
Effects of Physical Exercise on Symptoms and Quality of Life in Women in Climacteric: A Systematic Review and Meta-Analysis


 , , , and
, , , and
Abstract
1. Introduction
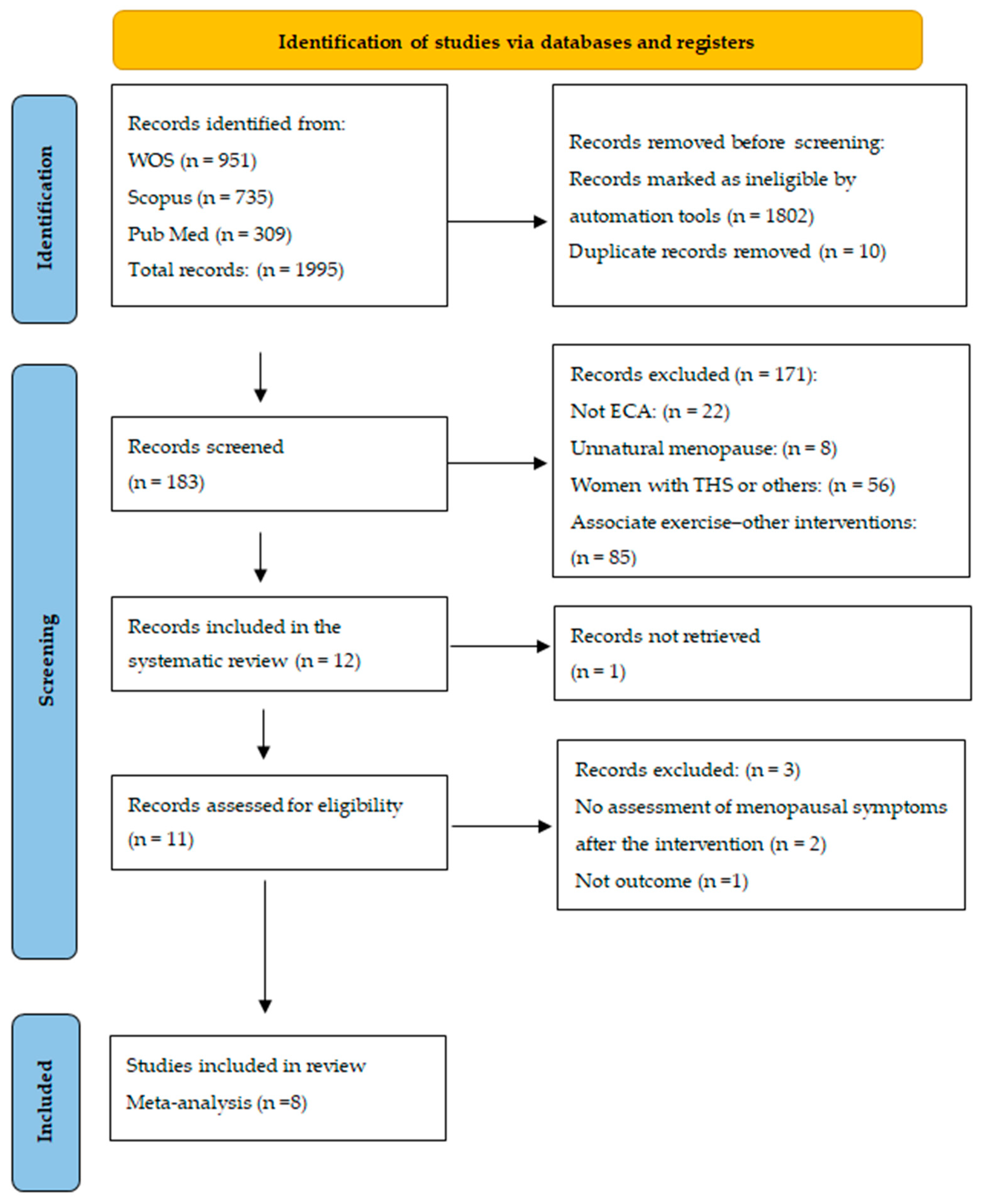
2. Materials and Methods
2.1. Study Design and Selection Criteria
- Patients (P): women in perimenopause, menopause, and postmenopause (stages included in climacteric), aged between 40 and 70 years. Studies of women with unnatural menopause or postmenopause and with medical conditions that could significantly influence physical activity or climacteric symptoms were excluded.
