
Factors Associated with Decisional Regret After Shared Decision Making for Patients Undergoing Total Knee Arthroplasty

 , ,
, ,  , and
, and
Abstract
1. Introduction
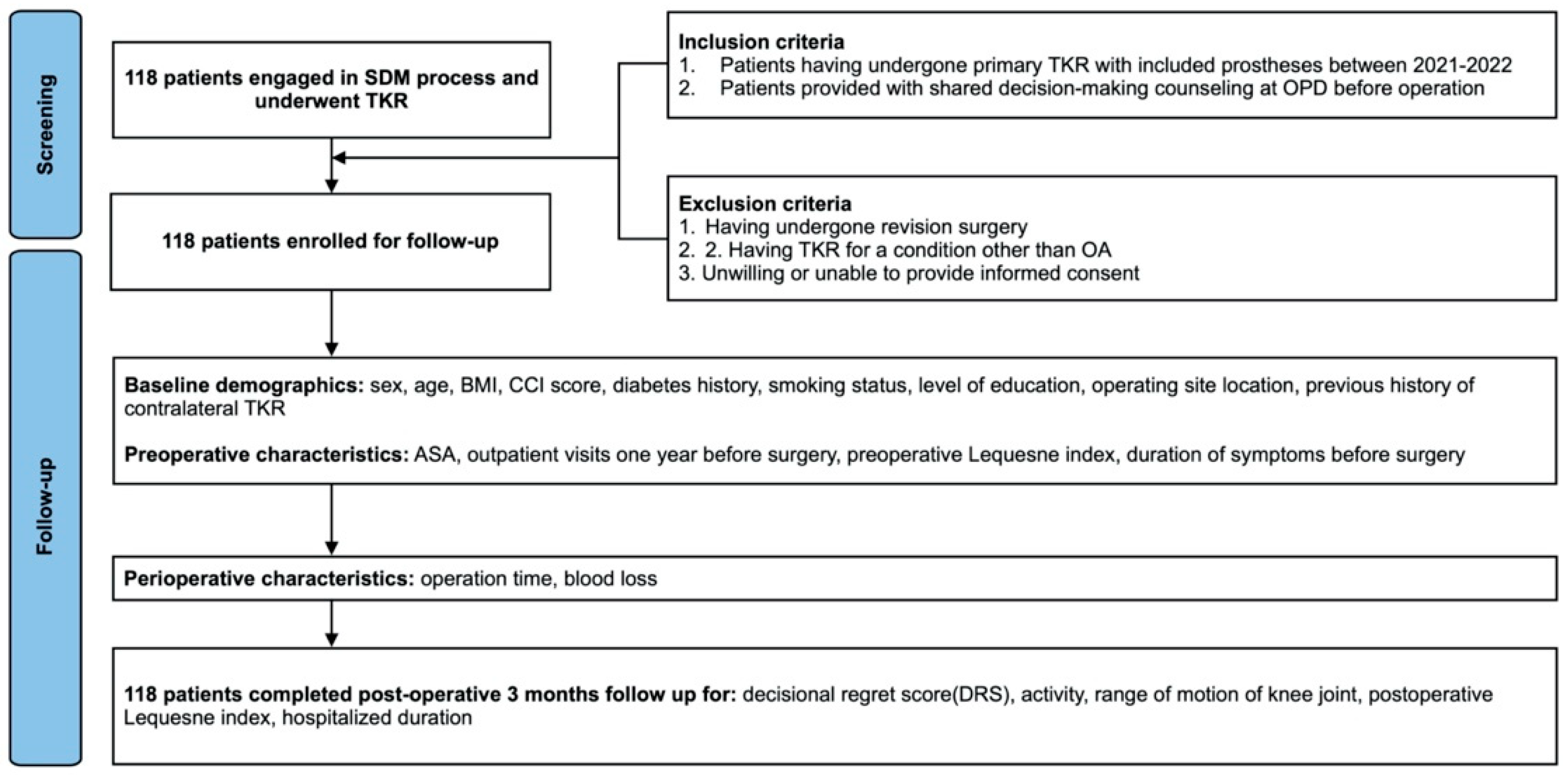
2. Materials and Methods
3. Result
4. Discussion
5. Conclusions
Practice Implications
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Scott, C.; Howie, C.; MacDonald, D.; Biant, L. Predicting dissatisfaction following total knee replacement: A prospective study of 1217 patients. J. Bone Jt. Surg. Br. Vol. 2010, 92, 1253–1258. [Google Scholar] [CrossRef] [PubMed]
- Kahlenberg, C.A.; Nwachukwu, B.U.; McLawhorn, A.S.; Cross, M.B.; Cornell, C.N.; Padgett, D.E. Patient satisfaction after total knee replacement: A systematic review. HSS J. 2018, 14, 192–201. [Google Scholar] [CrossRef] [PubMed]
- Baker, P.; Van der Meulen, J.; Lewsey, J.; Gregg, P. The role of pain and function in determining patient satisfaction after total knee replacement: Data from the National Joint Registry for England and Wales. J. Bone Jt. Surg. Br. Vol. 2007, 89, 893–900. [Google Scholar] [CrossRef] [PubMed]
- Dailiana, Z.H.; Papakostidou, I.; Varitimidis, S.; Liaropoulos, L.; Zintzaras, E.; Karachalios, T.; Michelinakis, E.; Malizos, K.N. Patient-reported quality of life after primary major joint arthroplasty: A prospective comparison of hip and knee arthroplasty. BMC Musculoskelet. Disord. 2015, 16, 1–8. [Google Scholar] [CrossRef]
- Dhurve, K.; Scholes, C.; El-Tawil, S.; Shaikh, A.; Weng, L.K.; Levin, K.; Fritsch, B.; Parker, D.; Coolican, M. Multifactorial analysis of dissatisfaction after primary total knee replacement. Knee 2017, 24, 856–862. [Google Scholar] [CrossRef]
- Jacobs, C.A.; Christensen, C.P. Factors influencing patient satisfaction two to five years after primary total knee arthroplasty. J. Arthroplast. 2014, 29, 1189–1191. [Google Scholar] [CrossRef]
- Ali, A.; Lindstrand, A.; Sundberg, M.; Flivik, G. Preoperative anxiety and depression correlate with dissatisfaction after total knee arthroplasty: A prospective longitudinal cohort study of 186 patients, with 4-year follow-up. J. Arthroplast. 2017, 32, 767–770. [Google Scholar] [CrossRef]
- Zabawa, L.; Li, K.; Chmell, S. Patient dissatisfaction following total knee arthroplasty: External validation of a new prediction model. Eur. J. Orthop. Surg. Traumatol. 2019, 29, 861–867. [Google Scholar] [CrossRef]
- Cassidy, R.S.; Bennett, D.B.; Beverland, D.E.; O’Brien, S. Decision regret after primary hip and knee replacement surgery. J. Orthop. Sci. 2021, 28, 167–172. [Google Scholar] [CrossRef]
- Shimanoff, S.B. Commonly named emotions in everyday conversations. Percept. Mot. Ski. 1984, 58, 514. [Google Scholar] [CrossRef]
