
_MD__MPH_PhD.png)
Physical Activity, Quality of Live and Well-Being in Individuals with Intellectual and Developmental Disability

 ,
,  , , , and
, , , and
Abstract
1. Introduction
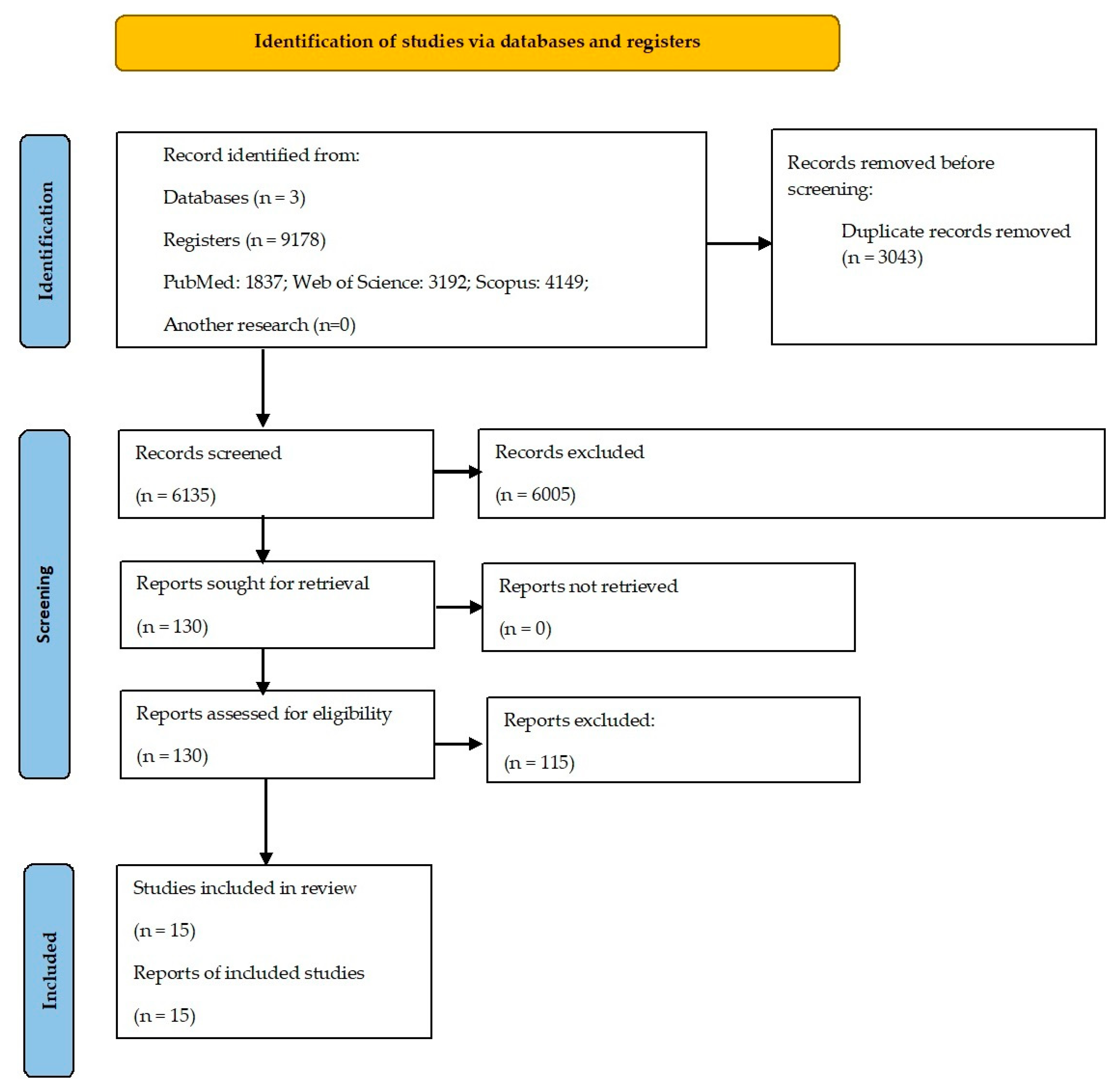
2. Materials and Methods
2.1. Information Sources and Research Strategies
2.2. Eligibility Criteria
2.3. Selection and Data Collection Process
3. Results
3.1. Selection of Studies
3.2. Methodological Quality
3.3. Characteristics of the Studies
3.4. Origin
3.5. Type of Studies
3.6. Participants
3.7. Exercise Prescription
3.8. Evaluation Techniques
4. Discussion
4.1. Quality of Life
4.2. Well-Being
4.3. Exercise Prescription
4.4. Limitations, Future Research and Practical Application
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Schalock, R.L.; Luckasson, R.; Tassé, M.J. An Overview of Intellectual Disability: Definition, Diagnosis, Classification, and Systems of Supports (12th Ed.). Am. J. Intellect. Dev. Disabil. 2021, 126, 439–442. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, A.R.; Santos, S.; Rodrigues, A.; Estevens, M.; Sousa, E. Executive Profile of Adults with Intellectual Disability and Psychomotor Intervention’ Effects on Executive Functioning. Physiother. Res. Rep. 2019, 2, 1–7. [Google Scholar] [CrossRef]
- Santos, S. Como Lidar Com a Dificuldade Intelectual e Desenvolvimental; Flora Editora: Braga, Portugal, 2020. [Google Scholar]
- Cleaver, S.; Hunter, D.; Ouellette-Kuntz, H. Physical Mobility Limitations in Adults with Intellectual Disabilities: A Systematic Review. J. Intellect. Disabil. Res. 2009, 53, 93–105. [Google Scholar] [CrossRef] [PubMed]
- Pitetti, K.H.; Yarmer, D.A. Lower Body Strength of Children and Adolescents with and Without Mild Mental Retardation: A Comparison. Adapt. Phys. Act. Q. 2002, 19, 68–81. [Google Scholar] [CrossRef] [PubMed]
- Carmeli, E.; Bar-Yossef, T.; Ariav, C.; Levy, R.; Liebermann, D.G. Perceptual-Motor Coordination in Persons with Mild Intellectual Disability. Disabil. Rehabil. 2008, 30, 323–329. [Google Scholar] [CrossRef]
- Bartlo, P.; Klein, P.J. Physical Activity Benefits and Needs in Adults with Intellectual Disabilities: Systematic Review of the Literature. Am. J. Intellect. Dev. Disabil. 2011, 116, 220–232. [Google Scholar] [CrossRef] [PubMed]
- Pierce, S.; Maher, A.J. Physical Activity among Children and Young People with Intellectual Disabilities in Special Schools: Teacher and Learning Support Assistant Perceptions. Br. J. Learn. Disabil. 2020, 48, 37–44. [Google Scholar] [CrossRef]
- Garavand, E.; Aslankhani, M.; Farsi, A. Effect of Selective Motor and Spark Programs on Loco-Motor Skills on Children with Mild Intellectual Disability. Middle East. J. Disabil. Stud. 2018, 8, 18. [Google Scholar]
- Bossink, L.W.M.; van der Putten, A.A.; Vlaskamp, C. Understanding Low Levels of Physical Activity in People with Intellectual Disabilities: A Systematic Review to Identify Barriers and Facilitators. Res. Dev. Disabil. 2017, 68, 95–110. [Google Scholar] [CrossRef]
- Cabeza-Ruiz, R.; Sánchez-López, A.M.; Trigo, M.E.; Gómez-Píriz, P.T. Feasibility and Reliability of the Assessing Levels of Physical Activity Health-Related Fitness Test Battery in Adults with Intellectual Disabilities. J. Intellect. Disabil. Res. 2020, 64, 612–628. [Google Scholar] [CrossRef]
- Calders, P.; Elmahgoub, S.; Roman de Mettelinge, T.; Vandenbroeck, C.; Dewandele, I.; Rombaut, L.; Vandevelde, A.; Cambier, D. Effect of Combined Exercise Training on Physical and Metabolic Fitness in Adults with Intellectual Disability: A Controlled Trial. Clin. Rehabil. 2011, 25, 1097–1108. [Google Scholar] [CrossRef]
- Apolone, G.; Mosconi, P. Techniques for Assessing the Quality of Life with a Particular Emphasis on Physical Exercise. In Role of Physical Exercise in Preventing Disease and Improving the Quality of Life; Stocchi, V., De Feo, P., Hood, D.A., Eds.; Springer: Milan, Italy, 2007; pp. 183–190. ISBN 978-88-470-0376-7. [Google Scholar]
