

Dementia Education for Workforce Excellence: Evaluation of a Novel Bichronous Approach

Abstract
1. Introduction
1.1. The Intervention
1.2. Participants in DEWE
1.3. Aim and Objectives
- To explore participants’ perceptions on the content and quality of the dementia training.
- To explore participants’ perceptions and experiences of accessing the dementia training using a bichronous approach.
2. Materials and Methods
2.1. Sampling and Recruitment
2.2. Data Collection
2.3. Data Analysis
3. Results: Survey Findings
3.1. Demographics
3.2. Experience of Dementia Care and Education
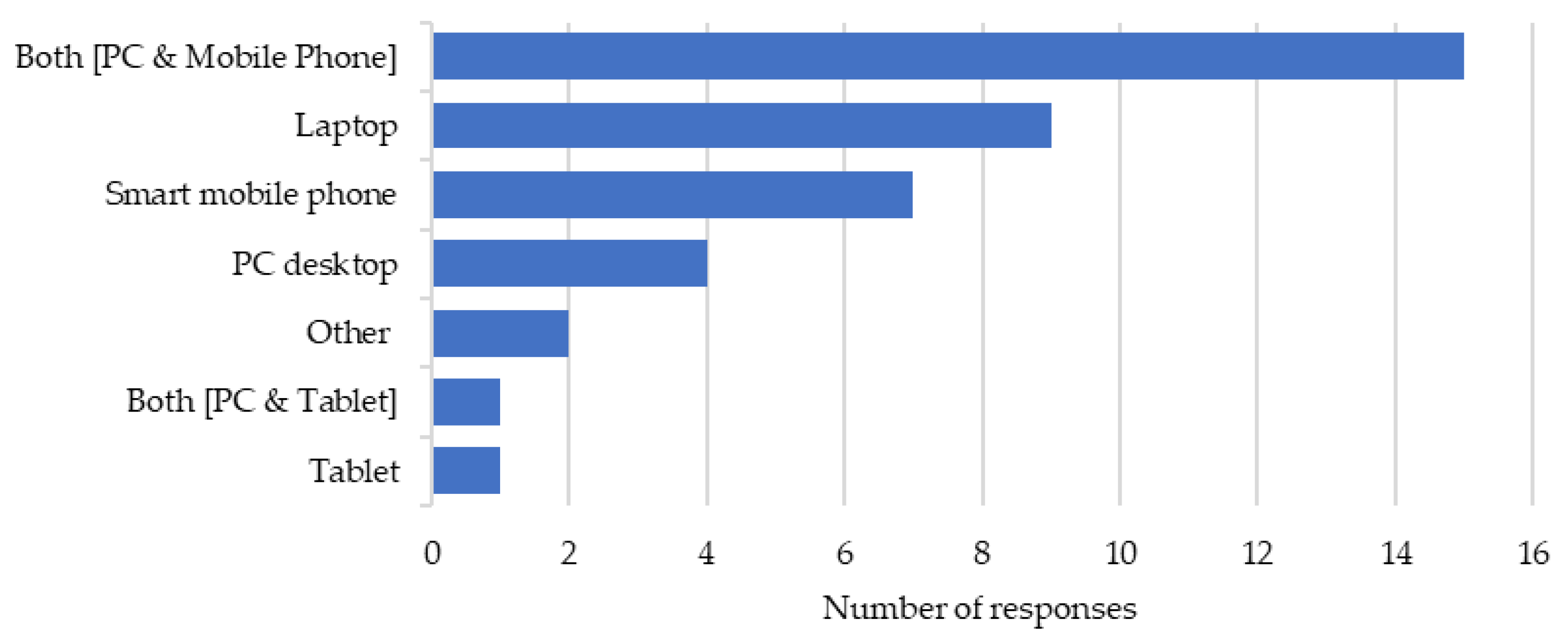
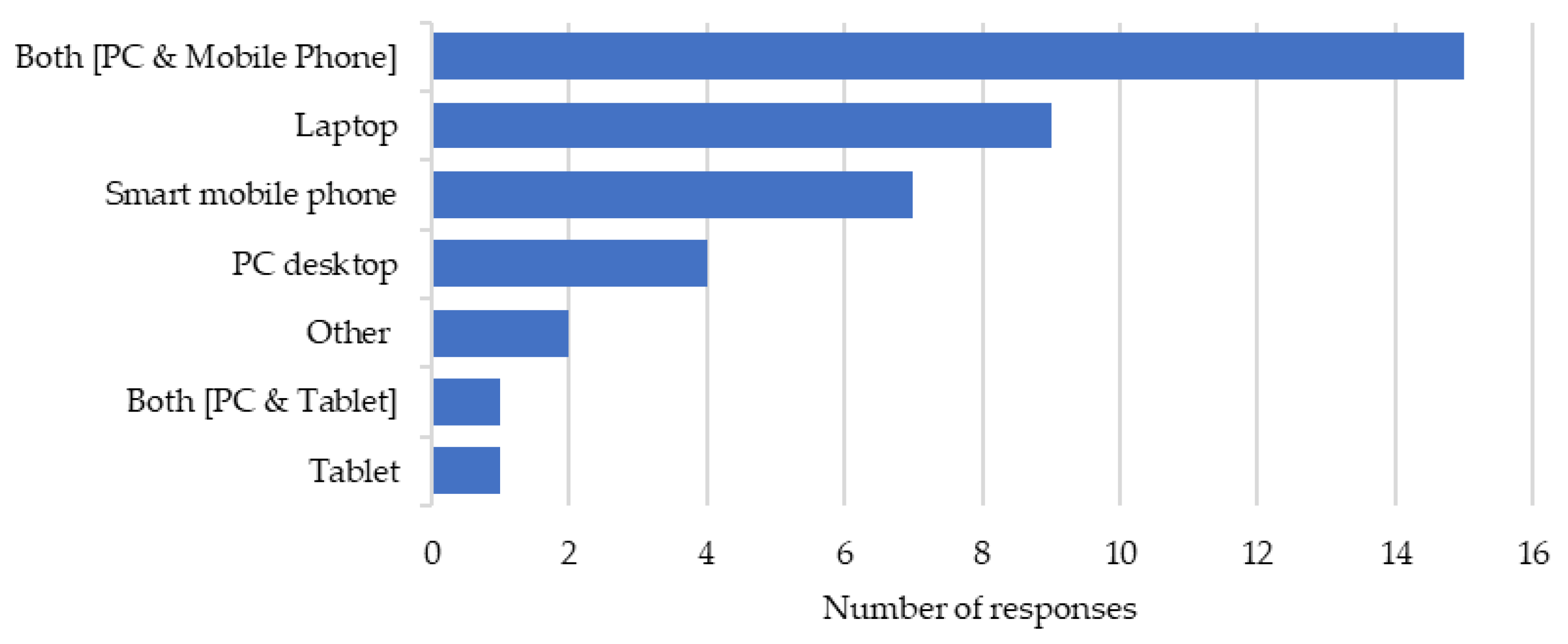
3.3. Access to DEWE
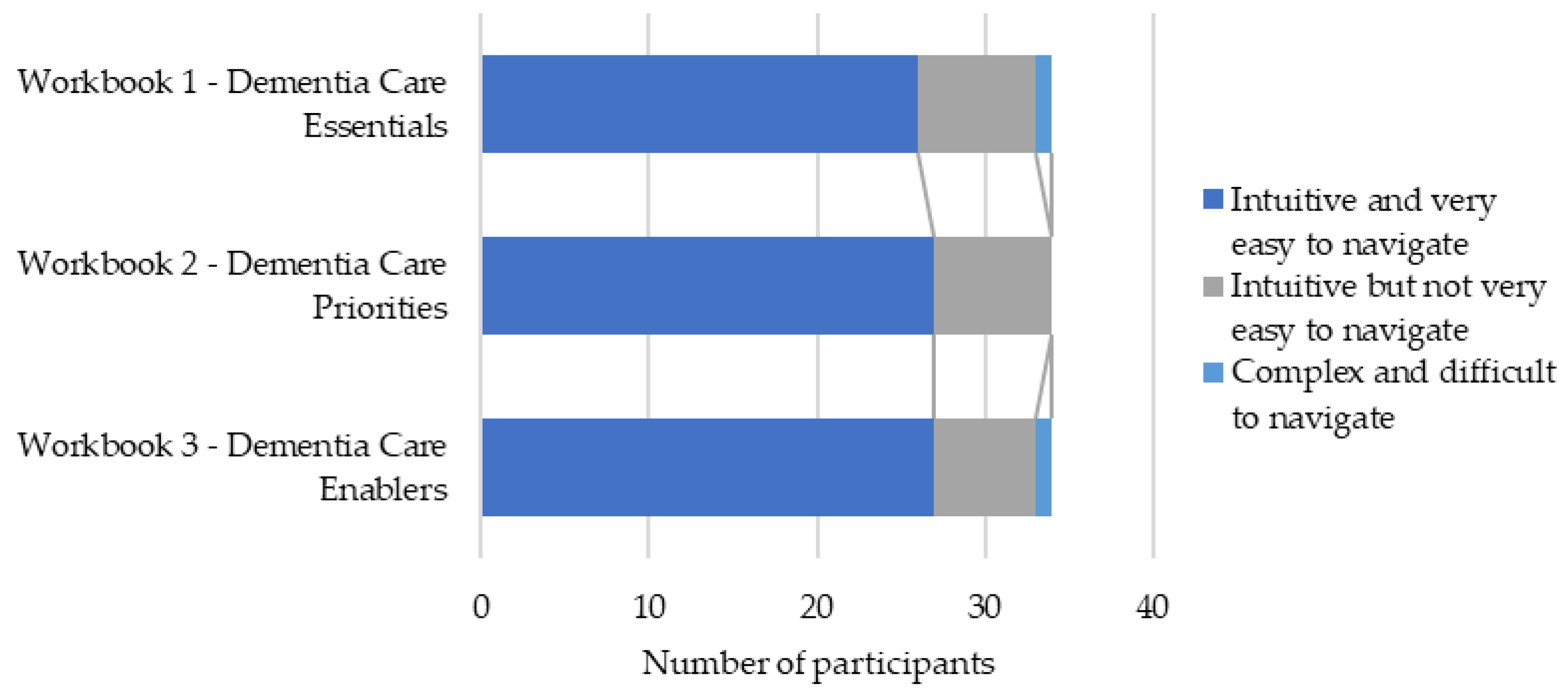
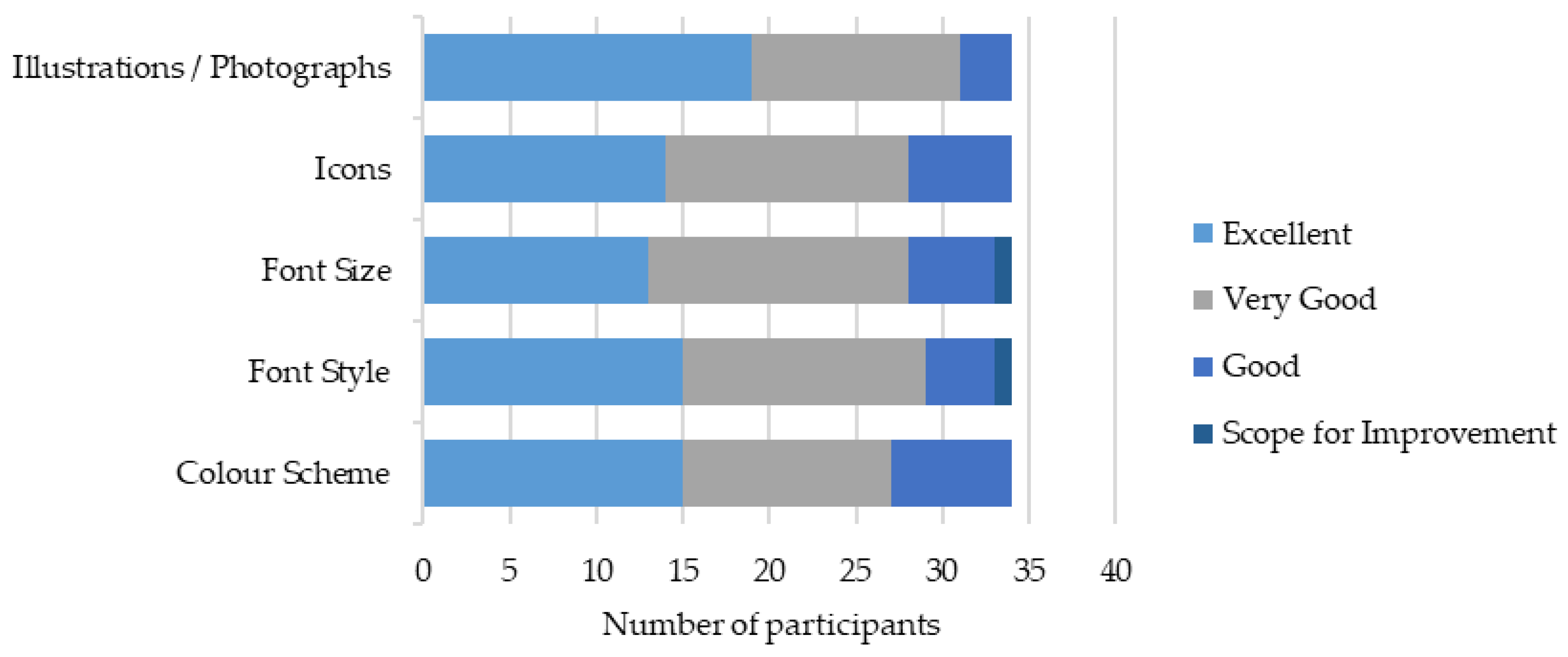
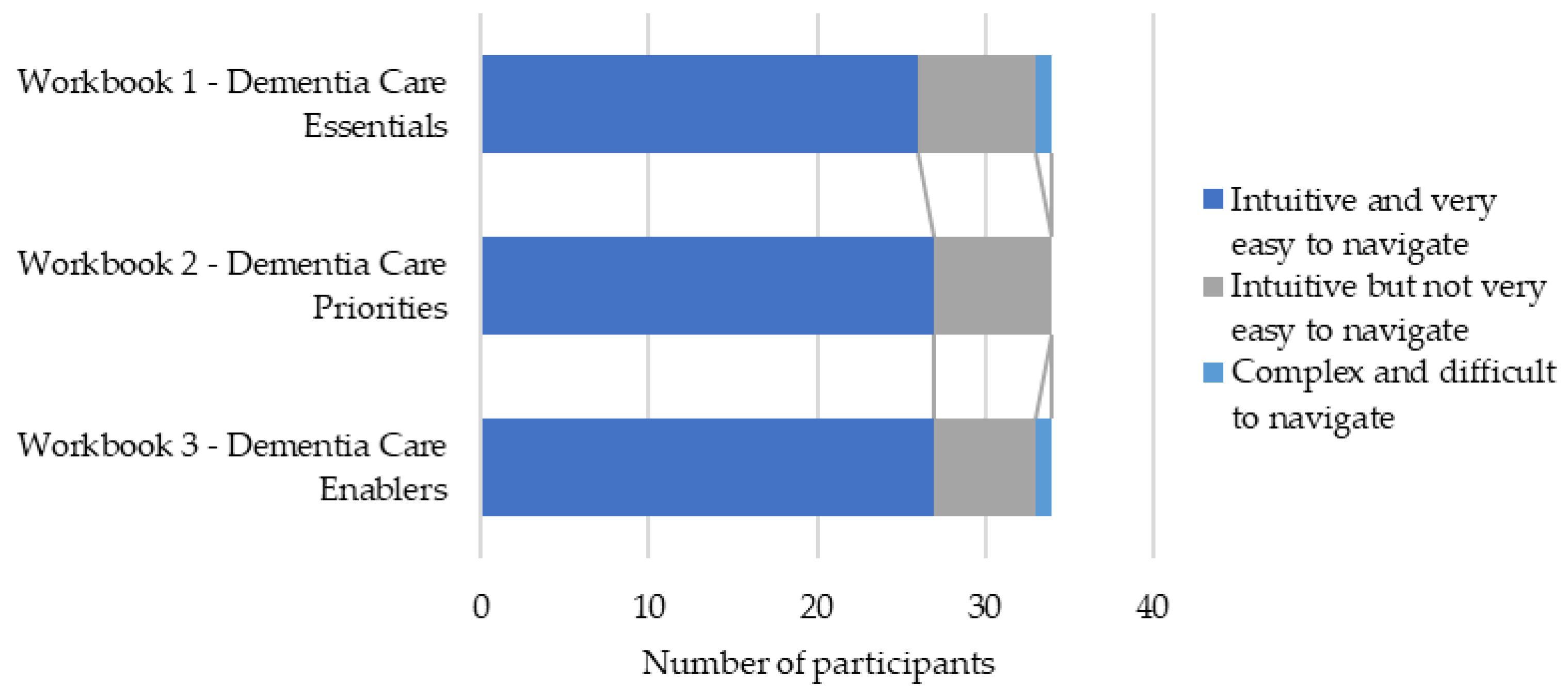
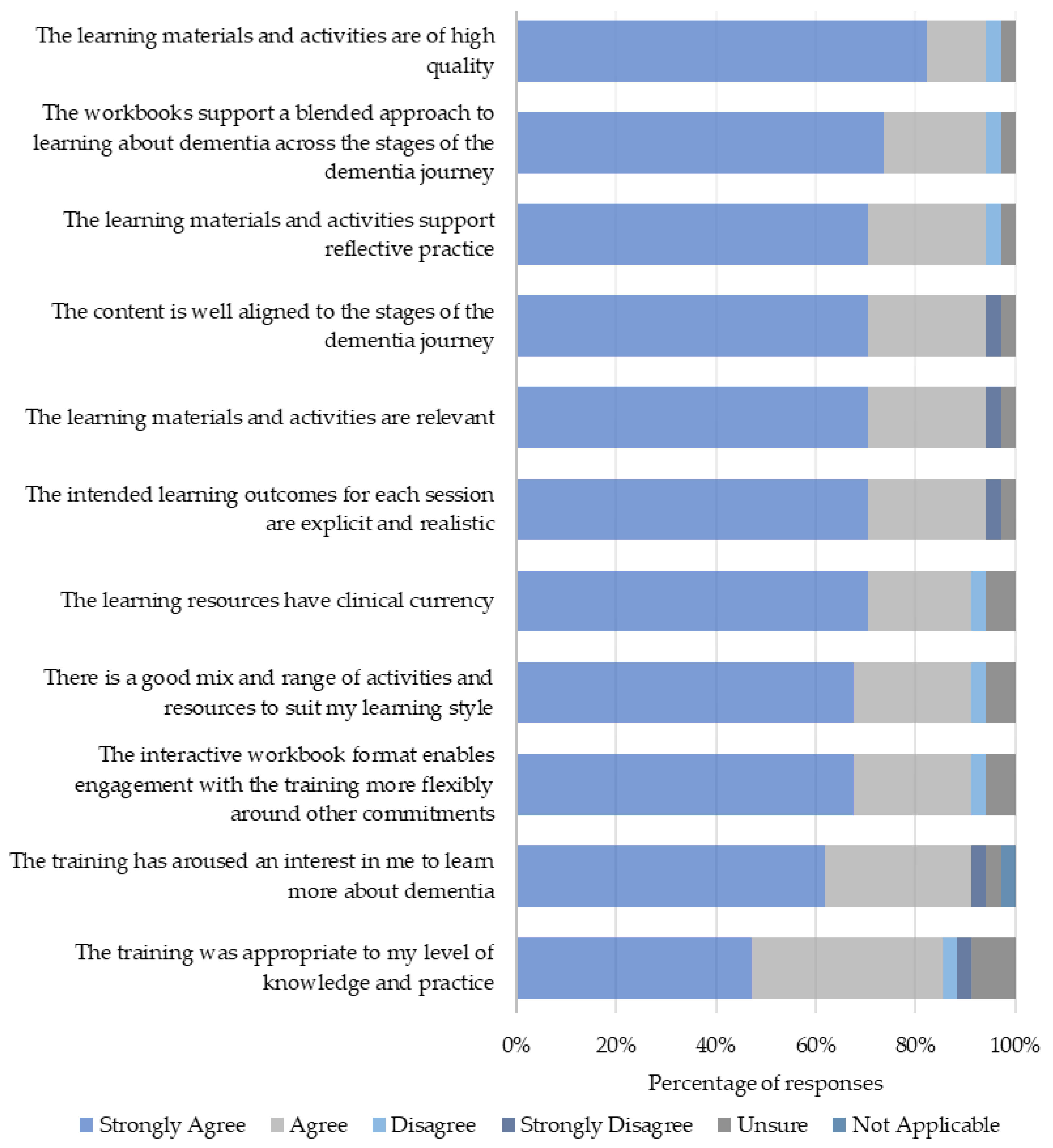
3.4. Level 1: Reaction to Asynchronous Resources
3.5. Level 1: Reaction to Synchronous Resources
3.6. Level 1: Reaction to Bichronous Learning
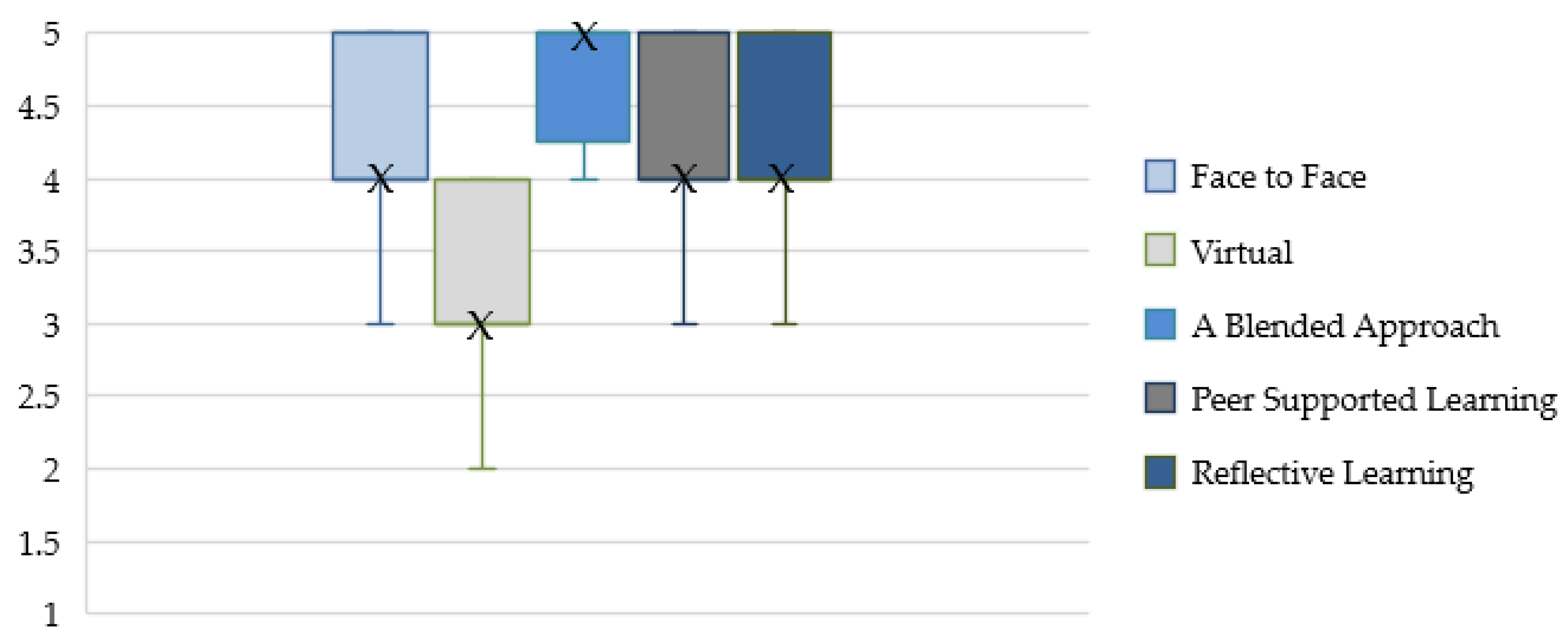
3.7. Preferred Mode of Learning
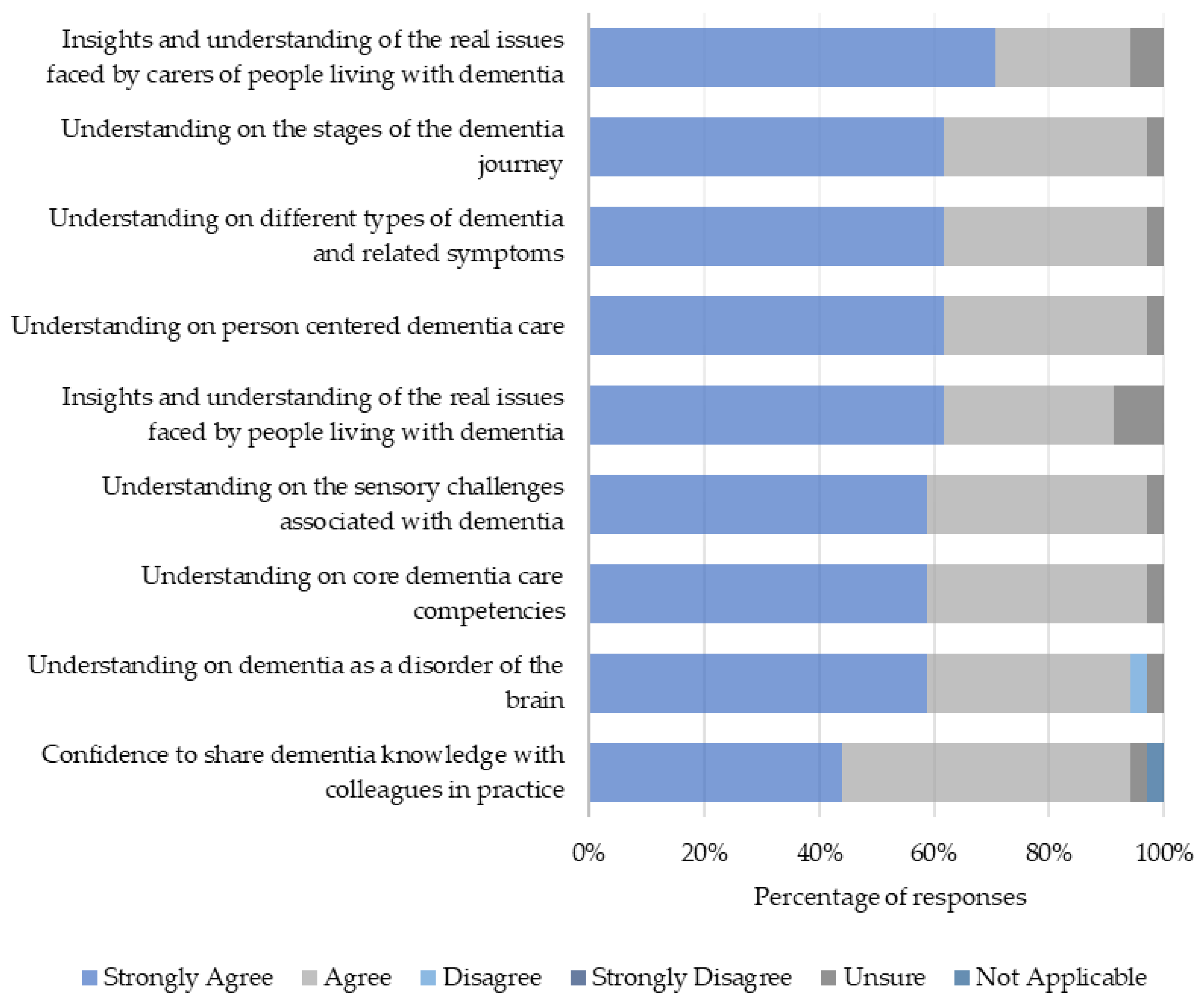
3.8. Level 2: Learning Gains
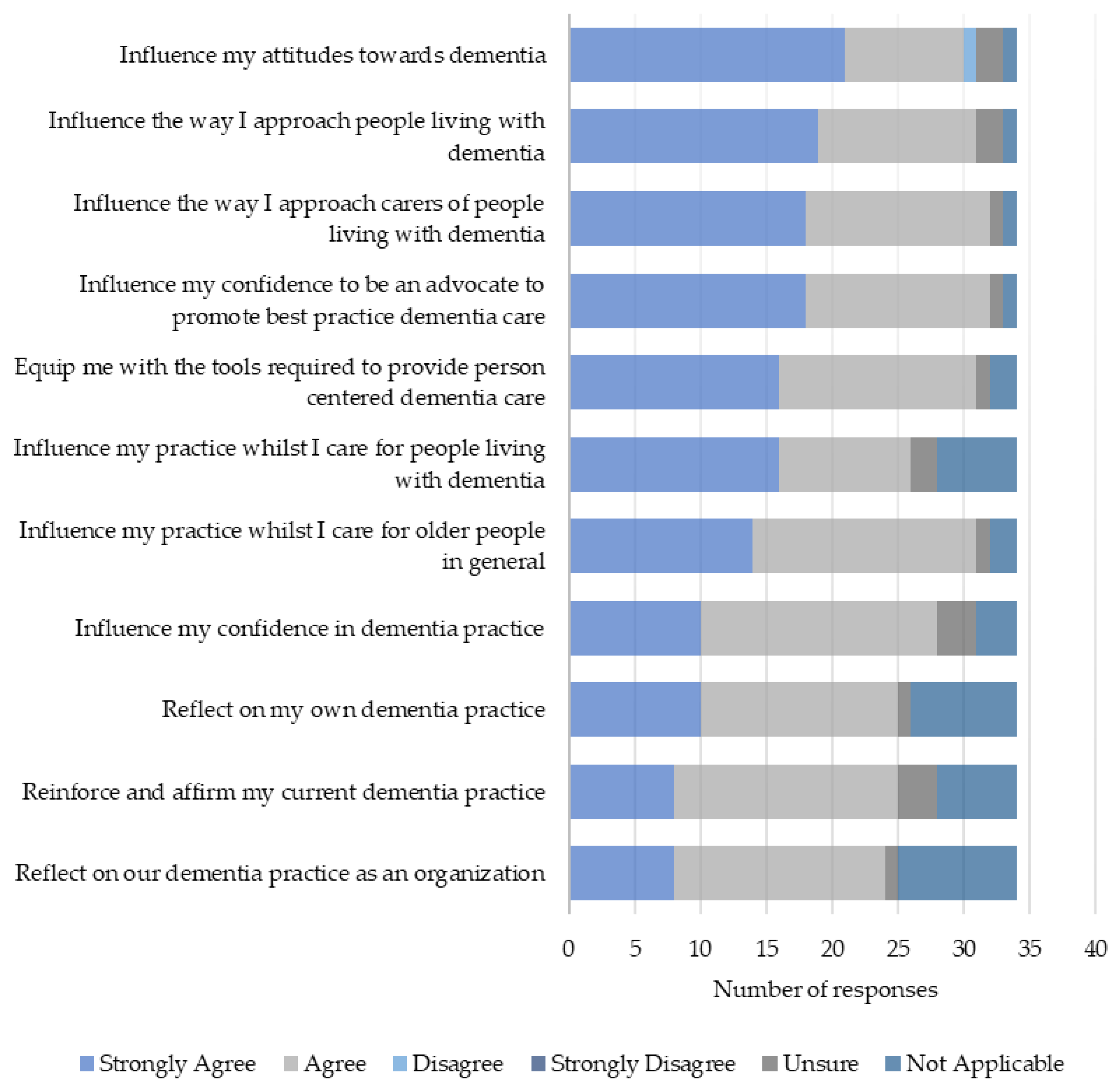
3.9. Level 3: Practice-Based Behavioral Change
3.10. Level 4: Results
“I would like to influence the way nurses learn and practice dementia care”.[93011072, Educator]
“I would like to help change the attitudes of some carers and give them a confidence boost and help them with their knowledge”.[81126963, Practitioner]
4. Results: Interview Findings
4.1. Demographics
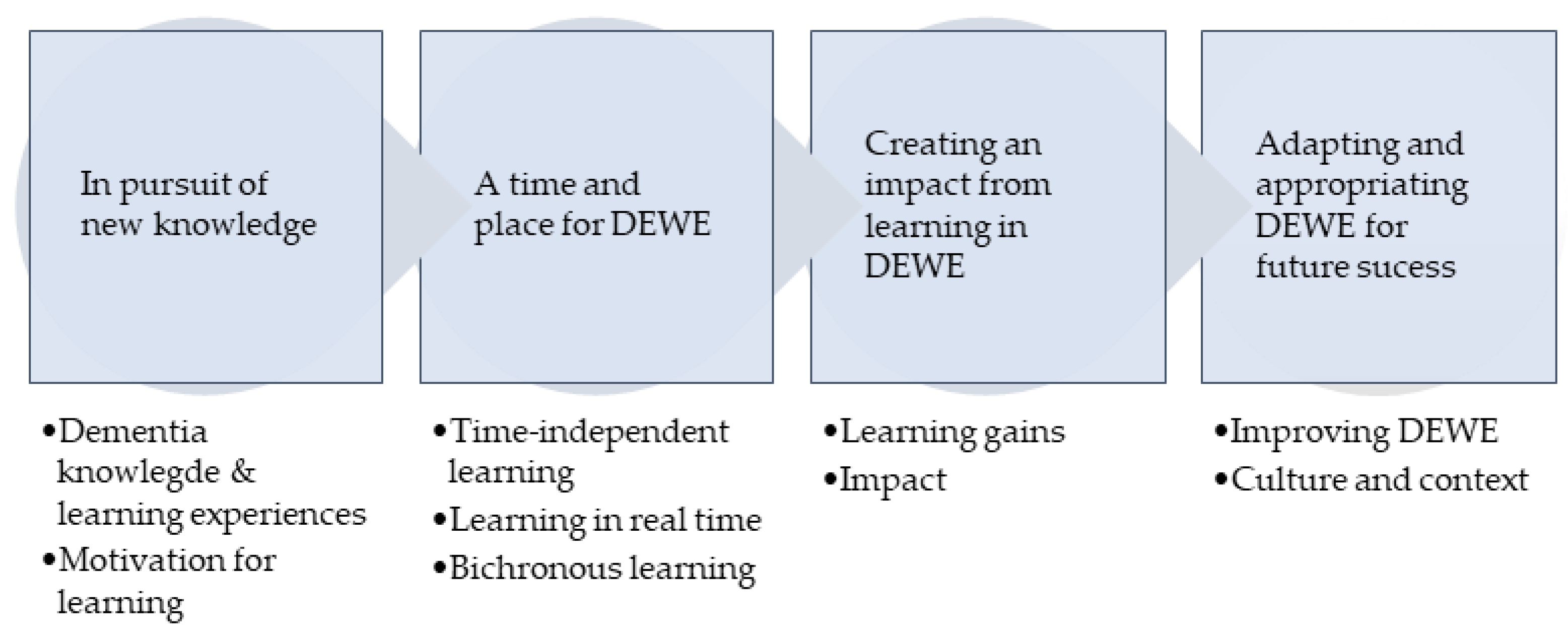
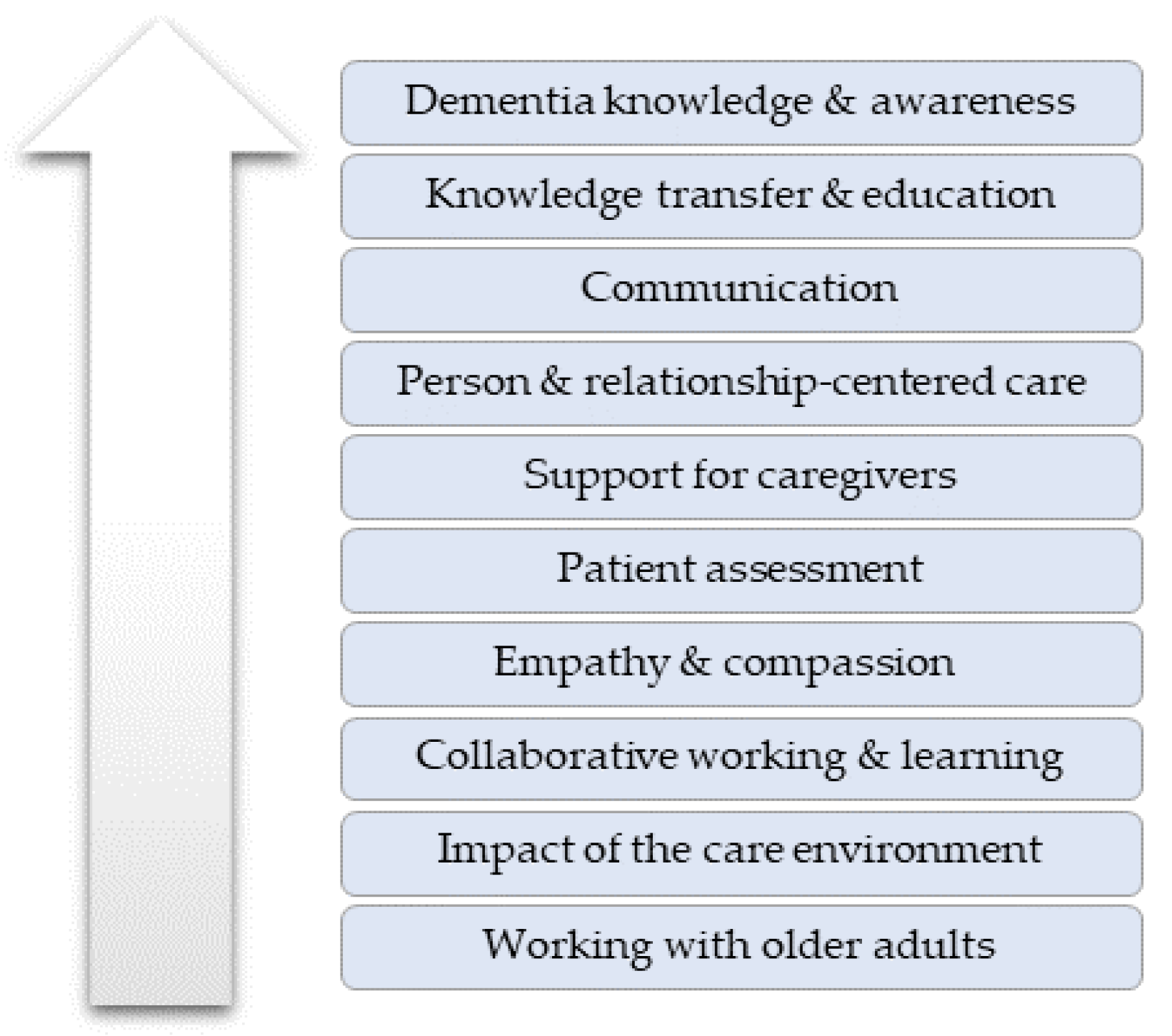
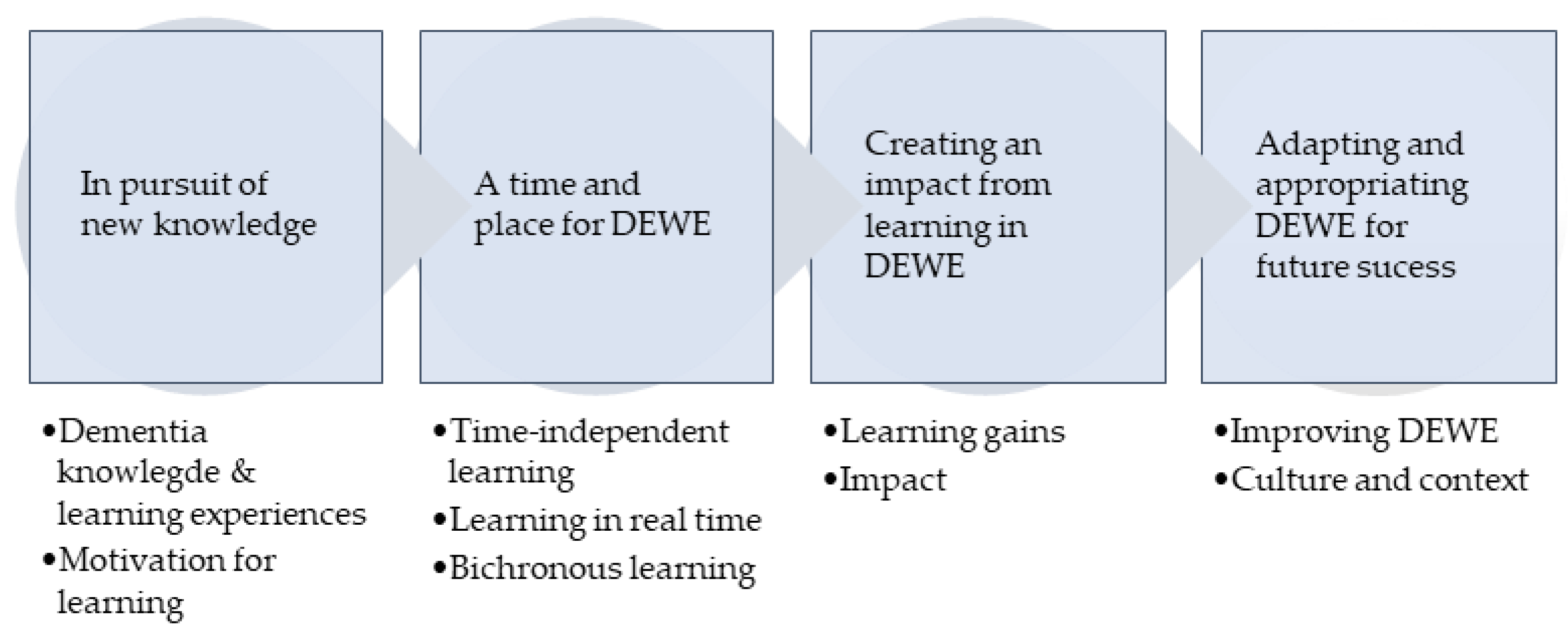
4.2. Themes
4.3. Theme 1: In Pursuit of New Knowledge
4.3.1. Dementia Knowledge and Learning Experiences
“Dementia is also a very important disorder that is on the rise, you know, like, more and more elderly patients are having this disorder and because of that I think, yeah, we should be really into understanding more about dementia, learning more about dementia and all that”.[P4-01-01]
