Abstract
Cotyledonoid dissecting leiomyoma (CDL), also known as Sternberg tumour, is a rare variant of leiomyoma that can be easily mistaken for a malignant neoplasm on clinical and radiological examination, posing a diagnostic challenge for clinicians. Background: Although the tumour can extend to neighbouring organs, it typically does not invade them and is considered benign. Therefore, it is essential to recognise and differentiate this leiomyoma variant from other malignancies to avoid misdiagnosis and overtreatment. Methods: This report depicts a unique case of CDL misdiagnosed as an ovarian tumour in a woman in her late 50s with post-menopausal bleeding and pelvic pressure. We initially planned and proceeded with a diagnostic laparoscopy and laparoscopic oophorectomy of the right ovarian mass, during which an intraoperative surprise of a retroperitoneal mass was explored and subsequently biopsied. Results: The final histopathology confirmed the presence of the rare fibroid variant CDL. The accompanying surgical video is among the first to feature a laparoscopic surgery of CDL and details the intraoperative findings and laparoscopic resection techniques utilised in this case. Conclusions: Given its rarity and non-specific clinical and radiological findings, diagnosing CDL pre-operatively can be challenging. This case prompts recognition and awareness of CDL and highlights the importance of careful consideration of uncommon differential diagnoses and thorough intraoperative exploration, with the goal of preventing the misdiagnosis and, consequently, overtreatment of unknown masses.
1. Introduction
Cotyledonoid dissecting leiomyoma (CDL) is an extremely rare variant of leiomyoma which can be locally invasive and extend to neighbouring organs such as the bladder, rectum, and fallopian tubes. It typically does not invade them and is considered a benign tumour with good prognosis [1,2,3]. However, CDL can easily be mistaken for a malignant neoplasm on clinical and radiological examination, posing a diagnostic challenge for clinicians [4]. Therefore, it is essential to recognise and differentiate this variant from other malignancies to avoid misdiagnosis and overtreatment, especially in women who wish to preserve their fertility. Herein, we report a rare case of CDL misdiagnosed pre-operatively as an ovarian tumour and explore the diagnostic challenges associated with CDL as well as the approach for its laparoscopic removal.
2. Case Presentation
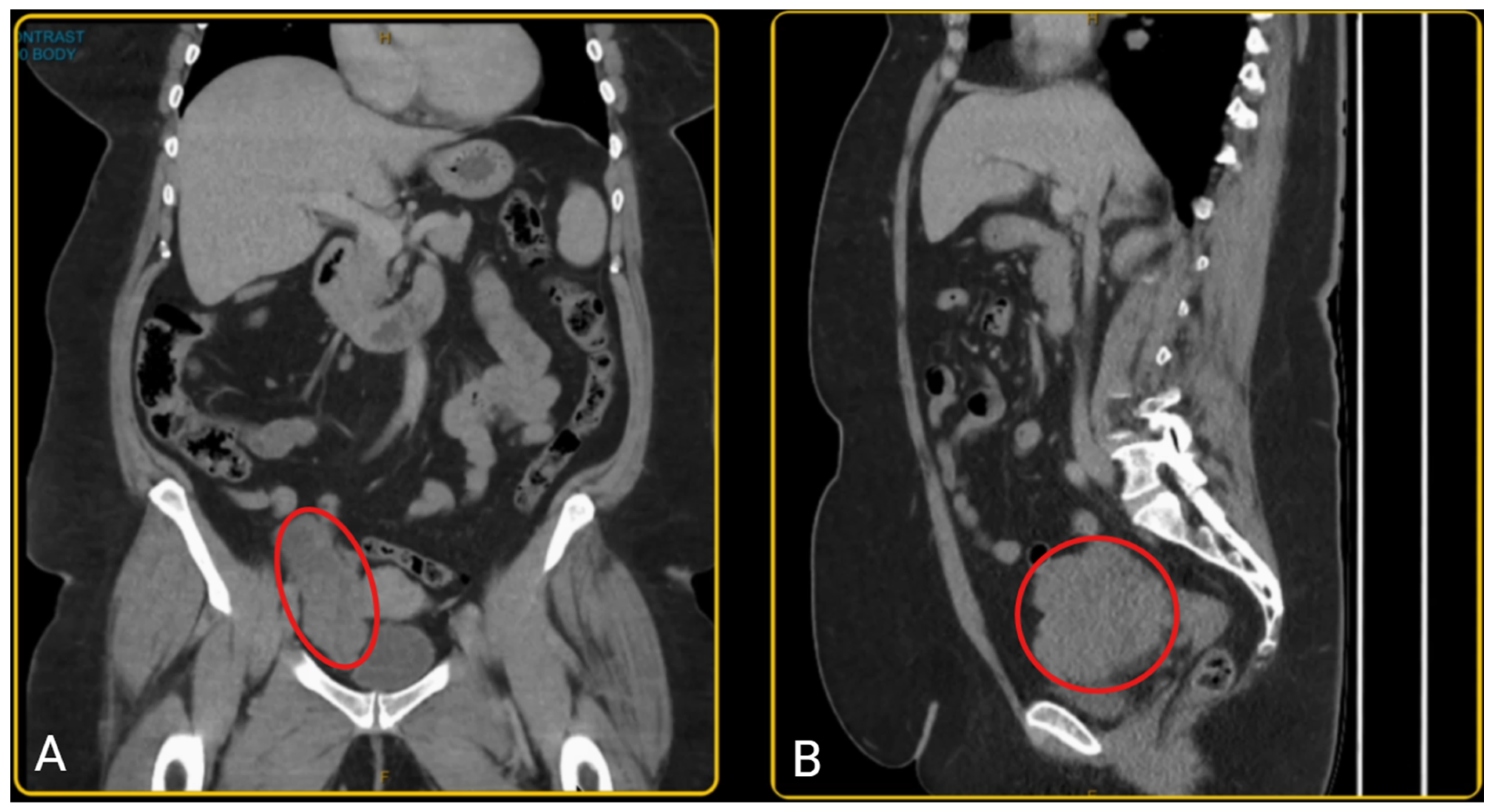
A woman in her late 50s presented with a history of post-menopausal bleeding and pelvic pressure. A pelvic ultrasound and CT scan showed a right adnexal mass measuring 103 × 98 × 50 mm (Figure 1). The mass had an irregular wall and a solid component. However, her tumour markers were normal (CA 125 = 13; Ca 19-9 = 22; CEA = 2.5; AFP = 7; RMI = 111). She was pre-emptively diagnosed with an ovarian tumour; however, since the diagnosis was not established, pre-operative biopsy was not performed due to the risk of tumour seeding and technical challenges. The patient was planned for hysteroscopy, endometrial sampling, laparoscopy +/− bilateral salpingo-oophorectomy after a detailed discussion of the diagnostic uncertainty and potential histopathological findings. Given her age, post-menopausal status, and clinical presentation, she understood the rationale for surgical intervention and provided informed consent for the proposed plan.
