
Impact of Hypnotherapy on Fear, Pain, and the Birth Experience: A Systematic Review

 ,
,  ,
,
Abstract
1. Introduction
2. Methodology
2.1. Review Protocol
2.2. Eligibility Criteria
2.3. Information Sources
2.4. Structured Language
2.5. Search Strategy
2.6. Data Extraction Process
2.7. Data Collection Process and Collected Data
2.8. Risk of Bias in Individual Studies
2.9. Summary of Results
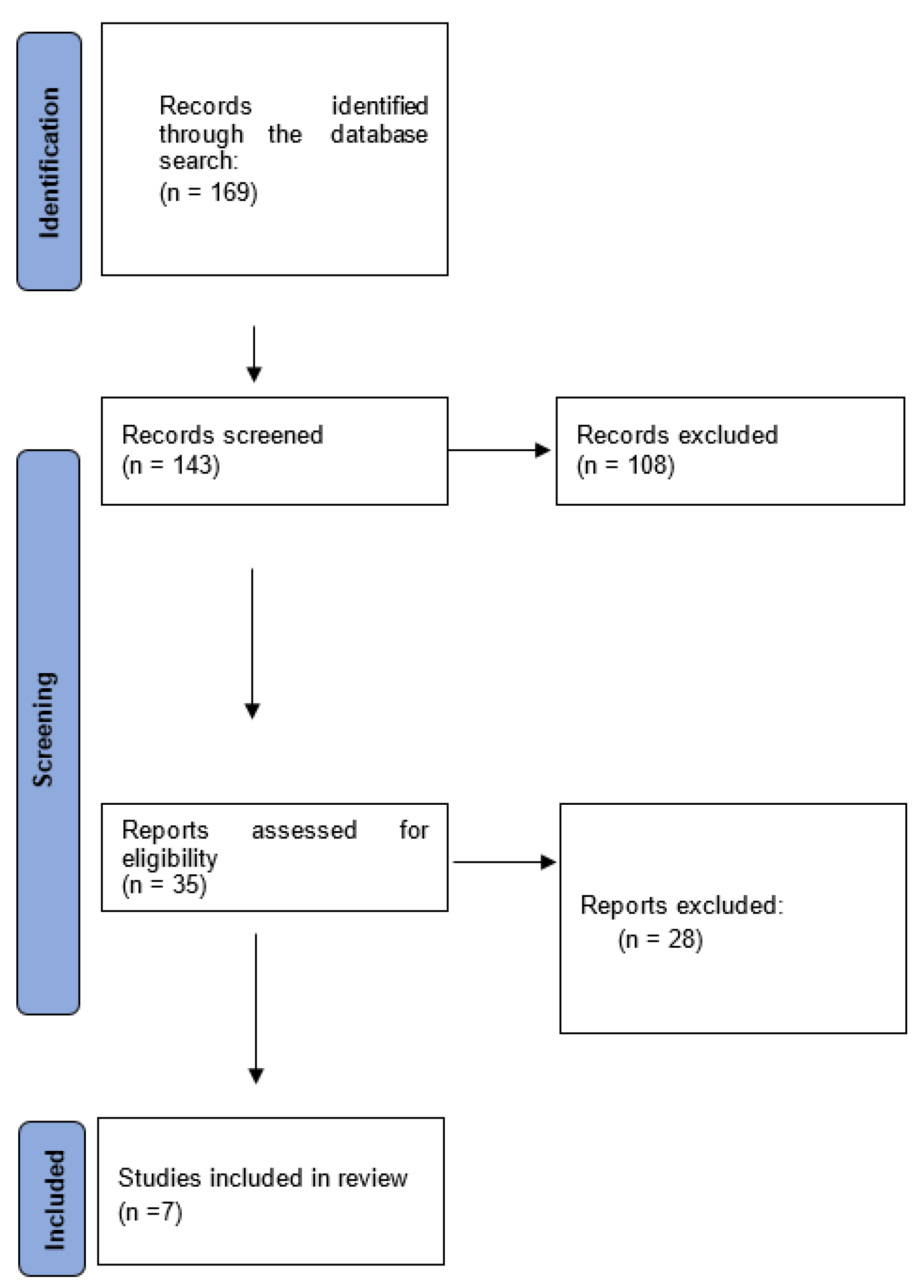
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Vasra, E.; Murdiningsih; Astuty, R.D.; Novita, N. Modeling of Gentle Birth and Hypnoprenatal Integrated Antenatal Class on Birth Process in Puskesmas and Midwives Practice, Palembang City. Pak. J. Med. Health Sci. 2020, 14, 1437–1441. [Google Scholar]
- Badaoui, A.; Kassm, S.A.; Naja, W. Fear and Anxiety Disorders Related to Childbirth: Epidemiological and Therapeutic Issues. Curr. Psychiatry Rep. 2019, 21, 27. [Google Scholar] [CrossRef]
- Soysal, C.; Yilmaz, E. Antenatal Hypnosis: Does it Have an Effect on Fear of Childbirth? Eurasian J. Med. Investig. 2022, 6, 394–400. [Google Scholar]
- Bonapace, J.; Gagné, G.P.; Chaillet, N.; Gagnon, R.; Hébert, E.; Buckley, S. No. 355-Physiologic Basis of Pain in Labour and Delivery: An Evidence-Based Approach to its Management. J. Obstet. Gynaecol. Can. 2018, 40, 227–245. [Google Scholar] [CrossRef]
- Nursanti, R.; Eprila; Taswin, M. Experiences of Pregnant Women in Overcoming Anxiety Facing the Childbirth Process by Attending Hypno Prenatal Class. Pak. J. Med. Health Sci. 2020, 14, 1447–1450. [Google Scholar]
- McAllister, S.; Coxon, K.; Murrells, T.; Sandall, J. Healthcare professionals’ attitudes, knowledge and self-efficacy levels regarding the use of self-hypnosis in childbirth: A prospective questionnaire survey. Midwifery 2017, 47, 8–14. [Google Scholar] [CrossRef]
- Gueguen, J.; Huas, C.; Orri, M.; Falissard, B. Hypnosis for labour and childbirth: A meta-integration of qualitative and quantitative studies. Complement. Ther. Clin. Pract. 2021, 43, 101380. [Google Scholar] [CrossRef]
- Beebe, K.R. Hypnotherapy for Labor and Birth. Nurs. Womens Health 2014, 18, 48–59. [Google Scholar] [CrossRef]
- Waisblat, V.; Langholz, B.; Bernard, F.J.; Arnould, M.; Benassi, A.; Ginsbourger, F.; Guillou, N.; Hamelin, K.; Houssel, P.; Hugot, P.; et al. Impact of a Hypnotically-Based Intervention on Pain and Fear in Women Undergoing Labor. Int. J. Clin. Exp. Hypn. 2017, 65, 64–85. [Google Scholar] [CrossRef]
