
Measuring Motivations to Eat Palatable Foods: Adaptation and Psychometric Properties of the Italian Version of the Palatable Eating Motives Scale (PEMS-IT)

 ,
,  ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Translation and Cultural Adaptation
- Step 1: Translation
- Step 2: Synthesis of the translations
- Step 3: Back-translation
- Step 4: Expert committee evaluation
- Step 5: Pre-test of the pre-final version
2.2. Sample Size Calculation
2.3. Procedure
2.4. Participants
2.5. Measures
2.6. Statistical Analysis
3. Results
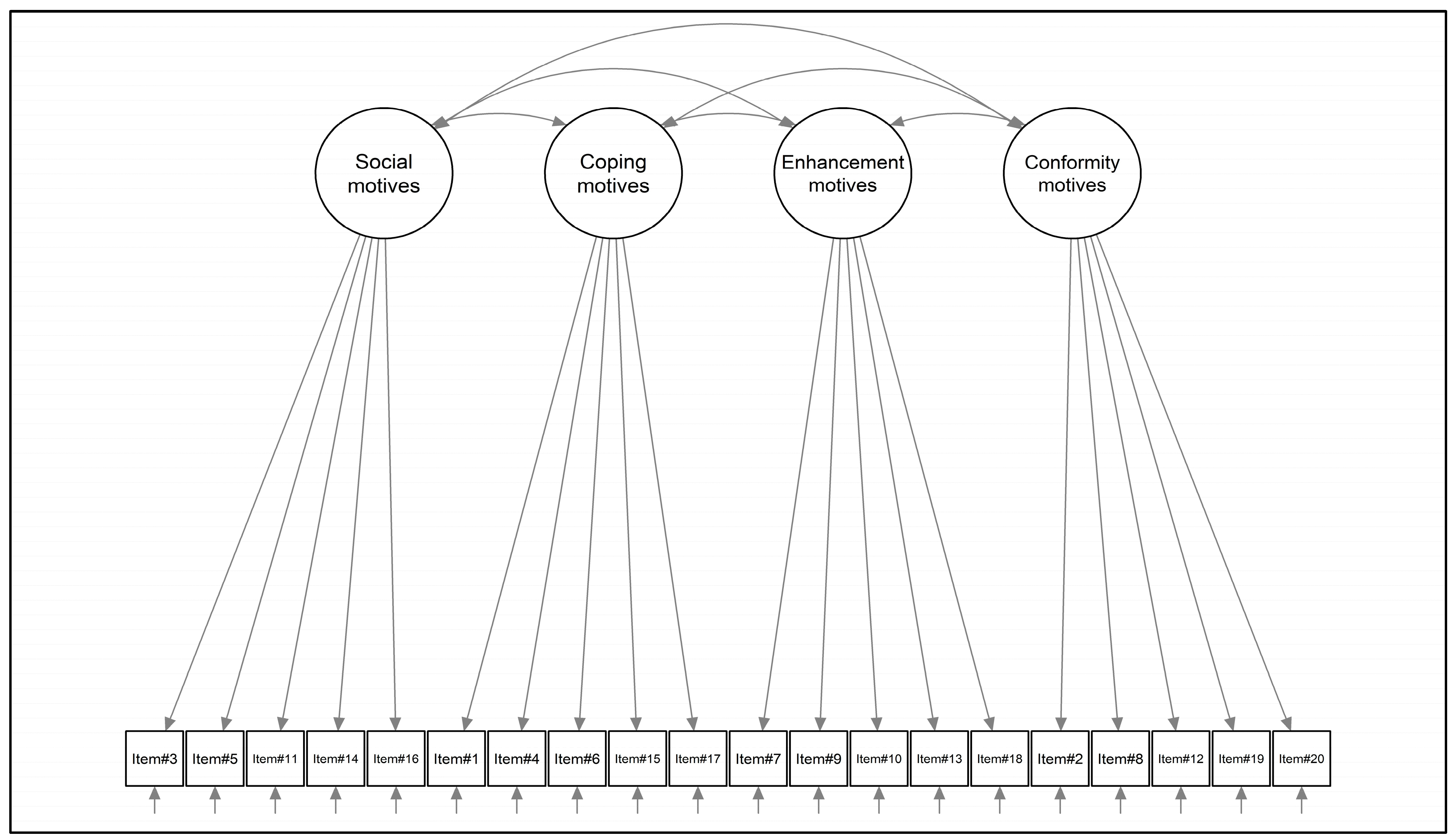
3.1. Structural Validity
3.2. Internal Consistency
3.3. Convergent Validity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Popov, V.B.; Aytaman, A.; Aleman, J.O. Obesity: The Forgotten Pandemic. Am. J. Gastroenterol. 2022, 117, 7–10. [Google Scholar] [CrossRef]
- Pietrabissa, G.; Manzoni, G.M.; Corti, S.; Vegliante, N.; Molinari, E.; Castelnuovo, G. Addressing motivation in globesity treatment: A new challenge for clinical psychology. Front. Psychol. 2012, 3, 317. [Google Scholar] [CrossRef]
- Greaves, C.; Poltawski, L.; Garside, R.; Briscoe, S. Understanding the challenge of weight loss maintenance: A systematic review and synthesis of qualitative research on weight loss maintenance. Health Psychol. Rev. 2017, 11, 145–163. [Google Scholar] [CrossRef]
- Castelnuovo, G.; Manzoni, G.M.; Villa, V.; Cesa, G.L.; Pietrabissa, G.; Molinari, E. The STRATOB study: Design of a randomized controlled clinical trial of Cognitive Behavioral Therapy and Brief Strategic Therapy with telecare in patients with obesity and binge-eating disorder referred to residential nutritional rehabilitation. Trials 2011, 12, 114. [Google Scholar] [CrossRef] [PubMed]
- Evert, A.B.; Franz, M.J. Why Weight Loss Maintenance Is Difficult. Diabetes Spectr. 2017, 30, 153–156. [Google Scholar] [CrossRef] [PubMed]
- Hall, K.D.; Kahan, S. Maintenance of Lost Weight and Long-Term Management of Obesity. Med. Clin. N. Am. 2018, 102, 183–197. [Google Scholar] [CrossRef]
- Jackson, J.B.; Pietrabissa, G.; Rossi, A.; Manzoni, G.M.; Castelnuovo, G. Brief strategic therapy and cognitive behavioral therapy for women with binge eating disorder and comorbid obesity: A randomized clinical trial one-year follow-up. J. Consult. Clin. Psychol. 2018, 86, 688–701. [Google Scholar] [CrossRef]
- Harb, A.A.; Shechter, A.; Koch, P.A.; St-Onge, M.P. Ultra-processed foods and the development of obesity in adults. Eur. J. Clin. Nutr. 2023, 77, 619–627. [Google Scholar] [CrossRef]
