Abstract
Background/Objectives: Exercise has gained attention as a potentially beneficial non-pharmacological intervention, but whether this type of intervention presents a higher dropout rate compared to other interventions is still unknown. This systematic review, with a meta-analysis of randomized controlled trials, aims to determine whether exercise or comparators present lower or higher attrition in patients with migraine. Methods: A search was conducted in PubMed, Scopus, Web of Science, and Cochrane Library until March 2025. The methodological quality was evaluated using the JBI scale for randomized trials. Proportion meta-analysis calculated the dropout rate. Results: Odds ratio meta-analysis under 1 indicated lower attrition in experimental participants. Subgroup meta-analyses sorted by type of exercise, control, and migraine were conducted to explore variability in results based on the mentioned moderators. The overall pooled dropout rate was 6.7%, 11.6% for the exercise groups, and 10.1% for the comparators. No statistical difference was found between groups of studies, type of migraine, type of exercise, and type of comparator (p ≥ 0.05). Only the odds ratio results for migraine with auras showed a lower pooled dropout rate in favor of control participants, OR = 1.18. Conclusions: Although there is no statistically significant difference, the meta-analysis of proportions shows a higher loss rate in exercise-based interventions. However, the high heterogeneity found in the included studies prevents us from drawing firm conclusions. Furthermore, adequate adherence to the CONSORT guidelines in reporting losses and their reasons could help design appropriate retention strategies for studies and interventions based on exercise in patients with migraines.
1. Introduction
Globally, migraine is recognized as the sixth most significant and disabling condition that people experience throughout their lives, becoming a barrier in various aspects of daily life [1]. According to the World Health Organization (WHO), migraine is a primary headache disorder, typically episodic, lasting between 4 and 72 h. It is often accompanied by nausea, vomiting, and/or sensitivity to light (photophobia) and sound (phonophobia). In some cases, it is preceded by a short-duration aura consisting of unilateral, reversible visual, sensory, or other symptoms [2].
Nowadays, there are plenty of pharmacological options available for migraineurs, but at the same time, patients’ lack of adherence to the use of prophylactic medicines cannot be denied [3]. The limited availability of effective treatment options for managing migraines highlights the fact that there is still much we do not understand about the underlying causes and mechanisms of this condition. However, recent research highlights the effectiveness of non-pharmacological approaches in managing migraine attacks and controlling pain [4].
Exercise is one of the popular approaches for controlling chronic pain situations and common pathologies like sleeping disorders or psychological problems [4]. Considering the benefits of this intervention, it can be chosen as a non-pharmacological treatment for migraines. Nevertheless, contrary to all the points mentioned, there are some migraine patients who report an increase in their headaches after starting regular physical activity following exercise protocols [3]. This has led to physical inactivity, inability to engage in physical movement, and prolonged sedentary behavior becoming common symptoms among individuals affected by this pathology [5]. Migraine is a complex neurological disorder involving both peripheral and central sensitization mechanisms. Peripherally, the activation of the trigeminovascular system leads to the release of vasoactive neuropeptides and neurogenic inflammation. Centrally, brainstem dysfunction alters descending pain modulation. Exercise may influence these mechanisms by inhibiting nociceptive input at the spinal dorsal horn and enhancing central pain inhibitory pathways [6,7]. Moreover, physical activity patterns vary across migraine phases, with marked hypoactivity during attacks, suggesting that structured interventions should be phase-adapted [8]. Given the heterogeneity of migraine, with variability in attack frequency, aura, treatment response, and comorbidities, a multimodal and individualized approach is increasingly recommended. Recent studies support the role of slow aerobic exercise and physiotherapy in reducing symptom burden and enhancing neural mechanisms involved in pain modulation, such as insular and cingulate connectivity [9,10]. All these findings strengthen the rationale for integrating tailored exercise into migraine care.
Despite the potential benefits of exercise in reducing migraine frequency and intensity, adherence to exercise programs among individuals with migraines remains highly controversial. While some studies support the hypothesis that exercise can serve as a protective factor and a preventive approach to migraine attacks, others indicate that it may act as a trigger, exacerbating symptoms in certain individuals [3]. This dual effect contributes to the inconsistency in adherence levels, as patients may either benefit from exercise as a long-term management strategy or avoid it out of fear of worsening their symptoms [11].
Despite growing evidence supporting the benefits of exercise in migraine management, there is a lack of clarity regarding adherence to such interventions, particularly concerning dropout rates and their underlying causes. Understanding these patterns is critical, as dropout can limit the effectiveness and real-world applicability of exercise-based treatments. This systematic review aims to answer the following research question: What is the overall dropout rate in randomized controlled trials involving exercise interventions for migraine, and how does it compare with control interventions? Based on the previous literature, we hypothesize that exercise-based interventions may present slightly higher dropout rates, potentially due to the paradoxical effects of physical activity acting as both a therapeutic tool and a symptom trigger in certain individuals. Considering the previous information and the importance of different exercise protocols in controlling migraine pain and also the lack of systematic reviews with the aim of analyzing the reasons behind the dropouts that happen among the participants in exercise protocols to control migraine pain, we propose a systematic review of randomized clinical trials that use various exercise protocols as a non-medical intervention for this pathology, with the aim to meta-analyze the dropout rate in each and the reasons behind each one of them to know what the burdens on the way of migraineurs patients to use this type of intervention for treating their condition are.
2. Materials and Methods
2.1. Data Sources and Search Strategy
This systematic review was developed in accordance with the 2020 Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA 2020) statements [12]. The review protocol was registered in the OSF registry with DOI 10.17605/OSF.IO/NUHTQ. Two independent reviewers (ST and MDCV) conducted an independent systematic search in the different databases. A systematic search was conducted in the following databases: PubMed, Scopus, Web of Science, and Cochrane Library to identify studies analyzing the impact of different types of exercise on migraine or control in patients with migraines from the inception of databases to March 2025. No predefined filters were applied during the initial search, but specific keywords such as migraine, chronic migraine, episodic migraine, aerobics, and yoga, among others, were used to get more accurate results. Search terms were combined using Boolean operators such as AND or OR. The search strategy is shown in detail in Supplemental Material S1.