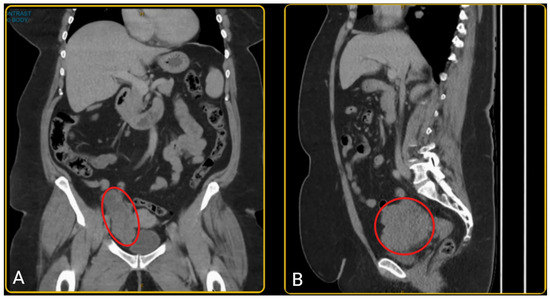
Figure 1.
(A) The coronal view of the pelvic CT scan; (B) the sagittal view of the pelvic CT scan showing a mass in the right lower quadrant of the abdomen, anteromedial to the iliac vessels and posterior to the bladder, consistent with a right adnexal mass (outlined in red). The mass measures 103 × 98 × 50 mm, with a well-demarcated, irregular border and has a heterogenous composition with varying internal density.
Endometrial cancer was ruled out with a hysteroscopy dilation and curettage and polypectomy immediately prior to the laparoscopy and oophorectomy, revealing an atrophic endometrium and a benign endometrial polyp.
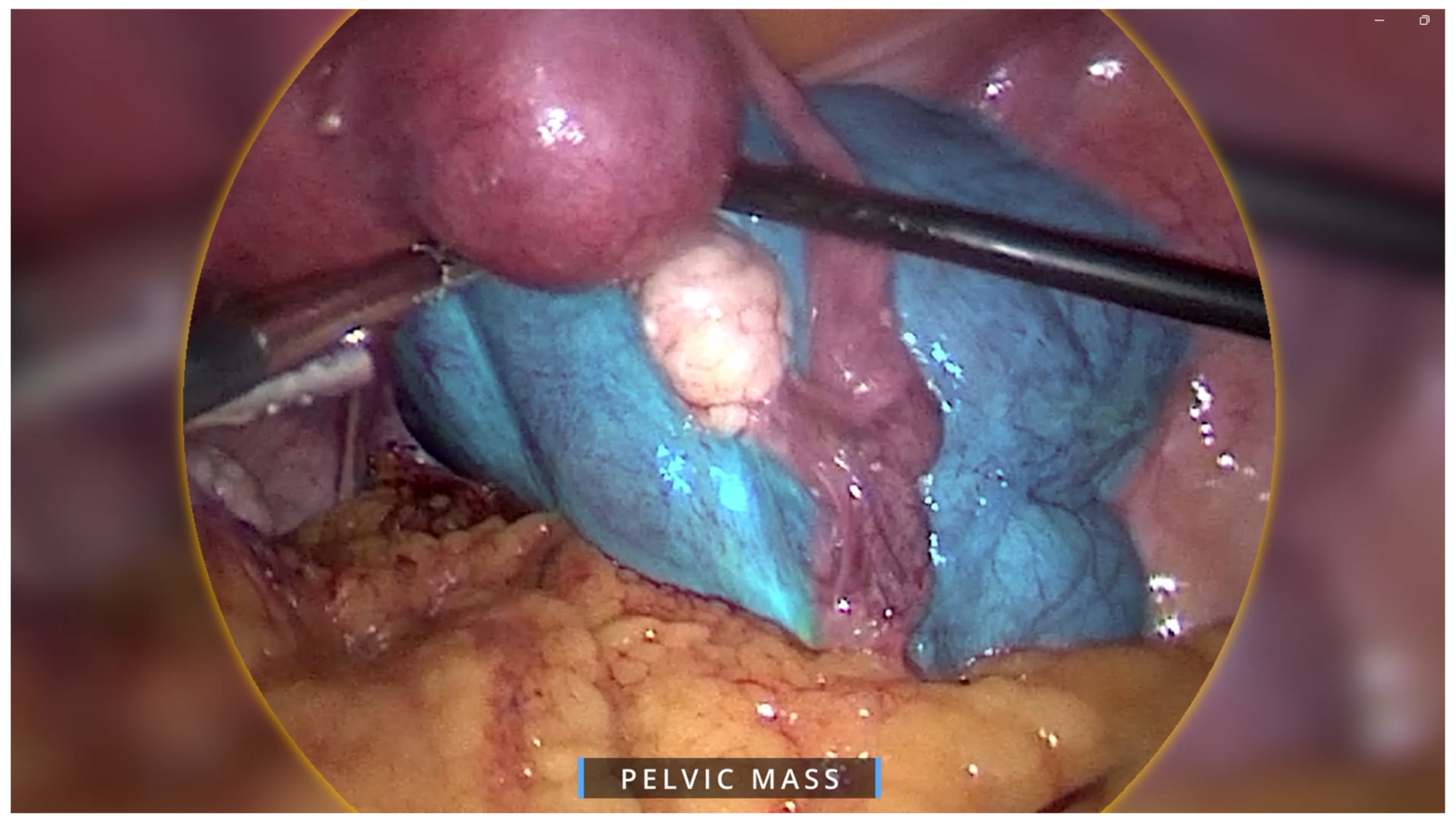
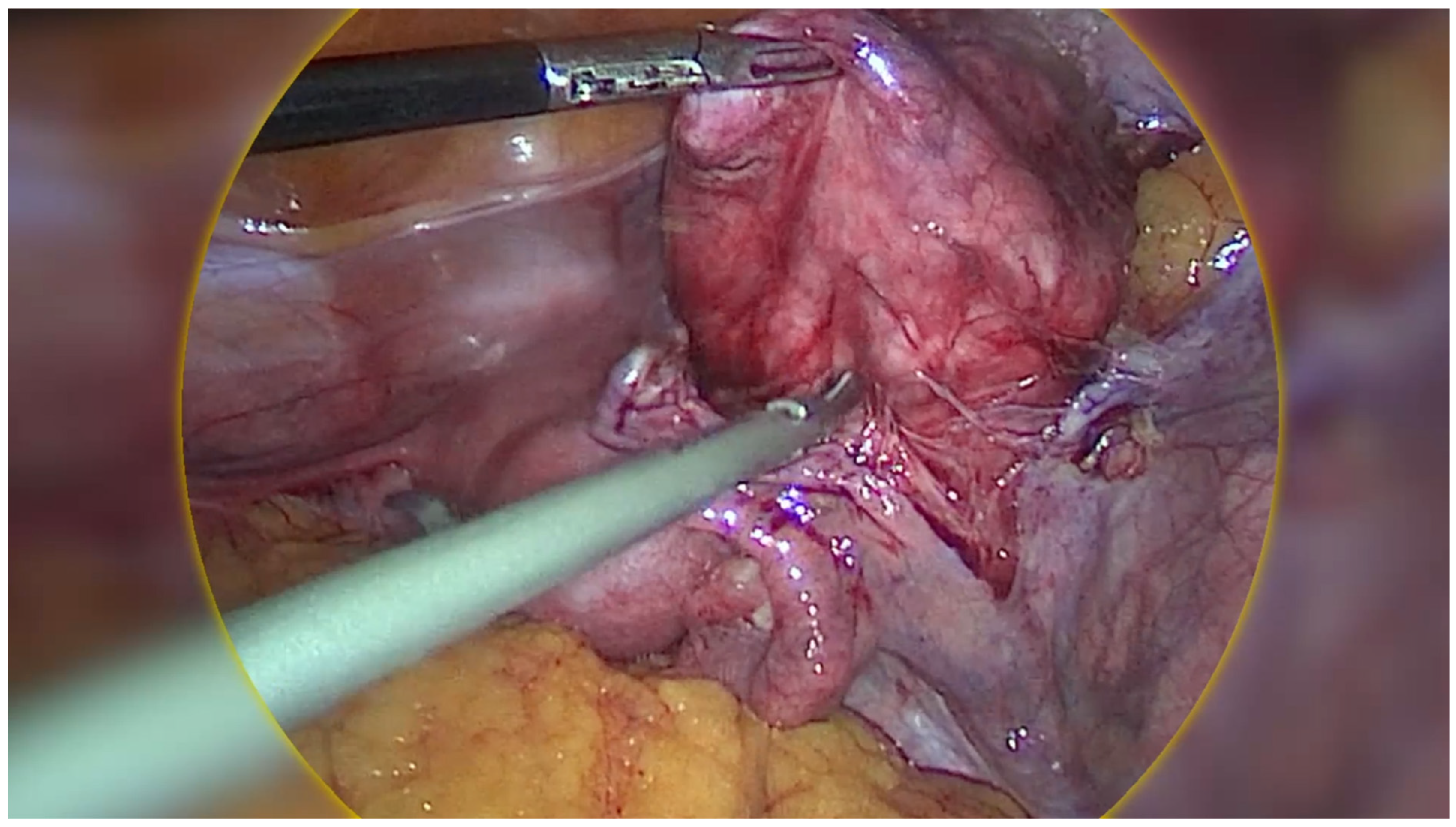
Regarding the ovarian tumour, the patient underwent a diagnostic laparoscopy using a 4-port laparoscopic technique with an ipsilateral configuration, during which we were met with an intraoperative surprise. A retroperitoneal pelvic mass of unknown origin was found and further explored. The mass measured around 8 × 8 cm and was found to be attached to the uterus laterally, anteriorly extending up to the paravesical space, laterally to the external iliac vessels, and posteriorly in the pararectal space (Figure 2). Initially, the mass was thought to be a fibroid; however, on palpation the consistency of the mass was different to that of a usual fibroid and was soft, almost jelly-like. The gross features also resembled cotyledons of the placenta (Figure 3). Due to the unique pattern of growth and inconclusive appearance of the retroperitoneal mass, we consulted with a gynaecology oncologist intraoperatively via telehealth and proceeded with their recommendation to perform an excisional biopsy.