- Palsson, O.S.; Kekecs, Z.; De Benedittis, G.; Moss, D.; Elkins, G.R.; Terhune, D.B.; Varga, K.; Shenefelt, P.D.; Whorwell, P.J. Current Practices, Experiences, and Views in Clinical Hypnosis: Findings of an International Survey. Int. J. Clin. Exp. Hypn. 2023, 71, 92–114. [Google Scholar] [CrossRef]
- Farnham, T. Reviewing pain management options for patients in active labor. Nursing 2020, 50, 25–30. [Google Scholar] [CrossRef]
- Catsaros, S.; Wendland, J. Psychological impact of hypnosis for pregnancy and childbirth: A systematic review. Complement. Ther. Clin. Pract. 2023, 50, 101713. [Google Scholar] [CrossRef]
- Dick-Read, G. Childbirth without Fear; Pollinger in Print: London, UK, 2006; pp. 1–577. [Google Scholar]
- Spicer, R. My body, my birth, my baby: The experience of childbirth for first-time mothers who have undertaken traditional antenatal education and those who have included hypnosis. Aust. J. Clin. Hypnother. Hypn. 2014, 36, 15–31. [Google Scholar]
- Mongan, M. Hipnonaissance la Méthode Mongan; Éditions Leduc: Paris, France, 2014; pp. 1–317. [Google Scholar]
- Lanfranco, R.C.; Canales-Johnson, A.; Huepe, D. Hypnoanalgesia and the study of pain experience: From Cajal to modern neuroscience. Front. Psychol. 2014, 5, 1126. [Google Scholar] [CrossRef]
- Atis, F.Y.; Rathfisch, G. The effect of hypnobirthing training given in the antenatal period on birth pain and fear. Complement. Ther. Clin. Pract. 2018, 33, 77–84. [Google Scholar] [CrossRef]
- Werner, A.; Uldbjerg, N.; Zachariae, R.; Nohr, E.A. Effect of self-hypnosis on duration of labor and maternal and neonatal outcomes: A randomized controlled trial. Acta Obstet. Gynecol. Scand. 2013, 92, 737–873. [Google Scholar] [CrossRef]
- Werner, A.; Uldbjerg, N.; Zachariae, R.; Wu, C.S.; Nohr, E.A. Antenatal Hypnosis Training and Childbirth Experience: A Randomized Controlled Trial. Birth 2013, 40, 272–280. [Google Scholar] [CrossRef]
- Cyna, A.; Crowther, C.; Robinson, J.; Andrew, M.; Antoniou, G.; Baghurst, P. Hypnosis Antenatal Training for Childbirth: A randomised controlled trial. BJOG Int. J. Obstet. Gynaecol. 2013, 120, 1248–1259. [Google Scholar] [CrossRef]
- Werner, A.; Uldbjerg, N.; Zachariae, R.; Rosen, G.; Nohr, E. Self-hypnosis for coping with labour pain: A randomised controlled trial. BJOG Int. J. Obstet. Gynaecol. 2013, 120, 346–353. [Google Scholar] [CrossRef]
- Finlayson, K.; Downe, S.; Hinder, S.; Carr, H.; Spiby, H.; Whorwell, P. Unexpected consequences: Women’s experiences of a self-hypnosis intervention to help with pain relief during labour. BMC Pregnancy Childbirth 2015, 15, 229. [Google Scholar] [CrossRef]
