
Cross-Cultural Adaptation, Validity and Reliability of the European Portuguese Version of the Kerlan-Jobe Orthopaedic Clinic Shoulder & Elbow Score (KJOC)

 , ,
, ,  , , , , and
, , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Translation and Cultural Adaptation
2.3. Participants
2.4. Eligibility Criteria
2.5. Instruments and Variables
2.6. Data Analysis
3. Results
3.1. Translation and Cultural Adaptation
3.2. Characterization of the Sample
3.3. Internal Consistency of the KJOC-PT
3.4. Validation of the Internal Structure of the KJOC-PT
3.5. Convergent Validity of the KJOC-PT
3.6. Reliability (Between-Day Test-Retest, Measurement Error and Agreement)
3.7. Floor and Ceiling Effect
4. Discussion
4.1. Translation and Cultural Adaptation
4.2. Internal Consistency
4.3. Convergent Validity
4.4. Reliability: Test-Retest
4.5. Measurement Error
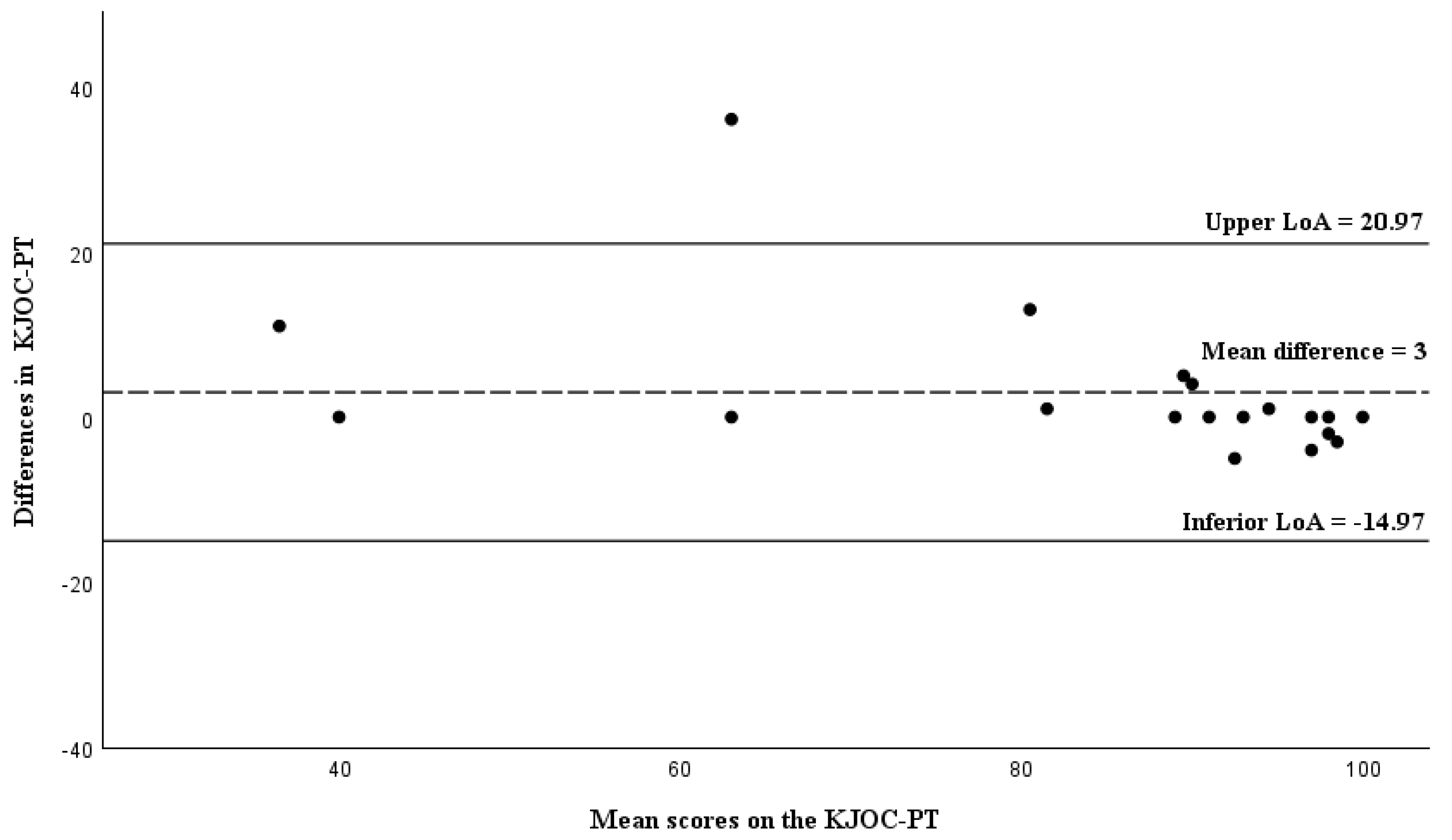
4.6. Agreement: Bland-Altman Analysis
4.7. Floor and Ceiling Effect
4.8. Limitations of the Study
4.9. Implications for Clinical and Sport Contexts and Suggestions for Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Total Number of Athletes (n = 100) | Asymptomatic Athletes (n = 30) | Symptomatic Athletes (n = 70) | ||
|---|---|---|---|---|
| Sports | Handball | 19 (18.6%) | 6 (20.0%) | 13 (18.6%) |
| Basketball | 7 (6.9%) | 4 (13.3%) | 3 (4.3%) | |
| Swimming | 11(10.8%) | 3 (10%) | 8 (11.4%) | |
| Football | 2 (2.0%) | 0 (0.0%) | 2 (2.9%) | |
| Volleyball | 21 (20.6%) | 5 (16.7%) | 16 (22.9%) | |
| Futsal | 1 (1.0%) | 1 (3.3%) | 0 (0.0%) | |
| Padel | 18(17.6%) | 9 (30.0%) | 9 (12.9%) | |
| Tennis | 1 (1.0%) | 0 (0.0%) | 1 (1.4%) | |
| Gymnastics | 6 (5.9%) | 0 (0.0%) | 6 (8.6%) | |
| Rugby | 1 (1.0%) | 0 (0.0%) | 1 (1.4%) | |
| Crossfit | 9 (8.8%) | 1 (3.3%) | 8 (11.4%) | |
| Table tennis | 4 (3.9%) | 1(3.3%) | 3 (4.3%) | |
| Level of practice | Professional | 19 (18.6%) | 4 (13.3%) | 15 (21.4%) |
| Semi-professional | 30 (29.4%) | 8 (26.7%) | 22 (31.4%) | |
| Amateur | 46 (45.1%) | 17 (56.7%) | 29 (41.4%) | |
| University sports | 2 (2.0%) | 0 (0.0%) | 2 (2.9%) | |
| School sports | 3 (2.9%) | 1 (3.3%) | 2 (2.9%) | |
| Types of injuries | Shoulder fracture | 1 (1.0%) | - | 1 (1.4%) |
| Elbow fracture | 0 (0.0%) | - | 0 (0.0%) | |
| Dislocation | 8 (7.8%) | - | 8 (11.4%) | |
| Biceps brachii tendon rupture | 0 (0.0%) | - | 0 (0.0%) | |
| Rotator cuff tendon rupture | 1 (1.0%) | - | 1 (1.4%) | |
| Bone edema | 1 (1.0%) | - | 1 (1.4%) | |
| SLAP | 2 (2.0%) | - | 2 (2.9%) | |