2.2. Research Question and Study Selection
The PICOS (Population, Intervention, Comparators, Outcomes, and Study Design) model was used to build the eligibility criteria for this systematic review [13].
The inclusion criteria were as follows:
P: Adult participant between 18 and 65 years old with any type of migraine;
I: Exercise interventions (e.g., aerobics, yoga, tai chi, relaxation, endurance, and strength, among others);
C: Any type of comparator, except those based on exercise;
O: Participants’ dropout;
S: Randomized clinical trials that report the dropout rate or number of participants who withdrew or studies that allow its indirect calculation.
The exclusion criteria were as follows:
- -
- Conference papers;
- -
- Dissertations.
2.3. Data Extraction and Quality Assessment
After the independent search, the same reviewers (ST and MDCV) carried out the screening and selection by title and abstract. Potential articles were managed using Mendeley desktop version 1.19.8, and duplicates were removed using this citation manager. In cases of disagreements, a third reviewer (CGM) was consulted. When a potential manuscript could not be accessed, or there were missing data, the corresponding authors were contacted. A list of excluded studies and their reasons is available in Supplementary Material S2.
Data of interest were recorded in a table of characteristics and an EXCEL spreadsheet for the meta-analysis. The extracted data were author, year, sample, participant characteristics (age, sex, type of migraine), experimental/control intervention description, overall retention rate, dropout rates by group, reasons for dropout, and adverse events.
The methodological quality of studies was assessed using the Joanne Brigs Institute tool (JBI) for randomized clinical trials [14]. This tool was designed for use in systematic reviews; it is also useful for critical appraisal of individual trials in clinical and research settings. Its application contributes to a better understanding of the available evidence and more informed decision-making in evidence-based practice. The JBI for randomized clinical trials is composed of 13 items that are scored as “yes”, “no”, “uncertain”, or “not applicable”. This scale is exempt from an overall score. The results were compiled in a table format.
In cases where data on dropout rates or reasons for withdrawal were not available in the included articles, the authors were contacted directly to gather the necessary information via e-mail. After the selection of studies, no corresponding author was contacted.
Certainty of evidence was assessed using the GRADE system. This system allows for the evaluation of five domains: (i) risk of bias, (ii) inconsistency, (iii) indirectness, (iv) imprecision, and (v) level of evidence. Randomized controlled trials begin with a “high” level of evidence, but domains could be downgraded.
2.4. Data Analysis
A participant was considered a dropout if he/she did not complete the study intervention or follow-up period following the randomization process. Comparisons between groups were conducted separately in a pairwise manner for studies that included more than two intervention groups.
For the quantitative analysis, R Studio software (version 4.1.2) was utilized, employing the metafor, meta, and dmetar packages [15,16,17]. All meta-analyses were performed using a random-effects model, assuming heterogeneity among the included randomized clinical trials. The corresponding forest plots illustrated the meta-analysis results. A proportion meta-analysis was conducted to estimate both the overall pooled dropout rate and the pooled dropout rate for each intervention group. Proportions were transformed using the logit transformation [18]. As some studies did not report dropout cases, a continuity correction of 0.5 was applied [19]. Additionally, a meta-analysis based on the odds ratio (OR) was performed to examine dropout patterns across intervention groups. An OR < 1 indicated a lower attrition rate among participants who received exercise training. To assess the effect measure, the 95% confidence interval (95% CI) was calculated, and data were adjusted using the inverse variance method for sparse data [20]. The restricted maximum likelihood estimator for Tau2 was employed to estimate between-study variance. Study heterogeneity was assessed using the I² statistic, with values exceeding 50% considered significantly high [21]. The OR meta-analysis was conducted to estimate both the overall pooled dropout rate and the dropout rate pattern for each intervention group.
Outliers were identified through sensitivity analysis, which included exploratory techniques generating Baujat, L’abbé, leave-one-out, and Influence plots. Studies detected as influential in sensitivity analysis and potentially introducing bias were excluded from the meta-analysis. Furthermore, publication bias was assessed using a contour-enhanced funnel plot, incorporating the trim-and-fill method for adjustment, alongside Egger’s tests for bias detection (presence of publication bias when p < 0.05) [22].
To identify how the type of migraine, type of exercise, and control comparator affected the overall pooled effects, subgroup meta-analyses displayed in forest plots were conducted.
3. Results
3.1. Study Selection and Methodological Quality Assessment
The initial search identified 389 potential articles in PubMed, Scopus, Web of Science, and Cochrane Library. After that, duplicate articles were removed automatically using the Mendeley software (v 1.19.8) (n = 73). After the screening by title and abstract, 27 potential reports were reviewed in full text. Supplementary Material S2 shows the 11 excluded reports and their reasons. Finally, 16 articles that met our inclusion criteria were selected [4,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37]. Figure 1 shows the PRISMA 2020 flowchart that describes the whole process of selection for this systematic review.
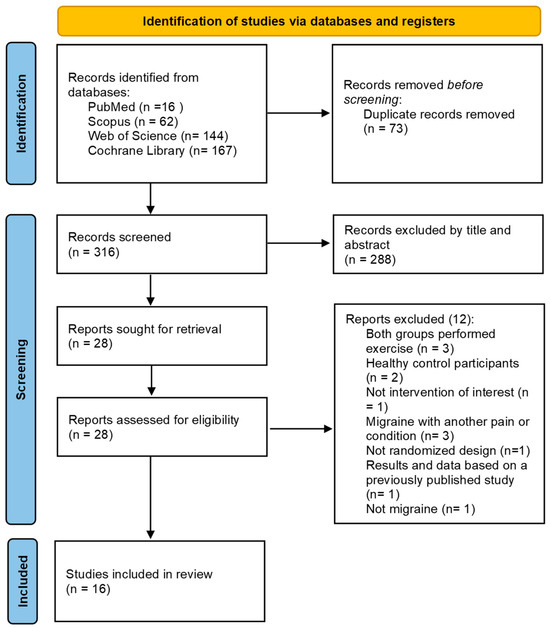
Figure 1.