- Jacinto, M.; Matos, R.; Monteiro, D.; Antunes, R.; Caseiro, A.; Gomes, B.; Campos, M.J.; Ferreira, J.P. Effects of a 24-Week Exercise Program on Anthropometric, Body Composition, Metabolic Status, Cardiovascular Response, and Neuromuscular Capacity, in Individuals with Intellectual and Developmental Disabilities. Front. Physiol. 2023, 14, 1205463. [Google Scholar] [CrossRef]
- Diz, S.; Gomes, F.; Santos, S. Does Physical Activity Improve Adaptive Behaviour, Fitness, and Quality of Life of Adults with Intellectual Disability? Rev. Bras. Ciênc. Esporte 2021, 43, e001621. [Google Scholar] [CrossRef]
- Carmeli, E.; Zinger-Vaknin, T.; Morad, M.; Merrick, J. Can Physical Training Have an Effect on Well-Being in Adults with Mild Intellectual Disability? Mech. Ageing Dev. 2005, 126, 299–304. [Google Scholar] [CrossRef]
- García Moltó, A.; Ovejero Bruna, M. Satisfacción Vital, Autodeterminación y Práctica Deportiva En Las Personas Con Discapacidad Intelectual. [Satisfaction with Life, Self-Determination and Sport Practice on People with Intellectual Disability]. Rev. Psicol. Deporte 2017, 26, 13–19. [Google Scholar]
- Crawford, C.; Burns, J.; Fernie, B.A. Psychosocial Impact of Involvement in the Special Olympics. Res. Dev. Disabil. 2015, 45–46, 93–102. [Google Scholar] [CrossRef]
- Williams, K.; Jacoby, P.; Whitehouse, A.; Kim, R.; Epstein, A.; Murphy, N.; Reid, S.; Leonard, H.; Reddihough, D.; Downs, J. Functioning, Participation, and Quality of Life in Children with Intellectual Disability: An Observational Study. Dev. Med. Child Neurol. 2021, 63, 89–96. [Google Scholar] [CrossRef]
- World Health Organization Quality of Life Group [WHOQOL Group]. WHOQOL–Measuring Quality of Life; Programme on Mental Health; WHO: Geneva, Switzerland, 1997. [Google Scholar]
- Schalock, R.; Keith, K.; Verdugo, M.; Gómez, L. Quality of Life Model Development and Use in the Field of Intellectual Disability. In Enhancing the Quality of Life of People with Intellectual Disabilities; Springer: Berlin/Heidelberg, Germany, 2011; pp. 17–32. ISBN 978-90-481-9649-4. [Google Scholar]
- Ryff, C.; Boylan, J.; Kirsch, J. Eudaimonic and Hedonic Well-Being: An Integrative Perspective with Linkages to Sociodemographic Factors and Health. In Measuring Well-Being: Interdisciplinary Perspectives from the Social Sciences and the Humanities; Oxford Academic: Oxford, UK, 2021; pp. 92–135. ISBN 978-0-19-751253-1. [Google Scholar]
- Diener, E. Subjective Well-Being. In The Science of Well-Being: The Collected Works of Ed Diener; Social indicators research series; Springer Science + Business Media: New York, NY, USA, 2009; pp. 11–58. ISBN 978-90-481-2349-0. [Google Scholar]
- Diener, E.; Emmons, R.A.; Larsen, R.J.; Griffin, S. The Satisfaction With Life Scale. J. Pers. Assess. 1985, 49, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Tellegen, A.; Watson, D.; Clark, L.A. On the Dimensional and Hierarchical Structure of Affect. Psychol. Sci. 1999, 10, 297–303. [Google Scholar] [CrossRef]
- Watson, D.; Clark, L.A.; Tellegen, A. Development and Validation of Brief Measures of Positive and Negative Affect: The PANAS Scales. J. Pers. Soc. Psychol. 1988, 54, 1063–1070. [Google Scholar] [CrossRef]
- Diener, E.; Lucas, R.E.; Oishi, S. Sujective Well-Being: The Science of Happiness and Life Satisfaction. In Handbook of Positive Psychology; Oxford University Press: New York, NY, USA, 2002; pp. 463–473. ISBN 978-0-19-513533-6. [Google Scholar]
- Cummins, R.A. Moving from the Quality of Life Concept to a Theory. J. Intellect. Disabil. Res. 2005, 49, 699–706. [Google Scholar] [CrossRef]
- Cummins, R.A.; Nistico, H. Maintaining Life Satisfaction: The Role of Positive Cognitive Bias. J. Happiness Stud. 2002, 3, 37–69. [Google Scholar] [CrossRef]
- Pavot, W.; Diener, E. The Satisfaction With Life Scale and the Emerging Construct of Life Satisfaction. J. Posit. Psychol. 2008, 3, 137–152. [Google Scholar] [CrossRef]
- Wei, L.; Hu, Y.; Tao, Y.; Hu, R.; Zhang, L. The Effects of Physical Exercise on the Quality of Life of Healthy Older Adults in China: A Systematic Review. Front. Psychol. 2022, 13, 895373. [Google Scholar] [CrossRef] [PubMed]