| Bennett lesion | 0 (0.0%) | - | 0 (0.0%) | |
| Shoulder tendinopathy | 29 (28.4%) | - | 29 (41.4%) | |
| Epicondylitis | 6 (5.9%) | - | 6 (8.6%) | |
| Epitrochleitis | 4 (3.9%) | - | 4 (5.7%) | |
| Presence of intra-articular bodies | 1 (1.0%) | - | 1 (1.4%) | |
| Other injury | 17 (16.7%) | - | 17 (24.3%) |
| KJOC | Corrected Total Item Correlation | Cronbach’s Alpha If Item Is Excluded |
|---|---|---|
| Q1 | 0.422 | 0.941 |
| Q2 | 0.703 | 0.933 |
| Q3 | 0.839 | 0.923 |
| Q4 | 0.644 | 0.933 |
| Q5 | 0.680 | 0.932 |
| Q6 | 0.847 | 0.923 |
| Q7 | 0.815 | 0.924 |
| Q8 | 0.835 | 0.924 |
| Q9 | 0.863 | 0.923 |
| Q10 | 0.841 | 0.924 |
| KJOC-PT | Total Number of Athletes (n = 31) | Asymptomatic Athletes (n = 12) | Symptomatic Athletes (n = 19) |
|---|---|---|---|
| ICC2,1 [95% CI] Cronbach’s α | |||
| Q1 | 0.55 [0.24–0.76] 0.70 | 0.83 [0.52–0.95] 0.91 | 0.49 [0.46–0.77] 0.65 |
| Q2 | 0.80 [0.62–0.90] 0.90 | 0.72 [0.31–0.91] 0.85 | 0.81 [0.58–0.92] 0.90 |
| Q3 | 0.91 [0.83–0.96] 0.96 | 1 [-] 1 | 0.90 [0.77–0.96] 0.95 |
| Q4 | 0.82 [0.66–0.91] 0.90 | 0.28 [−0.37–0.73] 0.42 | 0.89 [0.73–0.95] 0.94 |
| Q5 | 0.80 [0.63–0.90] 0.89 | 0.08 [−0.57–0.63] 0.14 | 0.84 [0.63–0.93] 0.91 |
| Q6 | 0.72 [0.50–0.86] 0.84 | 0.52 [−0.40–0.83] 0.68 | 0.70 [0.38–0.87] 0.83 |
| Q7 | 0.91 [0.82–0.95] 0.95 | 0.65 [0.16–0.88] 0.78 | 0.92 [0.77–0.97] 0.97 |
| Q8 | 0.92 [0.84–0.96] 0.96 | 0.90 [0.68–0.97] 0.94 | 0.92 [0.80–0.97] 0.96 |
| Q9 | 0.84 [0.69–0.92] 0.91 | 0.63 [0.10–0.88] 0.76 | 0.85 [0.66–0.94] 0.92 |
| Q10 | 0.95 [0.89–0.97] 0.97 | 0.89 [0.66–0.97] 0.94 | 0.95 [0.87–0.98] 0.97 |
References
- Hawkins, R.; Kennedy, J. Impingement Syndrome in Athletes. Am. J. Sports Med. 1980, 8, 151–158. [Google Scholar] [CrossRef] [PubMed]
- Alberta, F.G.; ElAttrache, N.S.; Bissell, S.; Mohr, K.; Browdy, J.; Yocum, L.; Jobe, F. The Development and Validation of a Functional Assessment Tool for the Upper Extremity in the Overhead Athlete. Am. J. Sports Med. 2010, 38, 903–911. [Google Scholar] [CrossRef]
- Kraeutler, M.J.; Ciccotti, M.G.; Dodson, C.C.; Frederick, R.W.; Cammarota, B.; Cohen, S.B. Kerlan-Jobe Orthopaedic Clinic Overhead Athlete Scores in Asymptomatic Professional Baseball Pitchers. J. Shoulder Elb. Surg. 2013, 22, 329–332. [Google Scholar] [CrossRef]
- Painter, D.F.; Quinn, M.; Dove, J.H.; Testa, E.J.; Snow, R.; Byrne, R.A.; Pavlu, M.M.; Jordan, R.; Owens, B.D. Arm Health in Elite Collegiate Summer League Baseball Players Assessed by the Kerlan-Jobe Orthopaedic Clinic Score. J. Athl. Train. 2024, 59, 255–261. [Google Scholar] [CrossRef]
