
Physiological Variability during Prehospital Stroke Care: Which Monitoring and Interventions Are Used?

 , , ,
, , , {kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Identification
2.2. Search Strategy
2.3. Inclusion and Exclusion Criteria
2.4. Data Extraction
2.5. Risk of Bias Assessment
2.6. Data Synthesis
3. Results
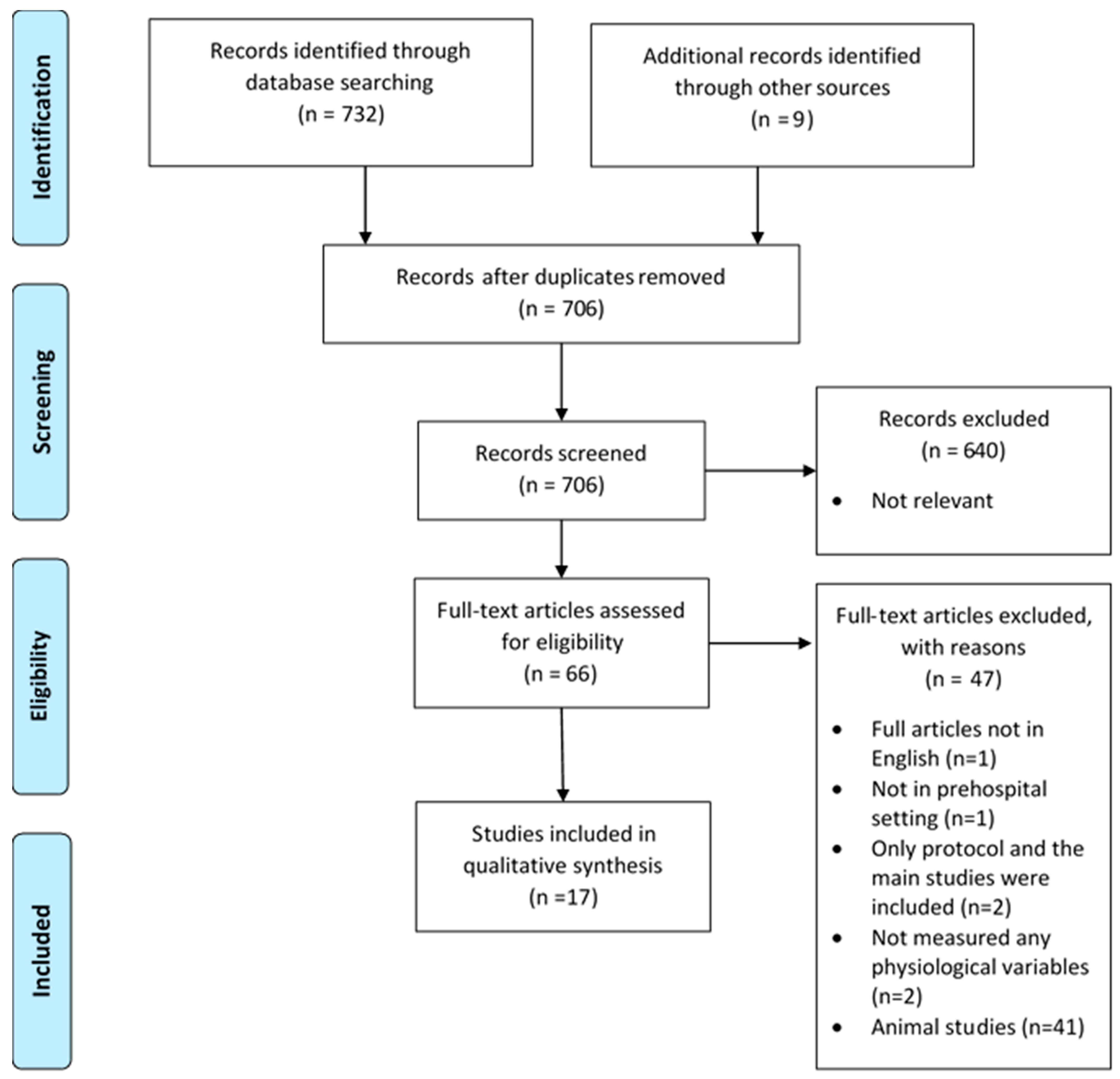
3.1. Study Selection
3.2. Main Findings
3.2.1. Physiological Monitoring Intervention
- Blood pressure and patient outcomes
- Other uses of blood pressure measurements
- Other physiological parameters
3.2.2. Pharmacological Therapy Intervention
4. Discussion
- Physiological monitoring interventions:
- Pharmacological interventions:
4.1. Strengths and Limitations
4.2. Future Work
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Geisler, F.; Wesirow, M.; Ebinger, M.; Kunz, A.; Rozanski, M.; Waldschmidt, C.; Weber, J.E.; Wendt, M.; Winter, B.; Audebert, H.J. Probability assessment of intracerebral hemorrhage in prehospital emergency patients. Neurol. Res. Pract. 2021, 3, 1. [Google Scholar] [CrossRef] [PubMed]
- Duvekot, M.H.C.; Venema, E.; Rozeman, A.D.; Moudrous, W.; Vermeij, F.H.; Biekart, M.; Lingsma, H.F.; Maasland, L.; Wijnhoud, A.D.; Mulder, L.J.M.M.; et al. Comparison of eight prehospital stroke scales to detect intracranial large-vessel occlusion in suspected stroke (PRESTO): A prospective observational study. Lancet Neurol. 2021, 20, 213–221. [Google Scholar] [CrossRef] [PubMed]
- Maxim, M.; Sameer, A.A.; Ryan, A.M.; Ketan, R.B.; Mayank, G.; Michael, C.; Justin, F.F. Indications for thrombectomy in acute ischemic stroke from emergent large vessel occlusion (ELVO): Report of the SNIS Standards and Guidelines Committee. J. NeuroInterv. Surg. 2019, 11, 215. [Google Scholar] [CrossRef]
- Yoshida, Y.; Hayashi, Y.; Shimada, T.; Hattori, N.; Tomita, K.; Miura, R.E.; Yamao, Y.; Tateishi, S.; Iwadate, Y.; Nakada, T.-a. Prehospital stroke-scale machine-learning model predicts the need for surgical intervention. Sci. Rep. 2023, 13, 9135. [Google Scholar] [CrossRef]
- Feigin, V.L.; Stark, B.A.; Johnson, C.O.; Roth, G.A.; Bisignano, C.; Abady, G.G.; Abbasifard, M.; Abbasi-Kangevari, M.; Abd-Allah, F.; Abedi, V.; et al. Global, regional, and national burden of stroke and its risk factors, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021, 20, 795–820. [Google Scholar] [CrossRef] [PubMed]
