
The Effectiveness of Dance Interventions on Health-Related Outcomes in Perimenopausal, Menopausal, and Postmenopausal Women: A Systematic Review and Meta-Analysis


Abstract
1. Introduction
2. Materials and Methods
2.1. Source Search Strategy
2.2. Research Options
2.3. Inclusion and Exclusion Criteria
2.3.1. Inclusion Criteria
2.3.2. Exclusion Criteria
2.4. Data Extraction
2.5. Quality Assessment
2.6. Data Synthesis and Analysis
3. Results
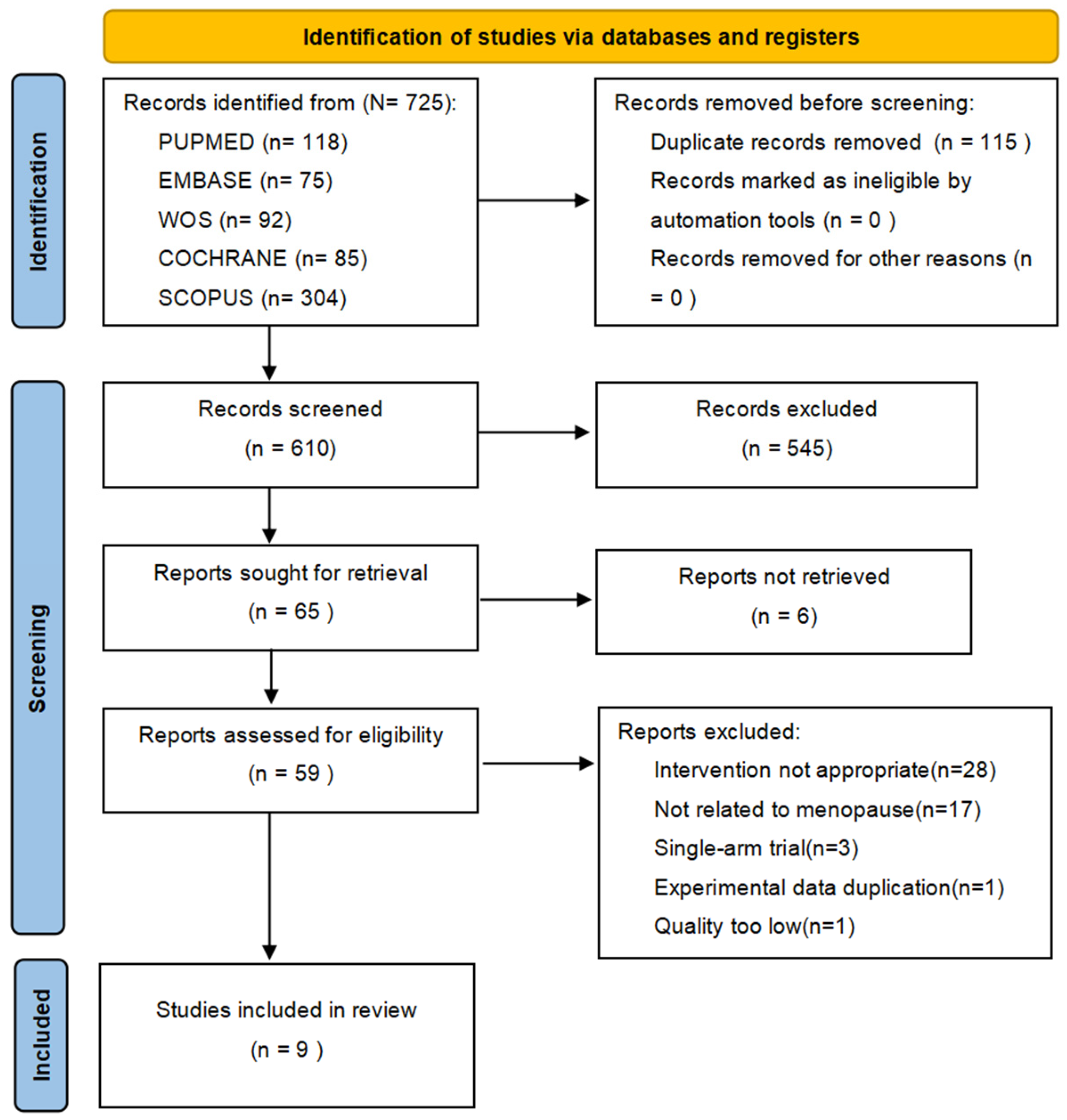