- Becerra Pérez, M.M.; Menear, M.; Brehaut, J.C.; Legare, F. Extent and predictors of decision regret about health care decisions: A systematic review. Med. Decis. Mak. 2016, 36, 777–790. [Google Scholar] [CrossRef] [PubMed]
- Faiman, B.; Tariman, J.D. Shared Decision Making: Improving Patient Outcomes by Understanding the Benefits of and Barriers to Effective Communication. Clin. J. Oncol. Nurs. 2019, 23, 540–542. [Google Scholar] [CrossRef] [PubMed]
- Chrenka, E.A.; Solberg, L.I.; Asche, S.E.; Dehmer, S.P.; Ziegenfuss, J.Y.; Whitebird, R.R.; Norton, C.K.M.; Reams, M.M.; Johnson, P.G.; Elwyn, G.M.B. Is shared decision-making associated with better patient-reported outcomes? a longitudinal study of patients undergoing total joint arthroplasty. Clin. Orthop. Relat. Res. 2022, 480, 82–91. [Google Scholar] [CrossRef] [PubMed]
- Suarez-Almazor, M.E.; Richardson, M.; Kroll, T.L.; Sharf, B.F. A qualitative analysis of decision-making for total knee replacement in patients with osteoarthritis. JCR J. Clin. Rheumatol. 2010, 16, 158–163. [Google Scholar] [CrossRef]
- Torrente-Jimenez, R.S.; Feijoo-Cid, M.; Rivero-Santana, A.J.; Perestelo-Pérez, L.; Torres-Castaño, A.; Ramos-García, V.; Bilbao, A.; Serrano-Aguilar, P. Gender differences in the decision-making process for undergoing total knee replacement. Patient Educ. Couns. 2022, 105, 3459–3465. [Google Scholar] [CrossRef]
- Agency for Healthcare Research and Quality. The SHARE Approach—Essential Steps of Shared Decisionmaking: Quick Reference Guide; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2020. [Google Scholar]
- Brehaut, J.C.; O’Connor, A.M.; Wood, T.J.; Hack, T.F.; Siminoff, L.; Gordon, E.; Feldman-Stewart, D. Validation of a decision regret scale. Med. Decis. Mak. 2003, 23, 281–292. [Google Scholar] [CrossRef]
- Ghidini, F.; Sekulovic, S.; Castagnetti, M. Parental decisional regret after primary distal hypospadias repair: Family and surgery variables, and repair outcomes. J. Urol. 2016, 195, 720–724. [Google Scholar] [CrossRef]
- Bourne, R.B.; Chesworth, B.M.; Davis, A.M.; Mahomed, N.N.; Charron, K.D. Patient satisfaction after total knee arthroplasty: Who is satisfied and who is not? Clin. Orthop. Relat. Res. 2010, 468, 57–63. [Google Scholar] [CrossRef]
- Gustke, K.; Golladay, G.; Roche, M.; Jerry, G.; Elson, L.; Anderson, C. Increased satisfaction after total knee replacement using sensor-guided technology. Bone Jt. J. 2014, 96, 1333–1338. [Google Scholar] [CrossRef]
- Beswick, A.D.; Wylde, V.; Gooberman-Hill, R.; Blom, A.; Dieppe, P. What proportion of patients report long-term pain after total hip or knee replacement for osteoarthritis? A systematic review of prospective studies in unselected patients. BMJ Open 2012, 2, e000435. [Google Scholar] [CrossRef]