- Wafa, H.A.; Wolfe, C.D.A.; Emmett, E.; Roth, G.A.; Johnson, C.O.; Wang, Y. Burden of Stroke in Europe: Thirty-Year Projections of Incidence, Prevalence, Deaths, and Disability-Adjusted Life Years. Stroke 2020, 51, 2418–2427. [Google Scholar] [CrossRef] [PubMed]
- Lindsberg, P.J.; Roine, R.O. Hyperglycemia in Acute Stroke. Stroke 2004, 35, 363–364. [Google Scholar] [CrossRef]
- Rowat, A.M.; Dennis, M.S.; Wardlaw, J.M. Hypoxaemia in Acute Stroke Is Frequent and Worsens Outcome. Cerebrovasc. Dis. 2006, 21, 166–172. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Kang, D.W. Induced hypertensive therapy in an acute ischemic stroke patient with early neurological deterioration. J. Clin. Neurol. 2007, 3, 187–191. [Google Scholar] [CrossRef][Green Version]
- Ishitsuka, K.; Kamouchi, M.; Hata, J.; Fukuda, K.; Matsuo, R.; Kuroda, J.; Ago, T.; Kuwashiro, T.; Sugimori, H.; Nakane, H.; et al. High Blood Pressure After Acute Ischemic Stroke Is Associated With Poor Clinical Outcomes. Hypertension 2014, 63, 54–60. [Google Scholar] [CrossRef]
- Salinet, A.S.M.; Minhas, J.S.; Panerai, R.B.; Bor-Seng-Shu, E.; Robinson, T.G. Do acute stroke patients develop hypocapnia? A systematic review and meta-analysis. J. Neurol. Sci. 2019, 402, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Price, C.I.; Shaw, L.; Islam, S.; Javanbakht, M.; Watkins, A.; McMeekin, P.; Snooks, H.; Flynn, D.; Francis, R.; Lakey, R.; et al. Effect of an Enhanced Paramedic Acute Stroke Treatment Assessment on Thrombolysis Delivery During Emergency Stroke Care: A Cluster Randomized Clinical Trial. JAMA Neurol. 2020, 77, 840–848. [Google Scholar] [CrossRef] [PubMed]
- Bath, P.M.; Scutt, P.; Anderson, C.S.; Appleton, J.P.; Berge, E.; Cala, L.; Dixon, M.; England, T.M.; Godolphin, P.J.; Havard, D.; et al. Prehospital transdermal glyceryl trinitrate in patients with ultra-acute presumed stroke (RIGHT-2): An ambulance-based, randomised, sham-controlled, blinded, phase 3 trial. Lancet 2019, 393, 1009–1020. [Google Scholar] [CrossRef] [PubMed]
- Sammut-Powell, C.; Ashton, C.; Paroutoglou, K.; Parry-Jones, A. Differences in Characteristics and Ambulance Pathway Adherence Between Strokes and Mimics Presenting to a Large UK Centralized Hyper Acute Stroke Unit (HASU). Front. Neurol. 2021, 12, 646015. [Google Scholar] [CrossRef] [PubMed]