- Interventions (I): AE such as warm-up, walking, mobility, and stretching with relaxation and RT with machines and/or strengthening with elastic bands. The minimum required duration of the intervention was 12 weeks, with 1–3 sessions/week, to ensure sufficient time to observe significant changes in the health of the women. Studies focusing on physical activity combined with other interventions (diet and/or medication) where the effects of physical activity could not be isolated or mental activities such as yoga, tai chi, Pilates, etc., were excluded.
- Comparators (C): groups with no intervention, minimal intervention, or placebo (health education without physical activity) and groups with activity, compared according to QoL scores. Studies with groups with interventions that were not well defined were excluded.
- Outcomes (O): symptoms related to menopause, such as hot flashes, insomnia, and mood changes, among others, and HRQOL assessment using validated questionnaires (Menopause-specific Quality of Life [MENQOL], SF-36 and SF-12) and the Cervantes scale. Studies in which symptoms of menopause were not evaluated after physical activity were excluded.
2.2. Data Collection and Publication Bias
2.3. Statistical Analysis
3. Results
3.1. Characteristics of the Studies
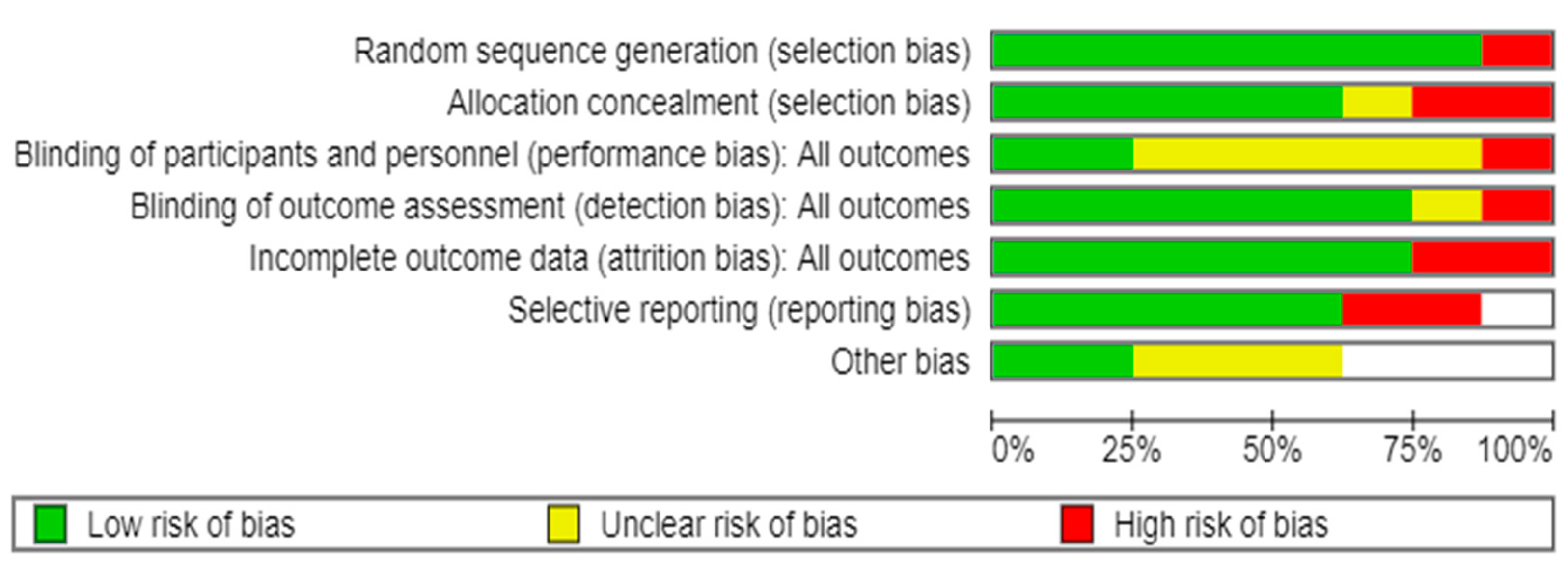
3.2. Quality Assessment
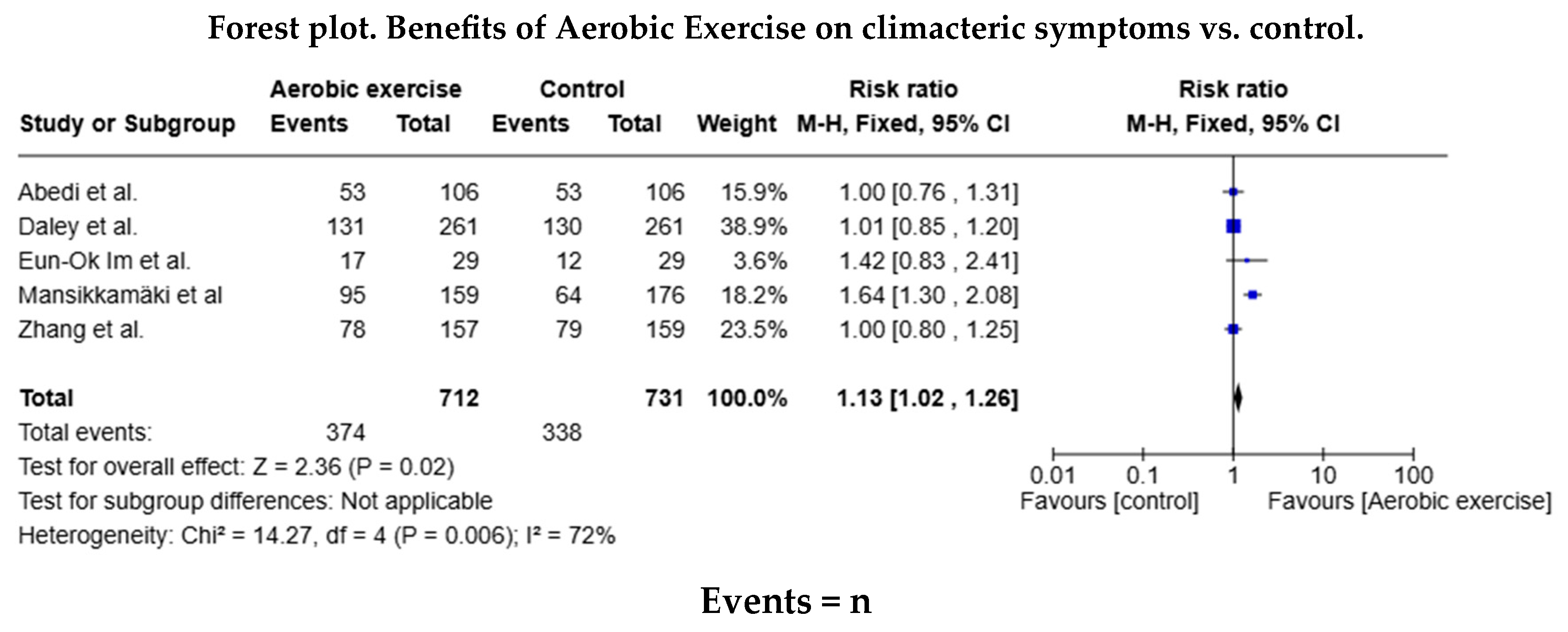
3.3. Effects of AE on Climacteric Symptoms and Quality of Life
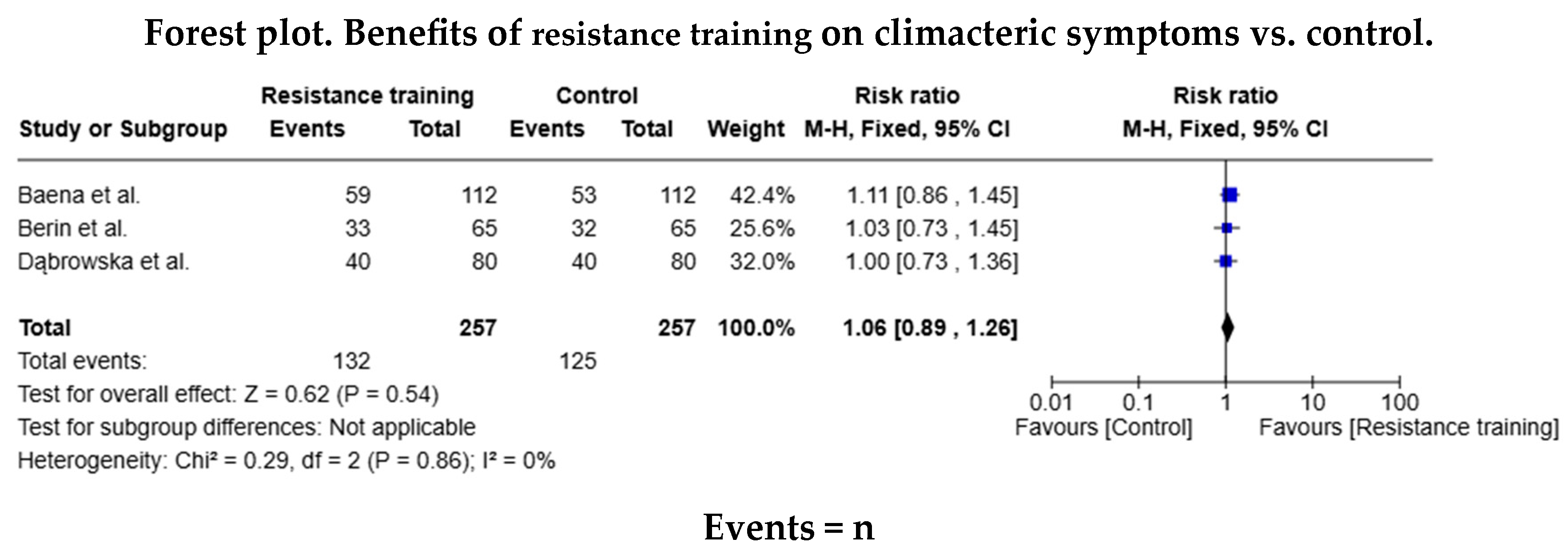
3.4. Effects of RT on Climacteric Symptoms and Quality of Life
3.5. Meta-Analysis Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ACSM | American College of Sports Medicine |
| AE | Aerobic exercise |
| AEEM | Association for the Study of Menopause |
