
Knowledge on Stroke Recognition and Management among Emergency Department Healthcare Professionals in the Republic of Cyprus

 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Setting
2.2. Participants and Sample Size
2.3. Data Collection and Instrument
- -
- Sociodemographic and employment characteristics (8 closed-ended questions): this section assessed factors as age, gender, profession, educational attainment, employment status, type of hospital (public or private), years of work experience, and previous education or training in stroke, along with the sources of such education.
- -
- Knowledge on stroke recognition and management (28 questions): this section included:
- (a)
- General knowledge on stroke (GKS): four questions with responses: ‘right’, ‘wrong’, or ‘I don’t know’.
- (b)
- Knowledge on stroke recognition (KSR): two multiple-choice questions and six questions with responses: ‘right’, ‘wrong’, or ‘I don’t know’.
- (c)
- Knowledge on stroke management (KSM): two multiple-choice questions and 14 questions with responses: ‘right’, ‘wrong’, or ‘I don’t know’.
- -
- Self-assessment on knowledge of stroke recognition and management: one question with responses: ‘poorly’, ‘well’, ‘very well’, and ‘expert’.
2.4. Questionnaire Development
2.5. Ethics Approval
2.6. Data Analysis
3. Results
3.1. Questionnaire Testing
3.2. Sociodemographic and Employment Characteristics of Study Participants
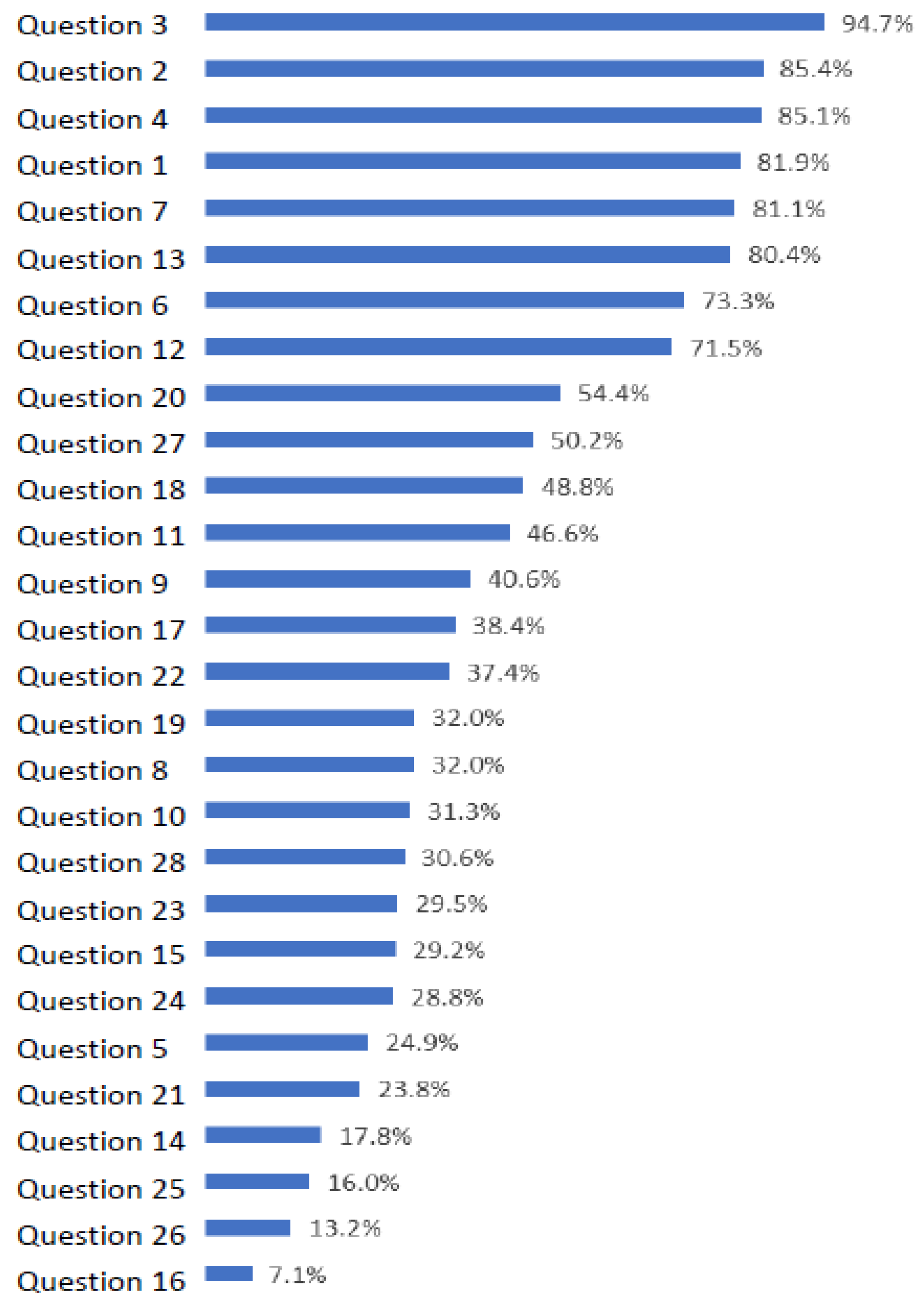
3.3. Stroke Knowledge Levels
3.4. Univariate and Multivariate Predictors of Stroke Knowledge