- Maratt, J.D.; Lee, Y.-y.; Lyman, S.; Westrich, G.H. Predictors of satisfaction following total knee arthroplasty. J. Arthroplast. 2015, 30, 1142–1145. [Google Scholar] [CrossRef] [PubMed]
- Mehta, S.; Perruccio, A.; Palaganas, M.; Davis, A. Do women have poorer outcomes following total knee replacement? Osteoarthr. Cartil. 2015, 23, 1476–1482. [Google Scholar] [CrossRef] [PubMed]
- Krushell, R.J.; Fingeroth, R.J. Primary total knee arthroplasty in morbidly obese patients: A 5-to 14-year follow-up study. J. Arthroplast. 2007, 22, 77–80. [Google Scholar] [CrossRef] [PubMed]
- Teo, B.J.; Chong, H.-C.; Yeo, W.; Tan, A.H. The impact of diabetes on patient outcomes after total knee arthroplasty in an Asian population. J. Arthroplast. 2018, 33, 3186–3189. [Google Scholar] [CrossRef]
- Kim, T.K.; Kwon, S.K.; Kang, Y.G.; Chang, C.B.; Seong, S.C. Functional disabilities and satisfaction after total knee arthroplasty in female Asian patients. J. Arthroplast. 2010, 25, 458–464.e2. [Google Scholar] [CrossRef]
- Howells, N.; Murray, J.; Wylde, V.; Dieppe, P.; Blom, A. Persistent pain after knee replacement: Do factors associated with pain vary with degree of patient dissatisfaction? Osteoarthr. Cartil. 2016, 24, 2061–2068. [Google Scholar] [CrossRef]
- Ha, C.-W.; Park, Y.-B.; Song, Y.-S.; Kim, J.-H.; Park, Y.-G. Increased range of motion is important for functional outcome and satisfaction after total knee arthroplasty in Asian patients. J. Arthroplast. 2016, 31, 1199–1203. [Google Scholar] [CrossRef]
- Devers, B.N.; Conditt, M.A.; Jamieson, M.L.; Driscoll, M.D.; Noble, P.C.; Parsley, B.S. Does greater knee flexion increase patient function and satisfaction after total knee arthroplasty? J. Arthroplast. 2011, 26, 178–186. [Google Scholar] [CrossRef]
- Wylde, V.; Trela-Larsen, L.; Whitehouse, M.R.; Blom, A.W. Preoperative psychosocial risk factors for poor outcomes at 1 and 5 years after total knee replacement: A cohort study of 266 patients. Acta Orthop. 2017, 88, 530–536. [Google Scholar] [CrossRef]
- Vissers, M.M.; Bussmann, J.B.; Verhaar, J.A.; Busschbach, J.J.; Bierma-Zeinstra, S.M.; Reijman, M. (Eds.) Psychological factors affecting the outcome of total hip and knee arthroplasty: A systematic review. In Seminars in Arthritis and Rheumatism; Elsevier: New York, NY, USA, 2012. [Google Scholar]
- Burns, L.C.; Ritvo, S.E.; Ferguson, M.K.; Clarke, H.; Seltzer Ze Katz, J. Pain catastrophizing as a risk factor for chronic pain after total knee arthroplasty: A systematic review. J. Pain Res. 2015, 8, 21–32. [Google Scholar]
- Lewis, G.; Rice, D.; McNair, P.; Kluger, M. Predictors of persistent pain after total knee arthroplasty: A systematic review and meta-analysis. Br. J. Anaesth. 2015, 114, 551–561. [Google Scholar] [CrossRef] [PubMed]