- Fox, C.K.; Northrop, E.F.; Rudser, K.D.; Ryder, J.R.; Kelly, A.S.; Bensignor, M.O.; Bomberg, E.M.; Bramante, C.T.; Gross, A.C. Contribution of Hedonic Hunger and Binge Eating to Childhood Obesity. Child. Obes. 2021, 17, 257–262. [Google Scholar] [CrossRef]
- Burdette, J.H.; Laurienti, P.J.; Miron, L.L.; Bahrami, M.; Simpson, S.L.; Nicklas, B.J.; Fanning, J.; Rejeski, W.J. Functional Brain Networks: Unique Patterns with Hedonic Appetite and Confidence to Resist Eating in Older Adults with Obesity. Obesity 2020, 28, 2379–2388. [Google Scholar] [CrossRef]
- Gearhardt, A.N.; DiFeliceantonio, A.G. Highly processed foods can be considered addictive substances based on established scientific criteria. Addiction 2023, 118, 589–598. [Google Scholar] [CrossRef]
- Lowe, M.R.; Butryn, M.L. Hedonic hunger: A new dimension of appetite? Physiol. Behav. 2007, 91, 432–439. [Google Scholar] [CrossRef] [PubMed]
- Ferriter, C.; Ray, L.A. Binge eating and binge drinking: An integrative review. Eat. Behav. 2011, 12, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Cattivelli, R.; Castelnuovo, G.; Musetti, A.; Varallo, G.; Spatola, C.A.M.; Riboni, F.V.; Usubini, A.G.; Tosolin, F.; Manzoni, G.M.; Capodaglio, P.; et al. ACTonHEALTH study protocol: Promoting psychological flexibility with activity tracker and mHealth tools to foster healthful lifestyle for obesity and other chronic health conditions. Trials 2018, 19, 659. [Google Scholar] [CrossRef]
- Boggiano, M.M. Palatable Eating Motives Scale in a college population: Distribution of scores and scores associated with greater BMI and binge-eating. Eat. Behav. 2016, 21, 95–98. [Google Scholar] [CrossRef] [PubMed]
- Fazzino, T.L.; Raheel, A.; Peppercorn, N.; Forbush, K.; Kirby, T.; Sher, K.J.; Befort, C. Motives for drinking alcohol and eating palatable foods: An evaluation of shared mechanisms and associations with drinking and binge eating. Addict. Behav. 2018, 85, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Burgess, E.E.; Turan, B.; Lokken, K.L.; Morse, A.; Boggiano, M.M. Profiling motives behind hedonic eating. Preliminary validation of the Palatable Eating Motives Scale. Appetite 2014, 72, 66–72. [Google Scholar] [CrossRef] [PubMed]
- Rogers, P.J. Determinants of food reward and some parallels with vehicles for self-administration of nicotine, caffeine and alcohol. Addiction 2023, 118, 601–602. [Google Scholar] [CrossRef] [PubMed]
- Cooper, M.L.; Kuntsche, E.; Levitt, A.; Barber, L.L.; Wolf, S. Motivational models of substance use: A review of theory and research on motives for using alcohol, marijuana, and tobacco. In The Oxford Handbook of Substance Use and Substance Use Disorders; Oxford University Press: New York, NY, USA, 2016; Volume 1. [Google Scholar]
