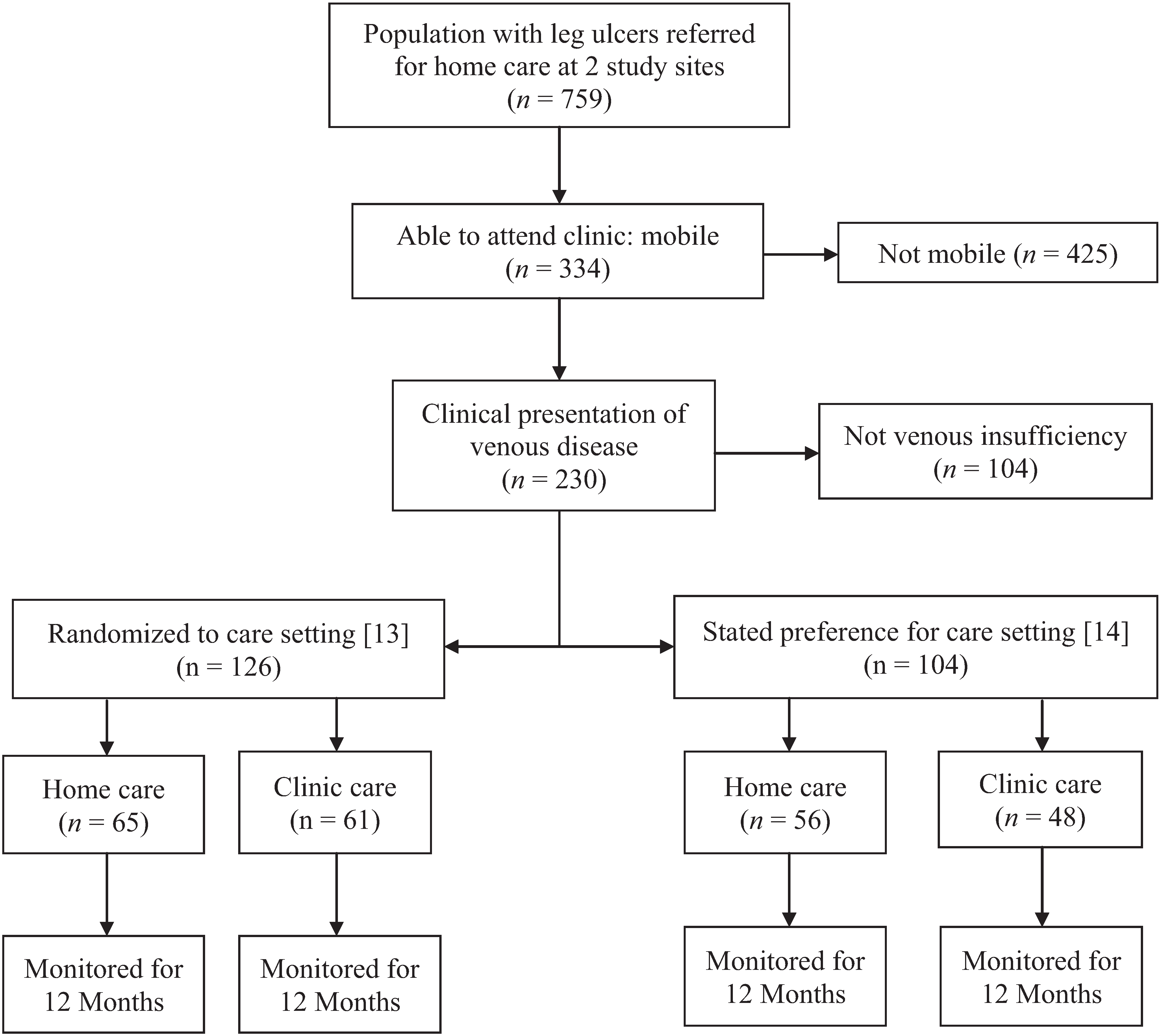

{kind=link}
{kind=link}
{kind=link}
| Characteristics 1 | TOTAL (n = 230) | ALLOCATED Care Setting (n = 126) | CHOICE of Care Setting (n = 104) | p-Value |
|---|---|---|---|---|
| Setting of Care | ||||
| ○ Home | 121 (52.6) | 65 (51.6) | 56 (53.8) | 0.79 |
| ○ Clinic | 109 (47.4) | 61 (48.4) | 48 (46.2) | |
| Etiology of leg Ulcer | ||||
| ○ Venous | 154 (67.0) | 86 (68.3) | 68 (65.4) | 0.67 |
| ○ Mixed | 76 (33.0) | 40 (31.7) | 36 (34.6) | |
| Gender-Female | 118 (51.3) | 71 (56.3) | 47 (45.2) | 0.11 |
| Language-English | 193 (83.9) | 106 (84.1) | 87 (83.7) | 0.99 |
| Living Alone | 87 (37.8) | 54 (42.9) | 33 (31.7) | 0.10 |
| Independently Mobile | 167 (72.9) | 89 (71.2) | 78 (75.0) | 0.55 |
| Ulcer Duration | ||||
| ○ ≤3 Months | 129 (56.1) | 73 (57.9) | 56 (53.8) | 0.30 |
| ○ >3 to ≤12 Months | 68 (29.6) | 39 (31.0) | 29 (27.9) | |
| ○ > 12 Months | 33 (14.3) | 14 (11.1) | 19 (18.3) | |
| Ulcer Size | ||||
| ○ ≤2.5 cm² | 124 (53.9) | 69 (54.8) | 55 (52.9) | 0.66 |
| ○ 2.5 to ≤10 cm² | 61 (26.5) | 35 (27.8) | 26 (25.0) | |
| ○ >10 cm² | 45 (19.6) | 22 (17.5) | 23 (22.1) | |
| Previous Ulceration (yes) | 116 (50.4) | 62 (49.2) | 54 (51.9) | 0.69 |
| Ulcer Size (cm2) † | 2.4 [0.98/6.7] | 2.3 [1.1/5.8] | 2.4 [0.82/9.0] | 1.00 2 |
| Diathesis in years † | 7 [3/12] | 8 [3/16] | 5 [2.5/9.0] | 0.05 2 |
| Duration at initial assessment in weeks † | 11.4 [4.6/24] | 10.6 [4.7/22.7] | 12.1 [4.4/30.6] | 0.73 2 |
| ABPI † | 1.07 [0.99/1.16] | 1.06 [0.98/1.14] | 1.08 [1.00/1.20] | 0.06 2 |
| Age (years) * | 68.0 (14.2) | 68.5 (14.1) | 67.5 (14.5) | 0.62 |
| SF12 Scores * | ||||
| ○ Mental Component | 49.4 (11.1) | 49.7 (11.0) | 49.0 (11.3) | 0.64 |
| ○ Physical Component | 35.7 (10.1) | 35.1 (9.9) | 36.4 (10.4) | 0.36 |
| Clinical Care 3 | ||||
| ABPI completed | 223 (97.0) | 122 (96.8) | 101 (97.1) | 1.00 |