3.1. Search Results
3.2. Description of Included Studies
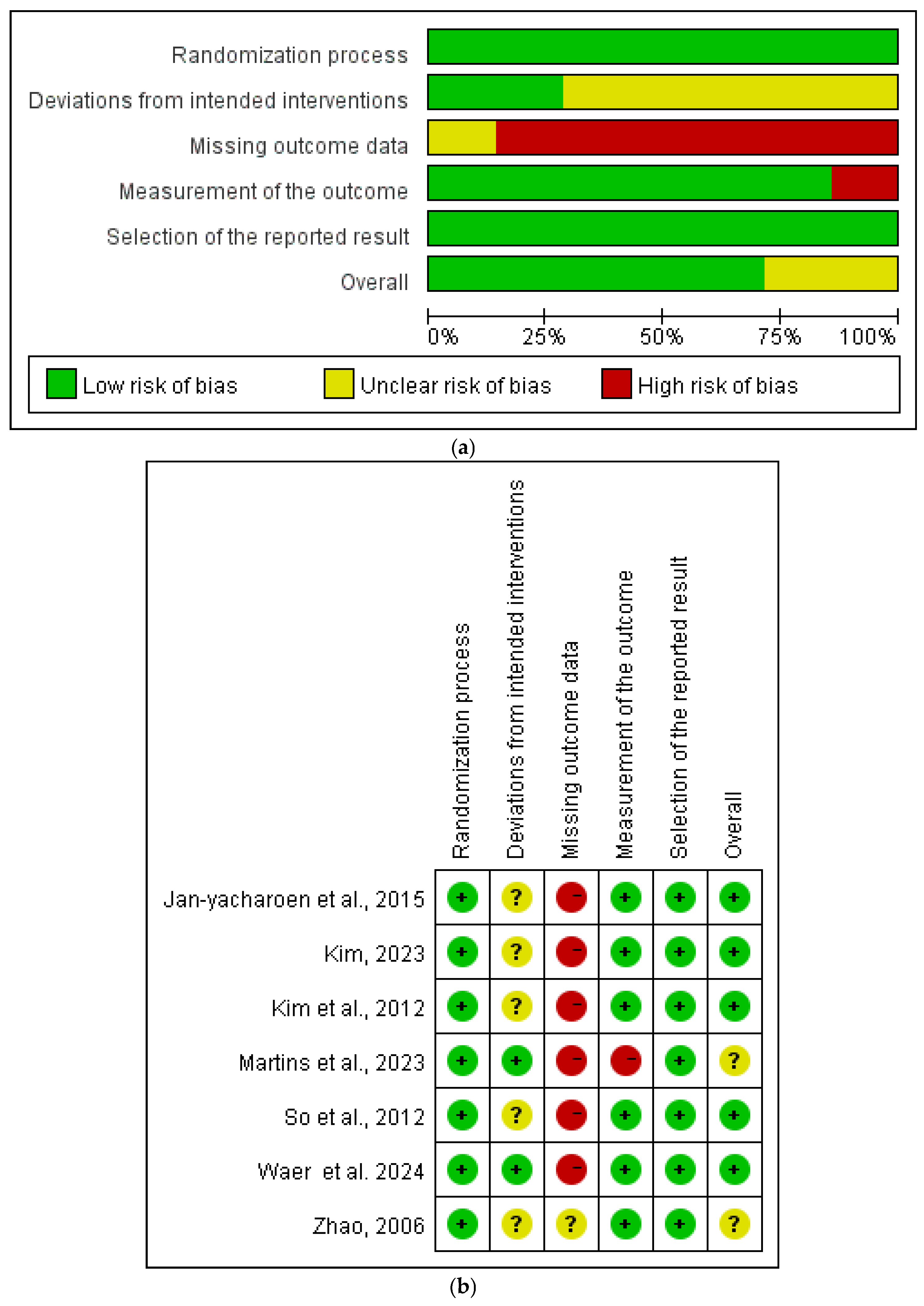
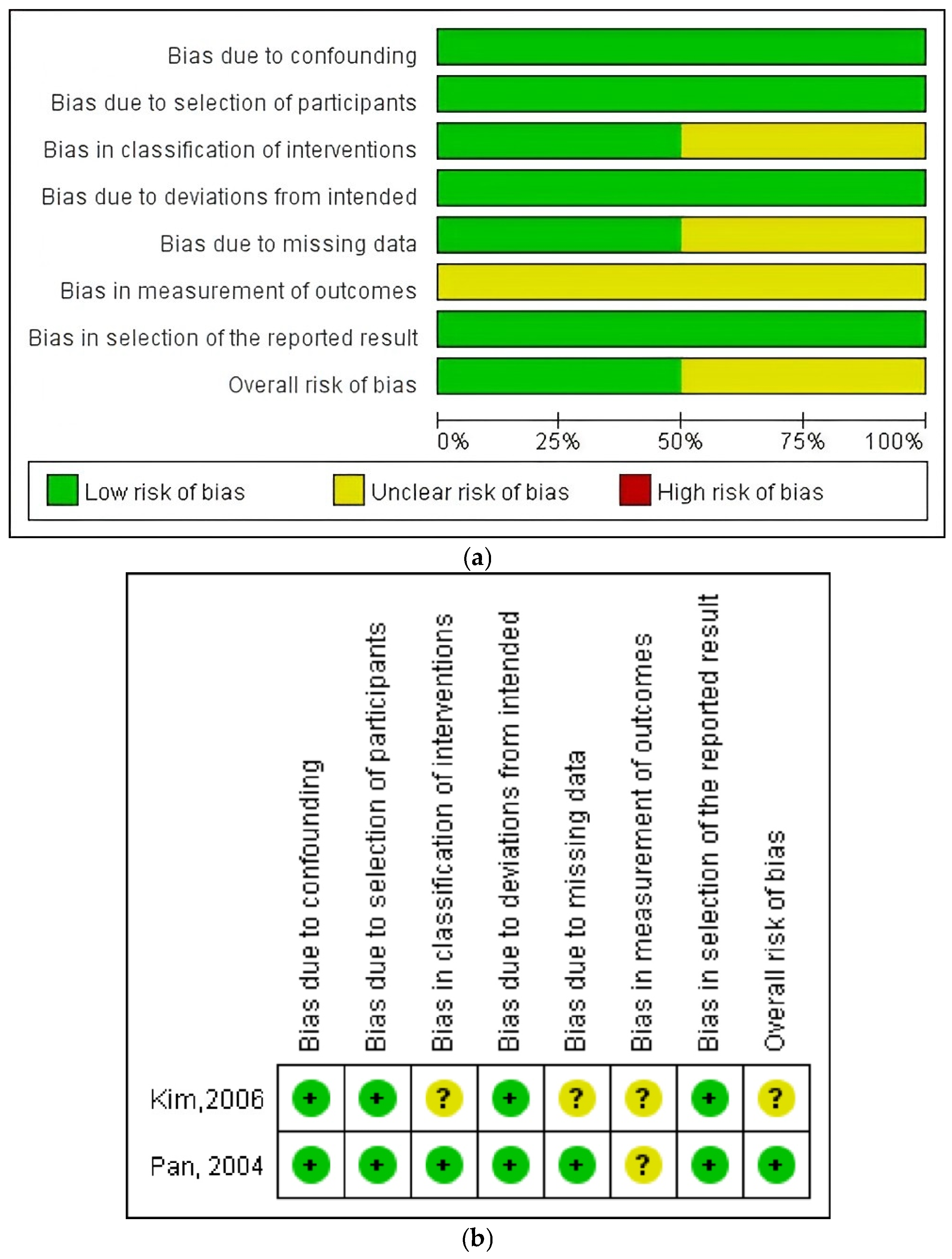
3.3. Assessment of Risk of Bias
3.4. Meta-Analysis Results
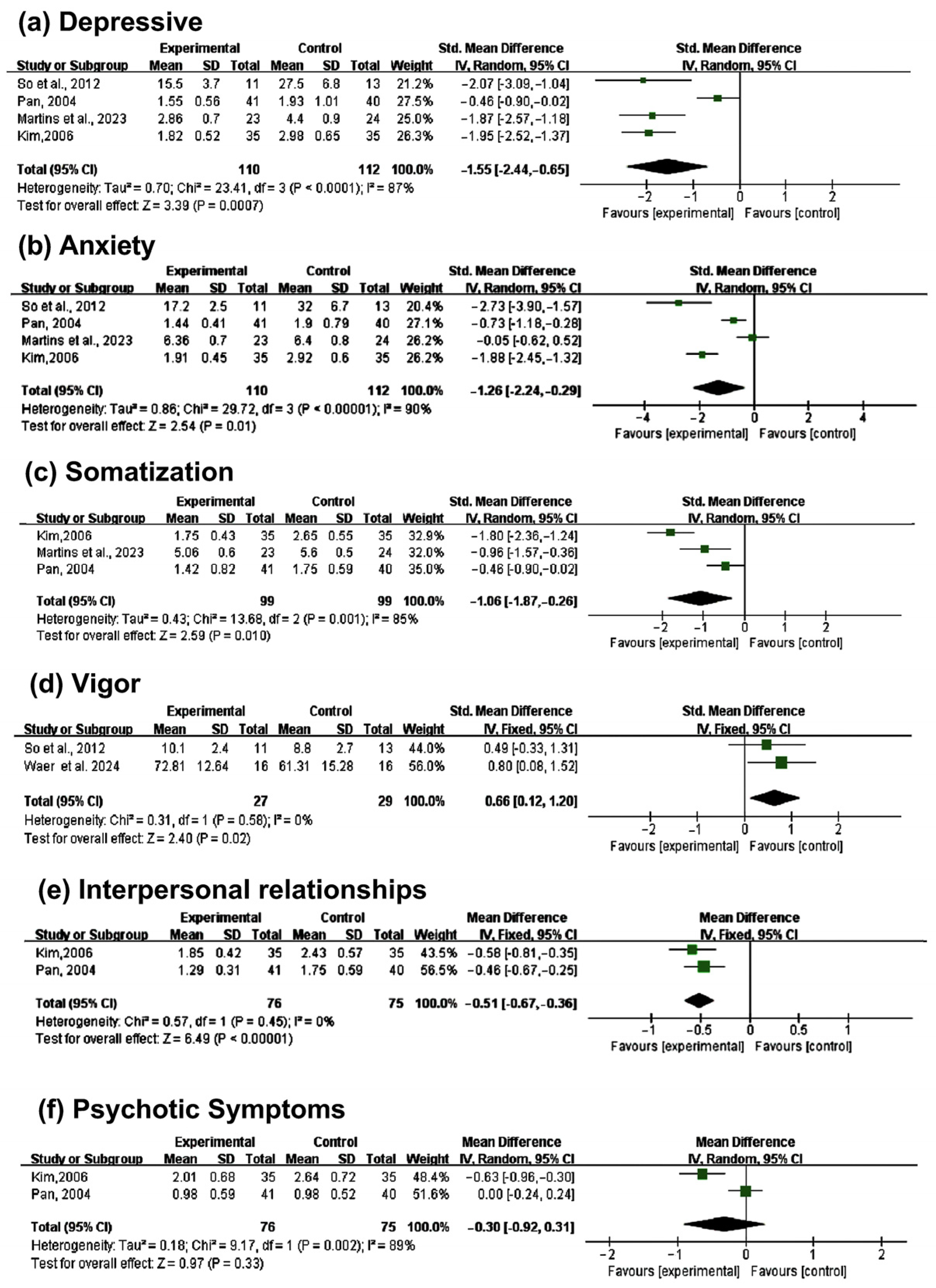
3.4.1. Depression
3.4.2. Anxiety
3.4.3. Somatization
3.4.4. Vigor
3.4.5. Interpersonal Relationships
3.4.6. Psychotic Symptoms
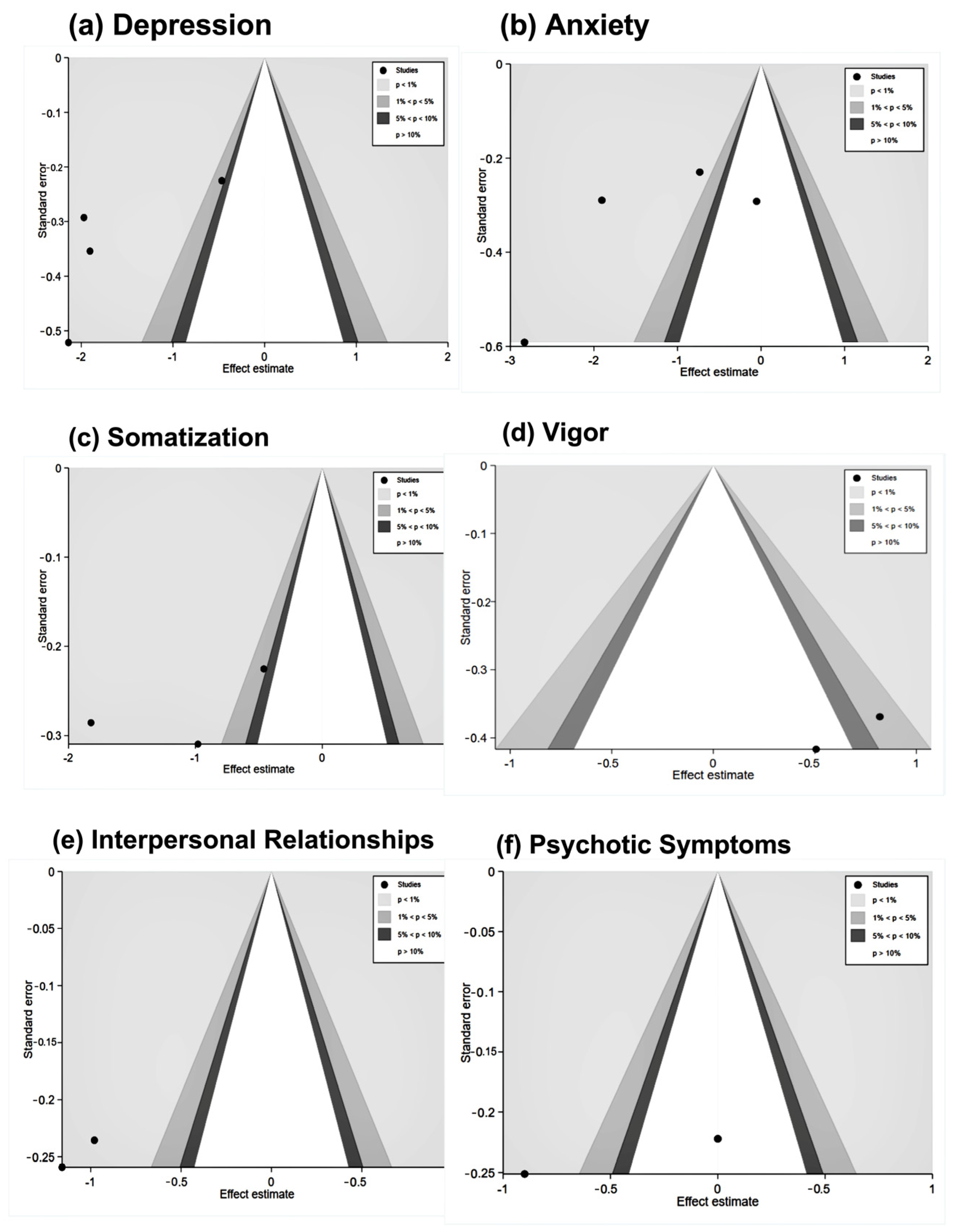
3.5. Publication Bias
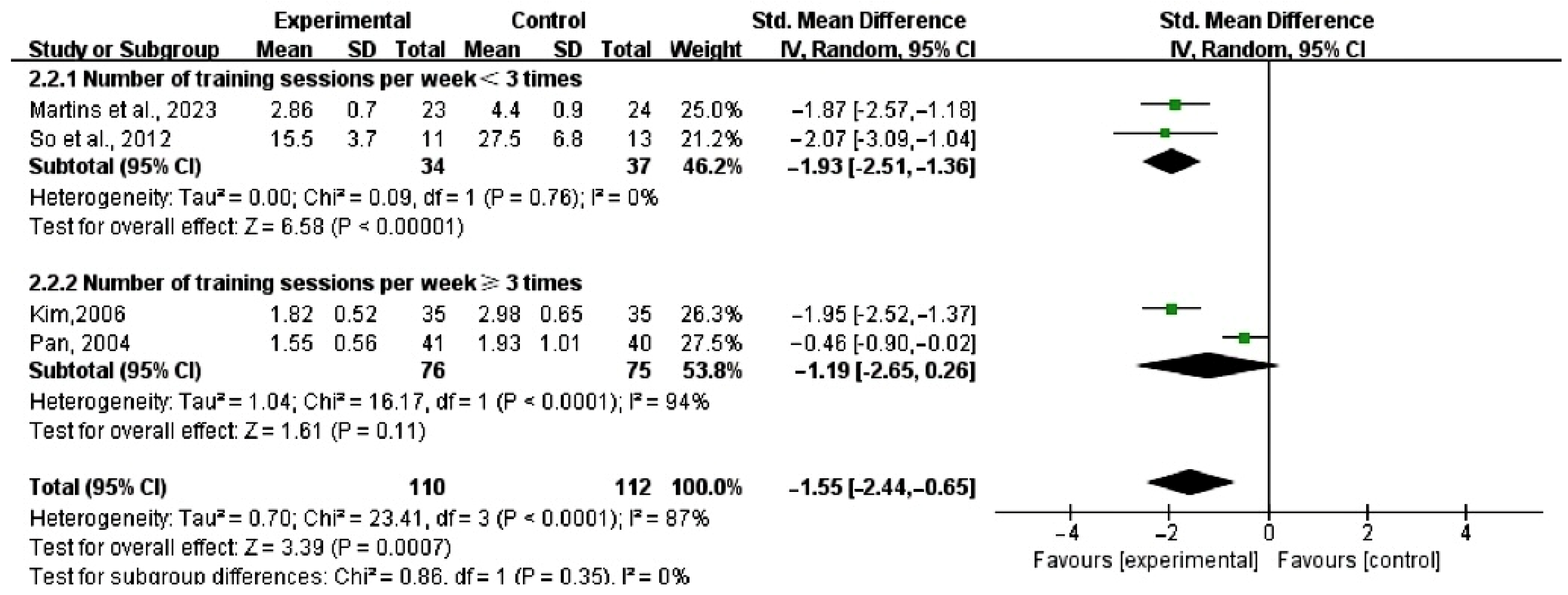
3.6. Subgroup Analysis
3.7. Narrative Results
3.7.1. Zumba Dance
3.7.2. Jazz Dance
3.7.3. Sports Dance
3.7.4. Traditional Dance
3.7.5. Dance Movement Therapy (DMT)
4. Discussion
4.1. Summary of Findings
4.1.1. Psychological Outcomes
4.1.2. Physiological Outcomes
4.2. Strengths and Limitations
4.3. Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| HT | Hormone therapy |
| NHDT | Non-hormonal drug therapy |
| CHD | Coronary heart disease |
| SMD | Standardized Mean Difference |
| MD | Mean Difference |
| ROB2.0 | Risk of Bias 2.0 |
| ROBINS-I | Risk of Bias in Non-randomized Studies of Interventions |
| I2 | I-Square |
| DMT | Dance movement therapy |
| CI | Confidence interval |
| P | P-value |
| LDL-C | Low-density lipoprotein cholesterol |
| HDL-C | High-density lipoprotein cholesterol |
References
- Management of Menopause-Related Symptoms: Summary. Available online: https://www.ncbi.nlm.nih.gov/books/NBK11956/ (accessed on 20 December 2024).