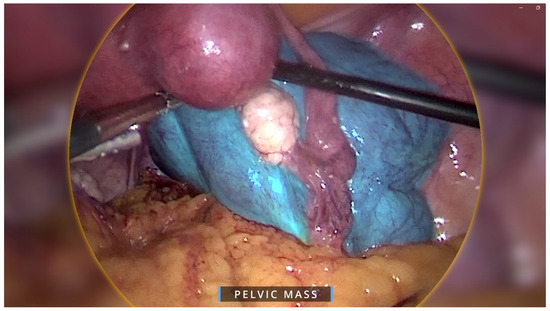
Figure 2.
Intraoperative image showing overall view of pelvic mass in blue overlay. The mass was attached to the uterus laterally, anteriorly extending up to the paravesical space, laterally to the external iliac vessels, and posteriorly in the pararectal space.
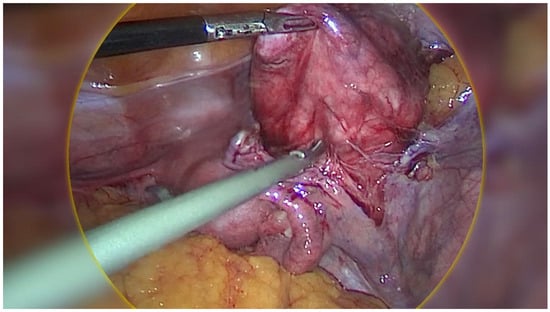
Figure 3.
Intraoperative image of cotyledonoid dissecting leiomyoma (CDL) which grossly resembles cotyledons of the placenta.
The mass’s jelly-like consistency and attachment to the iliac vessels laterally required us to develop a plane between the lymph nodes of the pelvic side wall and the tumour in order to prevent injury to the iliac vessels. Once the mass was carefully dissected and fully mobilised, it was placed in a laparoscopic bag and removed from the abdominal cavity. Surprisingly, the bag was able to be extracted through the 15 mm port site via the umbilicus without any extension due to the jelly-like nature of the mass.
The excised mass was sent for testing, which revealed a CDL, a rare variant of leiomyoma. Macroscopically, it appeared to have a smooth peritonealised surface with a solid, lobulated, white, fibrotic cut surface, with the lobules ranging from 2 to 22 mm in diameter. Areas of haemorrhage and increased vascularity were also noted. Histopathological examination of the mass demonstrated moderate vascularity and prominent oedematous areas separating the lobules of smooth muscle. Immunohistochemical analysis showed that the smooth muscle was desmin positive, S100 negative, ruling out endometrial stromal tumours as well as melanocytic and neural tissue lesions, respectively. There was no atypia of the smooth muscle cells, mitotic activity, or evidence of necrosis. No malignant cells were seen in the peritoneal washings sent for cytology.
The patient recovered well and was discharged the following day without complications. She was informed of the benign histopathology findings at her 6-week follow-up appointment and expressed relief and satisfaction with the outcome, as well as appreciation for the surgical restraint shown and preservation of her ovaries. During her follow-up in a year the patient was well with no evidence of clinical symptoms or disease progression.
3. Discussion
CDL, also known as Sternberg tumour, was first reported by Roth et al. It has been reported in women aged 23–73 years old, with most cases occurring in women aged 30–50, where common symptoms include lower abdominal pain and abnormal uterine bleeding [1,2]. The pathogenesis of CDL is not well understood, but it is believed to arise from a stem cell population in the myometrium [1]. Table 1 summarises CDL cases reported in the literature, including patient age, clinical presentation, tumour size, and management received.

Table 1.
Reported cases of cotyledonoid dissecting leiomyoma in the literature.
CDL is a rare histological variant of leiomyoma (benign uterine smooth muscle tumour) with less than 70 cases reported in the English literature [2]. Other well-recognised variants within the leiomyoma spectrum are summarised in Table 2 [35,36]. Importantly, CDL should not be confused with leiomyomas exhibiting disseminated, intravascular, or metastasizing growth, such as disseminated peritoneal leiomyomatosis (DPL), intravenous leiomyomas, or benign metastasizing leiomyomas, as it is a distinct entity which does not invade surrounding structures and lacks vascular and extrauterine invasion [35,36]. Another important differential to consider is smooth muscle tumours of uncertain malignant potential (STUMP) which are a clinically and pathologically heterogenous group of uterine smooth muscle tumours [37]. These tumours exceed the criteria for a leiomyoma and demonstrate malignant potential to develop into a low-grade leiomyosarcoma in a minority of cases yet satisfy insufficient criteria for leiomyosarcoma (marked nuclear atypia, high mitotic rate of >10 mitoses per 10 high-power fields, and tumour cell necrosis) [38]. More often, the rarity and non-specific, alarming features of CDL lead to its misdiagnosis for more sinister differentials including ovarian tumours, leiomyosarcomas, and endometrial stromal sarcoma, even though CDL is benign and carries a good prognosis [34]. This poses a diagnostic challenge for clinicians, especially in the pre-operative setting, and can lead to overtreatment. Therefore, recognition and awareness of CDL is essential to prevent such misdiagnosis and overtreatment.