- Jacob, U.S.; Pillay, J.; Johnson, E.; Omoya, O.T.; Adedokun, A.P. A Systematic Review of Physical Activity: Benefits and Needs for Maintenance of Quality of Life among Adults with Intellectual Disability. Front. Sports Act. Living 2023, 5, 1184946. [Google Scholar] [CrossRef] [PubMed]
- Carmeli, E.; Barak, S.; Morad, M.; Kodesh, E. Physical Exercises Can Reduce Anxiety and Improve Quality of Life among Adults with Intellectual Disability. Int. Sport. J. 2009, 10, 77–85. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Bento, T. Revisões sistemáticas em desporto e saúde: Orientações para o planeamento, elaboração, redação e avaliação. Motricidade 2014, 10, 107–123. [Google Scholar] [CrossRef]
- Methley, A.M.; Campbell, S.; Chew-Graham, C.; McNally, R.; Cheraghi-Sohi, S. PICO, PICOS and SPIDER: A Comparison Study of Specificity and Sensitivity in Three Search Tools for Qualitative Systematic Reviews. BMC Health Serv. Res. 2014, 14, 579. [Google Scholar] [CrossRef]
- Downs, S.H.; Black, N. The Feasibility of Creating a Checklist for the Assessment of the Methodological Quality Both of Randomised and Non-Randomised Studies of Health Care Interventions. J. Epidemiol. Community Health 1998, 52, 377–384. [Google Scholar] [CrossRef]
- Barnet-Lopez, S.; Pérez Testor, S.; Sanromà, J.; Oviedo, G.; Guerra-Balic, M. Dance/Movement Therapy and Emotional Well-Being for Adults with Intellectual Disabilities. Arts Psychother. 2016, 51, 10–16. [Google Scholar] [CrossRef]
- Bowers, K.; Corby, D.; Lambert, V.; Staines, A.; McVeigh, T.; McKeon, M.; Hoey, E.; Belton, S.; Meegan, S.; Walsh, D.; et al. People with Intellectual Disability and Their Families’ Perspectives of Special Olympics Ireland: Qualitative Findings from the SOPHIE Study. J. Intellect. Disabil. 2016, 20, 354–370. [Google Scholar] [CrossRef]
- Carbó-Carreté, M.; Guàrdia-Olmos, J.; Giné, C.; Schalock, R.L. A Structural Equation Model of the Relationship between Physical Activity and Quality of Life. Int. J. Clin. Health Psychol. 2016, 16, 147–156. [Google Scholar] [CrossRef]
- Fjellstrom, S.; Hansen, E.; Hölttä, J.; Zingmark, M.; Nordström, A.; Lund Ohlsson, M. Web-Based Training Intervention to Increase Physical Activity Level and Improve Health for Adults with Intellectual Disability. J. Intellect. Disabil. Res. 2022, 66, 967–977. [Google Scholar] [CrossRef]
- Mercado García, E.; Merino Gallego, C.; González Casas, D. Los beneficios de la danza en la mejora de la calidad de vida (CdV) de personas con discapacidad intelectual (PcDI). Altern. Cuad. Trab. Soc. 2021, 28, 215–246. [Google Scholar] [CrossRef]
- Özkan, Z.; Kale, R. Investigation of the Effects of Physical Education Activities on Motor Skills and Quality of Life in Children with Intellectual Disability. Int. J. Dev. Disabil. 2021, 69, 578–592. [Google Scholar] [CrossRef] [PubMed]
- Pérez, C.A.; Carral, J.M.C.; Costas, A.Á.; Martínez, S.V.; Martínez-Lemos, R.I. Water-Based Exercise for Adults with Down Syndrome: Findings from a Preliminary Study. Int. J. Ther. Rehabil. 2017, 25, 20–28. [Google Scholar] [CrossRef]
- Snapp, E.; Martin, J.; Ketcheson, L.; Centeio, E. Enhancing Quality of Life for Children with Intellectual and Developmental Disabilities. Int. J. Disabil. Sports Health Sci. 2020, 3, 33–41. [Google Scholar] [CrossRef]
- Shields, N.; Taylor, N.F. The Feasibility of a Physical Activity Program for Young Adults with Down Syndrome: A Phase II Randomised Controlled Trial. J. Intellect. Dev. Disabil. 2015, 40, 115–125. [Google Scholar] [CrossRef]
- Tomaszewski, B.; Savage, M.N.; Hume, K. Examining Physical Activity and Quality of Life in Adults with Autism Spectrum Disorder and Intellectual Disability. J. Intellect. Disabil. 2022, 26, 1075–1088. [Google Scholar] [CrossRef]
- Ganesh, S.; Mishra, C. Physical Activity and Quality of Life among Adults with Paraplegia in Odisha, India. Sultan Qaboos Univ. Med. J. 2016, 16, e54–e61. [Google Scholar] [CrossRef] [PubMed]