- Downe, S.; Finlayson, K.; Melvin, C.; Spiby, H.; Ali, S.; Diggle, P.; Gyte, G.; Hinder, S.; Miller, V.; Slade, P.; et al. Self-hypnosis for intrapartum pain management in pregnant nulliparous women: A randomised controlled trial of clinical effectiveness. BJOG Int. J. Obstet. Gynaecol 2015, 122, 1151–1276. [Google Scholar] [CrossRef]
- Beevi, Z.; Low, W.Y.; Hassan, J. The Effectiveness of Hypnosis Intervention for Labor: An Experimental Study. Am. J. Clin. Hypn. 2017, 60, 172–191. [Google Scholar] [CrossRef]


{kind=link}
| Database | Search String |
|---|---|
| SCOPUS | ((TITLE-ABS-KEY (hypnosis) OR TITLE-ABS-KEY (“hypnotism” OR “hypnoanalysis” OR “hypnotherapy” OR “hypnotherapies” OR “mesmerism”))) AND ((TITLE-ABS-KEY (parturition) OR TITLE-ABS-KEY (“parturitions” OR “birth” OR “births” OR “childbirth” OR “childbirths”))) |
| PUBMED | Search: ((hypnosis[MeSH Terms]) OR (“hypnotism”[Title/Abstract] OR “hypnoanalysis”[Title/Abstract] OR “hypnotherapy”[Title/Abstract] OR “hypnotherapies”[Title/Abstract] OR “mesmerism”[Title/Abstract]) AND ((y_10[Filter]) AND (clinicaltrial[Filter]))) AND ((parturition[MeSH Terms]) OR (“parturitions”[Title/Abstract] OR “birth”[Title/Abstract] OR “births”[Title/Abstract] OR “childbirth”[Title/Abstract] OR “childbirths”[Title/Abstract]) |
| CINAHL | (MH “Hypnosis+”) AND (MH “Labor+”) |
| WOS | (TS=(hypnosis)) OR TS=(“hypnotism” OR “hypnoanalysis” OR “hypnotherapy” OR “hypnotherapies” OR “mesmerism”) AND (TS=(parturition)) OR TS=(“parturitions” OR “birth” OR “births” OR “childbirth” OR “childbirths”) |
| ARTICLE | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | TOTAL | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Atis y Rathfish, 2018 [17] | YES | YES | YES | YES | ¿? | ¿? | YES | ¿? | YES | YES | 7 | |
| Werner et al., 2013 [18] | YES | YES | YES | YES | YES | ¿? | YES | ¿? | YES | YES | 8 | |
| Werner et al., 2013 [19] | YES | YES | YES | YES | YES | ¿? | YES | ¿? | YES | YES | 8 | |
| Cyna et al., 2013 [20] | YES | YES | ¿? | YES | YES | YES | YES | YES | YES | YES | 9 | |
| Werner et al., 2013 [21] | YES | YES | YES | YES | YES | ¿? | YES | YES | YES | YES | 9 | |
| Finlayson et al., 2015 [22] | YES | YES | YES | NO | NO | SI | YES | ¿? | YES | YES | 7 | |
| Downe et al., 2015 [23] | YES | YES | YES | NO | NO | SI | YES | ¿? | YES | YES | 7 | |
| AVERAGE | 7857 |
| STUDY | PARTICIPANTS | INTERVENTION | COMPARISON | OUTCOME |
|---|---|---|---|---|