| AHA | American Health Association |
| HRQOL | Health-related quality of life |
| MENQOL | Menopause-specific Quality of Life |
| QoL | Quality of life |
| RCTs | Randomised controlled trials |
| RT | Resistance training |
| VMSs | Vasomotor symptoms |
| WHQ | Women’s Health Questionnaire |
| WHO | The World Health Organization |
References
- Turiño Sarduy, M.I.; Colomé González, T.; Fuentes Guirola, E.; Palmas Mora, S. Síntomas y enfermedades asociadas al climaterio y la menopausia. Medicentro Electrónica 2019, 23, 116–124. [Google Scholar]
- Sochocka, M.; Karska, J.; Pszczołowska, M.; Ochnik, M.; Fułek, M.; Fułek, K.; Kurpas, D.; Chojdak-Łukasiewicz, J.; Rosner-Tenerowicz, A.; Leszek, J. Cognitive Decline in Early and Premature Menopause. Int. J. Mol. Sci. 2023, 24, 6566. [Google Scholar] [CrossRef]
- Vanderzalm, J.; Deschenes, S.; Kunyk, D. Women’s health nurses’ experiences of menopause. Nurs. Manag. (Harrow) 2023, 54, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, C.; Beck, V.; Brewis, J.; Davies, A.; Duberley, J. Menopause and the workplace: New directions in HRM research and HR practice. Hum. Resour. Manag. J. 2021, 31, 49–64. [Google Scholar] [CrossRef]
- Santos, M.A.D.; Vilerá, A.N.; Wysocki, A.D.; Pereira, F.H.; Oliveira, D.M.; Santos, V.B. Sleep quality and its association with menopausal and climacteric symptoms. Rev. Bras. Enferm. 2021, 74 (Suppl. S2), e20201150. [Google Scholar] [CrossRef]
- Curta, J.C.; Weissheimer, A.M. Perceptions and feelings about physical changes in climacteric women. Rev. Gaucha Enferm. 2020, 41, e20190198. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.M.; Do, T.T.T.; Tran, T.N.; Kim, J.H. Exercise and Quality of Life in Women with Menopausal Symptoms: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2020, 17, 7049. [Google Scholar] [CrossRef]