- Leenen, J.P.L.; Leerentveld, C.; van Dijk, J.D.; van Westreenen, H.L.; Schoonhoven, L.; Patijn, G.A. Current Evidence for Continuous Vital Signs Monitoring by Wearable Wireless Devices in Hospitalized Adults: Systematic Review. J. Med. Internet Res. 2020, 22, e18636. [Google Scholar] [CrossRef] [PubMed]
- Sen, A.; Miller, J.; Wilkie, H.; Moyer, M.; Lewandowski, C.; Nowak, R. Continuous hemodynamic monitoring in acute stroke: An exploratory analysis. West. J. Emerg. Med. 2014, 15, 345–350. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Wong, A.A.; Read, S.J. Early changes in physiological variables after stroke. Ann. Indian. Acad. Neurol. 2008, 11, 207–220. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Lin, X.; Cai, Y.; Huang, R.; Yang, S.; Zhang, G. A Systematic Review of Mobile Stroke Unit Among Acute Stroke Patients: Time Metrics, Adverse Events, Functional Result and Cost-Effectiveness. Front. Neurol. 2022, 13, 803162. [Google Scholar] [CrossRef] [PubMed]
- Mathur, S.; Walter, S.; Grunwald, I.Q.; Helwig, S.A.; Lesmeister, M.; Fassbender, K. Improving Prehospital Stroke Services in Rural and Underserved Settings with Mobile Stroke Units. Front. Neurol. 2019, 10, 159. [Google Scholar] [CrossRef]
- Grunwald, I.Q.; Phillips, D.J.; Sexby, D.; Wagner, V.; Lesmeister, M.; Bachhuber, M.; Mathur, S.; Guyler, P.; Fisher, J.; Perera, S.; et al. Mobile Stroke Unit in the UK Healthcare System: Avoidance of Unnecessary Accident and Emergency Admissions. Cerebrovasc. Dis. 2020, 49, 388–395. [Google Scholar] [CrossRef]
- Walter, S.; Audebert, H.J.; Katsanos, A.H.; Larsen, K.; Sacco, S.; Steiner, T.; Turc, G.; Tsivgoulis, G. European Stroke Organisation (ESO) guidelines on mobile stroke units for prehospital stroke management. Eur. Stroke J. 2022, 7, XXVII–LIX. [Google Scholar] [CrossRef] [PubMed]
- Royal College of Physicians. Sentinal Stroke National Audit Programme (SSNAP). 2017. Available online: https://www.strokeaudit.org/Documents/National/Clinical/AprJul2017/AprJul2017-PublicReport.aspx (accessed on 1 April 2023).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The, P.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLOS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan-a web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle–Ottawa Scale (NOS) for Assessing the Quality of Non-Randomized Studies in Meta-Analysis. 2000. Available online: https://www3.med.unipmn.it/dispense_ebm/2009-2010/Corso%20Perfezionamento%20EBM_Faggiano/NOS_oxford.pdf (accessed on 1 April 2023).