- Leenen, A.J.R.; Hoozemans, M.J.M.; van Dis, F.; van der Graaff, E.; Veeger, H.E.J.; Verhagen, E.A.L.M. Shoulder and Elbow Symptoms in Dutch High School Baseball Pitchers: Results of a Two-Season Prospective Study. J. Athl. Train. 2024, 59, 1118–1125. [Google Scholar] [CrossRef]
- Wilkins, S.J.; Bell, D.R.; Kahanov, L.; Martin, M.; Post, E.G. Early Sport Specialization and Long-Term Throwing Arm Health in College Baseball Players. Sports Health 2023, 15, 746–752. [Google Scholar] [CrossRef]
- Michelin, R.M.; Gornick, B.R.; Schlechter, J.A. Adolescent Athletes Achieve High Levels of Athletic and Daily Function after Arthroscopic Marrow Stimulation for Elbow Capitellar Osteochondritis Dissecans. Arthrosc. Sports Med. Rehabil. 2022, 4, e1985–e1992. [Google Scholar] [CrossRef]
- Jackson, G.R.; Jawanda, H.; Batra, A.; Familiari, F.; Khan, Z.A.; Brusalis, C.M.; Verma, N.N. Elbow Ulnar Collateral Ligament Repair with Suture Augmentation Results in Good Clinical Results, a Return-to-Play Rate between 67% and 93%, and a Postoperative Complication Rate up to 11.9%: A Systematic Review. Arthrosc. Sports Med. Rehabil. 2023, 5, 100761. [Google Scholar] [CrossRef] [PubMed]
- Tsuruike, M.; Ellenbecker, T.S.; Hirose, N. Kerlan-Jobe Orthopaedic Clinic (Kjoc) Score and Scapular Dyskinesis Test in Collegiate Baseball Players. J. Shoulder Elb. Surg. 2018, 27, 1830–1836. [Google Scholar] [CrossRef] [PubMed]
- Steffes, M.J.; Heaps, B.M.; ElAttrache, N.S.; Haselman, W.T. Outcomes after Medial Ulnar Collateral Ligament Graft Repair in Professional Baseball Pitchers with Minimum 2-Year Follow-Up. Orthop. J. Sports Med. 2022, 10, 23259671221092728. [Google Scholar] [CrossRef]
- Desai, S.S.; Alrabaa, R.G.; Alexander, F.J.; Anderson, M.J.; Mastroianni, M.A.; Popkin, C.A.; Ahmad, C.S. Posteromedial Osteophyte Resection in Baseball Players Undergoing Ulnar Collateral Ligament Reconstruction Has No Effect on Return to Play but Decreases Patient-Reported Satisfaction and Throwing Control. Arthrosc. Sports Med. Rehabil. 2023, 5, e833–e838. [Google Scholar] [CrossRef] [PubMed]
- Faherty, M.S.; Plata, A.; Chasse, P.; Zarzour, R.; Sell, T.C. Upper Extremity Musculoskeletal Characteristics and the Kerlan-Jobe Orthopaedic Clinic Questionnaire Score in Collegiate Baseball Athletes. J. Athl. Train. 2019, 54, 945–952. [Google Scholar] [CrossRef] [PubMed]
- Wardell, M.; Creighton, D.; Kovalcik, C. Glenohumeral Instability and Arm Pain in Overhead Throwing Athletes: A Correlational Study. Int. J. Sports Phys. Ther. 2022, 17, 1351–1357. [Google Scholar] [CrossRef]