Table 2.
Summary of histological leiomyoma variants.
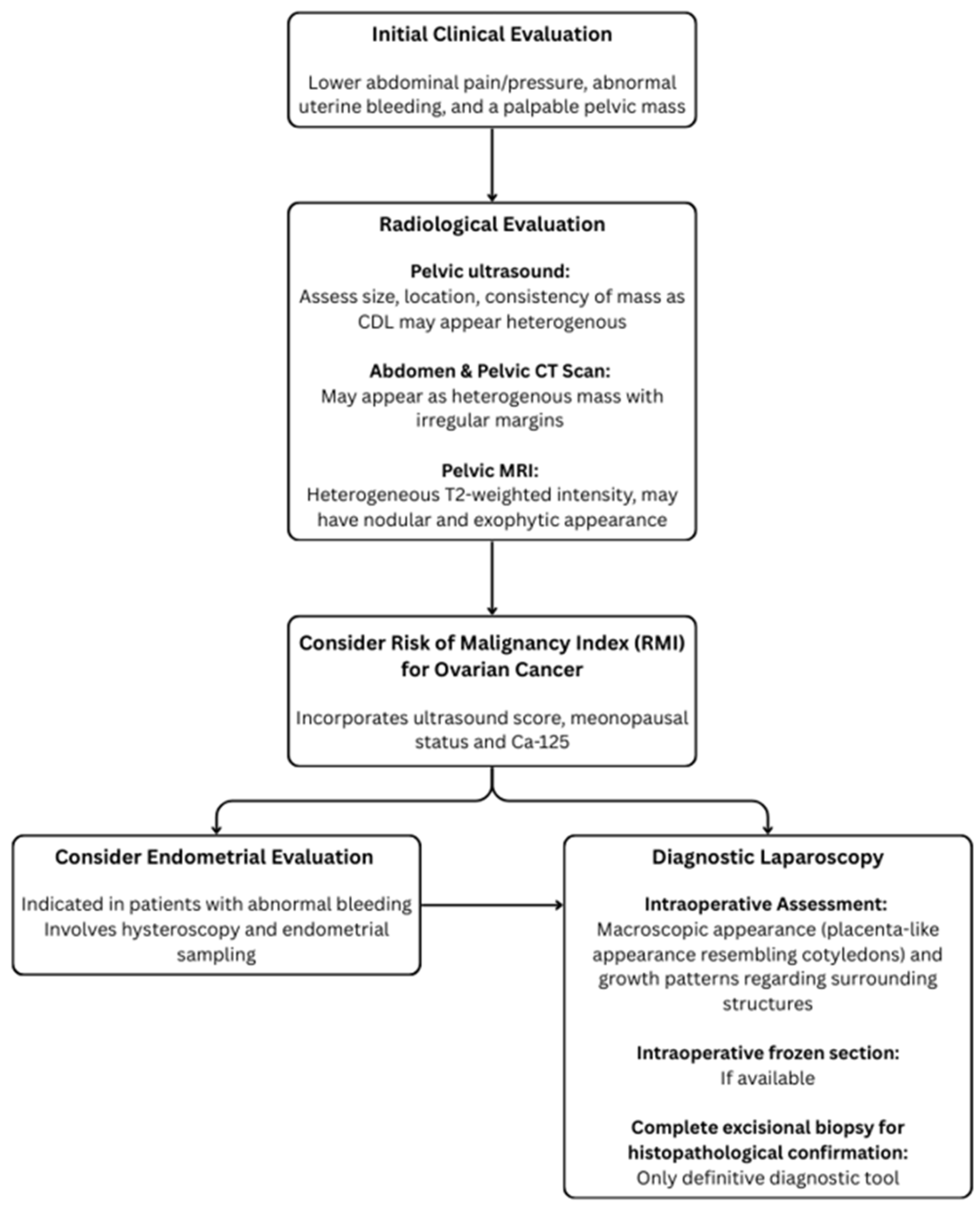
Pre-operative diagnostic techniques for CDL often yield an inconclusive or incorrect diagnosis. The diagnostic work-up for CDL is summarised in Figure 4 and begins with clinical evaluation and screening for signs and symptoms similar to those of typical leiomyomas, including lower abdominal pain/pressure, abnormal uterine bleeding, and a palpable pelvic mass. Radiological evaluation can include pelvic ultrasound and CT as well as MRI, where CDL often presents as heterogenous mass, raising concerns of malignancies such as leiomyosarcomas. However, to date, these imaging modalities cannot clearly differentiate malignant differentials from CDL [39]. An incisional core biopsy can be valuable for pre-operative diagnosis but is limited by sampling errors and insufficient information, where the biopsy may not capture the representative tissue, especially in heterogeneous tumours. Additionally, the risk of tumour seeding discourages the use of incisional core biopsies in situations where the diagnosis has not been confirmed [40]. In our case, since the pre-operative diagnosis was not established, an incisional core biopsy was not applicable.