- Fan, J.-S.; Chen, Y.-C.; Huang, H.-H.; How, C.-K.; Yen, D.H.-T.; Huang, M.-S. The association between on-scene blood pressure and early neurological deterioration in patients with spontaneous intracerebral haemorrhage. Emerg. Med. J. 2015, 32, 239. [Google Scholar] [CrossRef] [PubMed]
- Tsou, Y.J.; Lan, K.P.; Fan, J.S. Relationship Between Changes in Prehospital Blood Pressure and Early Neurological Deterioration in Spontaneous Intracerebral Hemorrhage. Adv. Emerg. Nurs. J. 2019, 41, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Larsen, K.T.; Selseth, M.N.; Jahr, S.H.; Hillestad, V.; Koubaa, N.; Sandset, E.C.; Ronning, O.M.; Kristoffersen, E.S. Prehospital Blood Pressure and Clinical and Radiological Outcomes in Acute Spontaneous Intracerebral Hemorrhage. Stroke 2022, 53, 3633–3641. [Google Scholar] [CrossRef] [PubMed]
- Atsumi, H.; Sorimachi, T.; Sakakibara, Y.; Nonaka, Y.; Matsumae, M. Prehospital information and spot sign are complementary predictors of post-admission outcomes of intracerebral hematoma. J. Clin. Neurosci. 2019, 67, 75–79. [Google Scholar] [CrossRef]
- Slavin, S.J.; Sucharew, H.; Alwell, K.; Moomaw, C.J.; Woo, D.; Adeoye, O.; Flaherty, M.L.; Ferioli, S.; McMullan, J.; Mackey, J.; et al. Prehospital neurological deterioration in stroke. Emerg. Med. J. 2018, 35, 507–510. [Google Scholar] [CrossRef] [PubMed]
- Hatcher, S.; Chen, C.; Govindarajan, P. Prehospital Systolic Hypertension and Outcomes in Patients with Spontaneous Intracerebral Hemorrhage. Cureus 2017, 9, e998. [Google Scholar] [CrossRef]
- Rodriguez-Luna, D.; Rodriguez-Villatoro, N.; Juega, J.M.; Boned, S.; Muchada, M.; Sanjuan, E.; Pagola, J.; Rubiera, M.; Ribo, M.; Coscojuela, P.; et al. Prehospital Systolic Blood Pressure Is Related to Intracerebral Hemorrhage Volume on Admission. Stroke 2018, 49, 204–206. [Google Scholar] [CrossRef]
- Shkirkova, K.; Saver, J.L.; Starkman, S.; Wong, G.; Weng, J.; Hamilton, S.; Liebeskind, D.S.; Eckstein, M.; Stratton, S.; Pratt, F.; et al. Frequency, Predictors, and Outcomes of Prehospital and Early Postarrival Neurological Deterioration in Acute Stroke: Exploratory Analysis of the FAST-MAG Randomized Clinical Trial. JAMA Neurol. 2018, 75, 1364–1374. [Google Scholar] [CrossRef] [PubMed]
- Kobsa, J.; Prasad, A.; Soto, A.; Kodali, S.; Nguyen, C.K.; Peshwe, K.U.; Orozco, D.Q.; Farooqui, M.; Zevallos, C.; Sansing, L.; et al. Prehospital Blood Pressure Reductions Are Associated with Neurologic Worsening in Patients with Large-vessel Occlusion Stroke (2844). Neurology 2021, 96, 2844. [Google Scholar] [CrossRef]
- Nardin, C.; Rattazzi, M.; Pauletto, P. Blood Pressure Variability and Therapeutic Implications in Hypertension and Cardiovascular Diseases. High. Blood Press. Cardiovasc. Prev. 2019, 26, 353–359. [Google Scholar] [CrossRef]
- Kench, C.A. Effect of blood pressure on stroke severity and outcomes in acute cases. J. Paramed. Pract. 2020, 12, 157–166. [Google Scholar] [CrossRef]
- Gioia, L.C.; Zewude, R.T.; Kate, M.P.; Liss, K.; Rowe, B.H.; Buck, B.; Jeerakathil, T.; Butcher, K. Prehospital systolic blood pressure is higher in acute stroke compared with stroke mimics. Neurology 2016, 86, 2146–2153. [Google Scholar] [CrossRef]