- Menopausal Women—Care for Your Family. Available online: https://cniw.org/ (accessed on 20 December 2024).
- Menopause Diagnosis and Treatment. Available online: http://motaean.co.kr/chi/sub.php?code=02_gyne02 (accessed on 20 December 2024).
- Lialy, H.E.; Mohamed, M.A.; AbdAllatif, L.A.; Khalid, M.; Elhelbawy, A. Effects of Different Physiotherapy Modalities on Insomnia and Depression in Perimenopausal, Menopausal, and Post-Menopausal Women: A Systematic Review. BMC Women’s Health 2023, 23, 363. [Google Scholar] [CrossRef] [PubMed]
- WebMD Editorial Contributors. Menopause Information. Available online: https://www.webmd.com/menopause/menopause-information (accessed on 20 December 2024).
- Rossouw, J.E.; Anderson, G.L.; Prentice, R.L.; LaCroix, A.Z.; Kooperberg, C.; Stefanick, M.L.; Jackson, R.D.; Beresford, S.A.A.; Howard, B.V.; Johnson, K.C.; et al. Risks and Benefits of Estrogen Plus Progestin in Healthy Postmenopausal Women: Principal Results from the Women’s Health Initiative Randomized Controlled Trial. JAMA 2002, 288, 321–333. [Google Scholar] [CrossRef] [PubMed]
- Teede, H.J. Hormone Replacement Therapy, Cardiovascular and Cerebrovascular Disease. Best Pract. Res. Clin. Endocrinol. Metab. 2003, 17, 73–90. [Google Scholar] [CrossRef]
- Shorey, S.; Ang, L.; Lau, Y. Efficacy of Mind-Body Therapies and Exercise-Based Interventions on Menopausal-Related Outcomes among Asian Perimenopausal Women: A Systematic Review, Meta-Analysis, and Synthesis without a Meta-Analysis. J. Adv. Nurs. 2020, 76, 1098–1110. [Google Scholar] [CrossRef]
- Duarte Machado, E.; Cole, M.H.; Miller, L.; McGuckian, T.B.; Wilson, P.H. The Efficacy of Dance Interventions for the Activity and Participation of Individuals with Cerebral Palsy—A Systematic Review and Meta-Analysis. Disabil. Rehabil. 2024, 46, 1485–1501. [Google Scholar] [CrossRef]
- Abu-Odah, H.; Wang, M.; Su, J.J.; Collard-Stokes, G.; Sheffield, D.; Molassiotis, A. Effectiveness of Dance Movement Therapy and Dance Movement Interventions on Cancer Patients’ Health-Related Outcomes: A Systematic Review and Meta-Analysis. Support. Care Cancer 2024, 32, 235. [Google Scholar] [CrossRef]
- Chen, T.; Wen, R.; Liu, H.; Zhong, X.; Jiang, C. Dance Intervention for Negative Symptoms in Individuals with Autism Spectrum Disorder: A Systematic Review and Meta-Analysis. Complement. Ther. Clin. Pract. 2022, 47, 101565. [Google Scholar] [CrossRef]
- Ares-Benitez, I.; Billot, M.; Rigoard, P.; Cano-Bravo, F.; David, R.; Luque-Moreno, C. Feasibility, Acceptability and Effects of Dance Therapy in Stroke Patients: A Systematic Review. Complement. Ther. Clin. Pract. 2022, 49, 101662. [Google Scholar] [CrossRef]
- Rossmeissl, A.; Lenk, S.; Hanssen, H.; Donath, L.; Schmidt-Trucksäss, A.; Schäfer, J. ZumBeat: Evaluation of a Zumba Dance Intervention in Postmenopausal Overweight Women. Sports 2016, 4, 5. [Google Scholar] [CrossRef]
- Yang, X.; Bi, Y. Study on the Intervention of Line Dance Exercise on Abnormal Psychological Symptoms of Menopausal Women. J. Shandong Inst. Phys. Educ. 2015, 5, 68–71. Available online: https://oversea.cnki.net/KCMS/detail/detail.aspx?dbcode=CJFD&dbname=CJFDLAST2016&filename=TIRE201505014&uniplatform=OVERSEA&v=56-ElLiwikT3vNW7_1M3hkfl2s99sxFZTdKUa1HbbSO0Z6ObjS2m6OMJolvZu0Si (accessed on 3 December 2024).