| Compression Therapy | ||||
| ○ All | 208 (91.2) | 118 (94.4) | 90 (87.4) | 0.10 |
| ○ Venous disease | 143 (94.1) | 82 (96.5) | 61 (91.0) | 0.18 |
| ○ Mixed disease | 65 (85.5) | 36 (90.0) | 29 (80.6) | 0.33 |
| Characteristic 1 | ALLOCATED Group (n = 102) | CHOICE Group (n = 80) | p-value |
|---|---|---|---|
| n (%) | n (%) | ||
| ISSUES (n = 182) | |||
| Some problems walking about | 54 (52.9) | 39 (48.8) | 0.65 |
| Some problems with washing, dressing self | 16 (15.7) | 14 (17.5) | 0.84 |
| Some problems performing my usual activities | 50 (49.0) | 44 (55.7) | 0.48 |
| Not anxious or depressed | 74 (72.5) | 56 (70.0) | 0.27 |
| EuroQol EQ-5D Index † | 0.77 [0.70/0.84] | 0.77 [0.71/0.84] | 0.77 2 |
| ALLOCATED Group (n = 97) | CHOICE Group (n = 80) | ||
| CARE AND SERVICE SURVEY ( n = 177) | |||
| Wait Time | |||
| ▪ Less than 30 min | 86 (88.7) | 72 (91.1) | 0.43 |
| ▪ Waiting 30 min–1 h | 9 (9.3) | 7 (8.9) | |
| ▪ Waiting 1–2 h | 2 (2.1) | 0 (0.0) | |
| Knows the name of the nurse who takes care of leg ulcer most of the time | 72 (74.2) | 69 (86.2) | 0.06 |
| Very/quite satisfied with information nurse provided for how to care for leg ulcer | 94 (96.9) | 78 (97.5) | 0.65 |
| Very/quite satisfied with information nurse provided for leg ulcer prevention | 83 (85.6) | 69 (87.3) | 0.74 |
| Very/quite Satisfied with nurses’ skill | 91 (94.8) | 78 (97.5) | 0.41 |
| Comfortable with bandages and dressings used for treatment | 55 (62.5) | 53 (69.7) | 0.41 |
| Very/quite Satisfied with treatment last 12 weeks | 88 (93.6) | 74 (96.1) | 0.67 |
| Recommend/highly recommend care you receive to others | 86 (92.5) | 75 (94.9) | 0.55 |
| Overall rating of the nursing care (1 = Poor to 10 = Excellent) † | 10 [9/10] | 10 [10/10] | 0.26 2 |
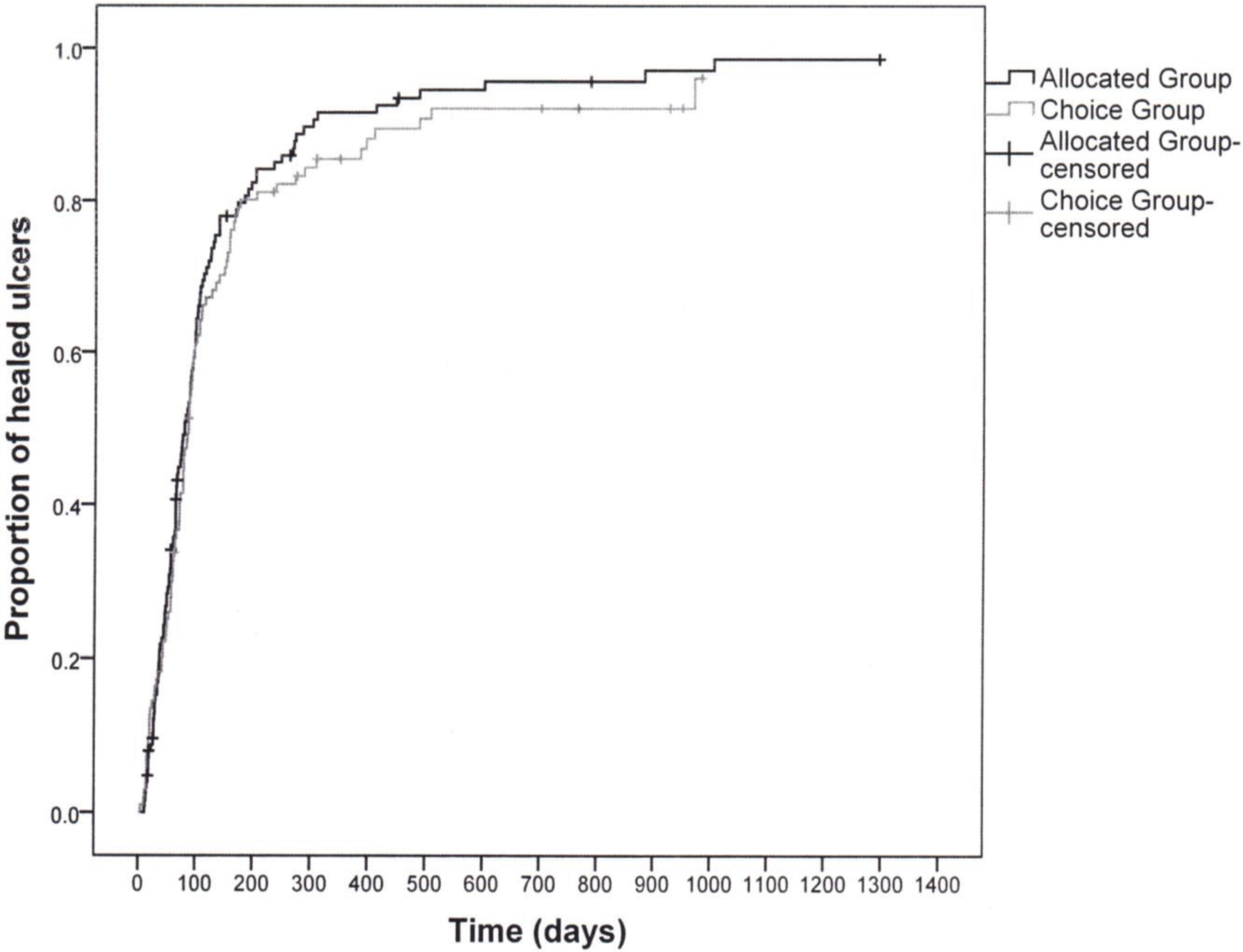
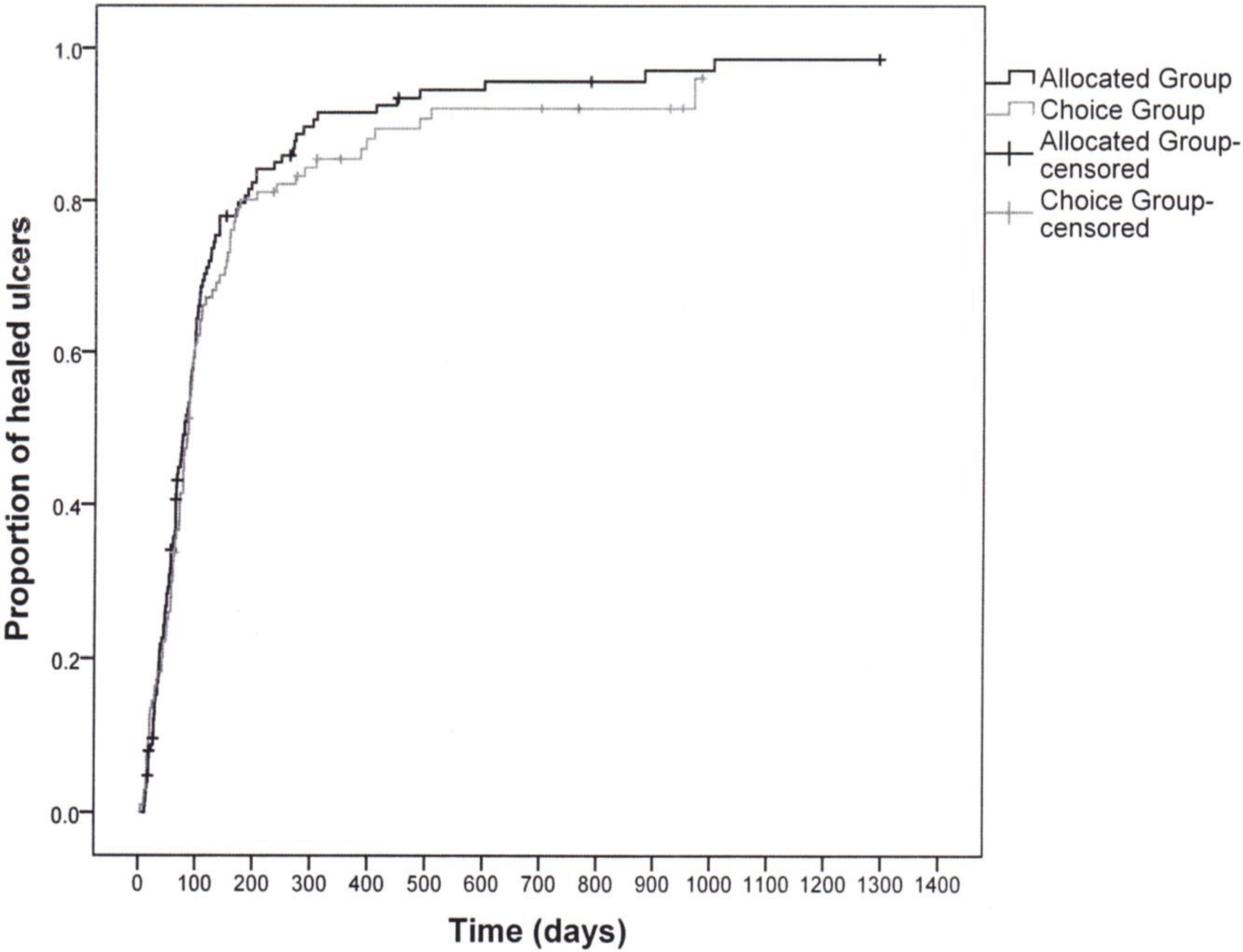
3.2. Healing