- Asaithambi, G.; Chaudhry, S.A.; Hassan, A.E.; Rodriguez, G.J.; Suri, M.F.; Qureshi, A.I. Adherence to guidelines by emergency medical services during transport of stroke patients receiving intravenous thrombolytic infusion. J. Stroke Cerebrovasc. Dis. 2013, 22, e42–e45. [Google Scholar] [CrossRef] [PubMed]
- Fouche, P.F.; Jennings, P.A.; Boyle, M.; Bernard, S.; Smith, K. The utility of the brain trauma evidence to inform paramedic rapid sequence intubation in out-of-hospital stroke. BMC Emerg. Med. 2020, 20, 5. [Google Scholar] [CrossRef] [PubMed]
- Yperzeele, L.; van Hooff, R.J.; De Smedt, A.; Nagels, G.; Hubloue, I.; De Keyser, J.; Brouns, R. Feasibility, Reliability and Predictive Value of In-Ambulance Heart Rate Variability Registration. PLoS ONE 2016, 11, e0154834. [Google Scholar] [CrossRef]
- Tran, Q.K.; Strong, J.; Al Rebh, H.; Gatz, J.D.; Pope, K.; Jenkins, R.; Nguyen, T.; Tuteja, G.; Vuchula, S.; Chang, W.T. 123 Emergency Providers Adequately Manage Mechanical Ventilation in Critically Ill Patients with Spontaneous Intracranial Hemorrhage and Elevated Intracranial Pressure. Ann. Emerg. Med. 2017, 70, S50. [Google Scholar] [CrossRef]
- Ankolekar, S.; Fuller, M.; Cross, I.; Renton, C.; Cox, P.; Sprigg, N.; Siriwardena, A.N.; Bath, P.M. Feasibility of an ambulance-based stroke trial, and safety of glyceryl trinitrate in ultra-acute stroke: The rapid intervention with glyceryl trinitrate in hypertensive stroke trial (RIGHT, ISRCTN66434824). Stroke 2013, 44, 3120–3128. [Google Scholar] [CrossRef]
- Shaw, L.; Price, C.; McLure, S.; Howel, D.; McColl, E.; Younger, P.; Ford, G.A. Paramedic Initiated Lisinopril for Acute Stroke Treatment (PIL-FAST): Results from the pilot randomised controlled trial. Emerg. Med. J. 2014, 31, 994–999. [Google Scholar] [CrossRef] [PubMed]
- Saver, J.L.; Starkman, S.; Eckstein, M.; Stratton, S.J.; Pratt, F.D.; Hamilton, S.; Conwit, R.; Liebeskind, D.S.; Sung, G.; Kramer, I.; et al. Prehospital use of magnesium sulfate as neuroprotection in acute stroke. N. Engl. J. Med. 2015, 372, 528–536. [Google Scholar] [CrossRef] [PubMed]
- Dylla, L.; Cushman, J.T.; Abar, B.; Benesch, C.; Jones, C.M.; O’Banion, M.K.; Adler, D.H. Retrospective analysis of the hemodynamic consequences of prehospital supplemental oxygen in acute stroke. Acad. Emerg. Med. 2020, 27, S252. [Google Scholar] [CrossRef] [PubMed]
- Plowman, K.; Lindner, D.; Valle-Giler, E.; Ashkin, A.; Bass, J.; Ruthman, C. Subdural hematoma expansion in relation to measured mean and peak systolic blood pressure: A retrospective analysis. Front. Neurol. 2022, 13, 1026471. [Google Scholar] [CrossRef] [PubMed]
- Chung, P.-W.; Kim, J.-T.; Sanossian, N.; Starkmann, S.; Hamilton, S.; Gornbein, J.; Conwit, R.; Eckstein, M.; Pratt, F.; Stratton, S.; et al. Association Between Hyperacute Stage Blood Pressure Variability and Outcome in Patients with Spontaneous Intracerebral Hemorrhage. Stroke 2018, 49, 348–354. [Google Scholar] [CrossRef]
- Manning, L.S.; Rothwell, P.M.; Potter, J.F.; Robinson, T.G. Prognostic Significance of Short-Term Blood Pressure Variability in Acute Stroke. Stroke 2015, 46, 2482–2490. [Google Scholar] [CrossRef] [PubMed]
- Lees, T.; Shad-Kaneez, F.; Simpson, A.M.; Nassif, N.T.; Lin, Y.; Lal, S. Heart Rate Variability as a Biomarker for Predicting Stroke, Post-stroke Complications and Functionality. Biomark. Insights 2018, 13, 1177271918786931. [Google Scholar] [CrossRef] [PubMed]