“It is just a very small, small, minute part of the curriculum which, by the time the student becomes the staff, they would have forgotten, they wouldn’t even sometimes remember I feel”.[P4-01-01]
“We are used to like monotonous resource person going on and on and sometimes very few programs have some participation, but there is no variety in the program, you know, live program”.[P5-01-01]
“I don’t know how familiar you are with nursing curricula but they’re always very challenging to get everything into a relatively short period of time, three years is never long enough”.[P7-01-02]
“The system that we use for our staff …you log in by yourself, you watch twenty plus videos and after each video clip you have a multiple-choice question…its quite basic”.[P9-02-02]
4.3.2. Motivation for Learning
“I’ve been a caregiver for last 20 years now to my in-laws and three years ago my mother-in-law suffered a stroke and then she had an onset of dementia…and also at [workplace] we focus a lot on senior citizens care, that is one of our main areas of work, so, I thought both professionally and personally this is going to give me a lot of insights”.[P8-02-01]
“As an educator, always keen to try to enrich any students learning and, so, ……it was really good to sort of develop my own learning and understand things that are really helpful in others, in helping others to learn as well, you know, around dementia”.[P7-01-02]
4.4. Theme 2: A Time and a Place for DEWE
4.4.1. Time-Independent Learning
“I just found them really helpful and the fact that you can then revisit things because, you know, because my memories good at some points but others it isn’t… being able to revisit it and you could download some of the pages from that…which again was just helpful”.[P7-01-02]
“Seeing videos like that, you’re seeing it from the other person’s point of view…I understand now that they can’t help it, you know, it’s confusing for them”.[P9-02-02]