- Boggiano, M.M.; Burgess, E.E.; Turan, B.; Soleymani, T.; Daniel, S.; Vinson, L.D.; Lokken, K.L.; Wingo, B.C.; Morse, A. Motives for eating tasty foods associated with binge-eating. Results from a student and a weight-loss seeking population. Appetite 2014, 83, 160–166. [Google Scholar] [CrossRef]
- Boggiano, M.M.; Wenger, L.E.; Burgess, E.E.; Tatum, M.M.; Sylvester, M.D.; Morgan, P.R.; Morse, K.E. Eating tasty foods to cope, enhance reward, socialize or conform: What other psychological characteristics describe each of these motives? J. Health Psychol. 2017, 22, 280–289. [Google Scholar] [CrossRef]
- Bjorlie, K.; Forbush, K.T.; Chapa, D.A.N.; Richson, B.N.; Johnson, S.N.; Fazzino, T.L. Hyper-palatable food consumption during binge-eating episodes: A comparison of intake during binge eating and restricting. Int. J. Eat. Disord. 2022, 55, 688–696. [Google Scholar] [CrossRef]
- Carbone, E.A.; Aloi, M.; Rania, M.; de Filippis, R.; Quirino, D.; Fiorentino, T.V.; Segura-Garcia, C. The relationship of food addiction with binge eating disorder and obesity: A network analysis study. Appetite 2023, 190, 107037. [Google Scholar] [CrossRef]
- Ratkovic, D.; Knezevic, V.; Dickov, A.; Fedrigolli, E.; Comic, M. Comparison of binge-eating disorder and food addiction. J. Int. Med. Res. 2023, 51, 3000605231171016. [Google Scholar] [CrossRef]
- Gearhardt, A.N.; White, M.A.; Potenza, M.N. Binge eating disorder and food addiction. Curr. Drug Abus. Rev. 2011, 4, 201–207. [Google Scholar] [CrossRef]
- Cooper, M.L.; Russell, M.; Skinner, J.B.; Windle, M. Development and validation of a three-dimensional measure of drinking motive. Psychol. Assess. 1992, 4, 123–132. [Google Scholar] [CrossRef]
- Cooper, M.L. Motivations for alcohol use among adolescents: Development and validation of a four-factor model. Psychol. Assess. 1994, 6, 117–128. [Google Scholar] [CrossRef]
- Beaton, D.E.; Bombardier, C.; Guillemin, F.; Ferraz, M.B. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine 2000, 25, 3186–3191. [Google Scholar] [CrossRef] [PubMed]
- Kline, R.B. Principles and Practice of Structural Equation Modeling; The Guilford Press: New York, NY, USA, 2023. [Google Scholar]
- Manzoni, G.M.; Rossi, A.; Pietrabissa, G.; Mannarini, S.; Fabbricatore, M.; Imperatori, C.; Innamorati, M.; Gearhardt, A.N.; Castelnuovo, G. Structural validity, measurement invariance, reliability and diagnostic accuracy of the Italian version of the Yale Food Addiction Scale 2.0 in patients with severe obesity and the general population. Eat. Weight. Disord. 2021, 26, 345–366. [Google Scholar] [CrossRef] [PubMed]