- Laferrier, J.Z.; Teodorski, E.; Cooper, R.A. Investigation of the Impact of Sports, Exercise, and Recreation Participation on Psychosocial Outcomes in a Population of Veterans with Disabilities: A Cross-Sectional Study. Am. J. Phys. Med. Rehabil. 2015, 94, 1026–1034. [Google Scholar] [CrossRef] [PubMed]
- Windle, G.; Hughes, D.; Linck, P.; Russell, I.; Woods, B. Is Exercise Effective in Promoting Mental Well-Being in Older Age? A Systematic Review. Aging Ment. Health 2010, 14, 652–669. [Google Scholar] [CrossRef]
- Borland, R.L.; Hu, N.; Tonge, B.; Einfeld, S.; Gray, K.M. Participation in Sport and Physical Activity in Adults with Intellectual Disabilities. J. Intellect. Disabil. Res. 2020, 64, 908–922. [Google Scholar] [CrossRef]
- Hassmén, P.; Koivula, N.; Uutela, A. Physical Exercise and Psychological Well-Being: A Population Study in Finland. Prev. Med. 2000, 30, 17–25. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Studies | Aims | Participants | Duration/Frequency | Exercise/Intensity | Measurements | Results | Methodology Quality |
|---|---|---|---|---|---|---|---|
| Barnet-Lopez et al. [38], Spain, Europe | To analyze changes in the emotional well-being of adults with IDD after 26 sessions of dance/movement therapy. | N = 42 (male = 24; female = 18); 19–66 years old; moderate to severe IDD. Convenience sample. Randomized groups: EG (N = 22) and CG (N = 20). No sample size calculation. | 3 months; 2× a week; 60 min/session. | Session phases: check-in, warm-up, transition-process and check out. Components and elements of the activities: body scheme, rhythms, self-concept, relationship, identification of the different types of emotions, Laban effort, balance and coordination, grounding and free dance. | Emotional well-being—Human Figure Drawing Test (HFD) | Experimental group (pre vs. post intervention): 5.55 ± 3.648 vs. 4.05 ± 3.258. Control group (pre vs. post intervention): 4.30 ± 0.669 vs. 4.50 ± 0.686. Significant differences between pre-test and post-test for the EG (p = 0.007) and no significant differences for the CG (p = 0.560). The emotional indicators are reduced in 13 participants from the EG, while in the CG, there were only 6 participants with reduced emotional indicators. Five emotional items increased their frequency after the program and fourteen emotional items decreased their frequency after the program, showing improvement. | Fair |
| Bowers et al. [39], Irland, Europe | To examine the experiences and perspectives of people with IDD, their families and staff who work with them about the Special Olympics on the island of Ireland. | N = 47 (no reference to sex); 15 athletes; 11 family members of athletes; 6 non-athletes; 7 family members of non-athletes and 8 staff members. No sample size calculation. | Not applicable | Not applicable | Focus group interviews; individual semi-structured telephone interviews; supplementary qualitative data extracted from four open ended questions contained in a quantitative survey used within the SOPHIE study. | For the athletes: benefits to physical health and well-being; the possibility of connecting socially; have a sense of purpose and belonging; they claim that the selection process is a barrier to progression. For athletes’ families: the Special Olympics promotes family commitment; community social networks; provided opportunities to witness their achievements and be proud; To promote participation in the Special Olympics: better information about the Special Olympics. | Poor |
| Carbó-Carreté et al. [40], Spain, Europe | To analyze the relationship between the practice of PA and the QoL of people with IDD. | N = 529 (male = 296; female = 233); 16-66 years old; borderline, mild, moderate and severe IDD. Convenience sample; no sample size calculation. | Not applicable | Not applicable | QoL—Personal Outcomes Scale–Spanish Adaptation; | The value obtained in the structural equation model (β11 = 0.703, p < 0.001) allows the authors to confirm that the levels of PA have an impact on the QoL of people with IDD. Thus, the data confirmed that PA acts as an important predictor of QoL improvement. The results present acceptable coefficients for the eight first-order factors (QoL domains) and for the three second-order factors (Independence, Social Participation and Well-Being). The well-being factor was the one that presented the highest values. A high value was also found in the Independence factor, specifically in the self-determination domain. The lowest value was associated with the Social Participation factor, in the domain of social inclusion, although this was considered a significant result. | Poor |