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Patel, A.; Berdunov, V.; King, D.; Quayyum, Z.; Wittenberg, R.; Knapp, M. Current, Future and Avoidable Costs of Stroke in the UK; Executive Summary Part 2; Stroke Association: London, UK, 2017; 12p. [Google Scholar]
- Virani, S.S.; Alonso, A.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Delling, F.N.; et al. Heart Disease and Stroke Statistics—2020 Update: A Report from the American Heart Association. Circulation 2020, 141, e139–e596. [Google Scholar] [CrossRef] [PubMed]
- Wafa, H.A.; Wolfe, C.D.A.; Emmett, E.; Roth, G.A.; Johnson, C.O.; Wang, Y. Burden of Stroke in Europe: Thirty-Year Projections of Incidence, Prevalence, Deaths, and Disability-Adjusted Life Years. Stroke 2020, 51, 2418–2427. [Google Scholar] [CrossRef] [PubMed]
- He, A.H.; Churilov, L.; Mitchell, P.J.; Dowling, R.J.; Yan, B. Every 15-Min Delay in Recanalization by Intra-Arterial Therapy in Acute Ischemic Stroke Increases Risk of Poor Outcome. Int. J. Stroke 2015, 10, 1062–1067. [Google Scholar] [CrossRef] [PubMed]
- Powers, W.J.; Rabinstein, A.A.; Ackerson, T.; Adeoye, O.M.; Bambakidis, N.C.; Becker, K.; Biller, J.; Brown, M.; Demaerschalk, B.M.; Hoh, B.; et al. Guidelines for the Early Management of Patients with Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline for Healthcare Professionals from the American Heart Association/American Stroke. Stroke 2019, 50, e344–e418. [Google Scholar] [CrossRef]
- Angels Initiative—Global Stroke Hospitals & E-Learning Centre. Available online: https://www.angels-initiative.com/ (accessed on 19 December 2023).
- ASLS Course. American Heart Association CPR & First Aid. Available online: https://cpr.heart.org/en/cpr-courses-and-kits/healthcare-professional/asls-course (accessed on 19 December 2023).