- González León, F.M.; Baabel Zambrano, N.S.; Romero Sacoto, L.A.; Faican Rocano, P.F. Calidad de vida en mujeres posmenopáusicas. Vive Rev. Salud 2021, 4, 35–43. [Google Scholar] [CrossRef]
- Costa, J.G.; Giolo, J.S.; Mariano, I.M.; Batista, J.P.; Ribeiro, A.L.A.; Souza, T.C.F.; de Oliveira, E.P.; Resende, A.P.M.; Puga, G.M. Combined exercise training reduces climacteric symptoms without the additive effects of isoflavone supplementation: A clinical, controlled, randomised, double-blind study. Nutr. Health Bicester 2017, 23, 271–279. [Google Scholar] [CrossRef]
- Gómez, C.; Martínez Gil, J.L.; Carrasco, J.J.; Alakhdar, Y.; Chulvi-Medrano, I. Efectos de un año de entrenamiento con bandas elásticas sobre el dolor en mujeres menopáusicas. Fisioterapia 2018, 40, 178–182. [Google Scholar] [CrossRef]
- Harper, J.C.; Phillips, S.; Biswakarma, R.; Yasmin, E.; Saridogan, E.; Radhakrishnan, S.; Davies, M.C.; Talaulikar, V. An online survey of perimenopausal women to determine their attitudes and knowledge of the menopause. Womens Health 2022, 18, 17455057221106890. [Google Scholar] [CrossRef] [PubMed]
- Santoro, N.; Roeca, C.; Peters, B.A.; Neal-Perry, G. The Menopause Transition: Signs, Symptoms, and Management Options. J. Clin. Endocrinol. Metab. 2021, 106, 1–15. [Google Scholar] [CrossRef]
- Geraci, A.; Calvani, R.; Ferri, E.; Marzetti, E.; Arosio, B.; Cesari, M. Sarcopenia and Menopause: The Role of Estradiol. Front. Endocrinol. 2021, 12, 682012. [Google Scholar] [CrossRef]
- Buckinx, F.; Aubertin-Leheudre, M. Sarcopenia in Menopausal Women: Current Perspectives. Int. J. Womens Health 2022, 14, 805–819. [Google Scholar] [CrossRef] [PubMed]