| Carmeli et al. [6], Israel, Asia | To understand whether there is a positive relationship between the perception of well-being and physical exercise among adults with IDD. | N = 60 (male = 14; female = 46); 46–77 years old. Mild IDD. Non-randomly selected sample; non-randomized groups: EG (N = 31) and CG (N = 29). No sample size calculation. | 10 months; 3x a week; 40-45 min/session. | Warming-up movements; large body movements in sitting and standing for stability and flexibility; dynamic balance exercises; general strength training (light hand weights and elastic bands). | Self-perceived well-being—Harter’s Self-Perception Profile Modified; Health and QoL—Nottingham Health Profile (NHP). | Higher change in self-perception of well-being assessed by the NHP for the EG. After the intervention program, significant differences were found for the EG in the following NHP domains: energy (p = 0.001), social isolation (p = 0.001) and physical mobility (p = 0.001). The authors observed significant differences in the mean NHP questionnaire score between the initial assessment and the final assessment in the EG. Through an analysis of variance, the authors found a significant difference between the groups in the specific domains of social acceptance (F = 8.79) and physical appearance (F = 3.15). | Fair |
| Carmeli et al. [16], Israel, Asia | To analyze the effect of a physical exercise program on balance, strength and general well-being in adults with IDD. | N = 22 (male = 7; female = 15); 54–66 years old; mild IDD. Non-randomly selected sample, divided into two groups qualitatively and quantitatively: general group A (n = 10: 7 = female; 3 = male) and group B (n = 12; 8 = female; 4 = male). No sample size calculation. | 6 months; 3× a week; 40–45 min/session. | Balance-training program (group A): warming up movements; dynamic balance exercises (i.e., toe-to-heel walk, tandem standing, side walking, dance, roll a ball, push, pull, catching and throwing). Muscle strengthening program (group A): in each session seven basic exercises were used (knee extension, knee flexion, ankle plantar flexion, hip extension, hip abduction, trunk flexion and trunk extension); 1–2 sets; 8–10 repetitions; resting period of 2–4 min between sets; 5–10 min to complete each muscle group. General exercise program (group B): warming-up movements; large body movements in sitting, standing and walking for general mobility, stability and flexibility. | Well-being questionnaire—the authors modified the Harter’s self-perception profile (Aasland and Diseth, 1999). | Both groups showed improvements in self-concept of well-being. Group A (pre training vs. post training): 68 ± 7 vs. 83 ± 9, p = 0.05. Group B (pre training vs. post training): 67 ± 8 vs. 85 ± 8, p = 0.05. | Fair |
| Crawford et al. [18], United Kingdom, Europe | To compare the impact of sports on the psychosocial behavior of people with IDD who (1) are Special Olympics athletes, (2) do not practice any type of sport and (3) practice physical exercise or sports, but not through the Special Olympics. | N = 101 (male = 57; female = 44); 18–67 years old. Special Olympics group n = 51 Mencap Sport group n = 20 Mencap No Sport group n = 30 Missing data for eight participants reduced the total sample for statistical analyses to 93. Power calculations were performed to establish appropriate sample sizes (calculations suggested a sample size of 40 in each group). | Not applicable | Not applicable | QoL—The Life Experiences Checklist (LEC); | The Special Olympics group reported differences between the groups on total scores of LEC (Special Olympics: 23.4 ± 3.7; Mencap Sport: 21.0 ± 3.5; Mencap no Sport: 21.2 ± 3.7; Group Comparison: x²(2, 101) = 10.1; p = 0.006), but also in the leisure and relationships subscales. No differences were found between the groups regarding the “opportunities” subscale. | Poor |