- Brzoska, R.; Laprus, H.; Malik, S.S.; Solecki, W.; Juszczak, B.; Blasiak, A. Return to Preinjury-Level Sports after Arthroscopic Latarjet for Recurrent Anterior Shoulder Instability in Professional Athletes. Orthop. J. Sports Med. 2023, 11, 23259671231166371. [Google Scholar] [CrossRef]
- Karpinski, K.; Akgün, D.; Gebauer, H.; Festbaum, C.; Lacheta, L.; Thiele, K.; Moroder, P. Arthroscopic Posterior Capsulolabral Repair with Suture-First Versus Anchor-First Technique in Patients with Posterior Shoulder Instability (Type B2): Clinical Midterm Follow-Up. Orthop. J. Sports Med. 2023, 11, 23259671221146167. [Google Scholar] [CrossRef]
- Migliorini, F.; Asparago, G.; Cuozzo, F.; Oliva, F.; Hildebrand, F.; Maffulli, N. Patient Outcomes and Return to Play after Arthroscopic Rotator Cuff Repair in Overhead Athletes: A Systematic Review. J. Orthop. Traumatol. 2023, 24, 3. [Google Scholar] [CrossRef] [PubMed]
- Ishigaki, T.; Kimura, R.; Kikumoto, T.; Matsuura, Y.; Ushiro, K.; Ebihara, Y.; Tanaka, S.; Wada, T.; Jigami, H.; Takahashi, Y.; et al. Comparison of Kerlan-Jobe Orthopaedic Clinic Scores in College Athletes with and without Arm Trouble across Overhead Sports. J. Athl. Train. 2025, 60, 486–491. [Google Scholar] [CrossRef]
- Merolla, G.; Corona, K.; Zanoli, G.; Cerciello, S.; Giannotti, S.; Porcellini, G. Cross-Cultural Adaptation and Validation of the Italian Version of the Kerlan–Jobe Orthopaedic Clinic Shoulder and Elbow Score. J. Orthop. Traumatol. 2017, 18, 415–421. [Google Scholar] [CrossRef]
- Oh, J.H.; Kim, J.Y.; Limpisvasti, O.; Lee, T.Q.; Song, S.H.; Kwon, K.B. Cross-Cultural Adaptation, Validity and Reliability of the Korean Version of the Kerlan-Jobe Orthopedic Clinic Shoulder and Elbow Score. JSES Open Access 2017, 1, 39–44. [Google Scholar] [CrossRef]
- Turgut, E.; Tunay, V.B. Cross-Cultural Adaptation of Kerlan-Jobe Orthopaedic Clinic Shoulder and Elbow Score: Reliability and Validity in Turkish-Speaking Overhead Athletes. Acta Orthop. Traumatol. Turc. 2018, 52, 206–210. [Google Scholar] [CrossRef]
- Fredriksen, H.; Myklebust, G. Norwegian Translation, Cross-Cultural Adaptation and Validation of the Kerlan-Jobe Orthopaedic Clinic Shoulder and Elbow Questionnaire. BMJ Open Sport Exerc. Med. 2019, 5, e000611. [Google Scholar] [CrossRef]
- Moarref, S.; Dehkordi, S.N.; Akbari, M.; Sedighimehr, N. Persian Translation and Cross-Cultural Adaptation of the Kerlan-Jobe Orthopaedic Clinic Shoulder and Elbow Score in Overhead Athletes. Funct. Disabil. J. 2020, 3, 35–44. [Google Scholar] [CrossRef]