- Jauch, E.C.; Saver, J.L.; Adams, H.P.; Bruno, A.; Connors, J.J.B.; Demaerschalk, B.M.; Khatri, P.; McMullan, P.W.; Qureshi, A.I.; Rosenfield, K.; et al. Guidelines for the Early Management of Patients with Acute Ischemic Stroke: A Guideline for Healthcare Professionals from the American Heart Association/American Stroke Association. Stroke 2013, 44, 870–947. [Google Scholar] [CrossRef] [PubMed]
- Kleindorfer, D.O.; Towfighi, A.; Chaturvedi, S.; Cockroft, K.M.; Gutierrez, J.; Lombardi-Hill, D.; Kamel, H.; Kernan, W.N.; Kittner, S.J.; Leira, E.C.; et al. 2021 Guideline for the Prevention of Stroke in Patients with Stroke and Transient Ischemic Attack: A Guideline from the American Heart Association/American Stroke Association. Stroke 2021, 52, e364–e467. [Google Scholar] [CrossRef] [PubMed]
- Althubaity, E.; Yunus, F.; Khathaami, A. Al Assessment of the Experience of Saudi Emergency Medical Services Personnel with Acute Stroke. Neurosciences 2013, 18, 40–45. [Google Scholar] [PubMed]
- Li, T.; Munder, S.P.; Chaudhry, A.; Madan, R.; Gribko, M.; Arora, R. Emergency Medical Services Providers’ Knowledge, Practices, and Barriers to Stroke Management. Open Access Emerg. Med. 2019, 11, 297–303. [Google Scholar] [CrossRef]
- Dibiasio, E.L.; Jayaraman, M.V.; Oliver, L.; Paolucci, G.; Clark, M.; Watkins, C.; Delisi, K.; Wilks, A.; Yaghi, S.; Hemendinger, M.; et al. Emergency Medical Systems Education May Improve Knowledge of Pre-Hospital Stroke Triage Protocols. J. Neurointerv. Surg. 2020, 12, 370–373. [Google Scholar] [CrossRef]
- Shire, F.; Kasim, Z.; Alrukn, S.; Khan, M. Stroke Awareness among Dubai Emergency Medical Service Staff and Impact of an Educational Intervention. BMC Res. Notes 2017, 10, 255. [Google Scholar] [CrossRef]
- Gorchs-Molist, M.; Solà-Muñoz, S.; Enjo-Perez, I.; Querol-Gil, M.; Carrera-Giraldo, D.; Nicolàs-Arfelis, J.M.; Jiménez-Fàbrega, F.X.; de la Ossa, N.P. An Online Training Intervention on Prehospital Stroke Codes in Catalonia to Improve the Knowledge, Pre-Notification Compliance and Time Performance of Emergency Medical Services Professionals. Int. J. Environ. Res. Public Health 2020, 17, 6183. [Google Scholar] [CrossRef]
- Sveikata, L.; Melaika, K.; Wiśniewski, A.; Vilionskis, A.; Petrikonis, K.; Stankevičius, E.; Jurjans, K.; Ekkert, A.; Jatužis, D.; Masiliūnas, R. Interactive Training of the Emergency Medical Services Improved Prehospital Stroke Recognition and Transport Time. Front. Neurol. 2022, 13, 765165. [Google Scholar] [CrossRef]
- Prabhakaran, S.; Ward, E.; John, S.; Lopes, D.K.; Chen, M.; Temes, R.E.; Mohammad, Y.; Lee, V.H.; Bleck, T.P. Transfer Delay Is a Major Factor Limiting the Use of Intra-Arterial Treatment in Acute Ischemic Stroke. Stroke 2011, 42, 1626–1630. [Google Scholar] [CrossRef]
- McTaggart, R.A.; Ansari, S.A.; Goyal, M.; Abruzzo, T.A.; Albani, B.; Arthur, A.J.; Alexander, M.J.; Albuquerque, F.C.; Baxter, B.; Bulsara, K.R.; et al. Initial Hospital Management of Patients with Emergent Large Vessel Occlusion (ELVO): Report of the Standards and Guidelines Committee of the Society of NeuroInterventional Surgery. J. Neurointerv. Surg. 2017, 9, 316–323. [Google Scholar] [CrossRef]