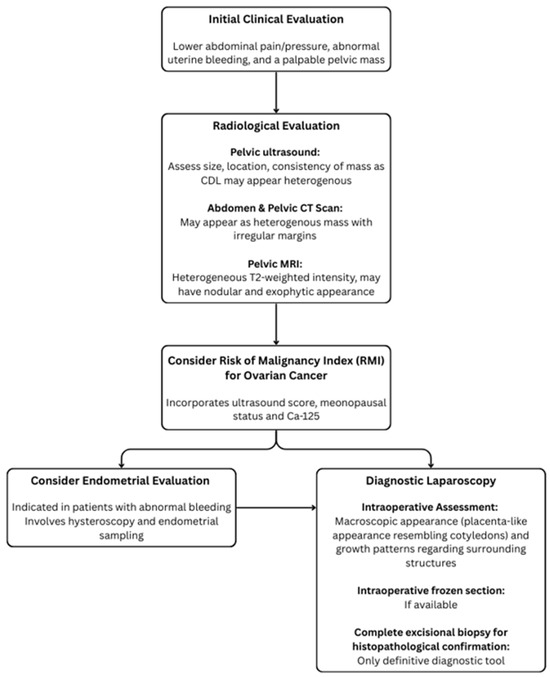
Figure 4.
Structured diagnostic pathway for suspected cotyledonoid dissecting leiomyoma (CDL).
CDL is often found incidentally in the intraoperative setting based on its unusual macroscopic appearance and pattern of growth. The size range has been reported from 25 mm to 410 mm in diameter, although most fall between 100 and 200 mm (average = 148.2 mm), with our case representing a smaller CDL mass. This could be attributed to the effect of hormone depletion in menopause, leading to smaller-sized lesions with advancing age, as described by Buonomo et al. [41]. Macroscopically, CDL typically appears as a soft, jelly-like, multinodular, grape-like mass that is red-brown in colour, and has a placenta-like appearance resembling cotyledons. Despite being able to dissect its way through adjacent organs such as the bladder, rectum, and fallopian tubes, CDL does not invade these surroundings structures [4,13,42]. Thus, despite its atypical gross appearance and pattern of growth which can raise suspicions of sarcomas, CDL does not metastasise and carries a good prognosis. This demonstrates how careful intraoperative exploration and recognition of CDL based on its unique features can prompt consideration of alternative diagnoses rather than malignancies, hence guiding intraoperative decision-making to avoid overtreatment.
When in doubt, intraoperative frozen sections may be considered as they can provide immediate information to guide surgical decisions on whether a more conservative approach is sufficient or if more extensive surgery is required but may have limitations in accuracy due to the presence of artefacts and can prolong surgery [43]. In this case, the facility where the surgery was performed did not have intraoperative frozen section capabilities. Instead, we consulted with a gynaecologic oncologist, and decided to proceed with an excisional biopsy instead of the initial intended oophorectomy, thus sparing the patient from unnecessary overtreatment.
Ultimately, histopathological examination remains the only diagnostic tool for a definitive diagnosis of CDL, whereby it is uniquely characterised by the presence of irregular nodular dissections of smooth muscle cells within the myometrium [13].
The treatment options for CDL depend on several factors, including the patient’s age, symptoms, and desire for future fertility. In many cases, observation may be appropriate, especially in post-menopausal women who are asymptomatic. For symptomatic women, surgical resection may be recommended [34]. Although surgical management of CDL in the literature has mostly involved total abdominal hysterectomy +/− bilateral salpingo-oophorectomy, good outcomes have been reported for more conservative approaches including total tumour excisional biopsy/resection and myomectomy, thus they may be preferred, especially in patients desiring fertility-sparing techniques [41].
Overall, CDL carries a good prognosis with most patients remaining disease-free on long-term follow up, and no confirmed cases of recurrence, malignant transformation, or metastasis have been reported [41].
4. Conclusions
CDL is a rare, benign variant of leiomyoma with a good prognosis. However, it can be easily misdiagnosed as ovarian tumours, posing a diagnostic challenge for clinicians. This case and the accompanying surgical video is among the first to feature a laparoscopic surgery of CDL and highlights the importance of thorough intraoperative exploration and careful consideration of uncommon differential diagnoses for ovarian tumours. Recognition and awareness of CDL by clinicians and pathologists can prevent misdiagnosis for a more sinister malignant condition, and consequently overtreatment, especially in fertility-seeking women. Further research may be required to gain a more comprehensive understanding of this pathological variant and develop more robust pre- and intraoperative diagnostic techniques.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/healthcare13121367/s1, Surgical video depicting the case presentation and laparoscopic discovery and excision of the rare cotyledonoid dissecting leiomyoma (CDL), initially misdiagnosed as an ovarian tumour.
Author Contributions
K.N.: Drafting manuscript, narrating and editing of surgical video, critical review and editing of manuscript. T.R.: Supervision, conceptualisation, lead clinician responsible for patient care including diagnosis and surgical treatment, recording of surgical video, and critical review of manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review and approval were waived for this study due to its nature as a single-patient case report with no identifiable personal information disclosed. The case was conducted in accordance with the ethical standards of the SWSLHD Human Research Ethics Committee (HREC) and with the 1964 Helsinki Declaration and its later amendments.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The original contributions presented in this study are included in the article/Supplementary Materials. Further inquiries can be directed to the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest. The article complies with institutional ethics guidelines.