“I don’t think you learn in the same way when something is strictly online…a topic like dementia is about people, and you almost want to test out, sort of, you know, your own learning with others”.[P7-01-02]
4.4.2. Learning in Real Time
“Like it says like ‘none of us is smarter than all of us’, so, it’s like the years of wisdom comes in a room and all that, all those years of experience and learning, so that was very rich”.[P1-01-01]
“Lived experiences of people was more encouraging and practical and to learn from their life experiences, so that was very good and that was really touching our hearts”.[P5-01-01]
“I just thought she was amazing, so much passion, and you could tell that she loved making the lives better for the people that they had living with dementia, and it was just, yeah, it was heart-warming”.[P09-02-02]
“We had lots of opportunities to understand our perspectives as well as other perspectives, like it was a platform for us to introspect whether our understanding or our perspectives about dementia is right or what else I can look for when it comes to the care of patients”.[P6-01-01]
“I think that is just a fact of, you know, learning this way…obviously we encounter it all the time…there’s usually somebody who’s quite vocal, somebody else is trying to talk, but because you can’t see them you aren’t really aware of that, so that to me was probably a drawback”.[P7-01-02]
“We did have challenges using Webex because many times our people were not able to join, we are so accustomed to Zoom, that was the first time I think many of us were using Webex”.[P5-01-01]
4.4.3. Bichronous Learning
“It was actually perfect blending or perfect package of all three components, like all three domains of teaching, affective, cognitive, and psychomotor…so, it’s a perfect blending of all three domains of teaching”.[P6-01-01]