- Leong, B.Y.G.; Ni, H.M.J.; Tiah, L.; Tan, C. The Challenge of Tightening Door-to-Needle Timings in a Telestroke Setting: An Emergency Medicine Driven Initiative. Cureus 2020, 12, e12316. [Google Scholar] [CrossRef]
- Craig, L.E.; McInnes, E.; Taylor, N.; Grimley, R.; Cadilhac, D.A.; Considine, J.; Middleton, S. Identifying the Barriers and Enablers for a Triage, Treatment, and Transfer Clinical Intervention to Manage Acute Stroke Patients in the Emergency Department: A Systematic Review Using the Theoretical Domains Framework (TDF). Implement. Sci. 2016, 11, 157. [Google Scholar] [CrossRef]
- Baatiema, L.; Otim, M.; Mnatzaganian, G.; Aikins, A.D.G.; Coombes, J.; Somerset, S. Towards Best Practice in Acute Stroke Care in Ghana: A Survey of Hospital Services. BMC Health Serv. Res. 2017, 17, 108. [Google Scholar] [CrossRef]
- Bruins Slot, K.; Murray, V.; Boysen, G.; Berge, E. Thrombolytic Treatment for Stroke in the Scandinavian Countries. Acta Neurol. Scand. 2009, 120, 270–276. [Google Scholar] [CrossRef]
- Meurer, W.J.; Majersik, J.J.; Frederiksen, S.M.; Kade, A.M.; Sandretto, A.M.; Scott, P.A. Provider Perceptions of Barriers to the Emergency Use of TPA for Acute Ischemic Stroke: A Qualitative Study. BMC Emerg. Med. 2011, 11, 5. [Google Scholar] [CrossRef]
- Lamba, S.; Murano, T.; Nagurka, R. Emergency Department Healthcare Providers’ Knowledge of Ischemic Stroke. Res. Dev. Med. Educ. 2013, 2, 50–53. [Google Scholar] [CrossRef]
- Williams, J.M.; Jude, M.R.; Levi, C.R. Recombinant Tissue Plasminogen Activator (Rt-PA) Utilisation by Rural Clinicians in Acute Ischaemic Stroke: A Survey of Barriers and Enablers. Aust. J. Rural Health 2013, 21, 262–267. [Google Scholar] [CrossRef] [PubMed]
- Stecksén, A.; Lundman, B.; Eriksson, M.; Glader, E.L.; Asplund, K. Implementing Thrombolytic Guidelines in Stroke Care: Perceived Facilitators and Barriers. Qual. Health Res. 2014, 24, 412–419. [Google Scholar] [CrossRef] [PubMed]
- Grady, A.M.; Bryant, J.; Carey, M.L.; Paul, C.L.; Sanson-Fisher, R.W.; Levi, C.R. Agreement with Evidence for Tissue Plasminogen Activator Use among Emergency Physicians: A Cross-Sectional Survey. BMC Res. Notes 2015, 8, 267. [Google Scholar] [CrossRef] [PubMed]
- Al Khathaami, A.M.; Aloraini, H.; Almudlej, S.; Al Issa, H.; Elshammaa, N.; Alsolamy, S. Knowledge and Attitudes of Saudi Emergency Physicians toward T-PA Use in Stroke. Neurol. Res. Int. 2018, 2018, 3050278. [Google Scholar] [CrossRef] [PubMed]
- Alanazi, A.; Alosaimi, M.; Aldawsari, R.M.; Alatwai, A.M.; Idris, M.A. Saudi Emergency Physicians’ Knowledge about Recombinant Tissue Plasminogen Activator for Acute Ischemic Stroke. Arch. Pharm. Pract. 2019, 10, 49–53. [Google Scholar]
- Sbampato dos Santos, J.V.; Aparecida de Melo, E.; Lopes da Silveira Junior, J.; Nascimento Vasconcelos, N.; de Castro Lima, M.; Moreira Damázio, L.C. The Effects of Nursing Training on the Evaluation of Patients with Cerebrovascular Accident. J. Nurs. UFPE/Rev. Enferm. UFPE 2017, 11, 1763–1768. [Google Scholar] [CrossRef]