- Thuraisingham, C.; Nalliah, S. Is menopause managed well enough in general practice? Malays. Fam. Physician 2023, 18, 49–100. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Baena-García, L.; Flor-Alemany, M.; Marín-Jiménez, N.; Aranda, P.; Aparicio, V.A. A 16-week multicomponent exercise training program improves menopause-related symptoms in middle-aged women. The FLAMENCO project randomized control trial. Menopause 2022, 29, 537–544. [Google Scholar] [CrossRef]
- Almeida, J.N.; Prado, W.L.; Terra, C.M.; Oliveira, M.G.; Garcia, R.A.; Pinfildi, C.E.; Botero, J.P. Effects of photobiomodulation on muscle strength in post-menopausal women submitted to a resistance training program. Lasers Med. Sci. 2020, 35, 355–363. [Google Scholar] [CrossRef] [PubMed]
- Alonso-Domínguez, R.; Sánchez-Aguadero, N.; Llamas-Ramos, I.; Lugones-Sánchez, C.; González-Sánchez, S.; Gómez-Marcos, M.A.; García-Ortiz, L.; Ewomen Investigators. Effect of an intensive intervention on the increase of physical activity and the decrease of sedentary lifestyle in inactive postmenopausal. J. Adv. Nurs. 2021, 77, 2064–2072. [Google Scholar] [CrossRef]
- Berin, E.; Hammar, M.; Lindblom, H.; Lindh-Åstrand, L.; Spetz Holm, A.C. Effects of resistance training on quality of life in postmenopausal women with vasomotor symptoms. Climacteric J. Int. Menopause Soc. 2021, 25, 264–270. [Google Scholar] [CrossRef]
- Daley, A.J.; Thomas, A.; Roalfe, A.K.; Stokes-Lampard, H.; Coleman, S.; Rees, M.; Hunter, M.S.; MacArthur, C. The effectiveness of exercise as treatment for vasomotor menopausal symptoms: Randomised controlled trial. BJOG-Int. J. Obstet. Gynaecol. 2015, 122, 565–575. [Google Scholar] [CrossRef]