References
- Roth, L.M.; Reed, R.J.; Sternberg, W.H. Cotyledonoid dissecting leiomyoma of the uterus. The Sternberg tumor. Am. J. Surg. Pathol. 1996, 20, 1455–1461. [Google Scholar] [CrossRef] [PubMed]
- Xu, T.; Wu, S.; Yang, R.; Zhao, L.; Sui, M.; Cui, M.; Chang, W. Cotyledonoid dissecting leiomyoma of the uterus: A report of four cases and a review of the literature. Oncol. Lett. 2016, 11, 2865–2868. [Google Scholar] [CrossRef]
- Jamal, I.; Gupta, R.K.; Sinha, R.K.; Bhadani, P.P. Cotyledonoid dissecting leiomyoma: An uncommon form of a common disease. Obstet. Gynecol. Sci. 2019, 62, 362–366. [Google Scholar] [CrossRef] [PubMed]
- Abreu, R.F.; Bovolim, G.; Baiocchi, G.; De Brot, L. Cotyledonoid dissecting leiomyoma of the uterus: A gross and radiologic malignancy mimicker. Int. J. Gynecol. Cancer 2023, 33, 1827–1829. [Google Scholar] [CrossRef]
- David, M.P.; Homonnai, T.Z.; Deligdish, L.; Loewenthal, M. Grape-like leiomyomas of the uterus. Int. Surg. 1975, 60, 238–239. [Google Scholar]
- Brand, A.H.; Scurry, J.P.; Planner, R.S.; Grant, P.T. Grape-like leiomyoma of the uterus. Am. J. Obstet. Gynecol. 1995, 173, 959–961. [Google Scholar] [CrossRef]
- Roth, L.M.; Reed, R.J. Dissecting leiomyomas of the uterus other than cotyledonoid dissecting leiomyomas: A report of eight cases. Am. J. Surg. Pathol. 1999, 23, 1032–1039. [Google Scholar] [CrossRef]
- Kim, M.J.; Park, Y.K.; Cho, J.H. Cotyledonoid dissecting leiomyoma of the uterus: A case report and review of the literature. J. Korean Med. Sci. 2002, 17, 840–844. [Google Scholar] [CrossRef]
- Cheuk, W.; Chan, J.K.; Liu, J.Y. Cotyledonoid leiomyoma: A benign uterine tumor with alarming gross appearance. Arch. Pathol. Lab. Med. 2002, 126, 210–213. [Google Scholar] [CrossRef]
- Stewart, K.A.; Ireland-Jenkin, K.; Quinn, M.; Armes, J.E. Cotyledonoid dissecting leiomyoma. Pathology 2003, 35, 177–179. [Google Scholar]
- Gurbuz, A.; Karateke, A.; Kabaca, C.; Arik, H.; Bilgic, R. A case of cotyledonoid leiomyoma and review of the literature. Int. J. Gynecol. Cancer 2005, 15, 1218–1221. [Google Scholar] [CrossRef] [PubMed]
- Jordan, L.B.; Al-Nafussi, A.; Beattie, G. Cotyledonoid hydropic intravenous leiomyomatosis: A new variant leiomyoma. Histopathology 2002, 40, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Saeed, A.S.; Hanaa, B.; Faisal, A.S.; Najla, A.M. Cotyledonoid dissecting leiomyoma of the uterus: A case report of a benign uterine tumor with sarcoma-like gross appearance and review of literature. Int. J. Gynecol. Pathol. 2006, 25, 262–267. [Google Scholar] [CrossRef]
- Maimoon, S.; Wilkinson, A.; Mahore, S.; Bothale, K.; Patrikar, A. Cotyledonoid leiomyoma of the uterus. Indian. J. Pathol. Microbiol. 2006, 49, 289–291. [Google Scholar]
- Shelekhova, K.V.; Kazakov, D.V.; Michal, M. Cotyledonoid dissecting leiomyoma of the uterus with intravascular growth: Report of two cases. Virchows Arch. 2007, 450, 119–121. [Google Scholar] [CrossRef]
- Weissferdt, A.; Maheshwari, M.B.; Downey, G.P.; Rollason, T.P.; Ganesan, R. Cotyledonoid dissecting leiomyoma of the uterus: A case report. Diagn. Pathol. 2007, 2, 18. [Google Scholar] [CrossRef]
- Adedipe, T.O.; Vine, S.J. Dissecting Cotyledonoid Leiomyoma: A Rare Cause of Chronic Intractable Menorrhagia (Not Amenable to Medical Treatment). Case Report. Eur. J. Gynaecol. Oncol. 2010, 31, 230–232. [Google Scholar]
- Raga, F.; Sanz-Cortés, M.; Casañ, E.M.; Burgues, O.; Bonilla-Musoles, F. Cotyledonoid dissecting leiomyoma of the uterus. Fertil. Steril. 2009, 91, 1269–1270. [Google Scholar] [CrossRef]
- Preda, L.; Rizzo, S.; Gorone, M.S.; Fasani, R.; Maggioni, A.; Bellomi, M. MRI features of cotyledonoid dissecting leiomyoma of the uterus. Tumori 2009, 95, 532–534. [Google Scholar] [CrossRef]
- Fukunaga, M.; Suzuki, K.; Hiruta, N. Cotyledonoid dissecting leiomyoma of the uterus: A report of four cases. APMIS 2010, 118, 331–333. [Google Scholar] [CrossRef]
- Gezginç, K.; Yazici, F.; Selimoğlu, R.; Tavli, L. Cotyledonoid dissecting leiomyoma of the uterus with intravascular growth in postmenopausal woman: A case presentation. Int. J. Clin. Oncol. 2011, 16, 701–704. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, R.; Radhika, A.G.; Malik, R.; Radhakrishnan, G. Cotyledonoid leiomyoma and non-descent vaginal hysterectomy. Arch. Gynecol. Obstet. 2010, 281, 971–972. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, H.; Toriyabe, K.; Senda, T.; Sakakura, Y.; Yoshida, K.; Asakura, T.; Taniguchi, H.; Nagao, K. Cotyledonoid dissecting leiomyoma treated by laparoscopic surgery: A case report. Asian J. Endosc. Surg. 2013, 6, 122–125. [Google Scholar] [CrossRef] [PubMed]