| Diz et al. [15]. Portugal, Europe | To analyze the effect of a regular PA program on the adaptive skills, motor competences, and QoL of institutionalized adults with IDD. | N = 16 (male = 7; female = 9); 24–61 years old; mild to moderate IDD. Convenience sample. Randomized groups: EG (N = 8) and CG (N = 8). No sample size calculation. | 20 weeks; 2× a week; 50 min/session. | Active warm-up, core activities and stretching. PA program included rhythmic exercises, muscle strength and amplitude, spatial orientation, balance, body awareness, attention and memory. | QoL—Portuguese version of the Personal Outcomes Scale (P_POS) | In the last two assessment periods, better scores were recorded in most QoL domains for the EG, with a significant difference recorded between the pre-intervention and post-intervention periods, in the total quality of life score, in the proxy version (pre- vs. post-intervention: 97.75 ± 8.46 vs. 101.750 ± 7.69, p = 0.01, r = 0.32). | Fair |
| Fjellstrom et al. [41], Sweden, Europe | To explore the feasibility and effectiveness of a web-based PA training program for people with IDD. A secondary outcome was to assess enjoyment of the training program and QoL. | N = 22 (male = 12; female = 10); 18–60 years old; mild to moderate IDD. No sample size calculation. | 12 weeks; 3× a week; 50 min/session. | 150 min per week of moderate PA; Combination of strength exercises and resistance exercises length with balance and flexibility. Different progression levels were applied to be able to meet the participants requirements (e.g., the participants could choose between jumping and walking to be able to meet the moderate intensity level). | QoL—Manchester Short Assessment of Quality of Life (MANSA); | The mean scores of the satisfaction items were 5.9 ± 0.92 pre-training and 5.8 ± 0.9 post-training. No significant differences were observed in QoL (p = 0.26 and r = 0.006), except for “leisure activities”, where the score on the post-intervention tests was lower when compared to the score obtained before the intervention (p = 0.046). | Fair |
| Mercado et al. [42], Spain, Europe | To study the benefits of dance as a tool for improving the QoL of people with IDD. | N = 9 (male = 1; female = 8); 22–58 years old; 3 dance teachers, 1 mother, 1 president of an association and 4 persons with IDD. Convenience sample. Level of education: 45% primary, 33% secondary and 22% university studies. | Not applicable | Not applicable | Semi-structured interview: vision and perception of the group’s social inclusion and QoL. | The findings show the benefits and potential of dance regarding different dimensions of QoL and human functioning in IDD persons, like personal development, physical and emotional well-being and interpersonal relationships. The results indicate that dance benefits the QoL of people with IDD. | Poor |
| Moltó and Bruna [17], Spain, Europe | (1) To analyze the practice of sports as a significant activity for people with IDD; (2) to analyze the association of sport with life satisfaction and self-determination; (3) to establish which type of sport is most associated with life satisfaction and self-determination. | N = 74 (male = 49; female = 25); aged 18 or over; mild to moderate IDD. EG (N = 42) and CG (N = 32). No sample size calculation. | Not applicable | Not applicable | Sociodemographic and sports questionnaire (constructed ad hoc for this investigation); satisfaction with life—Satisfaction with Life Scale (SWLS); self-determination—Arc’s Self-Determination Scale. | The three main reasons why the participants participate in sport are as follows: (1) because they enjoy it and find it pleasurable, (2) for health reasons and (3) for the possibility of interacting with other people and making friends. No significant differences (p = 0.37) were found in SWLS between participants who played sports (28.36 ± 5.63) and those who did not (27.91 ± 4.60). Participants who practice team sports are more satisfied with their lives (p = −2.06; r = 0.58) and satisfied with the sporting activity (p = −3.63; r = 1.03). Also, individuals who practice team sports value their living conditions more (p = −2.28 and r = 0.59). | Poor |