- Rossi, A.A.; Mannarini, S.; Castelnuovo, G.; Pietrabissa, G. Disordered Eating Behaviors Related to Food Addiction/Eating Addiction in Inpatients with Obesity and the General Population: The Italian Version of the Addiction-like Eating Behaviors Scale (AEBS-IT). Nutrients 2022, 15, 104. [Google Scholar] [CrossRef]
- Rossi, A.A.; Pietrabissa, G.; Gearhardt, A.N.; Musetti, A.; Castelnuovo, G.; Mannarini, S. Eating Compulsivity in Inpatients with Severe Obesity and the General Population: The Italian Version of the Measure of Eating Compulsivity (MEC10-IT). Nutrients 2023, 15, 1378. [Google Scholar] [CrossRef]
- Rossi, A.A.; Pietrabissa, G.; Tagliagambe, A.; Scuderi, A.; Montecchiani, L.; Castelnuovo, G.; Mannarini, S.; Dalla Ragione, L. Many Facets of Eating Disorders: Profiling Key Psychological Features of Anorexia Nervosa and Binge Eating Disorder. Behav. Sci. 2023, 13, 276. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Physical Status: The Use and Interpretation of Anthropometry, Report of a WHO Expert Committee; WHO Technical Report Series 854; World Health Organization: Geneva, Switzerland, 1995.
- Imperatori, C.; Fabbricatore, M.; Lester, D.; Manzoni, G.M.; Castelnuovo, G.; Raimondi, G.; Innamorati, M. Psychometric properties of the modified Yale Food Addiction Scale Version 2.0 in an Italian non-clinical sample. Eat. Weight Disord. 2019, 24, 37–45. [Google Scholar] [CrossRef]
- Ricca, V.; Mannucci, E.; Moretti, S.; Di Bernardo, M.; Zucchi, T.; Cabras, P.L.; Rotella, C.M. Screening for binge eating disorder in obese outpatients. Compr. Psychiatry 2000, 41, 111–115. [Google Scholar] [CrossRef]
- Rossi, A.A.; Pietrabissa, G.; Castelnuovo, G.; Mannarini, S. Cognitive Restraint, Uncontrolled Eating, and Emotional Eating. The Italian Version of the Three Factor Eating Questionnaire—Revised 18 (TFEQ-R-18): A Three-step Validation Study. Eat. Weight. Disord. 2024, 29, 16. [Google Scholar] [CrossRef]
- Rossi, A.A.; Mannarini, S.; Castelnuovo, G.; Pietrabissa, G. Grazing: A different form of food addiction. The Italian version of the Repetitive Eating Questionnaire (Rept(Eat)-Q). Nutrients 2023, in press. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2017. [Google Scholar]
- R Core Team. The R Project for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2014. [Google Scholar]
- Rosseel, Y. Lavaan: An R Package for Structural Equation Modeling. J. Stat. Softw. 2012, 48, 1–36. [Google Scholar] [CrossRef]
- Rosseel, Y.; Oberski, D.L.; Byrnes, J.; Vanbrabant, L.; Savalei, V.; Merkle, E.; Hallquist, M.; Rhemtulla, M.; Katsikatsou, M.; Barendse, M.; et al. Package ‘lavaan’; 2017; pp. 1–89. Available online: http://cran.nexr.com/web/packages/lavaan/lavaan.pdf (accessed on 11 January 2024).