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A Revised Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A Tool for Assessing Risk of Bias in Non-Randomised Studies of Interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef]
- So, S.H.; Kim, H.J.; Ha, H.Y.; Kim, N.S. The Effect of Dance Movement Therapy on Anxiety, Depression, and the Quality of Life in Climacteric Women. J. Orient. Gynecol. 2012, 25, 154–173. [Google Scholar] [CrossRef]
- Kim, J.-H.; Yoon, J.-S.; Baek, S.-H. Effects of Dance Sports Training on Changes in the Bone Mineral Density, Size of Rectus Femoris and Body Composition in Menopause Middle-Aged Women. Off. J. Korean Soc. Danc. Sci. 2012, 28, 127–139. [Google Scholar]
- Kim, M.-H. Effects of Dance Sports Participation on the Mental Health of Postmenopausal Women. Korea Sports Res. 2006, 17, 731–742. Available online: https://www.riss.kr/link?id=A104416655 (accessed on 3 December 2024).
- Kim, J.-H. The Effect of Korean Dance Training on Immunity and Changes of Body Temperature in Menopausal Middle-Aged Women. Arts Cult. 2023, 4, 61–74. Available online: https://www.riss.kr/link?id=A108741559 (accessed on 3 December 2024).
- Pan, L. Comprehensive effects of sports dance training on menopausal women. J. Yulin Teach. Coll. 2004, 5, 80–83. Available online: https://oversea.cnki.net/KCMS/detail/detail.aspx?dbcode=CJFD&dbname=CJFD2004&filename=YLSZ200405022&uniplatform=OVERSEA&v=1No5rJC73NDfGVNv1zm9JJK1ZjIaMydT_Ccbx9ZrDXaRqJ7RB0DOTzpLqeBq3Ynj (accessed on 1 December 2024).
- Zhao, H. Effects of moderate-intensity sports dance on estrogen and blood lipid levels in menopausal women. Chin. J. Clin. Rehabil. 2006, 10, 29–31. Available online: https://oversea.cnki.net/KCMS/detail/detail.aspx?dbcode=CJFD&dbname=CJFD2006&filename=XDKF200616013&uniplatform=OVERSEA&v=pc6hHp21kk2ubv9HsIJkcosGVT3dT75K05o7GQCpuRYrEa7Ps-9y3hDaRTjw1IAQ (accessed on 1 December 2024).
- Ben Waer, F.; Lahiani, M.; Alexe, C.I.; Badau, D.; Onoi, M.P.; Alexe, D.I.; Sahli, S. The effects of Pilates vs. Zumba dancing on functional performance, mood and health-related quality of life in postmenopausal women. Appl. Sci. 2024, 14, 2886. [Google Scholar] [CrossRef]
- Martins, J.B.B.; Fausto, D.Y.; Flores, F.S.; Sonza, A.; Matias, T.S.; Guimarães, A.C.d.A. Jazz dance on menopausal symptoms and psychological aspects: A randomized clinical trial pilot study with follow-up. Res. Q. Exerc. Sport 2024, 1–11. [Google Scholar] [CrossRef]
- Janyacharoen, T.; Phusririt, C.; Angkapattamakul, S.; Hurst, C.P.; Sawanyawisuth, K. Cardiopulmonary effects of traditional Thai dance on menopausal women: A randomized controlled trial. J. Phys. Ther. Sci. 2015, 27, 2569–2572. Available online: https://www.jstage.jst.go.jp/article/jpts/27/8/27_jpts-2015-294/_article/-char/en (accessed on 10 December 2024). [CrossRef] [PubMed]
- Easterbrook, P.J.; Berlin, J.A.; Gopalan, R.; Matthews, D.R. Publication bias in clinical research. Lancet 1991, 337, 867–872. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Koch, S.C.; Morlinghaus, K.; Fuchs, T. The Joy Dance: Specific Effects of a Single Dance Intervention on Psychiatric Patients with Depression. Arts Psychother. 2007, 34, 340–349. [Google Scholar] [CrossRef]
- Ji, H. Using Dance-Based Interventions to Overcome Anxiety and Stress in China. Curr. Psychol. 2024, 43, 24557–24564. [Google Scholar] [CrossRef]
- Gordon, A.J. Focusing on Positive Affect in Dance/Movement Therapy: A Qualitative Study. Am. J. Danc. Ther. 2014, 36, 60–76. [Google Scholar] [CrossRef]
- Behrends, A.; Müller, S.; Dziobek, I. Dancing Supports Empathy: The Potential of Interactional Movement and Dance for Psychotherapy. Eur. Psychother. 2016, 13, 99–131. Available online: https://api.semanticscholar.org/CorpusID:201600427 (accessed on 10 December 2024).
- Duberg, A.; Jutengren, G.; Hagberg, L.; Möller, M. The Effects of a Dance Intervention on Somatic Symptoms and Emotional Distress in Adolescent Girls: A Randomized Controlled Trial. J. Int. Med. Res. 2020, 48, 0300060520902610. [Google Scholar] [CrossRef]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.T.; Rothstein, H.R. Introduction to Meta-Analysis; Wiley: Hoboken, NJ, USA, 2009; Available online: https://onlinelibrary.wiley.com/doi/book/10.1002/9780470743386 (accessed on 10 December 2024).