PRISMA 2020 Flowchart [12].
Table 1 shows the methodological quality assessment of the included studies using the JBI scales for randomized controlled trials. All the included studies have unblinded participants and providers of the interventions. Also, most of the studies did not report whether the allocation of participants was concealed.

Table 1.
Quality assessment using JBI for randomized controlled trials.
3.2. Study Design and Population Characteristics
Table 2 shows the main key characteristics of the included and revised studies. All the articles focused on adults with migraines (episodic and chronic) as the target group and examined the impact of exercise on migraines or controlling parameters related to migraine symptoms. Across the 16 included randomized controlled trials [4,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37], a total of 1217 participants were analyzed (considering trials with two arms of interventions, but after the different interventions, a total of 174 participants withdrew from the studies due to various reasons such as dropout, non-compliance, or other external factors. The reason for dropout was only reported in 12 of 16 cases. Only three out of 16 of the included studies reported adverse events during the protocol of this study [24,31,37], but most of the trials did not report this information.
Table 2.
Main characteristics and data of interest from included studies.
A total of eight studies [23,25,26,27,28,29,30,37] (15 arms of intervention) based their intervention on aerobic exercise, one study [4](two arms) on strength exercise, six studies on yoga [24,32,33,34,35,36], and one on tai-chi [31]. In contrast, most of the participants in the control groups received usual care (n = 13), while one study offered dual-task interventions [4], one waitlist [25], one no intervention [31], and one out of 16 education programs [35].
3.3. Sensitivity Analysis
One study [24] was identified as an outlier after the sensitivity analysis. Meta-analysis before the sensitivity analysis is displayed in Supplementary Material S3–S6. L’abbe plot shows a homogeneous dispersion of the results, not favoring control or experimental dropout rates. Baujat plot, influence graph, and leave-one-out plot did not present a notable influence of studies with low sample sizes. The funnel plot and Egger’s test (p = 0.42) show the absence of publication bias. All these sensitivity analyses are provided in Supplementary Materials S7–S11.
3.4. Meta-Analysis of Proportions
After the sensitivity analysis, 23 arms of study of 15 randomized controlled trials were meta-analyzed. Figure 2 shows the forest plot for the overall pooled dropout rate of 6.7% (95% CI 3–71.7%; I2 = 68%). When dropout events were sorted by study groups, the results were 11.6% (95%CI 7.9–16.7%; I2 = 39%) and 10.1% (95%CI 6.4–15.6%; I2 = 30%) for exercise groups (Figure 3) and control groups (Figure 4), respectively.
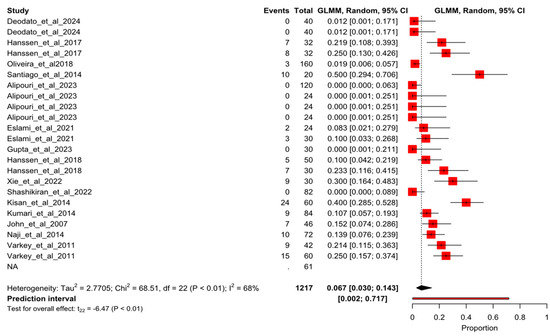
Figure 2.
Forest plot of proportion for the overall pooled dropout rate. Deodato et al., 2024 [4], Hanssen et al., 2017 [4], Kumar et al., 2020 [23], Oliveira et al., 2018 [24], Santiago et al., 2014 [25], Alipouri et al., 2023 [26], Eslami et al., 2021 [27], Gupta et al., 2023 [28], Hanssen et al., 2018 [29], Xie et al., 2022 [30], Shashikiran et al., 2022 [31], Kisan et al., 2014 [32], Kumari et al., 2022 [33], John et al., 2007 [34], Naji-Esfahani et al., 2014 [35], Varkey et al., 2011 [36].
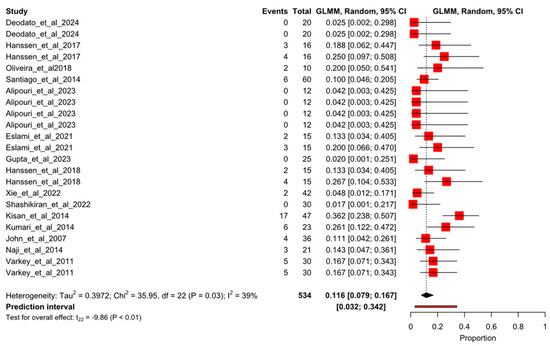
Figure 3.
Forest plot of proportion for the experimental pooled dropout rate. Deodato et al., 2024 [4], Hanssen et al., 2017 [4], Kumar et al., 2020 [23], Oliveira et al., 2018 [24], Santiago et al., 2014 [25], Alipouri et al., 2023 [26], Eslami et al., 2021 [27], Gupta et al., 2023 [28], Hanssen et al., 2018 [29], Xie et al., 2022 [30], Shashikiran et al., 2022 [31], Kisan et al., 2014 [32], Kumari et al., 2022 [33], John et al., 2007 [34], Naji-Esfahani et al., 2014 [35], Varkey et al., 2011 [36].
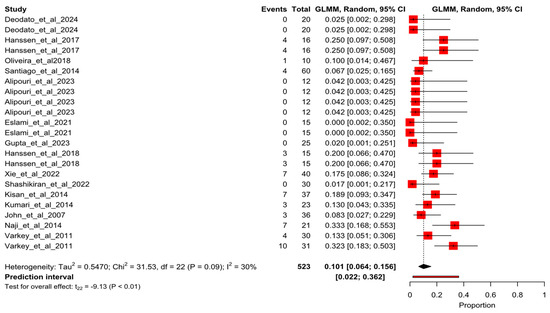
Figure 4.