- Revelle, W. psych: Procedures for Personality and Psychological Research; Northwestern University: Evanston, IL, USA, 2018. [Google Scholar]
- Revelle, W. psychTools:Tools to Accompany the ‘psych’ Package for Psychological Research; Northwestern University: Evanston, IL, USA, 2020. [Google Scholar]
- Wickham, H.; Averick, M.; Bryan, J.; Chang, W.; McGowan, L.D.; François, R.; Grolemund, G.; Hayes, A.; Henry, L.; Hester, J.; et al. Welcome to the tidyverse. J. Open Source Softw. 2019, 4, 1686. [Google Scholar] [CrossRef]
- Epskamp, S. semPlot: Unified Visualizations of Structural Equation Models. Struct. Equ. Model. Multidiscip. J. 2015, 22, 474–483. [Google Scholar] [CrossRef]
- Brown, T.A. Confirmatory Factor Analysis for Applied Research, 2nd ed.; The Guilford Press: New York, NY, USA, 2015. [Google Scholar]
- Hoyle, R.H. Handbook of Structural Equation Modeling, 2nd ed.; The Guilford Press: New York, NY, USA, 2023. [Google Scholar]
- Hu, L.; Bentler, P.M. Cutoff Criteria for Fit Indexes in Covariance Structure Analysis: Conventional Criteria versus New Alternatives. Struct. Equ. Model. Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Yu, C.-Y. Evaluating Cutoff Criteria of Model Fit Indices for Latent Variable Models with Binary and Continuous Outcomes. Doctoral Dissertation, University of California, Los Angeles, CA, USA, 2002. [Google Scholar]
- McDonald, R.P. Test Theory: A Unified Treatment; Lawrence Erlbaum Associates Publishers: Mahwah, NJ, USA, 1999. [Google Scholar]
- Tabachnick, B.G.; Fidell, L.S. Using Multivariate Statistics; Pearson: Harlow, UK, 2014. [Google Scholar]
- Howell, D.C. Statistical Methods for Psychology; Wadsworth, Cengage Learning: Belmont, CA, USA, 2013. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Arexis, M.; Feron, G.; Brindisi, M.C.; Billot, P.E.; Chambaron, S. A scoping review of emotion regulation and inhibition in emotional eating and binge-eating disorder: What about a continuum? J. Eat. Disord. 2023, 11, 197. [Google Scholar] [CrossRef]
- Tonelli, H.; de Siqueira Rotenberg, L. Emotion perception and theory of mind in obesity: A systematic review on the impact of social cognitive deficits on dysfunctional eating behaviors. Surg. Obes. Relat. Dis. 2021, 17, 618–629. [Google Scholar] [CrossRef] [PubMed]
- Christensen, K.A.; Haynos, A.F. A theoretical review of interpersonal emotion regulation in eating disorders: Enhancing knowledge by bridging interpersonal and affective dysfunction. J. Eat. Disord. 2020, 8, 21. [Google Scholar] [CrossRef]
- Leehr, E.J.; Krohmer, K.; Schag, K.; Dresler, T.; Zipfel, S.; Giel, K.E. Emotion regulation model in binge eating disorder and obesity--a systematic review. Neurosci. Biobehav. Rev. 2015, 49, 125–134. [Google Scholar] [CrossRef]
- Leppanen, J.; Brown, D.; McLinden, H.; Williams, S.; Tchanturia, K. The Role of Emotion Regulation in Eating Disorders: A Network Meta-Analysis Approach. Front. Psychiatry 2022, 13, 793094. [Google Scholar] [CrossRef]