- Tomaz, G.G.; Souza, M.V.C.; Carneiro, M.A.S.; Lima, M.L.; Assumpção, C.O.; Orsatti, F.L. Propulsive forces and muscle activation during gait: Comparisons between premenopausal and postmenopausal midlife women. Menopause 2024, 31, 194–201. [Google Scholar] [CrossRef]
- Teixeira-Machado, L.; Arida, R.M.; de Jesus Mari, J. Dance for neuroplasticity: A descriptive systematic review. Neurosci. Biobehav. Rev. 2019, 96, 232–240. [Google Scholar] [CrossRef]
- Dabrowska-Galas, M.; Dabrowska, J.; Ptaszkowski, K.; Plinta, R. High physical activity level may reduce menopausal symptoms. Medicina 2019, 55, 466. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Lozano, S.; Zhang, N.; Armstrong, R.; León, K.; Kelly-Lahon, C.; Sánchez-González, P.; Martínez-González-Moro, I.; Hurtado-Guapo, M.A.; Vargas-Macías, A. The Concept of Neuromuscular Repatterning in Dancers: A Systematic Review. Healthcare 2024, 12, 402. [Google Scholar] [CrossRef] [PubMed]
- Krasnow, D. CI Training: The Merger of Conditioning and Imagery as an Alternative Training Methodology for Dance. Med. Probl. Perform. Art. 1997, 12, 3–8. Available online: https://www.jstor.org/stable/45440597 (accessed on 10 December 2024).
- Brodie, J.; Lobel, E. Integrating Fundamental Principles Underlying Somatic Practices into the Dance Technique Class. J. Danc. Educ. 2004, 4, 80–87. [Google Scholar] [CrossRef]
- Dimache, A.M.; Șalaru, D.L.; Sascău, R.; Stătescu, C. The Role of High Triglycerides Level in Predicting Cognitive Impairment: A Review of Current Evidence. Nutrients 2021, 13, 2118. [Google Scholar] [CrossRef]
- Xiaoyan, L.; Jianhua, Z. The Effect of Square Dance Combined with Calcium on Bone Mineral Density, Serum Sex Hormones and Balance Ability in Postmenopausal Women. Chin. J. Osteoporos. 2017, 23, 1063–1066. [Google Scholar] [CrossRef]
- Araneta, M.R.; Tanori, D. Benefits of Zumba Fitness® among Sedentary Adults with Components of the Metabolic Syndrome: A Pilot Study. J. Sports Med. Phys. Fit. 2015, 55, 1227–1233. Available online: https://europepmc.org/article/med/24921620 (accessed on 3 April 2025).
- Rodrigues-Krause, J.; Farinha, J.B.; Ramis, T.R.; Macedo, R.C.O.; Boeno, F.P.; Dos Santos, G.C.; Vargas, J., Jr.; Lopez, P.; Grazioli, R.; Costa, R.R.; et al. Effects of Dancing Compared to Walking on Cardiovascular Risk and Functional Capacity of Older Women: A Randomized Controlled Trial. Exp. Gerontol. 2018, 114, 67–77. [Google Scholar] [CrossRef]
- Cardozo, L.; Bachmann, G.; McClish, D.; Fonda, D.; Birgerson, L. Meta-analysis of estrogen therapy in the management of urogenital atrophy in postmenopausal women: Second report of the Hormones and Urogenital Therapy Committee. Obstet. Gynecol. 1998, 92, 722–727. Available online: https://journals.lww.com/greenjournal/abstract/1998/10001/META_ANALYSIS_OF_ESTROGEN_THERAPY_IN_THE.45.aspx (accessed on 3 April 2025). [CrossRef]
- Kissler, K.; Yount, S.M.; Rendeiro, M.; Zeidenstein, L. Primary Prevention of Urinary Incontinence: A Case Study of Prenatal and Intrapartum Interventions. J. Midwifery Women’s Health 2016, 61, 507–511. [Google Scholar] [CrossRef]
- Kim, J.W.; Kim, D.Y. Effects of Aerobic Exercise Training on Serum Sex Hormone Binding Globulin, Body Fat Index, and Metabolic Syndrome Factors in Obese Postmenopausal Women. Metab. Syndr. Relat. Disord. 2012, 10, 452–457. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Nieves, I.; Jakobsche, C.E. Biomolecular Effects of Dance and Dance/Movement Therapy: A Review. Am. J. Danc. Ther. 2022, 44, 241–263. [Google Scholar] [CrossRef]
- Pasquali, R.; Casimirri, F.; Labate, A.M.; Tortelli, O.; Pascal, G.; Anconetani, B.; Gatto, M.R.; Flamia, R.; Capelli, M.; Barbara, L. Body Weight, Fat Distribution and the Menopausal Status in Women. The VMH Collaborative Group. Int. J. Obes. Relat. Metab. Disord. 1994, 18, 614–621. Available online: https://europepmc.org/article/med/7812415 (accessed on 3 April 2025). [PubMed]
- Toth, M.J.; Tchernof, A.; Sites, C.K.; Poehlman, E.T. Effect of Menopausal Status on Body Composition and Abdominal Fat Distribution. Int. J. Obes. 2000, 24, 226–231. [Google Scholar] [CrossRef]
- Ley, C.J.; Lees, B.; Stevenson, J.C. Sex- and Menopause-Associated Changes in Body-Fat Distribution. Am. J. Clin. Nutr. 1992, 55, 950–954. [Google Scholar] [CrossRef]
- Toth, M.J.; Tchernof, A.; Sites, C.K.; Poehlman, E.T. Menopause-Related Changes in Body Fat Distribution. Ann. New York Acad. Sci. 2000, 904, 502–506. [Google Scholar] [CrossRef]
- Li, Y.; Zhai, Q.; Li, G.; Peng, W. Effects of Different Aerobic Exercises on Blood Lipid Levels in Middle-Aged and Elderly People: A Systematic Review and Bayesian Network Meta-Analysis Based on Randomized Controlled Trials. Healthcare 2024, 12, 1309. [Google Scholar] [CrossRef]