Forest plot of proportion for the control pooled dropout rate. Deodato et al., 2024 [4], Hanssen et al., 2017 [4], Kumar et al., 2020 [23], Oliveira et al., 2018 [24], Santiago et al., 2014 [25], Alipouri et al., 2023 [26], Eslami et al., 2021 [27], Gupta et al., 2023 [28], Hanssen et al., 2018 [29], Xie et al., 2022 [30], Shashikiran et al., 2022 [31], Kisan et al., 2014 [32], Kumari et al., 2022 [33], John et al., 2007 [34], Naji-Esfahani et al., 2014 [35], Varkey et al., 2011 [36].
3.5. Meta-Analysis of Odds Ratio
After removing the outlier, the overall odds ratio meta-analysis showed no statistical difference in the likelihood of dropout events comparing exercise-based intervention and control comparators with an odds ratio of 1.09 (95%CI 0.77–1.54; I2 = 0%). Figure 5 shows the forest plot for this result.
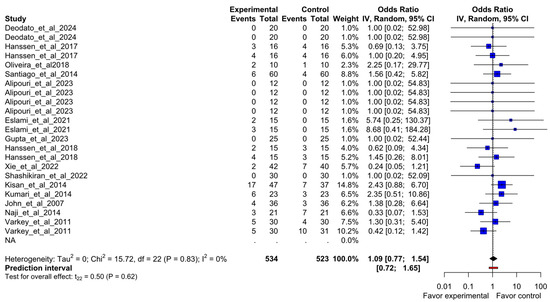
Figure 5.
Forest plot of overall odds ratio meta-analysis to compare dropout from study groups of included randomized clinical trials. Deodato et al., 2024 [4], Hanssen et al., 2017 [4], Kumar et al., 2020 [23], Oliveira et al., 2018 [24], Santiago et al., 2014 [25], Alipouri et al., 2023 [26], Eslami et al., 2021 [27], Gupta et al., 2023 [28], Hanssen et al., 2018 [29], Xie et al., 2022 [30], Shashikiran et al., 2022 [31], Kisan et al., 2014 [32], Kumari et al., 2022 [33], John et al., 2007 [34], Naji-Esfahani et al., 2014 [35], Varkey et al., 2011 [36].
3.6. Subgroup Meta-Analysis of Odds Ratio
The forest plots of the subgroup meta-analyses sorted by type of exercise, control intervention, and type of migraine are shown in Supplementary Materials S12–S14.
None of the subgroup analyses showed statistical differences for any types of exercise, control, or type of migraine, except for the migraines with aura. The odds ratio results for migraines with auras showed a lower pooled dropout rate in favor of control participants (participants with migraine aura) OR = 1.18 (95%CI 1.01–1.38; I2 = 0%) (Supplementary File S12), but most of the arms of the included studies belonged to Alipouri et al. [27], who did not present any dropout from their participants. This indicates that participants with migraines with aura who received exercise-based interventions had 1.18 times higher odds of dropping out compared to those receiving non-exercise-based comparators.
3.7. Certainty of Evidence: GRADE
The GRADE system was conducted for odds ratio meta-analysis. The certainty of evidence was rated as “very low” (Supplementary File S15).
4. Discussion
The primary objective of this systematic review with meta-analysis was to assess the current state of attrition in studies comparing exercise-based interventions to other approaches in patients with migraines. This study calculated the overall pooled dropout rate, as well as the dropout rates by intervention group in the included randomized controlled trials. When comparing dropout rates between participants receiving exercise-based interventions and those undergoing other treatments using an odds ratio meta-analysis, the results did not show statistically significant differences, even when subgroup analyses were performed based on exercise type, control group, and migraine type. However, in the case of migraine with aura, a significantly lower pooled dropout rate was observed in favor of control participants. This finding should be interpreted with caution due to the inclusion of multi-arm studies and the small sample size. Additionally, several limitations and substantial heterogeneity were identified across the selected studies, which will be discussed in detail below.
This systematic review highlights the complex relationship between exercise interventions and dropout rates in individuals with migraines. While exercise is widely recognized as a non-pharmacological approach with potential benefits in migraine management, adherence remains a significant challenge [38].
One of the key aspects that may contribute to dropout in exercise-based interventions is the bidirectional behavior of physical activity’s effects on migraine [39]. Exercise presents a complex relationship with migraine. On the one hand, intense physical activity may act as an acute trigger, particularly when performed during the prodromal or attack phases, precipitating migraine episodes [37]. On the other hand, physical inactivity is recognized as a contributing factor that may increase migraine frequency and chronicity [5]. Several studies suggest that moderate, regular exercise may reduce the frequency and severity of migraine attacks by improving vascular function, decreasing inflammation, and modulating pain sensitivity [40,41]. Conversely, there is also evidence that exercise can act as a potential trigger for migraine in susceptible individuals, particularly in high-intensity or prolonged exertion scenarios [42]. This duality may partially explain the inconsistencies in adherence across different interventions, as individuals experiencing symptom exacerbation are more likely to discontinue participation. Regular exercise, when appropriately prescribed and progressively adapted, has been shown to promote peripheral and central desensitization mechanisms, potentially reducing the frequency and severity of migraine attacks over time [40]. This duality highlights the importance of tailoring exercise interventions to each patient’s tolerance and migraine phase.
The type and intensity of exercise also appear to play a role in the attrition or adherence of participants with migraine [43]. Our subgroup analyses indicate that aerobic exercises, particularly those involving high-intensity training, showed slightly higher dropout rates compared to moderate-intensity or low-impact interventions such as yoga and tai chi. These findings align with previous research suggesting that more strenuous exercise regimens may increase the risk of exercise-induced migraine episodes, discouraging continued participation [44]. Additionally, individual variability in response to exercise further complicates adherence patterns, emphasizing the need for personalized exercise prescriptions tailored to migraineurs’ tolerance levels.