- Prefit, A.B.; Candea, D.M.; Szentagotai-Tatar, A. Emotion regulation across eating pathology: A meta-analysis. Appetite 2019, 143, 104438. [Google Scholar] [CrossRef] [PubMed]
- Giusti, E.M.; Manna, C.; Scolari, A.; Mestre, J.M.; Prevendar, T.; Castelnuovo, G.; Pietrabissa, G. The Relationship between Emotional Intelligence, Obesity and Eating Disorder in Children and Adolescents: A Systematic Mapping Review. Int. J. Environ. Res. Public Health 2021, 18, 2054. [Google Scholar] [CrossRef]
- Baumeister, R.F.; Heatherton, T.F.; Tice, D.M.; Boekaerts, M.; Pintrich, P.R.; Zeidner, M. Losing control: How & why people fail at self-regulation and Handbook of selfregulation. J. Psychiatry Law 2002, 30, 283–284. [Google Scholar]
- Arnow, B.; Kenardy, J.; Agras, W.S. The Emotional Eating Scale: The development of a measure to assess coping with negative affect by eating. Int. J. Eat. Disord. 1995, 18, 79–90. [Google Scholar] [CrossRef]
- Panzeri, A.; Bettinardi, O.; Bottesi, G.; Bertolotti, G.; Brambatti, L.; Monfredo, M.; Mignemi, G.; Bruno, G.; Vidotto, G.; Spoto, A.; et al. Assessment of perceived support in the context of emergency: Development and validation of the psycho-social support scale. Curr. Psychol. 2023, 42, 22514–22525. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Descriptive Statistics | Properties | CFA | |||||
|---|---|---|---|---|---|---|---|
| M | SD | Sk | K | rit-tot | λ | R2 | |
| Social | |||||||
| Item#3 | 2.112 | 0.971 | 0.695 | −0.156 | 0.694 | 0.750 | 0.563 |
| Item#5 | 1.555 | 0.801 | 1.584 | 2.544 | 0.550 | 0.622 | 0.387 |
| Item#11 | 1.719 | 0.867 | 1.177 | 1.030 | 0.665 | 0.745 | 0.555 |
| Item#14 | 1.891 | 0.994 | 0.927 | −0.051 | 0.706 | 0.793 | 0.630 |
| Item#16 | 2.524 | 1.103 | 0.402 | −0.721 | 0.624 | 0.689 | 0.474 |
| Coping | |||||||
| Item#1 | 1.802 | 0.939 | 1.339 | 1.561 | 0.754 | 0.779 | 0.607 |
| Item#4 | 2.123 | 1.124 | 0.880 | −0.036 | 0.867 | 0.921 | 0.848 |
| Item#6 | 2.222 | 1.091 | 0.860 | 0.104 | 0.775 | 0.832 | 0.692 |
| Item#15 | 2.055 | 1.094 | 0.974 | 0.190 | 0.817 | 0.865 | 0.749 |
| Item#17 | 1.630 | 0.972 | 1.627 | 1.961 | 0.734 | 0.756 | 0.571 |
| Reward enhancement | |||||||
| Item#7 | 2.644 | 1.220 | 0.333 | −0.870 | 0.738 | 0.838 | 0.701 |
| Item#9 | 1.508 | 0.840 | 1.857 | 3.384 | 0.516 | 0.541 | 0.292 |
| Item#10 | 1.300 | 0.679 | 2.674 | 7.903 | 0.363 | 0.391 | 0.153 |
| Item#13 | 2.713 | 1.195 | 0.328 | −0.854 | 0.732 | 0.836 | 0.698 |
| Item#18 | 3.112 | 1.276 | −0.060 | −1.152 | 0.638 | 0.739 | 0.546 |
| Conformity | |||||||
| Item#2 | 1.880 | 0.903 | 1.024 | 0.617 | 0.274 | 0.317 | 0.100 |
| Item#8 | 1.170 | 0.555 | 4.298 | 21.771 | 0.600 | 0.733 | 0.537 |
| Item#12 | 1.367 | 0.700 | 2.268 | 5.746 | 0.636 | 0.756 | 0.572 |
| Item#19 | 1.170 | 0.486 | 3.470 | 14.535 | 0.625 | 0.748 | 0.560 |
| Item#20 | 1.185 | 0.527 | 3.711 | 17.259 | 0.641 | 0.807 | 0.651 |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | PEMS-SM | - | ||||||||||||||
| 2 | PEMS-CM | 0.203 *** | - | |||||||||||||