| Atis and Rathfish, 2018 [17] | Turkey. 60 participants. Experimental group (n = 30)|control group (n = 30) | Pregnant, primiparous, 20–36 weeks gestation, candidates for vaginal delivery, no prior illnesses, single fetus. | Experimental group: 3 h theoretical teaching weekly for 4 weeks. Control group: standard care. Second phase: experimental group—support in breathing, relaxation, imagination, and exercises. Control group: standard care. | Identify the effect of hypnobirthing training during pregnancy on fear and pain in childbirth. Women in the hypnobirthing group reported lower pain and fear during childbirth. They experienced calmness, relaxation, and better control. Shorter durations in the second and third stages of labor. Experimental group women initiated early breastfeeding. No differences in neonatal outcomes or Apgar scores. |
| Werner et al., 2013 [18] | Denmark. 1222 participants. Intervention group (n = 497)|active comparison group (n = 495)|control group (n = 230) | Nulliparous women, >18 years, Danish speakers, uncomplicated pregnancy, no chronic diseases, 27–30 weeks gestation. | Intervention group: 1 h self-hypnosis per week for three consecutive weeks. Active comparison group: Three 1 h prenatal classes on body awareness, relaxation, and mindfulness. Control group: standard prenatal care. | Examine the effect of a brief self-hypnosis course on labor duration and other outcomes. The self-hypnosis course had no effect on labor duration, mode of delivery, interventions, neonatal outcomes, or breastfeeding success. No reported adverse effects. |
| Werner et al., 2013 [21] | Denmark | Estimate epidural analgesia use and pain experienced during childbirth after a brief course in self-hypnosis. | No differences in epidural use. No statistically significant differences in self-reported pain measures. Fewer scheduled cesareans in the hypnosis group; more emergency cesareans. No significant differences in types of delivery. | There were no differences between the groups in the use of epidural analgesia. No statistically significant differences were observed among the three groups for any of the self-reported pain measures. The number of scheduled cesarean sections was lower in the hypnosis group, and the number of emergency cesarean sections was higher in this group. There were no significant differences between the types of delivery. |
| Werner et al., 2013 [19] | Denmark | Study the effect of hypnosis on the birth experience (secondary pre-specified outcome). | Women in the hypnosis group reported a better birth experience compared to the other groups. A brief self-hypnosis course improved women’s birth experiences. | Women in the hypnosis group experienced their childbirth better compared to the other two groups (average W-DEQ score of 42.9 in the hypnosis group, 47.2 in the relaxation group, and 47.5 in the usual care group (p = 0.01)).