3.3. Pain and Health Related Quality of Life
| Outcome 1 | ALLOCATED Care Setting (n = 126) | CHOICE of Care Setting (n = 104) | p-Value |
|---|---|---|---|
| n (%) | n (%) | ||
| Healing 2 | |||
| ○ 3-month (≤91 days) | 69 (57.5) | 58 (56.9) | 1.00 |
| ○ Recurrence rate in one year 3 | 29 (25.2) | 18 (19.4) | 0.40 |
| Pain at 3 Months | |||
| ○ No pain | 58 (57.4) | 49 (59.8) | 0.94 |
| ○ Mild/Discomfort | 32 (31.7) | 24 (29.3) | |
| ○ Distressing/horrible/excruciating | 11 (10.9) | 9 (11.0) | |
| SF12 Scores at 3 Months * | |||
| ○ Mental Component | 52.8 (10.4) | 52.5 (11.1) | 0.85 |
| ○ Physical Component | 39.0 (11.3) | 40.1 (12.4) | 0.55 |
| General Health Assessment | |||
| ○ Excellent or Very Good | 29 (29.3) | 26 (32.5) | 0.32 |
| ○ Good | 39 (39.4) | 37 (46.2) | |
| ○ Fair or Poor | 31 (31.3) | 17 (21.2) | |
| Resource Utilization for an Episode of Leg Ulcer Care 4 | |||
| ○ Number of Nursing Visits † | 23 [12/48] | 25 [14/51] | 0.40 |
| ○ Weeks on Service † | 13 [7/24] | 14 [8/27] | 0.38 |
| ○ Visits per Week † | 2 [1.6/2.3] | 2 [1.7/2.5] | 0.34 |
| ○ Nursing Costs † | $1135 [612/2347] | $1283 [698/2556] | 0.33 |
| ○ Cost of Wound Supplies † | $531 [251/1115] | $545 [191/1163] | 0.97 |
4. Discussion
5. Limitations of the Study
6. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Cullum, N.; Nelson, E.A.; Fletcher, A.W.; Sheldon, T.A. Compression for venous leg ulcers. Cochrane Database Syst. Rev. 2000. [Google Scholar] [CrossRef]
- Harrison, M.B.; VanDenKerkhof, E.G.; Hopman, W.M.; Graham, I.D.; Carley, M.E.; Nelson, E.A. The Canadian Bandaging Trial: Evidence-informed leg ulcer care and the effectiveness of two compression technologies. BMC Nurs. 2011, 10, e20. [Google Scholar] [CrossRef]
- National Health Services Centre for Reviews and Dissemination. Compression therapy for venous leg ulcers. Eff. Health Care Bull. 1997, 3, 1–12. [Google Scholar]