“I was able to take away much from the class because I was able to read and then come to the class, otherwise I don’t think it would have been so much of beneficial to me”.[P8-02-01]
“We can go over and over whenever we have a doubt, we can go back and learn from them, so the freedom to access that has been given to us…that is a positive thing”.[P5-01-01]
“Because this sort of fell during the pandemic, you know, we were adapting to online, you know, very quickly anyway…we were getting so familiar with the way that we were teaching anyway”.[P7-01-02]
4.5. Theme 3: Impact from Learning in DEWE
4.5.1. Learning Gains
“I have learned on how to be…an empathetic caregiver… an informed caregiver”.[P8-02-01]
4.5.2. Impact
“Earlier, it was not in my thinking, or it was not in part of my internal function, to think of something like this… to wonder if a person could have dementia”.[P1-01-01]
“On the last shift I did, I actually was in a bay, you know, with six ladies and one of whom, you know, did have dementia, so, you know, constantly I was just going back, you know, reiterating what I’d said, holding her hand and everything else and it was only when I was going back to another lady and they went ‘oh we’re going to have a quiet day today’ and I said ‘oh, have things been, you know, disturbing you?’ and she said, ‘yes’ she said ‘that’s the most attention she’s had since we’ve been here’”.[P7-01-02]
“There was something I learned, it was so profound, I put it on my social page…it was nice that some of the people within my friends circle who saw that, they replied back, and they told that, thank you so much it was a very good information and because they have somebody in their family who are living with dementia”.[P4-01-01]
“It was a particularly big blessing for me because I’ve written like some modules on elderly care, so I could apply this into that, and see, these modules and curriculum that we’ve designed is being used to train primary health level workers, nurses across India”.[P1-01-01]