- Baby, P.; Srijithesh, P.; Ashraf, J.; Kannan, D. Emergency Nurses’ Knowledge about Tissue Plasminogen Activator Therapy and Their Perception about Barriers for Thrombolysis in Acute Stroke Care. Int. J. Noncommunicable Dis. 2019, 4, 121. [Google Scholar] [CrossRef]
- Thomas, L.H.; Harrington, K.; Rogers, H.; Langhorne, P.; Smith, M.; Bond, S. Development of a Scale to Assess Nurses’ Knowledge of Stroke: A Pilot Study. Clin. Rehabil. 1999, 13, 518–526. [Google Scholar] [CrossRef]
- Harper, J.P. Emergency Nurses’ Knowledge of Evidence-Based Ischemic Stroke Care: A Pilot Study. J. Emerg. Nurs. 2007, 33, 202–207. [Google Scholar] [CrossRef]
- Traynelis, L. Emergency Department Nurses’ Knowledge of Evidence-Based Ischemic Stroke Care. Kaleidoscope 2012, 10, 44. [Google Scholar]
- Adelman, E.E.; Meurer, W.J.; Nance, D.K.; Kocan, M.J.; Maddox, K.E.; Morgenstern, L.B.; Skolarus, L.E. Stroke Awareness among Inpatient Nursing Staff at an Academic Medical Center. Stroke 2014, 45, 271–273. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, S.S.; Murray, L.L.; Mclennon, S.M.; Bakas, T. Implementation of a Stroke Competency Program to Improve Nurses’ Knowledge of and Adherence to Stroke Guidelines. J. Neurosci. Nurs. 2016, 48, 328–335. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.; Vakani, R.; Kussin, P.; Guhwe, M.; Farjat, A.E.; Choudhury, K.; Renner, D.; Oduor, C.; Graffagnino, C. Assessment of Healthcare Personnel Knowledge of Stroke Care at a Large Referral Hospital in Sub-Saharan Africa—A Survey Based Approach. J. Clin. Neurosci. 2017, 42, 71–74. [Google Scholar] [CrossRef] [PubMed]
- Berge, E.; Whiteley, W.; Audebert, H.; De Marchis, G.; Fonseca, A.C.; Padiglioni, C.; Pérez de la Ossa, N.; Strbian, D.; Tsivgoulis, G.; Turc, G. European Stroke Organisation (ESO) Guidelines on Intravenous Thrombolysis for Acute Ischaemic Stroke. Eur. Stroke J. 2021, 6, I–LXII. [Google Scholar] [CrossRef] [PubMed]
- Anderson, E.; Fernandez, S.; Ganzman, A.; Miller, E.C. Incorporating Nonphysician Stroke Specialists Into the Stroke Team. Stroke 2017, 48, e323–e325. [Google Scholar] [CrossRef] [PubMed]
- Vandenbroucke, J.P.; Von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and Elaboration. Int. J. Surg. 2014, 12, 1500–1524. [Google Scholar] [CrossRef]
- Erdfelder, E.; FAul, F.; Buchner, A.; Lang, A.G. Statistical Power Analyses Using G*Power 3.1: Tests for Correlation and Regression Analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef]
- Gnatzy, T.; Warth, J.; von der Gracht, H.; Darkow, I.L. Validating an Innovative Real-Time Delphi Approach—A Methodological Comparison between Real-Time and Conventional Delphi Studies. Technol. Forecast. Soc. Chang. 2011, 78, 1681–1694. [Google Scholar] [CrossRef]
- Sim, J.; Wright, C.C. The Kappa Statistic in Reliability Studies: Use, Interpretation, and Sample Size Requirements. Phys. Ther. 2005, 85, 257–268. [Google Scholar] [CrossRef]
- De Vet, H.C.W.; Terwee, C.B.; Mokkink, L.B.; Knol, D.L. Measurement in Medicine; A Practical Guide; Cambridge University Press (CUP): Cambridge, UK, 2011; pp. 1–338. [Google Scholar] [CrossRef]