- Onu, D.O.; Fiorentino, L.M.; Bunting, M.W. Cotyledonoid Dissecting Leiomyoma as a Possible Cause of Chronic Lower Back Pain. BMJ Case Rep. 2013, 2013, bcr2013201350. [Google Scholar] [CrossRef]
- Blake, E.A.; Cheng, G.; Post, M.D.; Guntupalli, S. Cotyledonoid dissecting leiomyoma with adipocytic differentiation: A case report. Gynecol. Oncol. Rep. 2015, 11, 7–9. [Google Scholar] [CrossRef]
- Shimizu, A.; Tanaka, H.; Iwasaki, S.; Wakui, Y.; Ikeda, H.; Suzuki, A. An unusual case of uterine cotyledonoid dissecting leiomyoma with adenomyosis. Diagn. Pathol. 2016, 11, 69. [Google Scholar] [CrossRef]
- Lenz, J.; Chvátal, R.; Konečná, P. Dissecting leiomyoma of the uterus with unusual clinical and pathological features. Ceska Gynekol. 2020, 85, 197–200. [Google Scholar]
- Rocha, A.C.; Oliveira, M.; Luís, P.; Nogueira, M. Cotyledonoid dissecting leiomyoma of the uterus: An unexpected diagnosis after delivery. Acta Med. Port. 2018, 31, 223–227. [Google Scholar] [CrossRef]
- Parker, W.H.; Turner, R.; Schwimer, S.; Foshag, L. Massive Cotyledenoid Leiomyoma Treated with Uterine-Conserving Surgery. FS Rep. 2020, 1, 314–316. [Google Scholar] [CrossRef]
- Kawashita, S.; Nonoshita, A.; Iwasaki, K.; Nakayama, D. Cotyledonoid dissecting leiomyoma: A rare benign uterine tumor mimicking malignancy. Clin Pathol. 2024, 17, 2632010X241281240. [Google Scholar] [CrossRef]
- Yadav, A.; Raychaudhuri, S.; Kaur, L.; Bhardwaj, M. Cotyledonoid dissecting leiomyoma: A rare case report. Caspian J. Reprod. Med. 2024, 10, 1–4. [Google Scholar]
- Xue Dong, R. Cotyledonoid dissecting leiomyoma mimicking ovarian malignancy: A case report and literature review. J. Minim Invasive Gynecol. 2024, 31, 817–818. [Google Scholar]
- Robichaud, S.; Wong, J.; Ouallouche, K.; Bleau, N.; Rahimi, K. Dissecting “Cotyledonoid” Leiomyoma Involved by Adenomyosis. Int. J. Surg. Pathol. 2025. [Google Scholar] [CrossRef] [PubMed]
- Chahkandi, M.; Ataei, M.; Bina, A.R.; Mozayani, F.; Fanoodi, A. Cotyledonoid dissecting leiomyoma of the uterus: A case report and review of the literature. J. Med. Case Rep. 2023, 17, 516. [Google Scholar] [CrossRef]
- WHO. Classification of Female Genital Tumours, 5th ed.; International Agency for Research on Cancer: Lyon, France, 2020. [Google Scholar]
- Arleo, E.K.; Schwartz, P.E.; Hui, P.; McCarthy, S. Review of leiomyoma variants. Am. J. Roentgenol. 2015, 205, 912–921. [Google Scholar] [CrossRef]
- Tinelli, A.; D’Oria, O.; Civino, E.; Morciano, A.; Hashmi, A.A.; Baldini, G.M.; Stefanovic, R.; Malvasi, A.; Pecorella, G. Smooth muscle tumor of uncertain malignant potential (STUMP): A comprehensive multidisciplinary update. Medicina 2023, 59, 1371. [Google Scholar] [CrossRef]
- National Organization for Rare Disorders (NORD). Leiomyosarcoma—Symptoms, Causes, Treatment. RareDiseases.org. 2023. Available online: https://rarediseases.org/rare-diseases/leiomyosarcoma/ (accessed on 10 November 2024).
- Asghari, K.M.; Tabrizi, A.D.; Madani, P.S. Unraveling the mystery of uterine cotyledonoid dissecting leiomyoma: A case report. Eur. J. Gynaecol. Oncol. 2024, 45, 167. [Google Scholar]
- Yarram, S.G.; Nghiem, H.V.; Higgins, E.; Fox, G.; Nan, B.; Francis, I.R. Evaluation of imaging-guided core biopsy of pelvic masses. Am. J. Roentgenol. 2007, 188, 1208–1211. [Google Scholar] [CrossRef]
- Buonomo, F.; Bussolaro, S.; Fiorillo, C.d.A.; Giorda, G.; Romano, F.; Biffi, S.; Ricci, G. The management of the cotyledonoid leiomyoma of the uterus: A narrative review of the literature. Int. J. Environ. Res. Public Health 2021, 18, 8521. [Google Scholar] [CrossRef]
- Fernandez, K.; Cheung, L.; Taddesse-Heath, L. Cotyledonoid dissecting leiomyoma: A rare variant of leiomyoma of the uterus. Cureus 2022, 14, e30352. [Google Scholar] [CrossRef]
- Karki, D.; Shrestha, G.; Joshi, S.L. A case of cotyledonoid dissecting leiomyoma with associated disseminated peritoneal leiomyomatosis: The significance of frozen section in identification of this unusual entity. Cureus 2024, 16, e55781. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).