- Nelson, E.A.; Iglesias, C.P.; Cullum, N.; Torgerson, D.J. Randomized clinical trial of four-layer and short-stretch compression bandages for venous leg ulcers (VenUS I). Br. J. Surg. 2004, 91, 1292–1299. [Google Scholar] [CrossRef] [PubMed]
- Castineira, F.; Fisher, H.; Coleman, D.; Grace, P.A.; Burke, P. The limerick leg ulcer project: Early results. Ir. J. Med. Sci. 1999, 168, 17–20. [Google Scholar] [CrossRef] [PubMed]
- Lambourne, L.A.; Moffatt, C.J.; Jones, A.C.; Dorman, M.C.; Franks, P.J. Clinical audit and effective change in leg ulcer services. J. Wound Care 1996, 5, 348–351. [Google Scholar] [PubMed]
- Moffatt, C.J.; Franks, P.J.; Oldroyd, M.; Bosanquet, N.; Brown, P.; Greenhalgh, R.M.; McCollum, C.N. Community clinics for leg ulcers and impact on healing. Br. Med. J. 1992, 305, 1389–1392. [Google Scholar] [CrossRef]
- Moffatt, C.J.; Oldroyd, M.I. A pioneering service to the community. The Riverside Community Leg Ulcer Project. Prof. Nurse 1994, 9, 486, 488, 490 passim. [Google Scholar]
- Morrell, C.J.; Walters, S.J.; Dixon, S. Cost effectiveness of community leg ulcer clinics: Randomised controlled trial. Br. Med. J. 1998, 316, 1487–1491. [Google Scholar] [CrossRef]
- Scriven, J.M.; Hartshorne, T.; Bell, P.R.F.; Naylor, A.R.; London, N.J.M. Single-visit venous ulcer assessment clinic: The first year. Br. J. Surg. 1997, 84, 334–336. [Google Scholar] [CrossRef] [PubMed]
- Simon, D.A.; Freak, L.; Kinsella, A. Community leg ulcer clinics: A comparative study in two health authorities. Br. Med. J. 1996, 312, 1648–1651. [Google Scholar] [CrossRef]
- Stevens, J.; Franks, P.; Harrington, M. A community/hospital leg ulcer service. J. Wound Care 1997, 6, 62–68. [Google Scholar] [PubMed]