- Albart, S.A.; Khan, A.H.K.Y.; Rashid, A.A.; Zaidi, W.A.W.; Bidin, M.Z.; Looi, I.; Hoo, F.K. Knowledge of Acute Stroke Management and the Predictors among Malaysian Healthcare Professionals. PeerJ 2022, 10, e13310. [Google Scholar] [CrossRef]
- Baatiema, L.; De-Graft Aikins, A.; Sav, A.; Mnatzaganian, G.; Chan, C.K.Y.; Somerset, S. Barriers to Evidence-Based Acute Stroke Care in Ghana: A Qualitative Study on the Perspectives of Stroke Care Professionals. BMJ Open 2017, 7, e015385. [Google Scholar] [CrossRef] [PubMed]
- Saeed, M.; Naga, A.; Bedier, N.A.; Salem, M.A.; Abdel, H.; Ahmed, M.; Elhfnawy, A.M. Effect of Competency Based Program on Nurses’ Knowledge, Skills and Attitude toward the Care of Patients with Stroke. ASNJ 2021, 23, 10–21. [Google Scholar] [CrossRef]
- Jones, S.P.; Miller, C.; Gibson, J.M.E.; Cook, J.; Price, C.; Watkins, C.L. The Impact of Education and Training Interventions for Nurses and Other Health Care Staff Involved in the Delivery of Stroke Care: An Integrative Review. Nurse Educ. Today 2018, 61, 249–257. [Google Scholar] [CrossRef]
- Dávalos, A.; Castillo, J.; Martinez-Vila, E. Delay in Neurological Attention and Stroke Outcome. Stroke 1995, 26, 2233–2237. [Google Scholar] [CrossRef]
- Lee, E.-J.; Kim, S.J.; Bae, J.; Lee, E.J.; Kwon, O.D.; Jeongid, H.-Y.; Kimid, Y.; Jeongid, H.-B. Impact of Onset-to-Door Time on Outcomes and Factors Associated with Late Hospital Arrival in Patients with Acute Ischemic Stroke. PLoS ONE 2021, 16, e0247829. [Google Scholar] [CrossRef] [PubMed]
- Larsen, K.; Jæger, H.S.; Hov, M.R.; Thorsen, K.; Solyga, V.; Lund, C.G.; Bache, K.G. Streamlining Acute Stroke Care by Introducing National Institutes of Health Stroke Scale in the Emergency Medical Services: A Prospective Cohort Study. Stroke 2022, 53, 2050–2057. [Google Scholar] [CrossRef]
- Liu, X.; Weng, Y.; Liu, R.; Zhao, J. Significant Stroke Knowledge Deficiencies in Community Physician Improved with Stroke 120. J. Stroke Cerebrovasc. Dis. 2019, 28, 104323. [Google Scholar] [CrossRef]
- Donnelly, S.C. In Stroke—When to Thrombolyse or Not to Thrombolyse—That Is the Question! QJM Int. J. Med. 2019, 112, 321–322. [Google Scholar] [CrossRef]
- Blek, N.; Szarpak, L. Profile of Practices and Knowledge on Stroke among Polish Emergency Medical Service Staff. Disaster Emerg. Med. J. 2021, 6, 55–62. [Google Scholar] [CrossRef]
- Feroze, R.; Prabhu, A.V.; Agarwal, N. Stroke Education Is Underrepresented in U.S. Undergraduate Clinical Curricula. Acad. Med. 2017, 92, 435. [Google Scholar] [CrossRef]
- Poppe, A.Y.; Casaubon, L.K.; Gubitz, G.; Shoamanesh, A. Education in Stroke Medicine a Canadian Perspective. Stroke 2019, 50, e421–e423. [Google Scholar] [CrossRef] [PubMed]
- Zarandona, J.; Hoyos Cillero, I.; Arrue, M. Teaching and Learning about Stroke Care in Undergraduate Nursing Students: A Scoping Review of the Literature. Rev. Científica Soc. Española Enfermería Neurológica 2019, 50, 32–38. [Google Scholar] [CrossRef]
- Hartnett, K.P.; Kite-Powell, A.; DeVies, J.; Coletta, M.A.; Boehmer, T.K.; Adjemian, J.; Gundlapalli, A.V. Impact of the COVID-19 Pandemic on Emergency Department Visits—United States, January 1, 2019–May 30, 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 699–704. [Google Scholar] [CrossRef] [PubMed]