- Vilagut, G.; Ferrer, M.; Rajmil, L.; Rebollo, P.; Permanyer-Miralda, G.; Quintana, J.M.; Santed, R.; Valderas, J.M.; Domingo-Salvany, A.; Alonso, J. El Cuestionario de Salud SF-36 español: Una década de experiencia y nuevos desarrollos. Gac. Sanit. 2005, 19, 135–150. [Google Scholar] [CrossRef]
- Vera-Villarroel, P.; Silva, J.; Celis-Atenas, K.; Pavez, P. Evaluación del cuestionario SF-12: Verificación de la utilidad de la escala salud mental. Rev. Médica Chile 2014, 142, 1275–1283. [Google Scholar] [CrossRef] [PubMed]
- Ayala-Peralta, F.; Rodriguez-Herrera, M.A.; Izaguirre-Lucano, H.; Ayala-Palomino, R.; Quiñones-Vásquez, L.A.; Ayala-Moreno, D.; Luna-Figueroa, A.; Carranza-Asmat, C.; Ochante-Rementería, J. Instrumentos utilizados para la medición de la calidad de vida relacionada con la salud durante el climacterio. Rev. Peru Investig. Materno Perinat. 2016, 5, 55–65. [Google Scholar] [CrossRef]
- Palacios, S.; Ferrer-Barriendos, J.; Parrilla, J.J.; Castelo-Branco, C.; Manubens, M.; Alberich, X.; Martí, A. Calidad de vida relacionada con la salud en la mujer española durante la perimenopausia y posmenopausia. Desarrollo y validación de la Escala Cervantes. Med. Clínica 2004, 122, 205–211. [Google Scholar] [CrossRef] [PubMed]
- PRISMA 2020. PRISMA Statement. Available online: https://www.prisma-statement.org/prisma-2020 (accessed on 10 September 2024).
- Zotero|Tu Asistente Personal de Investigación. Available online: https://www.zotero.org/ (accessed on 10 September 2024).
- RoB 2: Una Herramienta Cochrane Revisada Para Medir el Riesgo de Sesgo en Ensayos Aleatorizados|Cochrane Bias. Available online: https://methods.cochrane.org/bias/resources/rob-2-revised-cochrane-risk-bias-tool-randomized-trials (accessed on 10 September 2024).