- Van Onsem, S.; Van Der Straeten, C.; Arnout, N.; Deprez, P.; Van Damme, G.; Victor, J. A new prediction model for patient satisfaction after total knee arthroplasty. J. Arthroplast. 2016, 31, 2660–2667.e1. [Google Scholar] [CrossRef] [PubMed]
- Stacey, D.; Hawker, G.; Dervin, G.; Tugwell, P.; Boland, L.; Pomey, M.-P.; O’cOnnor, A.M.; Taljaard, M. Decision aid for patients considering total knee arthroplasty with preference report for surgeons: A pilot randomized controlled trial. BMC Musculoskelet. Disord. 2014, 15, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Zeelenberg, M.; Pieters, R. A theory of regret regulation 1.0. J. Consum. Psychol. 2007, 17, 3–18. [Google Scholar] [CrossRef]
- Bekker, H.L.; Winterbottom, A.E.; Butow, P.; Dillard, A.J.; Feldman-Stewart, D.; Fowler, F.J.; Jibaja-Weiss, M.L.; A Shaffer, V.; Volk, R.J. Do personal stories make patient decision aids more effective? A critical review of theory and evidence. BMC Med Inf. Decis Mak 2013, 13 (Suppl. S2), S9. [Google Scholar] [CrossRef]

{kind=link}
| Mean (SD) or n (%) | |
|---|---|
| Decision regret score | 18.22 (24.69) |
| Sociodemographic | |
| Gender | |
| Female | 87 (73.7%) |
| Male | 31 (26.3%) |
| Age | 72.31 (7.83) |
| BMI | 28.16 (4.82) |
| CCI | 0.64 (0.99) |
| Diabetes | |
| Yes | 23 (19.5%) |
| No | 95 (80.5%) |
| Smoking | |
| Yes | 6 (5.1%) |
| No | 112 (94.9%) |
| Level of education | |
| Primary school or below | 65 (55.0%) |
| High school | 37 (31.4%) |
| College or above | 16 (13.6%) |
| Side of TKR | |
| Right | 67 (56.8%) |
| Left | 51 (43.2%) |
| Previous history of contralateral TKR | |
| Yes | 22 (18.6%) |
| No | 96 (81.4%) |
| Preoperative Variables | |
| ASA grade | 2.15 (0.38) |
| Outpatient visits within 12 months prior to surgery | 3.58 (2.99) |
| Preoperative Lequesne Index | 12.25 (3.04) |
| Duration of symptoms present prior to surgery (year) | 4.64 (3.80) |
| Surgical Variables | |
| Operation time (min) | 134.58 (28.69) |
| Blood loss (mL) | 37.97 (61.72) |
| Post-operative Variables | |
| Mobility status | |
| Walks freely | 97 (82.2%) |
| Walker | 19 (16.1%) |
| Bedridden | 2 (1.7%) |
| ROM of knee joint (degree) | |
| >90 | 107 (90.7%) |
| <90 | 11 (9.3%) |
| Post-operative 3-month Lequesne Index | 5.02 (4.68) |
| Length of stay (day) | 6.05 (1.80) |
| No Regret | Mild Regret | Moderate-to-Severe Regret | Total | p-Value | |
|---|---|---|---|---|---|
| Sample size (%) | 58 (49.1) | 29 (24.6) | 31 (26.3) | 118 (100) | |
| Average (SD) of DRS | 0.00 (0.00) | 17.07 (8.08) | 53.39 (19.89) | 18.22 (24.69) | |
| Sociodemographic | |||||
| Gender | 0.469 | ||||
| Female (%) | 40 | 22 | 25 | 87 | |
| Male (%) | 18 | 7 | 6 | 31 | |
| Age (SD) | 73.05 (7.91) | 71.72 (8.10) | 71.48 (7.55) | 72.31 (7.83) | 0.602 |
| BMI (SD) | 28.14 (4.35) | 27.71 (3.80) | 28.63 (6.38) | 28.16 (4.82) | 0.763 |
| CCI (SD) | 0.64 (1.14) | 0.59 (0.83) | 0.68 (0.87) | 0.64 (0.99) | 0.939 |