|
| Cyna et al., 2013 [20] | Australia. 448 women. Hypnosis + CD group (n = 154)| CD-only group (n = 143)|control group (n = 151) | Pregnant, 34–39 weeks gestation, candidates for vaginal delivery, cephalic presentation, single fetus. | Hypnosis + CD (guided by a hypnotherapist): three live prenatal hypnosis sessions plus corresponding audio CDs. CD only (administered by nurses): used the same CD as the hypnosis + CD group, but without hypnosis training. Control group: standard prenatal care, no additional CD. | Determine the use of pharmacological analgesia during childbirth when prenatal hypnosis is added to standard care. No differences in pharmacological analgesia use, epidural use, perceived pain, or satisfaction with the birth experience. No differences in secondary outcomes. Hypnosis group reported increased prostaglandin use for induction. No differences in high-dependency unit admission, episiotomy, blood transfusion, or post-birth hospital stay. Similar rates of exclusive breastfeeding at discharge, but more control group women exclusively breastfeeding at 6 weeks. |
| Downe et al., 2015 [23] | United Kingdom. 678 participants. Self-hypnosis group (n = 343)|control group (n = 335) | Nulliparous women, no planned elective cesarean, no hypertension medication, no mental illness, >18 years. | Self-hypnosis group: two 1.5 h training sessions between 32 and 35 weeks gestation, daily self-hypnosis CDs. Control group: standard prenatal care. | Establish the effect of prenatal group self-hypnosis on epidural use during childbirth. Secondary outcomes: clinical and psychological results, cost analysis. No statistically significant difference in epidural use or secondary outcomes. No difference in pain experience. Intervention group women had lower actual levels of fear and anxiety than anticipated. |
| Finlayson et al., 2015 [22] | United Kingdom. Self-hypnosis group (n = 343)|control group (n = 335) | Pregnant women, >18 years | Self-hypnosis group: two 1.5 h training sessions between 32 and 35 weeks gestation, daily self-hypnosis CDs. Control group: standard prenatal care. | Explore the views and experiences of women receiving a prenatal self-hypnosis training program for labor pain relief. Most respondents reported positive experiences with self-hypnosis, feeling calm, confident, and empowered. They found the intervention beneficial and used innovative strategies to personalize their self-hypnosis practice. Occasionally, frustration or disappointment was reported when midwives misinterpreted their relaxed state during admission or when labor experiences did not match expectations. The focused relaxation state experienced by women using the technique should be acknowledged by providers if the intervention is to be implemented in maternity services. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernández-Gamero, L.; Reinoso-Cobo, A.; Ruiz-González, M.d.C.; Cortés-Martín, J.; Muñóz Sánchez, I.; Mellado-García, E.; Piqueras-Sola, B. Impact of Hypnotherapy on Fear, Pain, and the Birth Experience: A Systematic Review. Healthcare 2024, 12, 616. https://doi.org/10.3390/healthcare12060616
Fernández-Gamero L, Reinoso-Cobo A, Ruiz-González MdC, Cortés-Martín J, Muñóz Sánchez I, Mellado-García E, Piqueras-Sola B. Impact of Hypnotherapy on Fear, Pain, and the Birth Experience: A Systematic Review. Healthcare. 2024; 12(6):616. https://doi.org/10.3390/healthcare12060616
Chicago/Turabian StyleFernández-Gamero, Laura, Andrés Reinoso-Cobo, María del Carmen Ruiz-González, Jonathan Cortés-Martín, Inmaculada Muñóz Sánchez, Elena Mellado-García, and Beatriz Piqueras-Sola. 2024. "Impact of Hypnotherapy on Fear, Pain, and the Birth Experience: A Systematic Review" Healthcare 12, no. 6: 616. https://doi.org/10.3390/healthcare12060616
APA StyleFernández-Gamero, L., Reinoso-Cobo, A., Ruiz-González, M. d. C., Cortés-Martín, J., Muñóz Sánchez, I., Mellado-García, E., & Piqueras-Sola, B. (2024). Impact of Hypnotherapy on Fear, Pain, and the Birth Experience: A Systematic Review. Healthcare, 12(6), 616. https://doi.org/10.3390/healthcare12060616