- Leenen, A.J.R.; Hurry, A.; van Dis, F.; van der Graaff, E.; Veeger, H.E.J.; Hoozemans, M.J.M. Cross-Cultural Adaption and Validation of the Dutch Version of the Kerlan-Jobe Orthopaedic Clinic Questionnaire in Juvenile Baseball Pitchers. Sports 2022, 10, 163. [Google Scholar] [CrossRef]
- Schulz, C.; Eibl, A.D.; Radovanović, G.; Agres, A.; Nobis, T.; Legerlotz, K. Cross-Cultural Adaptation and Validation of the Kerlan-Jobe Orthopedic Clinic Shoulder and Elbow Score for German-Speaking Overhead Athletes. Physiother. Theory Pract. 2022, 38, 1059–1070. [Google Scholar] [CrossRef] [PubMed]
- Sukanen, M.; Pajari, J.; Äyrämö, S.; Paloneva, J.; Waller, B.; Häkkinen, A.; Multanen, J. Cross-Cultural Adaptation and Validation of the Kerlan-Jobe Orthopaedic Clinic Shoulder and Elbow Score in Finnish-Speaking Overhead Athletes. BMC Sports Sci. Med. Rehabil. 2022, 14, 190. [Google Scholar] [CrossRef]
- Yezhovam, O.; Babenko, Y.; Voropaiev, D.; Petrenko, N.; Tomyn, L. Cross-Cultural Adaptation of the Ukrainian Version of the Kerlan-Jobe Orthopedic Clinic Shoulder and Elbow Score for the Overhead Athletes. Phys. Educ. Sport Health Cult. Mod. Soc. 2023, 2, 86–93. [Google Scholar]
- Bailón-Cerezo, J.; La Touche, R.; Sánchez-Sánchez, B.; de la Rosa-Díaz, I.; Torres-Lacomba, M.; Hernández-Sánchez, S. Spanish Cross-Cultural Adaptation and Validation of the Kerlan-Jobe Orthopaedic Clinic Shoulder and Elbow Score. J. Sport Rehabil. 2024, 33, 12–19. [Google Scholar] [CrossRef]
- Ishigaki, T.; Yokota, H.; Akuzawa, H.; Akiho-Toyoda, N.; Ushiro, K.; Ebihara, Y.; Tanaka, S.; Wada, T.; Jigami, H.; Matsumoto, H.; et al. Translation and Cross-Cultural Adaptation of the Kerlan-Jobe Orthopaedic Clinic Shoulder and Elbow Score into Japanese and Comparison of Visual Analog Scale and 10-Point Scale Formats. Orthop. J. Sports Med. 2024, 12, 23259671241291861. [Google Scholar] [CrossRef]
- Paraskevopoulos, E.; Christakou, A.; Karanasios, S.; Louka, A.P.; Pamboris, G.M.; Papandreou, M. Translation, Adaptation and Validation of the Greek Version of the Kerlan-Jobe Orthopaedic Clinic Shoulder and Elbow Score in Greek Overhead Athletes. J. Funct. Morphol. Kinesiol. 2024, 9, 49. [Google Scholar] [CrossRef] [PubMed]
- Silva, F.; Lima, R.; Santos, G.; Barbosa, G.; Oliveira, V.; Kamonseki, D. Brazilian Version of the Kerlan-Jobe Orthopedic Clinic Shoulder and Elbow Score: Translation and Cross-Cultural Adaptation. Sao Paulo Med. J. 2024, 143, e2024139. [Google Scholar] [CrossRef] [PubMed]