“I think it should be rolled out everywhere, I think it should be like teamed up with the NHS, I think it should be done with all new staff starting, even old staff…. I think it would be a fantastic program to roll out”.[P9-02-02]
“I started to read articles on dementia related to India and South Asian countries, I found that there were very few nursing related articles, so, a colleague and I decided to conduct a small study and we’re in the process of doing that”.[P3-02-01]
4.6. Theme 4: Adapting and Appropriating DEWE for Future Success
4.6.1. Improving DEWE
“We want this to be given again and again with some other changes or a kind of recap, recapitulation, or kind of refresher course, we want this to be at least once a year or twice a year … I feel that it has to be refreshed”.[P6-01-01]
4.6.2. Culture and Context
“The context was good, but I think some of the tools which are available for people in probably UK settings are not available for people here, for example, like, xxxx shared about having a community of people with dementia and community helping each other so, we don’t have that kind of a network here”.[P8-02-01]
“For Northern India must have to think about the Hindi language and their perspectives, and South India might have to think a little different…like that, we might have to add a few videos or something… so that it feels that, yes, it is our own problems here and it is what our people are going through”.[P5-01-01]
5. Results: Mixed Methods
6. Discussion
Limitations
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Dementia A Public Health Priority. 2012. Available online: https://www.who.int/publications/i/item/dementia-a-public-health-priority (accessed on 3 April 2023).
- Alzheimer’s Society. Facts for the Media about Dementia. 2023. Available online: https://www.alzheimers.org.uk/about-us/news-and-media/facts-media (accessed on 3 April 2023).
- World Health Organization. Dementia: Key Facts. 2023. Available online: https://www.who.int/news-room/fact-sheets/detail/dementia (accessed on 3 April 2023).