| Ozkan and Kale [43], Turkey, Eurasian | To analyze whether there is a difference between the QoL and motor skills of children with IDD who participate in physical education activities for 14 weeks and those who do not. | N = 34 (male = 19; female = 15); 8–12 years old. EG 18 (male = 11; female = 7); CG: 16 (male = 8; female = 8). No sample size calculation. | 14 weeks; 2× a week; 60–70 min/session. | Educational games; 1–8 weeks, basic skills were practiced. In weeks 9–14, the progress of children was considered and practices requiring more rapid movement and coordination were included. | QoL—Pediatric Quality of Life Inventory (PedsQL). | The inventory total score (p = 0.000) and all the other sub-scales of PedsQL of children with IDD who participated in the physical education activities program improved more, with significant differences, than children with IDD who did not participate in the program. | Fair |
| Pérez et al. [44], Spain, Europe | To analyze the potential benefits of an aquatic exercise program on the health-related physical fitness and QoL of a group of adults with DS and identify the impact that the program may have on the self-perception of QoL of parents or caregivers. | N = 14 (male = 7; female = 7); 21–49 years old. Moderate or severe IDD. No sample size calculation. | 12 weeks; 2× a week; 45 min/session. | Warm up (15min): respiration exercises (time: 5 min; sets: 3 reps × 30 s × 2 sets; rest between repetitions: 5–10 s; rest between sets: 1 min; swimming speed: medium); crawl kicks while holding the edge of the pool (time: 5 min; sets: 3 reps × 30 s × 2 sets; rest between repetitions: 10 s; rest between sets: 1 min; swimming speed: medium-high); main part (30 min): crawl stroke (arms movement technique with pull buoy); crawl stroke (legs movement technique) and backstroke (legs movement technique)—time: 10 min; sets: 2 reps × 15 m × 3 sets; rest between repetitions: 10 s–passive rest; rest between sets: 1 min—active rest; swimming speed: high); cool down (5 min). | QoL—short modified version of a Spanish QoL questionnaire (applied to participants- self-report); QoL—World Health Organization Quality of Life-BREF (WHOQOL-BREF) (applied to parents/caregivers). | The authors did not observe significant changes, on the self-report scale, in any of the QoL dimensions assessed in the study, indicating that the exercise program did not have a significant impact on the QoL of the participants (self-esteem and health, test: 2.45 ± 0.74; retest: 2.59± 0.61, p = 0.336; healthy habits, test: 3.39 ± 0.56; retest: 3.14 ± 0.60, p = 0.187; leisure time, test: 2.90 ± 0.82; retest: 3.11 ± 0.57, p = 0.220; and personal satisfaction, test: 3.07 ± 0.54; retest: 3.07 ± 0.61, p = 0.987). The same happened with the perception of QoL of parents and caregivers in relation to the participants (total score, test: 13.53 ± 1.49; retest: 13.65 ± 1.384, p = 0.587). | Fair |