- Harrison, M.B.; Graham, I.D.; Lorimer, K.; VanDenKerkhof, E.; Buchanan, M.; Wells, P.; Brandys, T.; Pierscianowski, T. Nurse clinic versus home delivery of evidence-based community leg ulcer care: A randomized health services trial. BMC Health Serv. Res. 2008, 8, e243. [Google Scholar] [CrossRef]
- Harrison, M.B.; VanDenKerkhof, E.; Hopman, W.M.; Graham, I.D.; Lorimer, K.; Carley, M. Evidence-informed leg ulcer care: A cohort study comparing outcomes of individuals choosing nurse-led clinic or home care. Ostomy Wound Manage. 2011, 57, 38–45. [Google Scholar] [PubMed]
- Graham, I.D.; Harrison, M.D.; Brouwers, M. Evaluating and adapting practice guidelines for local use: A conceptual framework. In Clinical Governance in Practice; Pickering, S., Thompson, J., Eds.; Harcourt Publishers: London, UK, 2003; pp. 213–229. [Google Scholar]
- Graham, I.D.; Lorimer, K.; Harrison, M.B.; Pierscianowski, T. Evaluating the quality of international clinical practice guidelines for leg ulcers: Preparing for a Canadian adaptation. Can. Assoc. Enterostomal Ther. J. 2000, 19, 15–31. [Google Scholar]
- Graham, I.D.; Harrison, M.B. Evaluation and adaptation of clinical practice guidelines. Evid. Based Nurs. 2005, 8, 68–72. [Google Scholar] [CrossRef] [PubMed]
- Graham, I.D.; Harrison, M.B.; Shafey, M.; Keast, D. Knowledge and attitudes regarding care of leg ulcers. Survey of family physicians. Can. Fam. Physician 2003, 49, 896–902. [Google Scholar]
- Graham, I.D.; Harrison, M.B.; Moffat, C.; Franks, P. Leg ulcer care: Nursing attitudes and knowledge. Can. Nurse 2001, 97, 19–24. [Google Scholar] [PubMed]
- Graham, I.D.; Harrison, M.B.; Lorimer, K. Adapting national and international leg ulcer practice guidelines for local use: The Ontario Leg Ulcer Community Care Protocol. Adv. Skin Wound Care 2005, 18, 307–318. [Google Scholar] [CrossRef] [PubMed]
- Gilliss, C.L.; Kulkin, I.L. Monitoring nursing interventions and data collection in a randomized clinical trial. West. J. Nurs. Res. 1991, 13, 416–422. [Google Scholar] [CrossRef] [PubMed]