- Scutti, S. New Estimate of Dementia Prevalence Indicates Magnitude of India’s Challenge. 2023. Available online: https://www.fic.nih.gov/News/GlobalHealthMatters/march-april-2023/Pages/new-estimate-dementia-prevalence-magnitude-india-challenge.aspx (accessed on 10 April 2023).
- Lee, J.; Meijer, E.; Langa, K.M.; Ganguli, M.; Varghese, M.; Banerjee, J.; Khobragade, P.; Angrisani, M.; Kurup, R.; Chakrabarti, S.S.; et al. Prevalence of dementia in India: National and state estimates from a nationwide study. Alzheimer’s Dement. J. Alzheimer’s Assoc. 2023, 19, 2898–2912. [Google Scholar] [CrossRef] [PubMed]
- Dias, A.; Patel, V. Closing the treatment gap for dementia in India. Indian J. Psychiatry 2009, 51 (Suppl. S1), S93–S97. [Google Scholar]
- Alzheimer’s and Related Disorders Society of India. The Dementia India Report: Prevalence, Impact, Costs and Services for Dementia; Executive Summary; Alzheimer’s and Related Disorders Society of India: New Delhi, India, 2010. [Google Scholar]
- Department of Health. Prime Minister’s Challenge on Dementia. Delivering Major Improvements in Dementia Care and Research by 2015. 2012. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/215101/dh_133176.pdf (accessed on 10 April 2023).
- Department of Health and Social Care. Prime Ministers Challenge on Dementia 2020. 2015. Available online: https://www.gov.uk/government/publications/prime-ministers-challenge-on-dementia-2020/prime-ministers-challenge-on-dementia-2020#why-dementia-remains-a-priority (accessed on 10 April 2023).
- Scottish Government. Scotland’s National Dementia Strategy 2010; The Scottish Government: Edinburgh, UK, 2010. [Google Scholar]
- Scottish Government. Standard of Care for Dementia in Scotland. 2011. Available online: https://www.gov.scot/publications/standards-care-dementia-scotland-action-support-change-programme-scotlands-national-dementia-strategy/ (accessed on 10 April 2023).