| Snapp et al. [45], USA, North America | To provide evidence regarding the positive impact of interventions based on fundamental motor skills on the QoL of children with IDD. | N = 10 (no reference to sex); 4–14 years old; ASD, speech deficits, DS and fragile syndrome. No sample size calculation. | Three separate 10- week interventions; 1× a week; 1 h/session. | Each session followed the same general routine: 10–15 min of free play, 5 min warm up, 35 min of direct instruction, and 5 min cool down. | The instrument was applied six times, at the beginning and end of each 10-week intervention; QoL—Pediatric Quality of Life Inventory 4.0 (PedsQL); | Emotional function: an increase during the three interventions was observed, with a slight increase between the end of the first and the beginning of the second intervention and a decrease between the end of the second and the beginning of the third intervention. Social function: an increase during the three interventions was observed, with a continuous increase between the end of the first and the beginning of the second intervention and a decrease between interventions two and three. Physical function: a decrease during the first intervention and an increase during the second and third interventions were observed. School function: an increase was noticeable during the second intervention. | Fair |
| Shields et al. [46], Australia, Oceania | To investigate whether a PA program designed according to the Rimmer and Rowland (2008) framework was viable, whether the program was safe, and whether it led to improvements in walking ability, and to assess risk factors associated with chronic diseases and positive changes in participants’ perceptions of well-being and changes in PA. | N = 16 (male = 8; female = 8); 18–35 years old; mild to moderate IDD. Convenience sample. Randomized groups: EG (N = 8) and CG (N = 8). No sample size calculation. | 8 weeks; | 150 min of moderate-intensity PA per week—two 45 min walks per week with a student mentor and another 60 min of PA (independent—without mentor) | Perceptions of well-being—The Life Satisfaction Scale. | There were no significant differences between the groups for perceptions of well-being. Intervention group (pre vs. post): 29.8 ± 7.5 vs. 28.2 ± 7.5. Control group (pre vs. post): 30.6 ± 4.6 vs. 31.3 ± 4.8. Difference between groups (Week 9–Week 0): −2.8 [−9.3, 3.6]. | Good |
| Tomaszewski et al. [47], USA, North America | (1) To describe the average PA for adults with ASD and IDD using PA meters, (2) to describe the QoL of adults with ASD and IDD and (3) to examine the relationship between PA counts steps and QoL. | N = 38 (71.1% male); 18–55 years old. Non-convenience sample. No sample size calculation. | All waking hours for 1 week. | Not applicable | QoL—Quality of Life Questionnaire (QOL-Q) | Satisfaction domain was significantly higher (23.37 ± 2.721) than the domains of competence (18.89 ± 6.75), independence (20.61 ± 3.45) and social belonging (21.28 ± 3.16). The competence domain and the total QoL value were significantly associated with weekly step count (p = 0.004, r = 0.46 and p < 0.001, r = 0.56). The total QoL score was regressed onto average steps per day, nonverbal IQ and age. Average steps per day, nonverbal IQ, and age accounted for 34.2% of the variance in quality of life. For every 1000-step increase in steps per day, the total QoL score increases by 2.56 points. | Poor |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Diz, S.; Jacinto, M.; Costa, A.M.; Monteiro, D.; Matos, R.; Antunes, R. Physical Activity, Quality of Live and Well-Being in Individuals with Intellectual and Developmental Disability. Healthcare 2024, 12, 654. https://doi.org/10.3390/healthcare12060654
Diz S, Jacinto M, Costa AM, Monteiro D, Matos R, Antunes R. Physical Activity, Quality of Live and Well-Being in Individuals with Intellectual and Developmental Disability. Healthcare. 2024; 12(6):654. https://doi.org/10.3390/healthcare12060654
Chicago/Turabian StyleDiz, Susana, Miguel Jacinto, Aldo M. Costa, Diogo Monteiro, Rui Matos, and Raul Antunes. 2024. "Physical Activity, Quality of Live and Well-Being in Individuals with Intellectual and Developmental Disability" Healthcare 12, no. 6: 654. https://doi.org/10.3390/healthcare12060654
APA StyleDiz, S., Jacinto, M., Costa, A. M., Monteiro, D., Matos, R., & Antunes, R. (2024). Physical Activity, Quality of Live and Well-Being in Individuals with Intellectual and Developmental Disability. Healthcare, 12(6), 654. https://doi.org/10.3390/healthcare12060654