- Kirchhoff, K.T.; Dille, C.A. Issues in intervention research: Maintaining integrity. Appl. Nurs. Res. 1994, 7, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Rabeneck, L.; Viscoli, C.M.; Horwitz, R.I. Problems in the conduct and analysis of randomized clinical trials. Are we getting the right answers to the wrong questions? Arch. Intern. Med. 1992, 152, 507–512. [Google Scholar] [CrossRef] [PubMed]
- Nemeth, K.A.; Graham, I.D.; Harrison, M.B. The measurement of leg ulcer pain: Identification and appraisal of pain assessment tools. Adv. Skin Wound Care 2003, 16, 260–267. [Google Scholar] [CrossRef] [PubMed]
- Nemeth, K.A.; Harrison, M.B.; Graham, I.D.; Burke, S. Pain in pure and mixed aetiology venous leg ulcers: A three-phase point prevalence study. J. Wound Care 2003, 12, 336–340. [Google Scholar] [CrossRef] [PubMed]
- Walters, S.J.; Morell, C.J.; Dixon, S. Measuring health-related quality of life in patients with venous leg ulcers. Qual. Life Res. 1999, 8, 327–336. [Google Scholar] [CrossRef] [PubMed]
- Melzack, R. The McGill Pain Questionnaire: Major properties and scoring methods. Pain 1975, 1, 277–299. [Google Scholar] [CrossRef] [PubMed]
- Melzack, R.; Katz, J. The McGill Pain Questionnaire: Appraisal and current status. In Handbook of Pain Assessment; Guilford Press: New York, NY, USA, 1992; pp. 152–168. [Google Scholar]
- Melzack, R. The short-form McGill Pain Questionnaire. Pain 1987, 30, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.E.; Kosinski, M.; Keller, S.D. SF-12: How to Score the SF-12 Physical and Mental Health Summary Scales, 2nd ed.; The Health Institute, New England Medical Centre: Boston, MA, USA, 1995. [Google Scholar]
- Hopman, W.M.; Towheed, T.; Anastassiades, T. Canadian normative data for the SF-36 health survey. Can. Med. Assoc. J. 2000, 163, 265–271. [Google Scholar]