Psychosocial factors also influence adherence in migraine populations. Fear of exacerbating migraine symptoms, lack of motivation, and external barriers such as time constraints and scheduling conflicts are common reasons for discontinuation [38]. Studies included in this review reported that participants often cited logistical difficulties, competing obligations, and perceived ineffectiveness as primary reasons for dropout. Addressing these barriers through structured education, gradual exercise progression, and flexible scheduling may enhance adherence and optimize the long-term benefits of exercise for migraine management.
The dropout reasons observed in the included studies highlight important challenges related to participant retention in exercise-based interventions for migraine. Non-adherence to the protocol, personal circumstances, and adverse events were among the most common reasons for study withdrawals. In experimental groups, difficulties attending scheduled sessions, loss of interest, and symptom improvement were frequent factors contributing to dropout. In control groups, dissatisfaction with the assigned intervention, initiation of alternative treatments, and adverse effects related to pharmacological therapies were commonly reported. These findings suggest that retention strategies should be tailored to address the specific challenges faced by each group.
One key issue identified is the variability in how dropout reasons are reported across studies. Some trials provided detailed explanations, while others lacked transparency or grouped different causes under broad categories. This inconsistency limits the ability to draw strong conclusions about the factors influencing participant loss [45,46]. Moreover, while some studies explicitly mentioned adverse events as a cause of withdrawal, others failed to report whether such events occurred. This raises concerns regarding the accuracy of safety assessments in clinical trials involving physical activity interventions. A call for action is necessary to improve the transparency of studies related to dropout in randomized controlled trials focused on exercise and patients with migraine.
Considering that most studies did not document adverse events, we assumed that medical reasons were not directly linked to the interventions. We emphasize the need to standardize the reporting of dropout rates and reasons, as well as adverse events, in accordance with CONSORT guidelines to ensure transparency and improve the reliability of clinical research.
4.1. Clinical and Research Implications
The results of this review underscore the need to refine exercise-based interventions for migraine patients. Clinicians should advocate for tailored exercise prescriptions. One possibility for individualized exercise sessions is to start with lower-intensity regimens and gradually increase intensity based on patient tolerance. Additionally, behavioral strategies such as self-monitoring tools may enhance adherence and prevent premature dropout.
Exercise has been proposed to modulate several migraine-related mechanisms, particularly in chronic migraine. Regular physical activity may reduce central sensitization, enhance endorphin release, and improve mood and sleep quality, which are frequently impaired in chronic migraine patients [41]. These adaptations could explain its potential preventive role when appropriately prescribed and sustained over time, but this statement needs to be further studied and assessed to determine how it could influence attrition or retention. Our findings are aligned with recent research supporting the integration of structured exercise, including slow aerobic training and therapeutic physical activity, as part of comprehensive care for migraine. Such interventions may modulate central sensitization and improve quality of life, particularly when combined with pharmacological prophylaxis [47,48,49,50].
From a research perspective, standardizing exercise protocols across studies would improve comparability and facilitate meta-analyses. Moreover, greater consistency in reporting dropout reasons and adverse events is essential to identifying specific factors influencing non-adherence. Long-term follow-up studies are also warranted to assess whether initial dropouts eventually resume physical activity through alternative means.
Future studies should also explore sex, age, and migraine type-based differences in adherence. In addition, future studies should consider the specific migraine phase in which exercise is prescribed or initiated, as physical activity is typically contraindicated during the ictal phase due to heightened sensitivity and discomfort. The presence of comorbidities and simultaneous exposure to other potential migraine triggers should also be taken into account, as these may influence both adherence and dropout independently of the intervention itself. These exploratory studies and analyses will allow clinicians and researchers to elucidate sound conclusions to minimize the possibility of attrition in exercise-based studies, which could be extrapolated to clinical practice. Considering all the points mentioned above, a call for action standardizing the reporting of dropout and adverse events derived from exercise-based intervention in patients with migraines following CONSORT guidelines is required in future research [51]. Also, the use of the CONSORT harms guideline developed in 2022 could be useful for the studies that implemented exercise in patients with migraine since the mechanism of exercise in this condition remains unclear [52].
4.2. Limitations
Several limitations should be considered when interpreting the results of this systematic review. First, the included studies exhibited considerable heterogeneity in exercise protocols, migraine subtypes, and control conditions, potentially influencing the generalizability of the findings. Second, dropout reasons were not consistently reported across studies, limiting our ability to conduct a comprehensive analysis of specific factors driving attrition. Third, the reliance on self-reported data for adherence introduces the possibility of recall bias, which may impact the accuracy of dropout classifications. Addressing these limitations in future research will strengthen the evidence base for exercise interventions in migraine populations. Fourth, several studies with more than two arms of interventions were included in the meta-analysis, which is one of the added reasons for considering the results with caution.
5. Conclusions
This systematic review and meta-analysis provide a nuanced understanding of dropout rates in exercise-based interventions for migraine. While exercise does not appear to universally lead to higher attrition, individual variability in response, psychosocial barriers, and the nature of the intervention itself play critical roles in adherence. Future studies should focus on optimizing exercise protocols, addressing adherence barriers, and implementing long-term follow-ups to better understand the role of exercise in migraine management. By refining intervention strategies, researchers and clinicians can maximize the therapeutic potential of physical activity while minimizing dropout rates among patients with migraine. Finally, adequate adherence to the CONSORT guidelines in reporting losses and their reasons could help design appropriate retention strategies for studies and interventions based on exercise in patients with migraines.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/healthcare13091061/s1, Supplementary Material S1. Search strategy; Supplementary Material S2: list of excluded studies and reasons of exclusion; Suppelementary Material S3. All groups proportion meta-analysis previous to sensitivity analysis; Supplementary Material S4. Propotion meta-analysis of exercise-based interventions previous to sensitivity analysis; Supplementary Material S5. Proportion meta-analysis of comparator previous to sensitivity analysis; Supplementary Material S6. Odds ration meta-analysis previous to sensituvity analysis; Supplementary Material S7. Influence graph; Supplementary Material S8. L'Abbe plot; Supplementary Material S9. Leave-one-out analysis; Supplementary Material S10. Baujat plot; Supplementary Material S11. Funnel plot; Supplementary Material S12. Odds ratio meta-analysis sorted by migraine type; Supplementary Material S13. Odds ratio meta-analysis sorted by type of exercise; Supplementary Material S14. Odds ratio meta-analysis sorted by type of comparator; Supplementary File S15. Certainty of evidence (GRADE) for the odds ratio meta-analysis that compare dropout rates between experimental and control intervention.