- Zhang, J.; Chen, G.; Lu, W.; Yan, X.; Zhu, S.; Dai, Y.; Xi, S.; Yao, C.; Bai, W. Effects of physical exercise on health-related quality of life and blood lipids in perimenopausal women: A randomized placebo-controlled trial. Menopause-J. N. Am. Menopause Soc. 2014, 21, 1269–1276. [Google Scholar] [CrossRef]
- Abedi, P.; Nikkhah, P.; Najar, S. Effect of pedometer-based walking on depression, anxiety and insomnia among postmenopausal women. Climacteric 2015, 18, 841–845. [Google Scholar] [CrossRef]
- Mansikkamaki, K.; Raitanen, J.; Nygard, C.H.; Tomas, E.; Rutanen, R.; Luoto, R. Long-term effect of physical activity on health-related quality of life among menopausal women: A 4-year follow-up study to a randomised controlled trial. BMJ Open 2015, 5, e008232. [Google Scholar] [CrossRef]
- Dąbrowska, J.; Dąbrowska-Galas, M.; Rutkowska, M.; Michalski, B.A. Twelve-week exercise training and the quality of life in menopausal women—Clinical trial. Przeglad Menopauzalny 2016, 15, 20–25. [Google Scholar] [CrossRef]
- Im, E.O.; Kim, S.; Ji, X.; Park, S.; Chee, E.; Chee, W.; Tsai, H.M. Improving menopausal symptoms through promoting physical activity: A pilot Web-based intervention study among Asian Americans. Menopause-J. N. Am. Menopause Soc. 2017, 24, 653–662. [Google Scholar] [CrossRef]
- Revisiones Cochrane|Cochrane Library. Available online: https://www.cochranelibrary.com/es/ (accessed on 29 September 2024).
- Mascort, C.; Beltran i Vilella, M.; Solanas, P.; Vargas, S.; Saura, S.; Adalid, C. Validez y fiabilidad de la prueba de Kupperman. Clínica E Investig. En Ginecol. Obstet. 2008, 35, 126–130. [Google Scholar] [CrossRef]
- Asghari, M.; Mirghafourvand, M.; Mohammad-Alizadeh-Charandabi, S.; Malakouti, J.; Nedjat, S. Effect of aerobic exercise and nutrition education on quality of life and early menopause symptoms: A randomized controlled trial. Women Health 2017, 57, 173–188. [Google Scholar] [CrossRef] [PubMed]
- Menoguías—Aeem. 24 August 2022. Available online: https://aeem.es/nuevas-menoguias-para-profesionales/ (accessed on 23 October 2024).
- Mendoza, N.; De Teresa, C.; Cano, A.; Godoy, D.; Hita-Contreras, F.; Lapotka, M.; Llaneza, P.; Manonelles, P.; Martínez-Amat, A.; Ocón, O.; et al. Benefits of physical exercise in postmenopausal women. Maturitas 2016, 93, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Avilés-Martínez, M.A.; Lopez Roman, F.J.; Galiana Gómez de Cádiz, M.J.; Arnau Sánchez, J.; Martinez Ros, M.T.; Fernandez Lopez, L.; Garcia Sanchez, E.; Menárguez Puche, J.F. Benefits of a community physical exercise program prescribed from primary care for perimenopausal/menopausal women. Aten. Primaria 2022, 54, 102119. [Google Scholar] [CrossRef]
- Taylor, T.R.; Dash, C.; Sheppard, V.; Makambi, K.; Ma, X.; Adams-Campbell, L.L. The effect of a randomized controlled physical activity trial on health related quality of life in metabolically unhealthy African-American women: FIERCE STUDY. Contemp. Clin. Trials 2018, 67, 121–128. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Participants and Climacteric Stage | Groups | Interventions/Times | HRQOL Measurement | Outcomes |
|---|---|---|---|---|---|
| Daley et al., 2015 [20] United Kingdom | n = 261 Age = 48–57 years Perimenopause Postmenopause | Experimental group: (n = 131) Control Group: (n = 130) | Experimental Group: AE (30 min 3 days/week) Time: 6 months Control Group: social support for exercise | WHQ: measures women’s health SF-12: QoL | Aerobic exercise improves women’s quality of life but does not reduce hot flushes and night sweats |
| Zhang et al., 2014 [28] Beijing | n = 157 Age = 40–55 years Perimenopause | Experimental group: (n = 78) Control group: (n = 79) | Experimental group: AE (walking 4000 steps) Frequency: 3 times/week Duration: 30 min/session Time: 12 weeks Control group: usual care | Kupperman Index: assesses the severity of menopause-related symptoms | AE substantially reduces menopausal symptoms |