| 3 | PEMS-REM | 0.447 *** | 0.436 *** | - | ||||||||||||
| 4 | PEMS-CM | 0.546 *** | 0.151 *** | 0.129 ** | - | |||||||||||
| 5 | mYFAS2.0 | −0.004 | 0.426 *** | 0.113 * | 0.063 | - | ||||||||||
| 6 | BES | 0.028 | 0.587 *** | 0.229 *** | 0.163 ** | 0.740 *** | - | |||||||||
| 7 | MEC10-IT | 0.110 | 0.554 *** | 0.248 *** | 0.149 * | 0.492 *** | 0.804 *** | - | ||||||||
| 8 | TFEQ-CR | 0.015 | −0.068 | −0.065 | 0.001 | 0.322 *** | 0.402 *** | 0.363 *** | - | |||||||
| 9 | TFEQ-UE | 0.084 | 0.498 *** | 0.343 *** | 0.088 | 0.439 *** | 0.656 *** | 0.775 *** | −0.018 | - | ||||||
| 10 | TFEQ-EE | 0.122 * | 0.772 *** | 0.255 *** | 0.157 ** | 0.395 *** | 0.624 *** | 0.688 *** | −0.038 | 0.602 *** | - | |||||
| 11 | Rep(Eat)-Q | 0.153 *** | 0.528 *** | 0.282 *** | 0.146 ** | 0.437 *** | 0.601 *** | 0.599 *** | −0.077 | 0.574 *** | 0.636 *** | - | ||||
| 12 | Rep(Eat)-Q-RE | 0.104 * | 0.407 *** | 0.247 *** | 0.097 * | 0.273 *** | 0.405 *** | 0.407 *** | −0.061 | 0.449 *** | 0.508 *** | 0.903 *** | - | |||
| 13 | Rep(Eat)-Q-CG | 0.172 *** | 0.550 *** | 0.266 *** | 0.167 *** | 0.521 *** | 0.690 *** | 0.681 *** | −0.079 | 0.589 ** | 0.644 ** | 0.912 *** | 0.647 *** | - | ||
| 14 | BMI | −0.041 | 0.131 ** | −0.037 | −0.049 | 0.389 *** | 0.336 *** | 0.137 * | −0.071 | 0.098 * | 0.128 * | 0.048 | 0.025 | 0.062 | - | |
| 15 | Age | −0.152 ** | −0.085 * | −0.134 * | −0.157 ** | 0.134 * | 0.089 | −0.073 | 0.045 | −0.144 ** | −0.135 ** | −0.101 * | −0.092 * | −0.091 * | 0.349 *** | - |
| 16 | Sex (M/F) a | −0.005 | 0.180 *** | −0.025 | 0.064 | 0.061 | 0.183 *** | 0.089 | 0.156 ** | 0.065 | 0.204 *** | 0.092 * | 0.012 | 0.157 *** | −0.361 *** | −0.195 *** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pietrabissa, G.; Castelnuovo, G.; Semonella, M.; Mannarini, S.; Rossi, A.A. Measuring Motivations to Eat Palatable Foods: Adaptation and Psychometric Properties of the Italian Version of the Palatable Eating Motives Scale (PEMS-IT). Healthcare 2024, 12, 574. https://doi.org/10.3390/healthcare12050574
Pietrabissa G, Castelnuovo G, Semonella M, Mannarini S, Rossi AA. Measuring Motivations to Eat Palatable Foods: Adaptation and Psychometric Properties of the Italian Version of the Palatable Eating Motives Scale (PEMS-IT). Healthcare. 2024; 12(5):574. https://doi.org/10.3390/healthcare12050574
Chicago/Turabian StylePietrabissa, Giada, Gianluca Castelnuovo, Michelle Semonella, Stefania Mannarini, and Alessandro Alberto Rossi. 2024. "Measuring Motivations to Eat Palatable Foods: Adaptation and Psychometric Properties of the Italian Version of the Palatable Eating Motives Scale (PEMS-IT)" Healthcare 12, no. 5: 574. https://doi.org/10.3390/healthcare12050574
APA StylePietrabissa, G., Castelnuovo, G., Semonella, M., Mannarini, S., & Rossi, A. A. (2024). Measuring Motivations to Eat Palatable Foods: Adaptation and Psychometric Properties of the Italian Version of the Palatable Eating Motives Scale (PEMS-IT). Healthcare, 12(5), 574. https://doi.org/10.3390/healthcare12050574