- Beaton, D.E.; Bombardier, C.; Guillemin, F.; Ferraz, M.B. Guidelines for the Process of Cross-Cultural Adaptation of Self-Report Measures. Spine 2000, 25, 3186–3191. [Google Scholar] [CrossRef] [PubMed]
- Hudak, P.; Amadio, P.; Bombardier, C. Development of an Upper Extremity Outcome Measure: The Dash (Disabilities of the Arm, Shoulder and Hand) [Corrected]. The Upper Extremity Collaborative Group (Uecg). Am. J. Ind. Med. 1996, 29, 602–608. [Google Scholar] [CrossRef]
- Santos, J.; Gonçalves, R. Adaptação E Validação Cultural Da Versão Portuguesa Do Disabilities of the Arm Shoulder and Hand—Dash. Rev. Port. Ortop. E Traumatol. 2006, 14, 29–44. [Google Scholar]
- Bland, M.; Altman, D. Statistics Notes: Cronbach’s Alpha. BMJ 1997, 314, 572. [Google Scholar] [CrossRef]
- Terwee, C.B.; Bot, S.D.M.; de Boer, M.R.; van der Windt, D.A.W.M.; Knol, D.L.; Dekker, J.; Bouter, L.M.; de Vet, H.C.W. Quality Criteria Were Proposed for Measurement Properties of Health Status Questionnaires. J. Clin. Epidemiol. 2007, 60, 34–42. [Google Scholar] [CrossRef]
- Kaiser, H.F. An Index of Factorial Simplicity. Psychometrika 1974, 39, 31–36. [Google Scholar] [CrossRef]
- Schober, P.; Boer, C.; Schwarte, L.A. Correlation Coefficients: Appropriate Use and Interpretation. Anesth. Analg. 2018, 126, 1763–1768. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef]
- Bruton, A.; Conway, J.; Holgate, S. Reliability: What Is It, and How Is It Measured? Physiotherapy 2000, 86, 94–99. [Google Scholar] [CrossRef]
- Huang, S.-L.; Hsieh, C.-L.; Wu, R.-M.; Tai, C.-H.; Lin, C.-H.; Lu, W.-S. Minimal Detectable Change of the Timed up & Go Test and the Dynamic Gait Index in People with Parkinson Disease. Phys. Ther. 2011, 91, 114–121. [Google Scholar]
- Katajapuu, N.; Heinonen, A.; Saltychev, M. Minimal Clinically Important Difference and Minimal Detectable Change of the World Health Organization Disability Assessment Schedule 2.0 (Whodas 2.0) Amongst Patients with Chronic Musculoskeletal Pain. Clin. Rehabil. 2020, 34, 1506–1511. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Statistical Methods for Assessing Agreement between Two Methods of Clinical Measurement. Lancet 1986, 327, 307–310. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Measuring Agreement in Method Comparison Studies. Stat. Methods Med. Res. 1999, 8, 135–160. [Google Scholar] [CrossRef] [PubMed]