| Diabetes | 0.105 | ||||
| Yes (%) | 8 | 5 | 10 | 23 | |
| No (%) | 50 | 24 | 21 | 95 | |
| Smoking | 0.726 | ||||
| Yes (%) | 2 | 2 | 2 | 6 | |
| No (%) | 56 | 27 | 29 | 112 | |
| Level of education | 0.427 | ||||
| Primary school or below (%) | 36 | 13 | 16 | 65 | |
| High school (%) | 15 | 10 | 12 | 37 | |
| College or above (%) | 7 | 6 | 3 | 16 | |
| Side of TKR | 0.957 | ||||
| Right (%) | 33 | 17 | 17 | 67 | |
| Left (%) | 25 | 12 | 14 | 51 | |
| Previous history of contralateral TKR | 0.118 | ||||
| Yes (%) | 14 | 6 | 2 | 22 | |
| No (%) | 44 | 23 | 29 | 96 | |
| Preoperative Variables | |||||
| ASA grade (SD) | 2.10 (0.36) | 2.28 (0.46) | 2.13 (0.34) | 2.15 (0.38) | 0.132 |
| Outpatient visits within 12 months prior to surgery (SD) | 3.76 (3.28) | 3.52 (2.54) | 3.32 (2.89) | 3.58 (2.99) | 0.802 |
| Preoperative Lequesne Index (SD) | 12.19 (3.26) | 12.41 (2.69) | 12.19 (3.02) | 12.25 (3.04) | 0.944 |
| Duration of symptoms present prior to surgery (year) (SD) | 4.35 (3.25) | 4.83 (4.45) | 5.01 (4.19) | 4.64 (3.80) | 0.704 |
| Surgical Variables | |||||
| Operation time (min) (SD) | 137.59 (30.85) | 130.76 (25.72) | 132.52 (27.33) | 134.58 (28.69) | 0.523 |
| Blood loss (mL) (SD) | 37.93 (6.26) | 38.28 (48.11) | 37.74 (73.02) | 37.97 (61.72) | 0.999 |
| Post-operative Variables | |||||
| Mobility status | 0.005 | ||||
| Independent mobility (Walks freely) (%) | 54 | 24 | 19 | 97 | |
| Limited mobility (walker) (%) | 3 | 5 | 11 | 19 | |
| Dependent mobility (bedridden) (%) | 1 | 0 | 1 | 2 | |
| ROM of knee joint | 0.311 | ||||
| >90 (%) | 55 | 25 | 27 | 107 | |
| <90 (%) | 3 | 4 | 4 | 11 | |
| Post-operative at 3 months Lequesne Index (SD) | 3.64 (3.35) | 4.59 (3.75) | 8.00 (6.17) | 5.02 (4.68) | 0.000 |
| Length of stay (SD) | 5.95 (1.67) | 6.48 (2.44) | 5.84 (1.21) | 6.05 (1.80) | 0.320 |
| Post-Operative Lequesne Index (SD) (CI Interval) | Total | p-Value (CI Interval) | Unstandardized Coefficient | |
|---|---|---|---|---|
| Average | 5.02 (4.68) | 118 | ||
| Sociodemographic | ||||
| Gender | 0.238 (−3.097~0.776) | |||
| Female | 5.32 (5.05) | 87 | ||
| Male | 4.16 (3.40) | 31 | ||
| Age | 72.31 | 0.668 | 0.024 | |
| BMI | 28.16 | 0.171 | 0.123 | |
| CCI | 0.64 | 0.068 | 0.795 | |
| Diabetes | 0.013 (−4.787~−0.571) | |||
| Yes | 7.17 (6.44) | 23 | ||
| No | 4.49 (4.02) | 95 | ||
| Smoking | 0.368 (−2.116~5.664) | |||
| Yes | 3.33 (2.66) | 6 | ||
| No | 5.11 (4.76) | 112 | ||
| Level of education | 0.413 | |||
| Primary school or below | 5.26 (4.97) (4.03~6.49) | 65 | ||
| High school | 5.22 (4.38) (3.76~6.68) | 37 | ||
| College or above | 3.56 (4.13) (1.36~5.76) | 16 | ||
| Side of TKR | 0.902 (−1.839~1.623) | |||
| Right | 4.97 (4.95) | 67 | ||
| Left | 5.08 (4.36) | 51 | ||