| Abedi et al., 2015 [29] Iran | n = 106 Age = 40–60 years Postmenopause | Experimental group: (n = 53) Control group: (n = 53) | Experimental group: AE (walking with a pedometer, increasing by 500 steps/week) Time: 12 weeks Control group: usual care | GHQ28 and BECK: measures anxiety, depression and insomnia | AE decreases effects on depression, insomnia, and anxiety |
| Mansikkamäki et al., 2015 [30] Finland | n = 159 Age = 40–63 years Menopause | Experimental group: (n = 95) Control group: (n = 64) | Experimental group: AE (walking or Nordic 2 days a week) Frequency: 4 times/week Duration: 50 min Time: 12 weeks Control group: habitual physical activity | SF-36: measure QoL | Improves physical and mental dimensions of quality of life |
| Dąbrowska et al., 2016 [31] Poland | n = 80 Age = 40–65 years Menopause | Experimental group: (n = 40) Control group: (n = 40) | Experimental group: RT Frequency: 3 times/week Duration: 60 min Time: 12 weeks Control group: habitual physical activity | SF-36: measures QoL | Positive change in vitality and mental health |
| Eun-Ok Im et al., 2017 [32] United States | n = 29 Age = 40–60 years Menopause | Experimental group: (n = 17) Control group: (n = 12) | Experimental group: AE (training and information program to increase physical activity) Time: 3 months Control group: no access to the program | MSI: measures psychic, psychosomatic and physical symptoms Kaiser Physical Activity Survey: measures physical activity | Improves menopause symptoms + mood and physical endurance |
| Berin et al., 2021 [19] Sweden | n = 65 Age = 45–70 years Postmenopause | Experimental group: (n = 33) Control group: (n = 32) | Experimental group: RT (muscle strengthening and stretching) Time: 15 weeks Control group: usual care | WHQ: measures women’s health SF-36: measures QoL | Improves postmenopausal symptoms (hot flushes and night sweats) |
| Baena et al., 2022 [16] Spain | n = 112 Age = 45–60 years Menopause | Experimental group: (n = 59) Control group: (n = 53) | Experimental group: RT (balance training, muscle strengthening) Frequency: 3 times/week Duration: 60 min Time: 12 weeks Control group: 4 talks on the health benefits of physical exercise and the Mediterranean dietary pattern | Cervantes Scale: measures HRQoL in menopause | Improves menopause symptoms, relationship quality, mood, and VMSs |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trujillo-Muñoz, P.J.; Sánchez-Ojeda, M.A.; Rodríguez-Huamán, E.C.; Mezyani-Haddu, K.; Hoyo-Guillot, I.; Navarro-Prado, S. Effects of Physical Exercise on Symptoms and Quality of Life in Women in Climacteric: A Systematic Review and Meta-Analysis. Healthcare 2025, 13, 644. https://doi.org/10.3390/healthcare13060644
Trujillo-Muñoz PJ, Sánchez-Ojeda MA, Rodríguez-Huamán EC, Mezyani-Haddu K, Hoyo-Guillot I, Navarro-Prado S. Effects of Physical Exercise on Symptoms and Quality of Life in Women in Climacteric: A Systematic Review and Meta-Analysis. Healthcare. 2025; 13(6):644. https://doi.org/10.3390/healthcare13060644
Chicago/Turabian StyleTrujillo-Muñoz, Providencia Juana, María Angustias Sánchez-Ojeda, Eva Carolina Rodríguez-Huamán, Karima Mezyani-Haddu, Irene Hoyo-Guillot, and Silvia Navarro-Prado. 2025. "Effects of Physical Exercise on Symptoms and Quality of Life in Women in Climacteric: A Systematic Review and Meta-Analysis" Healthcare 13, no. 6: 644. https://doi.org/10.3390/healthcare13060644
APA StyleTrujillo-Muñoz, P. J., Sánchez-Ojeda, M. A., Rodríguez-Huamán, E. C., Mezyani-Haddu, K., Hoyo-Guillot, I., & Navarro-Prado, S. (2025). Effects of Physical Exercise on Symptoms and Quality of Life in Women in Climacteric: A Systematic Review and Meta-Analysis. Healthcare, 13(6), 644. https://doi.org/10.3390/healthcare13060644