- McHorney, C.A.; Tarlov, A.R. Individual-Patient Monitoring in Clinical Practice: Are Available Health Status Surveys Adequate? Qual. Life Res. 1995, 4, 293–307. [Google Scholar] [CrossRef] [PubMed]
- Mokkink, L.; Terwee, C.; de Vet, H. Key Concepts in Clinical Epidemiology: Responsiveness, the Longitudinal Aspect of Validity. J. Clin. Epidemiol. 2021, 140, 159–162. [Google Scholar] [CrossRef] [PubMed]



| Total of Athletes (n = 100) | Asymptomatic Athletes (n = 30) | Symptomatic Athletes (n = 70) | p Value | |
|---|---|---|---|---|
| Age (years) | 24 [17] | 23.5 [13] | 24 [20] | 0.592 * |
| Sex, male, n (%) | 72 (72%) | 22 (73.3%) | 50 (71.4%) | 0.122 # |
| Body mass (kg) | 77.3 ± 1.6 | 75.8 ± 3.1 | 77.9 ± 1.8 | 0.489 † |
| Height (m) | 1.8 ± 0.01 | 1.8 ± 0.02 | 1.8 ± 0.01 | 0.608 † |
| BMI (kg/m2) | 24.4 [4.1] | 23.7 [4.6] | 24.5 [4.2] | 0.414 * |
| Training hours (hours/week) | 7 [7.4] | 5 [2.3] | 8 [7] | <0.001 * |
| KJOC-PT (score) | 92 [16] | 98 [12] | 92 [17] | 0.003 * |
| DASH (score) | 1.7 [5.8] | 0 [2.7] | 1.7 [7.5] | 0.018 * |
| DASH Sports (score) | 0 [5–12] | 0 [3.1] | 0 [14.1] | 0.057 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almeida, G.; Amaral, L.; Vilarinho, R.; Magalhães, B.; Silva, F.; Abreu, V.; Magalhães, A.; Esteves, M.; Cervaens, M. Cross-Cultural Adaptation, Validity and Reliability of the European Portuguese Version of the Kerlan-Jobe Orthopaedic Clinic Shoulder & Elbow Score (KJOC). Healthcare 2025, 13, 3081. https://doi.org/10.3390/healthcare13233081
Almeida G, Amaral L, Vilarinho R, Magalhães B, Silva F, Abreu V, Magalhães A, Esteves M, Cervaens M. Cross-Cultural Adaptation, Validity and Reliability of the European Portuguese Version of the Kerlan-Jobe Orthopaedic Clinic Shoulder & Elbow Score (KJOC). Healthcare. 2025; 13(23):3081. https://doi.org/10.3390/healthcare13233081
Chicago/Turabian StyleAlmeida, Gonçalo, Luísa Amaral, Rui Vilarinho, Bárbara Magalhães, Fátima Silva, Verónica Abreu, André Magalhães, Mário Esteves, and Mariana Cervaens. 2025. "Cross-Cultural Adaptation, Validity and Reliability of the European Portuguese Version of the Kerlan-Jobe Orthopaedic Clinic Shoulder & Elbow Score (KJOC)" Healthcare 13, no. 23: 3081. https://doi.org/10.3390/healthcare13233081
APA StyleAlmeida, G., Amaral, L., Vilarinho, R., Magalhães, B., Silva, F., Abreu, V., Magalhães, A., Esteves, M., & Cervaens, M. (2025). Cross-Cultural Adaptation, Validity and Reliability of the European Portuguese Version of the Kerlan-Jobe Orthopaedic Clinic Shoulder & Elbow Score (KJOC). Healthcare, 13(23), 3081. https://doi.org/10.3390/healthcare13233081