Author Contributions
Conceptualization, C.G.-M.; data curation, C.G.-M., M.-D.C.-V. and S.T.; formal analysis, C.G.-M.; methodology, C.G.-M., M.-D.C.-V. and S.T.; project administration, M.-D.C.-V. and C.G.-M.; software (C.G.-M.); supervision (M.-D.C.-V.); visualization (C.G.-M.); writing—original draft, C.G.-M. and S.T.; writing—review and editing, M.-D.C.-V. All authors have read and agreed to the published version of this manuscript.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Data Availability Statement
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Polk, A.N.; Protti, T.A.; Smitherman, T.A. Allodynia and Disability in Migraine: The Mediating Role of Stress. Headache J. Head Face Pain 2020, 60, 2281–2290. [Google Scholar] [CrossRef]
- Steinmetz, J.D.; Seeher, K.M.; Schiess, N.; Nichols, E.; Cao, B.; Servili, C.; Cavallera, V.; Cousin, E.; Hagins, H.; Moberg, M.E.; et al. Global, Regional, and National Burden of Disorders Affecting the Nervous System, 1990–2021: A Systematic Analysis for the Global Burden of Disease Study 2021. Lancet Neurol. 2024, 23, 344–381. [Google Scholar] [CrossRef] [PubMed]
- Amin, F.M.; Aristeidou, S.; Baraldi, C.; Czapinska-Ciepiela, E.K.; Ariadni, D.D.; Di Lenola, D.; Fenech, C.; Kampouris, K.; Karagiorgis, G.; Braschinsky, M.; et al. The Association between Migraine and Physical Exercise. J. Headache Pain 2018, 19, 83. [Google Scholar] [CrossRef]
- Deodato, M.; Granato, A.; Buoite Stella, A.; Martini, M.; Marchetti, E.; Lise, I.; Galmonte, A.; Murena, L.; Manganotti, P. Efficacy of a Dual Task Protocol on Neurophysiological and Clinical Outcomes in Migraine: A Randomized Control Trial. Neurol. Sci. 2024, 45, 4015–4026. [Google Scholar] [CrossRef] [PubMed]
- Martins, I.P.; Gouveia, R.G.; Parreira, E. Kinesiophobia in Migraine. J. Pain 2006, 7, 445–451. [Google Scholar] [CrossRef] [PubMed]
- Belcarz, W.; Kalinowska, K.; Paprocka, A.; Świrk, U.; Fijałek, P.; Karczmarz, J.; Gutowska, M.; Balwierz, M.; Orzechowska, J.; Orzechowski, M. The Relationship Between Physical Activity and Migraines: Research on Prevention and Supportive Treatment. Qual. Sport 2025, 38, 58213. [Google Scholar] [CrossRef]
- Pietrobon, D.; Moskowitz, M.A. Pathophysiology of Migraine. Annu. Rev. Physiol. 2013, 75, 365–391. [Google Scholar] [CrossRef]
- Van Der Donckt, J.; Vandenbussche, N.; De Brouwer, M.; Steenwinckel, B.; Stojchevska, M.; Ongenae, F.; Paemeleire, K.; Van Hoecke, S. Analysis of Free-Living Daytime Movement in Patients with Migraine with Access to Acute Treatment. J. Headache Pain 2025, 26, 33. [Google Scholar] [CrossRef]
- Raggi, A.; Leonardi, M.; Arruda, M.; Caponnetto, V.; Castaldo, M.; Coppola, G.; Della Pietra, A.; Fan, X.; Garcia-Azorin, D.; Gazerani, P.; et al. Hallmarks of Primary Headache: Part 1—Migraine. J. Headache Pain 2024, 25, 189. [Google Scholar] [CrossRef]
- Fedeli, D.; Ciullo, G.; Demichelis, G.; Medina Carrion, J.P.; Bruzzone, M.G.; Ciusani, E.; Erbetta, A.; Ferraro, S.; Grisoli, M.; Guastafierro, E.; et al. Longitudinal Neurofunctional Changes in Medication Overuse Headache Patients after Mindfulness Practice in a Randomized Controlled Trial (the MIND-CM Study). J. Headache Pain 2024, 25, 97. [Google Scholar] [CrossRef]
- Hindiyeh, N.A.; Krusz, J.C.; Cowan, R.P. Does Exercise Make Migraines Worse and Tension Type Headaches Better? Curr. Pain Headache Rep. 2013, 17, 380. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Frandsen, T.F.; Bruun Nielsen, M.F.; Lindhardt, C.L.; Eriksen, M.B. Using the Full PICO Model as a Search Tool for Systematic Reviews Resulted in Lower Recall for Some PICO Elements. J. Clin. Epidemiol. 2020, 127, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Barker, T.H.; Stone, J.C.; Sears, K.; Klugar, M.; Tufanaru, C.; Leonardi-Bee, J.; Aromataris, E.; Munn, Z. The Revised JBI Critical Appraisal Tool for the Assessment of Risk of Bias for Randomized Controlled Trials. JBI Evid. Synth. 2023, 21, 494–506. [Google Scholar] [CrossRef]
- Harrer, M.; Cuijpers, P.; Furukawa, T.A.; Ebert, D.D. Doing Meta-Analysis with R; Chapman and Hall/CRC: Boca Raton, FL, USA, 2021; ISBN 9781003107347. [Google Scholar]
- Balduzzi, S.; Rücker, G.; Schwarzer, G. How to Perform a Meta-Analysis with R: A Practical Tutorial. Evid. Based Ment. Health 2019, 22, 153–160. [Google Scholar] [CrossRef]
- Viechtbauer, W. Conducting Meta-Analyses in R with the Metafor Package. J. Stat. Softw. 2010, 36, 1–48. [Google Scholar] [CrossRef]