- Quattrocchi, A.; Mamais, I.; Tsioutis, C.; Christaki, E.; Constantinou, C.; Koliou, M.; Pana, Z.-D.; Silvestros, V.; Theophanous, F.; Haralambous, C.; et al. Extensive Testing and Public Health Interventions for the Control of COVID-19 in the Republic of Cyprus between March and May 2020. J. Clin. Med. 2020, 9, 3598. [Google Scholar] [CrossRef]

{kind=link}
| Question | Kappa | Agreement Percentage |
|---|---|---|
| 0.73 | 87% |
| 0.86 | 93% |
| 1.00 | 100% |
| 0.33 | 73% |
| 0.55 | 80% |
| 0.47 | 80% |
| 0.59 | 87% |
| 0.48 | 73% |
| 0.21 | 67% |
| 0.71 | 87% |
| 1.00 | 100% |
| 0.59 | 80% |
| 1.00 | 100% |
| 0.57 | 80% |
| 0.47 | 80% |
| 0.25 | 73% |
| 0.86 | 93% |
| 0.66 | 87% |
| 0.86 | 93% |
| 0.42 | 87% |
| 0.66 | 87% |
| 0.81 | 93% |
| 0.42 | 87% |
| 0.84 | 93% |
| 0.81 | 93% |
| 1.00 | 100% |
| 1.00 | 100% |
| 0.86 | 93% |
| Nurses | Physicians | Total | |
|---|---|---|---|
| If you had any prior education or training relevant to stroke care, what was the source of such education or training? | Ν (%) | Ν (%) | Ν (%) |
| Self-guided study | 3 (2.2) | 2 (10) | 5 (3.2) |
| Congress/educational workshop | 49 (35.8) | 8 (40) | 57 (36.3) |
| Class (postgraduate level) | 6 (4.4) | 1 (5) | 7 (4.5) |
| Class (undergraduate level) | 38 (27.7) | 8 (40) | 46 (29.3) |
| Brief presentation on stroke care | 37 (27) | 0 (0) | 37 (23.5) |
| Leaflet/other printed material | 4 (2.9) | 1 (5) | 5 (3.2) |
| Total | 137 (100) | 20 (100) | 157 (100) |
| Nurses | Physicians | Total | |
|---|---|---|---|
| Mean (SD) | Mean (SD) | Mean (SD) | |
| Total score | 12.6 (4.1) | 15.7 (4) | 12.9 (4.2) |
| General knowledge on stroke (4 items) | 3.5 (0.9) | 3.7 (0.9) | 3.5 (0.9) |
| Knowledge on stroke recognition (8 items) | 3.9 (1.6) | 5 (1.5) | 4 (1.6) |
| Knowledge on stroke management (16 items) | 5.2 (2.7) | 7 (2.4) | 5.4 (2.7) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rossis, C.; Michail, K.A.; Middleton, N.; Karanikola, M.; Papathanassoglou, E.; Mpouzika, M. Knowledge on Stroke Recognition and Management among Emergency Department Healthcare Professionals in the Republic of Cyprus. Healthcare 2024, 12, 77. https://doi.org/10.3390/healthcare12010077
Rossis C, Michail KA, Middleton N, Karanikola M, Papathanassoglou E, Mpouzika M. Knowledge on Stroke Recognition and Management among Emergency Department Healthcare Professionals in the Republic of Cyprus. Healthcare. 2024; 12(1):77. https://doi.org/10.3390/healthcare12010077
Chicago/Turabian StyleRossis, Christos, Koralia A. Michail, Nicos Middleton, Maria Karanikola, Elizabeth Papathanassoglou, and Meropi Mpouzika. 2024. "Knowledge on Stroke Recognition and Management among Emergency Department Healthcare Professionals in the Republic of Cyprus" Healthcare 12, no. 1: 77. https://doi.org/10.3390/healthcare12010077
APA StyleRossis, C., Michail, K. A., Middleton, N., Karanikola, M., Papathanassoglou, E., & Mpouzika, M. (2024). Knowledge on Stroke Recognition and Management among Emergency Department Healthcare Professionals in the Republic of Cyprus. Healthcare, 12(1), 77. https://doi.org/10.3390/healthcare12010077