- Cooke, W.H.; Salinas, J.; Convertino, V.A.; Ludwig, D.A.; Hinds, D.; Duke, J.H.; Moore, F.A.; Holcomb, J.B. Heart rate variability and its association with mortality in prehospital trauma patients. J. Trauma. 2006, 60, 363–370, discussion 370. [Google Scholar] [CrossRef]
- King, D.R.; Ogilvie, M.P.; Pereira, B.M.; Chang, Y.; Manning, R.J.; Conner, J.A.; Schulman, C.I.; McKenney, M.G.; Proctor, K.G. Heart rate variability as a triage tool in patients with trauma during prehospital helicopter transport. J. Trauma 2009, 67, 436–440. [Google Scholar] [CrossRef]
- Bath, P.M.; Woodhouse, L.J.; Krishnan, K.; Appleton, J.P.; Anderson, C.S.; Berge, E.; Cala, L.; Dixon, M.; England, T.J.; Godolphin, P.J.; et al. Prehospital Transdermal Glyceryl Trinitrate for Ultra-Acute Intracerebral Hemorrhage: Data from the RIGHT-2 Trial. Stroke 2019, 50, 3064–3071. [Google Scholar] [CrossRef]
- Li, Q.; Warren, A.D.; Qureshi, A.I.; Morotti, A.; Falcone, G.J.; Sheth, K.N.; Shoamanesh, A.; Dowlatshahi, D.; Viswanathan, A.; Goldstein, J.N. Ultra-Early Blood Pressure Reduction Attenuates Hematoma Growth and Improves Outcome in Intracerebral Hemorrhage. Ann. Neurol. 2020, 88, 388–395. [Google Scholar] [CrossRef] [PubMed]
- Song, L.; Chen, C.; Chen, X.; Guo, Y.; Liu, F.; Lin, Y.; Billot, L.; Li, Q.; Liu, H.; Si, L.; et al. INTEnsive ambulance-delivered blood pressure Reduction in hyper-ACute stroke Trial (INTERACT4): Study protocol for a randomized controlled trial. Trials 2021, 22, 885. [Google Scholar] [CrossRef] [PubMed]
- Avgerinos, K.I.; Chatzisotiriou, A.; Haidich, A.-B.; Tsapas, A.; Lioutas, V.-A. Intravenous Magnesium Sulfate in Acute Stroke. Stroke 2019, 50, 931–938. [Google Scholar] [CrossRef] [PubMed]
- Dylla, L.; Adler, D.H.; Abar, B.; Benesch, C.; Jones, C.M.C.; Kerry O’Banion, M.; Cushman, J.T. Prehospital supplemental oxygen for acute stroke—A retrospective analysis. Am. J. Emerg. Med. 2020, 38, 2324–2328. [Google Scholar] [CrossRef]
- Chan, Y.F.; Katz, M.; Moskowitz, A.; Levine, S.R.; Richardson, L.D.; Tuhrim, S.; Chason, K.; Barsan-Silverman, K.; Singhal, A. Supplemental oxygen delivery to suspected stroke patients in pre hospital and emergency department settings. Med. Gas. Res. 2014, 4, 16. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alshehri, A.; Ince, J.; Panerai, R.B.; Divall, P.; Robinson, T.G.; Minhas, J.S. Physiological Variability during Prehospital Stroke Care: Which Monitoring and Interventions Are Used? Healthcare 2024, 12, 835. https://doi.org/10.3390/healthcare12080835
Alshehri A, Ince J, Panerai RB, Divall P, Robinson TG, Minhas JS. Physiological Variability during Prehospital Stroke Care: Which Monitoring and Interventions Are Used? Healthcare. 2024; 12(8):835. https://doi.org/10.3390/healthcare12080835
Chicago/Turabian StyleAlshehri, Abdulaziz, Jonathan Ince, Ronney B. Panerai, Pip Divall, Thompson G. Robinson, and Jatinder S. Minhas. 2024. "Physiological Variability during Prehospital Stroke Care: Which Monitoring and Interventions Are Used?" Healthcare 12, no. 8: 835. https://doi.org/10.3390/healthcare12080835
APA StyleAlshehri, A., Ince, J., Panerai, R. B., Divall, P., Robinson, T. G., & Minhas, J. S. (2024). Physiological Variability during Prehospital Stroke Care: Which Monitoring and Interventions Are Used? Healthcare, 12(8), 835. https://doi.org/10.3390/healthcare12080835