- Schwarzer, G.; Chemaitelly, H.; Abu-Raddad, L.J.; Rücker, G. Seriously Misleading Results Using Inverse of Freeman-Tukey Double Arcsine Transformation in Meta-analysis of Single Proportions. Res. Synth. Methods 2019, 10, 476–483. [Google Scholar] [CrossRef]
- Gart, J.J.; Zweifel, J.R. On the Bias of Various Estimators of the Logit and Its Variance with Application to Quantal Bioassay. Biometrika 1967, 54, 181. [Google Scholar] [CrossRef]
- Nagashima, K.; Noma, H.; Furukawa, T.A. Prediction Intervals for Random-Effects Meta-Analysis: A Confidence Distribution Approach. Stat. Methods Med. Res. 2019, 28, 1689–1702. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; John Wiley & Sons: Chichester, UK, 2019. [Google Scholar]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in Meta-Analysis Detected by a Simple, Graphical Test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef]
- Hanssen, H.; Minghetti, A.; Magon, S.; Rossmeissl, A.; Papadopoulou, A.; Klenk, C.; Schmidt-Trucksäss, A.; Faude, O.; Zahner, L.; Sprenger, T.; et al. Superior Effects of High-Intensity Interval Training vs. Moderate Continuous Training on Arterial Stiffness in Episodic Migraine: A Randomized Controlled Trial. Front. Physiol. 2017, 8, 1086. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Bhatia, R.; Sharma, G.; Dhanlika, D.; Vishnubhatla, S.; Singh, R.K.; Dash, D.; Tripathi, M.; Srivastava, M.V.P. Effect of Yoga as Add-on Therapy in Migraine (CONTAIN). Neurology 2020, 94, e2203–e2212. [Google Scholar] [CrossRef]
- Oliveira, A.B.; Bachi, A.L.L.; Ribeiro, R.T.; Mello, M.T.; Vaisberg, M.; Peres, M.F.P. Exercise-Induced Change in Plasma IL-12p70 Is Linked to Migraine Prevention and Anxiolytic Effects in Treatment-Naïve Women: A Randomized Controlled Trial. Neuroimmunomodulation 2017, 24, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Santiago, M.D.S.; Carvalho, D.d.S.; Gabbai, A.A.; Pinto, M.M.P.; Moutran, A.R.C.; Villa, T.R. Amitriptyline and Aerobic Exercise or Amitriptyline Alone in the Treatment of Chronic Migraine: A Randomized Comparative Study. Arq. Neuropsiquiatr. 2014, 72, 851–855. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Alipouri, M.; Amiri, E.; Hoseini, R.; Hezarkhani, L.A. Effects of Eight Weeks of Aerobic Exercise and Vitamin D Supplementation on Psychiatric Comorbidities in Men with Migraine and Vitamin D Insufficiency: A Randomized Controlled Clinical Trial. J. Affect Disord. 2023, 334, 12–20. [Google Scholar] [CrossRef]
- Eslami, R.; Parnow, A.; Pairo, Z.; Nikolaidis, P.; Knechtle, B. The Effects of Two Different Intensities of Aerobic Training Protocols on Pain and Serum Neuro-Biomarkers in Women Migraineurs: A Randomized Controlled Trail. Eur. J. Appl. Physiol. 2021, 121, 609–620. [Google Scholar] [CrossRef]
- Gupta, A.; Kumar, S.; Gupta, A.; Rishi, P. Effect of Aerobic Exercises and Therapeutic Pain Neuroscience Education on Disability, Pain, Head Posture and QOL in Migraine Patients. Comp. Exerc. Physiol. 2023, 19, 119–126. [Google Scholar] [CrossRef]
- Hanssen, H.; Minghetti, A.; Magon, S.; Rossmeissl, A.; Rasenack, M.; Papadopoulou, A.; Klenk, C.; Faude, O.; Zahner, L.; Sprenger, T.; et al. Effects of Different Endurance Exercise Modalities on Migraine Days and Cerebrovascular Health in Episodic Migraineurs: A Randomized Controlled Trial. Scand. J. Med. Sci. Sports 2018, 28, 1103–1112. [Google Scholar] [CrossRef]
- Xie, Y.J.; Tian, L.; Hui, S.S.-C.; Qin, J.; Gao, Y.; Zhang, D.; Ma, T.; Suen, L.K.P.; Wang, H.H.; Liu, Z.-M.; et al. Efficacy and Feasibility of a 12-Week Tai Chi Training for the Prophylaxis of Episodic Migraine in Hong Kong Chinese Women: A Randomized Controlled Trial. Front. Public Health 2022, 10, 1000594. [Google Scholar] [CrossRef]
- Shashikiran, H.C.; Shetty, P.; Akshay, R.; Venugopal, A.; Shetty, S. Effect of Yoga Nidra on the Brain Activity in Individuals with Migraine. Yoga Mimamsa 2022, 54, 18–23. [Google Scholar] [CrossRef]
- Kisan, R.; Sujan, M.; Adoor, M.; Rao, R.; Nalini, A.; Kutty, B.; ChindandaMurthy, B.; Raju, T.; Sathyaprabha, T. Effect of Yoga on Migraine: A Comprehensive Study Using Clinical Profile and Cardiac Autonomic Functions. Int. J. Yoga 2014, 7, 126. [Google Scholar] [CrossRef] [PubMed]
- Kumari, S.; Dhar, M.; Pathania, M.; Kumar, N.; Kulshrestha, P.; Singh, A. Yoga as an Adjuvant Therapy in Management of Migraine- An Open Label Randomised Trial. J. Fam. Med. Prim. Care 2022, 11, 5410–5416. [Google Scholar] [CrossRef] [PubMed]