- The EuroQol Group. EuroQol—A new facility for the measurement of health-related quality of life. Health Policy 1990, 16, 199–208.
- Brooks, R. EuroQol: The current state of play. Health Policy 1996, 37, 53–72. [Google Scholar] [CrossRef] [PubMed]
- Bansback, N.; Tsuchiya, A.; Brazier, J.; Anis, A. Canadian valuation of EQ-5D health states: Preliminary value set and considerations for future valuation studies. PLoS One 2012, 7, e31115. [Google Scholar] [CrossRef] [PubMed]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Harrison, M.B.; VanDenKerkhof, E.G.; Hopman, W.M.; Carley, M.E. The Role of Preference on Outcomes of People Receiving Evidence-Informed Community Wound Care in Their Home or in a Nurse-Clinic Setting: A Cohort Study (n = 230). Healthcare 2014, 2, 401-416. https://doi.org/10.3390/healthcare2030401
Harrison MB, VanDenKerkhof EG, Hopman WM, Carley ME. The Role of Preference on Outcomes of People Receiving Evidence-Informed Community Wound Care in Their Home or in a Nurse-Clinic Setting: A Cohort Study (n = 230). Healthcare. 2014; 2(3):401-416. https://doi.org/10.3390/healthcare2030401
Chicago/Turabian StyleHarrison, Margaret B., Elizabeth G. VanDenKerkhof, Wilma M. Hopman, and Meg E. Carley. 2014. "The Role of Preference on Outcomes of People Receiving Evidence-Informed Community Wound Care in Their Home or in a Nurse-Clinic Setting: A Cohort Study (n = 230)" Healthcare 2, no. 3: 401-416. https://doi.org/10.3390/healthcare2030401
APA StyleHarrison, M. B., VanDenKerkhof, E. G., Hopman, W. M., & Carley, M. E. (2014). The Role of Preference on Outcomes of People Receiving Evidence-Informed Community Wound Care in Their Home or in a Nurse-Clinic Setting: A Cohort Study (n = 230). Healthcare, 2(3), 401-416. https://doi.org/10.3390/healthcare2030401