- Scottish Government. Scotland’s National Dementia Strategy 2013–2016. 2013. Available online: https://webarchive.nrscotland.gov.uk/3000/https://www.gov.scot/Resource/0042/00423472.pdf (accessed on 10 April 2023).
- Scottish Government. National Dementia Strategy: 2017–2020. 2017. Available online: https://www.gov.scot/publications/scotlands-national-dementia-strategy-2017-2020/pages/3/ (accessed on 10 April 2023).
- Scottish Government. Promoting Excellence 2021: A framework for All Health and Social Services Staff Working with People with Dementia, Their Families and Carers. 2021. Available online: https://www.gov.scot/publications/promoting-excellence-2021-framework-health-social-services-staff-working-people-dementia-families-carers/ (accessed on 10 April 2023).
- Muirhead, K.; Macaden, L.; Smyth, K.; Chandler, C.; Clarke, C.; Polson, R.; O’malley, C. Establishing the effectiveness of technology-enabled dementia education for health and social care practitioners: A systematic review. Syst. Rev. 2021, 10, 252. [Google Scholar] [CrossRef] [PubMed]
- Muirhead, K.; Macaden, L.; Smyth, K.; Chandler, C.; Clarke, C.; Polson, R.; O’malley, C. The characteristics of effective technology-enabled dementia education: A systematic review and mixed research synthesis. Syst. Rev. 2022, 11, 34. [Google Scholar] [CrossRef] [PubMed]
- Martin, F.; Kumar, S.; Ritzhaupt, A.D.; Polly, D. Bichronous online learning: Award-winning online instructor practices of blending asynchronous and synchronous online modalities. Internet High. Educ. 2023, 56, 100879. [Google Scholar] [CrossRef]
- Macaden, L. Being Dementia Smart (BDS): A Dementia Nurse Education Journey in Scotland. Int. J. Nurs. Educ. Scholarsh. 2016, 13, 45–53. [Google Scholar] [CrossRef]
- Baillie, L.; Sills, E.; Thomas, N. Educating a health service workforce about dementia: A qualitative study. Qual. Ageing Older Adults 2016, 17, 119–130. [Google Scholar] [CrossRef]
- Bute, J. Glorious Opportunity. Available online: https://www.gloriousopportunity.org/ (accessed on 17 April 2023).
- Gallagher, R. The lived experience of people with dementia. Br. Columbia Med. J. 2019, 61, 39–40. [Google Scholar]
- Nolan, M.R.; Davies, S.; Brown, J.; Keady, J.; Nolan, J. Beyond ‘person-centred’ care: A new vision for gerontological nursing. J. Clin. Nurs. 2004, 13, 45–53. [Google Scholar] [CrossRef] [PubMed]
- UK Government. Adults with Incapacity (Scotland) Act 2000. Available online: https://www.legislation.gov.uk/asp/2000/4/contents/enacted (accessed on 17 April 2023).
- NHS Education for Scotland. Staff Wellbeing Resources. 2021. Available online: https://www.nes.scot.nhs.uk/news/staff-wellbeing-resources/ (accessed on 17 April 2023).
- Kirkpatrick, D. Great Ideas Revisited. Techniques for evaluating training programs. Revisiting Kirkpatrick’s Four-Level Model. Train. Dev. 1996, 50, 54–59. [Google Scholar]
- Online Surveys. 2023. Available online: https://www.onlinesurveys.ac.uk/ (accessed on 24 April 2023).
- Braun, V.; Clarke, V. Thematic Analysis: A Practical Guide, 1st ed.; Sage: London, UK, 2021. [Google Scholar]
- Lincoln, Y.; Guba, E. Naturalistic Inquiry; Sage: Newbury Park, CA, USA, 1985. [Google Scholar]
- Fazio, S.; Pace, D.; Flinner, J.; Kallmyer, B. The Fundamentals of Person-Centered Care for Individuals with Dementia. Gerontologist 2018, 58 (Suppl. S1), S10–S19. [Google Scholar] [CrossRef]
- Kitwood, T. Dementia Reconsidered: The Person Comes First; Open University Press: Maidenhead, UK, 1997. [Google Scholar]
- Dhawan, S. Online Learning: A Panacea in the Time of COVID-19 Crisis. J. Educ. Technol. Syst. 2020, 49, 5–22. [Google Scholar] [CrossRef]
- Almutairi, H.; Stafford, A.; Etherton-Beer, C.; Flicker, L.; Saunders, R. Aged care staff perceptions of an online training program for responsive behaviours of residents with dementia. Australas. J. Ageing 2022, 41, e112–e121. [Google Scholar] [CrossRef]
- Gallant, N.; Hadjistavropoulos, T.; Winters, E.M.; Feere, E.K.; Wickson-Griffiths, A. Development, evaluation, and implementation of an online pain assessment training program for staff in rural long-term care facilities: A case series approach. BMC Geriatr. 2022, 22, 336. [Google Scholar] [CrossRef]
- Jones, C.; Moyle, W. Sexuality & dementia: An eLearning resource to improve knowledge and attitudes of aged-care staff. Educ. Gerontol. 2016, 42, 563–571. [Google Scholar] [CrossRef]
- Cleveland-Innes, M.; Wilton, D.; Guide to Blended Learning. Chapter 7: Synchronous and Asynchronous Activities. 2018. Available online: https://openbooks.col.org/blendedlearning/chapter/chapter-7-synchronous-and-asynchronous-activities/ (accessed on 24 April 2023).
- Knowles, M. Adult learning. In The ASTD Training and Development Handbook, 4th ed.; Craig, R., Ed.; McGraw-Hill: New York, NY, USA, 1996. [Google Scholar]
- Surr, C.A.; Parveen, S.; Smith, S.J.; Drury, M.; Sass, C.; Burden, S.; Oyebode, J. The barriers and facilitators to implementing dementia education and training in health and social care services: A mixed-methods study. BMC Health Serv. Res. 2020, 20, 512. [Google Scholar] [CrossRef]
- Enders, N.; Gaschler, R.; Kubik, V. Online Quizzes with Closed Questions in Formal Assessment: How elaborate feedback can promote learning. Psychol. Learn. Teach. 2021, 20, 91–106. [Google Scholar] [CrossRef]
- Mate, K.; Weidenhofer, J. Considerations and strategies for effective online assessment with a focus on the biomedical sciences. FASEB BioAdv. 2021, 4, 9–21. [Google Scholar] [CrossRef]
- Perera-Diltz, D.; Moe, J. Formative and summative assessment in online education. J. Res. Innov. Teach. 2014, 7, 130–142. [Google Scholar]
- Surr, C.A.; Gates, C.; Irving, D.; Oyebode, J.; Smith, S.J.; Parveen, S.; Drury, M.; Dennison, A. Effective Dementia Education and Training for the Health and Social Care Workforce: A systematic review of the literature. Rev. Educ. Res. 2017, 87, 966–1002. [Google Scholar] [CrossRef]
- Toubøl, A.; Moestrup, L.; Thomsen, K.; Ryg, J.; Hansen, D.L.; Foldager, M.; Jakobsen, S.; Nielsen, D.S. The impact of an education intervention on the approach of hospital staff to patients with dementia in a Danish general hospital setting: An explanatory sequential mixed-methods study. Nord. J. Nurs. Res. 2022, 42, 28–41. [Google Scholar] [CrossRef]
- Wenger-Trayner, E.; Wenger-Trayner, B. Introduction to Communities of Practice: A Brief Overview of the Concept and Its Uses. 2015. Available online: https://www.wenger-trayner.com/introduction-to-communities-of-practice/ (accessed on 8 May 2023).
- McLean, S.F. Case-Based Learning and Its Application in Medical and Health-Care Fields: A Review of Worldwide Literature. J. Med. Educ. Curric. Dev. 2016, 3, JMECD.S20377. [Google Scholar] [CrossRef]
- Kolb, D. Experiential Learning: Experience as the Source of Learning and Development; Prentice-Hall: Englewood Cliffs, NJ, USA, 1984. [Google Scholar]
- Seshan, V.; Matua, G.A.; Raghavan, D.; Arulappan, J.; Al Hashmi, I.; Roach, E.J.; Sunderraj, S.E.; Prince, E.J. Case Study Analysis as an Effective Teaching Strategy: Perceptions of Undergraduate Nursing Students from a Middle Eastern Country. SAGE Open Nurs. 2021, 7, 23779608211059265. [Google Scholar] [CrossRef]
- Toney-Butler, T.J.; Thayer, J.M. Nursing Process. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- HealthcareUK. India and the UK: Partners in Healthcare. 2014. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/311349/Healthcare_UK_India_and_the_UK_LOW.pdf (accessed on 8 May 2023).