- John, P.J.; Sharma, N.; Sharma, C.M.; Kankane, A. Effectiveness of Yoga Therapy in the Treatment of Migraine Without Aura: A Randomized Controlled Trial. Headache J. Head Face Pain 2007, 47, 654–661. [Google Scholar] [CrossRef] [PubMed]
- Naji-Esfahani, H.; Zamani, M.; Marandi, S.M.; Shaygannejad, V.; Javanmard, S.H. Preventive Effects of a Three-Month Yoga Intervention on Endothelial Function in Patients with Migraine. Int. J. Prev. Med. 2014, 5, 424–429. [Google Scholar]
- Varkey, E.; Cider, Å.; Carlsson, J.; Linde, M. Exercise as Migraine Prophylaxis: A Randomized Study Using Relaxation and Topiramate as Controls. Cephalalgia 2011, 31, 1428–1438. [Google Scholar] [CrossRef]
- La Touche, R.; de Oliveira, A.B.; Paris-Alemany, A.; Reina-Varona, Á. Incorporating Therapeutic Education and Exercise in Migraine Management: A Biobehavioral Approach. J. Clin. Med. 2024, 13, 6273. [Google Scholar] [CrossRef]
- Annalisa, G.; Davide, B.; Marco, A. Sport and Migraine—A Dynamic Relationship. Neurol. Sci. 2022, 43, 5749–5751. [Google Scholar] [CrossRef]
- Reina-Varona, Á.; Madroñero-Miguel, B.; Fierro-Marrero, J.; Paris-Alemany, A.; La Touche, R. Efficacy of Various Exercise Interventions for Migraine Treatment: A Systematic Review and Network Meta-analysis. Headache J. Head Face Pain 2024, 64, 873–900. [Google Scholar] [CrossRef]
- Ahn, A.H. Why Does Increased Exercise Decrease Migraine? Curr. Pain Headache Rep. 2013, 17, 379. [Google Scholar] [CrossRef]
- Lippi, G.; Mattiuzzi, C.; Sanchis-Gomar, F. Physical Exercise and Migraine: For or Against? Ann. Transl. Med. 2018, 6, 181. [Google Scholar] [CrossRef]
- La Touche, R.; Fierro-Marrero, J.; Sánchez-Ruíz, I.; Rodríguez de Rivera-Romero, B.; Cabrera-López, C.D.; Lerma-Lara, S.; Requejo-Salinas, N.; de Asís-Fernández, F.; Elizagaray-García, I.; Fernández-Carnero, J.; et al. Prescription of Therapeutic Exercise in Migraine, an Evidence-Based Clinical Practice Guideline. J. Headache Pain 2023, 24, 68. [Google Scholar] [CrossRef] [PubMed]
- Varkey, E.; Grüner Sveälv, B.; Edin, F.; Ravn-Fischer, A.; Cider, Å. Provocation of Migraine after Maximal Exercise: A Test-Retest Study. Eur. Neurol. 2017, 78, 22–27. [Google Scholar] [CrossRef] [PubMed]
- Kearney, A.; Rosala-Hallas, A.; Rainford, N.; Blazeby, J.M.; Clarke, M.; Lane, A.J.; Gamble, C. Increased Transparency Was Required When Reporting Imputation of Primary Outcome Data in Clinical Trials. J. Clin. Epidemiol. 2022, 146, 60–67. [Google Scholar] [CrossRef]
- Kearney, A.; Rosala-Hallas, A.; Bacon, N.; Daykin, A.; Shaw, A.R.G.; Lane, A.J.; Blazeby, J.M.; Clarke, M.; Williamson, P.R.; Gamble, C. Reducing Attrition within Clinical Trials: The Communication of Retention and Withdrawal within Patient Information Leaflets. PLoS ONE 2018, 13, e0204886. [Google Scholar] [CrossRef]
- Sierra-Mencía, Á.; Recio-García, A.; García-Azorín, D.; de la Torre, A.J.M.; González, I.R.; Guerrero-Peral, Á.L. Physical Activity as a Predictor of Fremanezumab Response in Chronic Migraine—The Phy-Fre-Mig Study. J. Headache Pain 2025, 26, 34. [Google Scholar] [CrossRef]
- Meise, R.; Schwarz, A.; Luedtke, K. Effectiveness of Patient Education and Cognitive Behavioural Treatment as a Non-Pharmacological Intervention for Migraine in Adults—A Systematic Review. SN Compr. Clin. Med. 2022, 4, 197. [Google Scholar] [CrossRef]
- Onan, D.; Arıkan, H.; Can, İ.; Özge, A.; Martelletti, P. Comparative Insights into Physiotherapy Expectations Among Chronic Migraine Patients with and without OnabotulinumtoxinA Treatment: A Case–Control Study. SN Compr. Clin. Med. 2024, 6, 125. [Google Scholar] [CrossRef]
- Petrušić, I.; Ha, W.-S.; Labastida-Ramirez, A.; Messina, R.; Onan, D.; Tana, C.; Wang, W. Influence of Next-Generation Artificial Intelligence on Headache Research, Diagnosis and Treatment: The Junior Editorial Board Members’ Vision—Part 1. J. Headache Pain 2024, 25, 151. [Google Scholar] [CrossRef]
- Moher, D.; Hopewell, S.; Schulz, K.F.; Montori, V.; Gotzsche, P.C.; Devereaux, P.J.; Elbourne, D.; Egger, M.; Altman, D.G. CONSORT 2010 Explanation and Elaboration: Updated Guidelines for Reporting Parallel Group Randomised Trials. BMJ 2010, 340, c869. [Google Scholar] [CrossRef]
- Junqueira, D.R.; Zorzela, L.; Golder, S.; Loke, Y.; Gagnier, J.J.; Julious, S.A.; Li, T.; Mayo-Wilson, E.; Pham, B.; Phillips, R.; et al. CONSORT Harms 2022 Statement, Explanation, and Elaboration: Updated Guideline for the Reporting of Harms in Randomised Trials. BMJ 2023, 381, e073725. [Google Scholar] [CrossRef]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).