- Sternfeld, B.; Bhat, A.K.; Wang, H.; Sharp, T.; Quesenberry, C.P. Menopause, physical activity, and body composition/fat distribution in midlife women. Med. Sci. Sports Exerc. 2005, 37, 1195–1202. [Google Scholar] [CrossRef]
- Klonizakis, M.; Moss, J.; Gilbert, S.; Broom, D.; Foster, J.; Tew, G.A. Low-Volume High-Intensity Interval Training Rapidly Improves Cardiopulmonary Function in Postmenopausal Women. Menopause 2014, 21, 1099–1105. [Google Scholar] [CrossRef]
- Durmuş, D.; Alayli, G.; Uzun, O.; Tander, B.; Cantürk, F.; Bek, Y.; Erkan, L. Effects of Two Exercise Interventions on Pulmonary Functions in Patients with Ankylosing Spondylitis. Jt. Bone Spine 2009, 76, 150–155. [Google Scholar] [CrossRef]
- Wang, A.; Wang, C. Research on the Application of Sport Dance in Colleges and Universities in the Healthy Development of Sports. Rev. Bras. Med. Esporte 2021, 27, 464–467. [Google Scholar] [CrossRef]
- Salari, N.; Hasheminezhad, R.; Hosseinian-Far, A.; Rasoulpoor, S.; Assefi, M.; Nankali, S.; Nankali, A.; Mohammadi, M. Global prevalence of sleep disorders during menopause: A meta-analysis. Sleep Breath. 2023, 27, 1883–1897. [Google Scholar] [CrossRef] [PubMed]
- Maki, P.M.; Panay, N.; Simon, J.A. Sleep disturbance associated with the menopause. Menopause 2024, 31, 724–733. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Yang, R.; Li, C.; Tao, M. Sleep Disorder, an Independent Risk Associated with Arterial Stiffness in Menopause. Sci. Rep. 2017, 7, 1904. [Google Scholar] [CrossRef]
- Acute Physiological Effects of Greek Traditional Dancing. Available online: https://clinicaltrials.gov/study/NCT06260124 (accessed on 7 June 2024).


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study ID and Year | Country/Type | Sample (EG/CG) | Average Age (EG/CG) | Type of Intervention | Intervention Cycle | Duration of Intervention (Hours) | Weekly Intervention Frequency | Total Duration of Intervention | |
|---|---|---|---|---|---|---|---|---|---|
| EG | CG | ||||||||
| Waer et al., 2024 [23] | Tunisia/RCT | EG: 16, CG (Pilates group): 16, CG (waiting group): 16 | 57 ± 2 | Zumba | The Pilates group performed training/the control group had no program | 12 weeks | Each session lasted 60 min | 3 times a week | 2160 min |
| Martins et al., 2023 [24] | Brazil/RCT | EG:23, CG:24 | None | Jazz | No changes in lifestyle and physical exercise habits (no dancing of any kind) | 16 weeks | Each class lasted 60 min | 2 times a week | 1920 min |
| Janyacharoen et al., 2015 [25] | Thailand/RCT | EG:31, CG:32 | EG: 54.6 ± 6.4 CG: 53.7 ± 7.8 | Thai Traditional Dance | No exercise program or general health guidance | 6 weeks | 60 min each time | 3 times a week | 1080 min |
| So et al., 2012 [17] | Korea/RCT | EG:14, CG:13 | EG: 50.2 CG: 51.1 | DMT | Non-intervention | 15 weeks | 90 min each time | 1 time a week | 1350 min |
| Zhao, 2006 [22] | China/RCT | EG:38, CG:22 | 47.4 ± 2.9 | Sports Dance | Daily activities | 6 months | Each session was more than 50 min | 5–6 days a week | 4800–7200 min |
| Kim et al., 2012 [18] | Korea/RCT | EG:10, CG:10 | EG: 55.5 ± 3.5 CG: 57.0 ± 3.3 | Sports Dance | None | 8 weeks | 60 min each time | 3 times a week | 2400 min |
| Kim, 2023 [20] | Korea/RCT | EG:8, CG:8 | EG: 53 ± 3.9 CG: 54.0 ± 4.2 | Korean Traditional Dance | None | 12 weeks | 60 min each time | 3 times a week | 2160 min |
| Kim, 2006 [19] | Korea/non-RCT | EG:35, CG:35 | None | Sports Dance | None | 12 weeks | 50 min each time | 3 times a week | 1800 min |
| Pan, 2004 [21] | China/non-RCT | EG:41, CG:40 | None | Sports Dance | Free time | 6 months | 60–90 min each time | 4–6 times a week | 2880–6480 min |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liao, D.; Mo, L.; Chen, M. The Effectiveness of Dance Interventions on Health-Related Outcomes in Perimenopausal, Menopausal, and Postmenopausal Women: A Systematic Review and Meta-Analysis. Healthcare 2025, 13, 881. https://doi.org/10.3390/healthcare13080881
Liao D, Mo L, Chen M. The Effectiveness of Dance Interventions on Health-Related Outcomes in Perimenopausal, Menopausal, and Postmenopausal Women: A Systematic Review and Meta-Analysis. Healthcare. 2025; 13(8):881. https://doi.org/10.3390/healthcare13080881
Chicago/Turabian StyleLiao, Diying, Lili Mo, and Maowei Chen. 2025. "The Effectiveness of Dance Interventions on Health-Related Outcomes in Perimenopausal, Menopausal, and Postmenopausal Women: A Systematic Review and Meta-Analysis" Healthcare 13, no. 8: 881. https://doi.org/10.3390/healthcare13080881
APA StyleLiao, D., Mo, L., & Chen, M. (2025). The Effectiveness of Dance Interventions on Health-Related Outcomes in Perimenopausal, Menopausal, and Postmenopausal Women: A Systematic Review and Meta-Analysis. Healthcare, 13(8), 881. https://doi.org/10.3390/healthcare13080881