| Previous history of contralateral TKR | 0.985 (−2.181~2.223) | |||
| Yes | 5.00 (3.74) | 22 | ||
| No | 5.02 (4.89) | 96 | ||
| Preoperative Variables | ||||
| ASA grade | 2.15 | 0.289 | 1.199 | |
| Outpatient visits within 12 months prior to surgery | 3.58 | 0.224 | −0.177 | |
| Preoperative Lequesne Index | 12.25 | 0.005 | 0.394 | |
| Duration of symptoms present prior to surgery (year) | 4.64 | 0.767 | 0.034 | |
| Surgical Variables | ||||
| Operation time (min) | 134.58 | 0.519 | −0.01 | |
| Blood loss (mL) | 37.97 | 0.163 | −0.01 | |
| Post-operative Variables | ||||
| Mobility status | 0.000 | |||
| Independent mobility (walks freely) | 3.98 (3.56)(3.26~4.70) | 97 | ||
| Limited mobility (walker) | 9.58 (5.72)(6.82~12.34) | 19 | ||
| Dependent mobility (bedridden) | 12.00 (12.73)(−102~126) | 2 | ||
| ROM of knee joint | 0.002 (−7.32~−1.66) | |||
| >90 | 4.60 (4.37) | 107 | ||
| <90 | 9.09 (5.86) | 11 | ||
| Length of stay | 6.05 | 0.151 | 0.347 | |
| Independent Variables | n (%) | B | SE B | β | p-Value |
|---|---|---|---|---|---|
| Constant | 0.559 | 1.532 | 0.716 | ||
| Diabetes | 23(19.5) | 1.638 | 0.953 | 0.139 | 0.088 |
| No diabetes | 95(80.5) | Reference group | |||
| Preop. Lequesne Index | 0.247 | 0.124 | 0.160 | 0.050 | |
| Mobility status (bedridden) | 2(1.7) | 4.077 | 3.162 | 0.113 | 0.200 |
| Mobility status (walker) | 19(16.1) | 4.874 | 1.021 | 0.384 | 0.000 |
| Mobility status (walks freely) | 97(82.2) | Reference group | |||
| ROM of knee joint (<90 degree) | 11(9.3) | 2.846 | 1.403 | 0.177 | 0.045 |
| ROM of knee joint (>90 degree) | 107(90.7) | Reference group |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lo, Y.-C.; Chen, Y.-P.; Lin, H.E.; Chang, W.-C.; Ho, W.-P.; Jang, J.-P.; Kuo, Y.-J. Factors Associated with Decisional Regret After Shared Decision Making for Patients Undergoing Total Knee Arthroplasty. Healthcare 2025, 13, 1597. https://doi.org/10.3390/healthcare13131597
Lo Y-C, Chen Y-P, Lin HE, Chang W-C, Ho W-P, Jang J-P, Kuo Y-J. Factors Associated with Decisional Regret After Shared Decision Making for Patients Undergoing Total Knee Arthroplasty. Healthcare. 2025; 13(13):1597. https://doi.org/10.3390/healthcare13131597
Chicago/Turabian StyleLo, Yu-Chieh, Yu-Pin Chen, Hui En Lin, Wei-Chun Chang, Wei-Pin Ho, Jia-Pei Jang, and Yi-Jie Kuo. 2025. "Factors Associated with Decisional Regret After Shared Decision Making for Patients Undergoing Total Knee Arthroplasty" Healthcare 13, no. 13: 1597. https://doi.org/10.3390/healthcare13131597
APA StyleLo, Y.-C., Chen, Y.-P., Lin, H. E., Chang, W.-C., Ho, W.-P., Jang, J.-P., & Kuo, Y.-J. (2025). Factors Associated with Decisional Regret After Shared Decision Making for Patients Undergoing Total Knee Arthroplasty. Healthcare, 13(13), 1597. https://doi.org/10.3390/healthcare13131597