- Ravindranath, V.; Sundarakumar, J.S. Changing demography and the challenge of dementia in India. Nat. Rev. Neurol. 2021, 17, 747–758. [Google Scholar] [CrossRef]
- Kember, D.; Ho, A.; Hong, C. The importance of establishing relevance in motivating student learning. Act. Learn. High. Educ. 2008, 9, 249–263. [Google Scholar] [CrossRef]
- Cashin, Z.; Daley, S.; Hebditch, M.; Hughes, L.; Banerjee, S. Involving people with dementia and their carers in dementia education for undergraduate healthcare professionals: A qualitative study of motivation to participate and experience. Int. Psychogeriatr. 2019, 31, 869–876. [Google Scholar] [CrossRef]
- Birden, H.; Glass, N.; Wilson, I.; Harrison, M.; Usherwood, T.; Nass, D. Teaching professionalism in medical education: A Best Evidence Medical Education (BEME) systematic review. BEME Guide No. 25. Med. Teach. 2013, 35, e1252–e1266. [Google Scholar] [CrossRef]
- Lepp, M.; Luik, P.; Tark, T.M. How Can Web Lessons Be Taught to Reduce Screen Fatigue, Motivational, and Concentration Problems in Different Disciplines? Front. Sociol. 2022, 7, 871770. [Google Scholar] [CrossRef]
- Sophonhiranrak, S. Features, barriers, and influencing factors of mobile learning in higher education: A systematic review. Heliyon 2021, 7, e06696. [Google Scholar] [CrossRef]
- Nikpeyma, N.; Zolfaghari, M.; Mohammadi, A. Barriers and facilitators of using mobile devices as an educational tool by nursing students: A qualitative research. BMC Nurs. 2021, 20, 226. [Google Scholar] [CrossRef]
- Oza, P. Digital Etiquette in Online Teaching Learning. 2022. Available online: https://ssrn.com/abstract=4217177 (accessed on 15 May 2023).
- Iqbal, S.; Hanif, R.; Ali, F.; Tahir, M.; Minhas, R.; Yasmeen, R.; Khokhar, A.; Laique, T. Teachers’ Perceptions of Netiquette Practices by undergraduate Dental Students During Online Classes in COVID-19 Pandemic. Pak. J. Med. Health Sci. 2021, 15, 3498–3500. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Asynchronous | Synchronous | |||
|---|---|---|---|---|
| Workbook | Session | Duration | Facilitator | |
| Introduction to DEWE and Workbooks | 1 | 30 min | 1 | |
| 1. Dementia Care Essentials | The Human Brain | 2 | 1 h | 1 |
| Dementia: What it is and what it is not | 3 | 1 h | 1 | |
| Memory Changes in Dementia | 4 | 30 min | 1 | |
| Sensory Changes in Dementia | 5 | 30 min | 1 | |
| 2. Dementia Care Priorities | Living with Dementia: Person-centered approaches | 6 | 1 h | 1 |
| Stages of the Dementia Journey (Barbara’s Story a) | 7 | 3 h | 2 | |
| Carer’s Perspectives in Dementia | 8 | 1 h | 3 | |
| Stress & Distress in Dementia | 9 | 1 h | 1, 4 | |
| Dementia, Delirium and Depression | 10 | 2 h | 2 | |
| 3. Dementia Care Enablers | Staff: Self-care and wellbeing during COVID-19 b | 11 | - | - |
| Dementia & COVID-19 in Care Homes | 12 | 1.5 h | 5 | |
| Implementing Change and Improvement | 13 | 1.5 h | 5 | |
| Dementia Inclusive and Enabling Environments | 14 | 2 h | 1, 6 | |
| End-of-life care in Dementia | 15 | 2 h | 1 | |
| Relationship-centered Approaches to Dementia Care using the Six Senses Framework | 16 | 2 h | 1 | |
| Enjoyed Most | Enjoyed Least |
|---|---|
| 1. Group discussion and interactivity | 1. Technical issues/videoconferencing platform |
| 2. Course presentation/expert facilitation | 2. Difficulty coordinating attendance |
| 3. Reflective activities | 3. Duration of interactive sessions (too long) |
| 4. Workbooks | 4. Duration of interactive sessions (too short) |
| 5. Use of real-life stories and examples | 5. Lack of participant interaction in break out rooms |
| 6. Videos | 6. Reflective activities |
| 7. Structure and content (general) | 7. Overall course duration (too short) |
| 8. New knowledge | 8. Digital skill requirements |
| 9. Technology-enabled/blended approach | 9. Technology-enabled delivery mode |
| 10. Convenience |
| Knowledge Aspect | Quote |
|---|---|
| Types of dementia | “We learned that there is like 200 different types of dementia…I had no idea, and I’ve got twenty plus years’ experience, like, in health and social care”. [P9-02-02] |
| Neurophysiology | “The role of hippocampus…so what is the difference between normal ageing and dementia, especially when we talk about memory changes…that is what is more important to know”. [P6-01-01] |
| Stress & Distress | “I really learned from this course…like analyzing a situation using the ABC chart…when something happens”. [P5-01-01] |
| Delirium | “Particularly in my clinical role, you know, in acute trauma, being able to identify things like delirium is so helpful, so those tools were really good”. [P7-01-02] |
| Person-centered care | “I have learned tools on how to handle different situations and how to understand why the person is behaving in a certain way and therefore how you kind of adapt your care to suit that person’s needs”. [P8-02-01] |
| Relationship-centered care | “I really liked the six senses approach, I thought that was really, really useful”. [P7-01-02] |
| Care for caregivers | “I understood that not only people living with dementia that needs attention, but we have to pay special attention even to the carers of people living with dementia”. [P4-01-01] |
| Dignity & Respect | “Taking your time with people, never getting cross, and the fact that you might have to answer the same thing…you’re answering the same questions but doing so every time with patience rather than frustration can make a huge difference”. [P7-01-02] |
| Care environment | “I remember some of the classes where they said how does the environment impact a person living with dementia, so, I think even the environment also is very, very important, the type of environment that we create around these people”. [P4-01-01] |
| Care empathy | “It can be very frustrating to have dementia and to place ourselves in their shoes, like some of those case studies we looked at, and listening to the various talks, that really helped me”. [P1-01-01] |
| Strengths | Areas for Development | |
|---|---|---|
| Satisfaction | ||
| Asynchronous | High quality resources | Consider cultural adaptations |
| Easy to use | Provide more assessments | |
| Time for learning | Improve placement of videos | |
| Learning on demand | Improve quality of resources in print form | |
| Active learning | Update content regularly | |
| Real-life videos | Consider strategies for learner motivation | |
| Preparation for synchronous sessions | ||
| Synchronous | Interactive | Include interactive icebreakers session |
| Active learning and reflection | Discuss/mitigate technical issues | |
| Diversity of participants | Discuss/mitigate poor online etiquette | |
| Includes dementia experts | Optimize session duration | |
| Includes people with lived experience | Optimize delivery platform | |
| Provides expert facilitation | Include more discussions on actual cases | |
| Consolidates asynchronous learning | Provide follow-up sessions | |
| Bichronous | Highly rated | - |
| Mutual learning between resources | ||
| Ongoing access to resources | ||
| Relevance post-COVID-19 | ||
| Learning | New knowledge | - |
| New skills | ||
| Positive attitudes | ||
| Behaviors | Positive behavior change | - |
| Results | ↑ Dementia awareness | - |
| ↑ Knowledge transfer | ||
| ↑ Development of educational resources | ||
| ↑ Engagement with dementia education | ||
| ↑ Engagement with dementia research | ||
| Dissemination of DEWE (wider audience) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Macaden, L.; Muirhead, K. Dementia Education for Workforce Excellence: Evaluation of a Novel Bichronous Approach. Healthcare 2024, 12, 590. https://doi.org/10.3390/healthcare12050590
Macaden L, Muirhead K. Dementia Education for Workforce Excellence: Evaluation of a Novel Bichronous Approach. Healthcare. 2024; 12(5):590. https://doi.org/10.3390/healthcare12050590
Chicago/Turabian StyleMacaden, Leah, and Kevin Muirhead. 2024. "Dementia Education for Workforce Excellence: Evaluation of a Novel Bichronous Approach" Healthcare 12, no. 5: 590. https://doi.org/10.3390/healthcare12050590
APA StyleMacaden, L., & Muirhead, K. (2024). Dementia Education for Workforce Excellence: Evaluation of a Novel Bichronous Approach. Healthcare, 12(5), 590. https://doi.org/10.3390/healthcare12050590