
Effects of Continuous Glucose Monitoring on Glycemic Control in Type 2 Diabetes: A Systematic Review and Meta-Analysis


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Inclusion and Exclusion Criteria
2.3. Literature Search Strategy
2.4. Quality Assessment of the Selected Studies
2.5. Selection Process for the Analyzed Literature
2.6. Data Coding
2.7. Data Analysis
3. Results
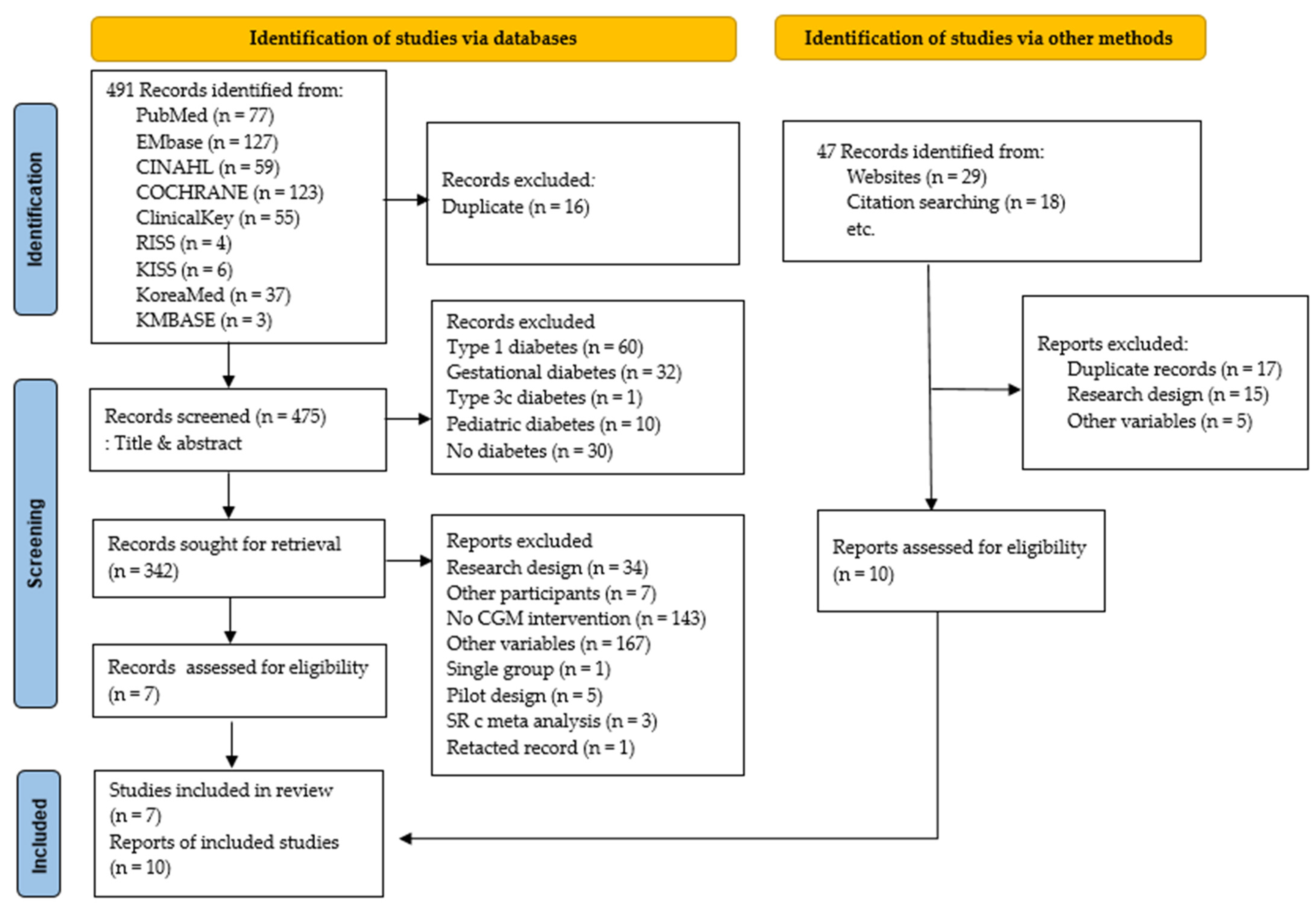
3.1. Literature Selection
3.2. Characteristics of the Included Studies
3.3. Quality Assessment
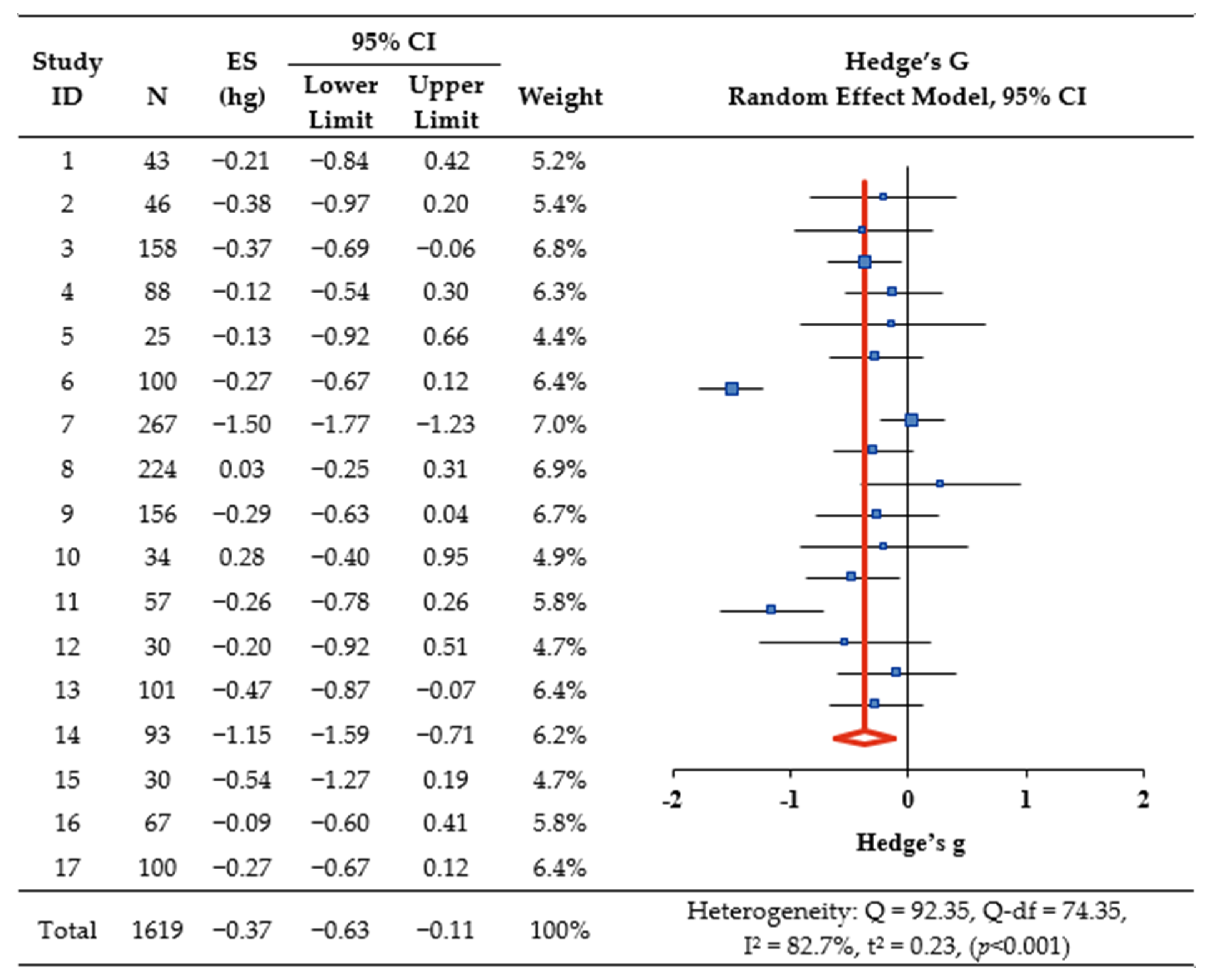
3.4. Effect of CGM Intervention on HbA1c
3.5. Effect of CGM Intervention on Secondary Outcomes
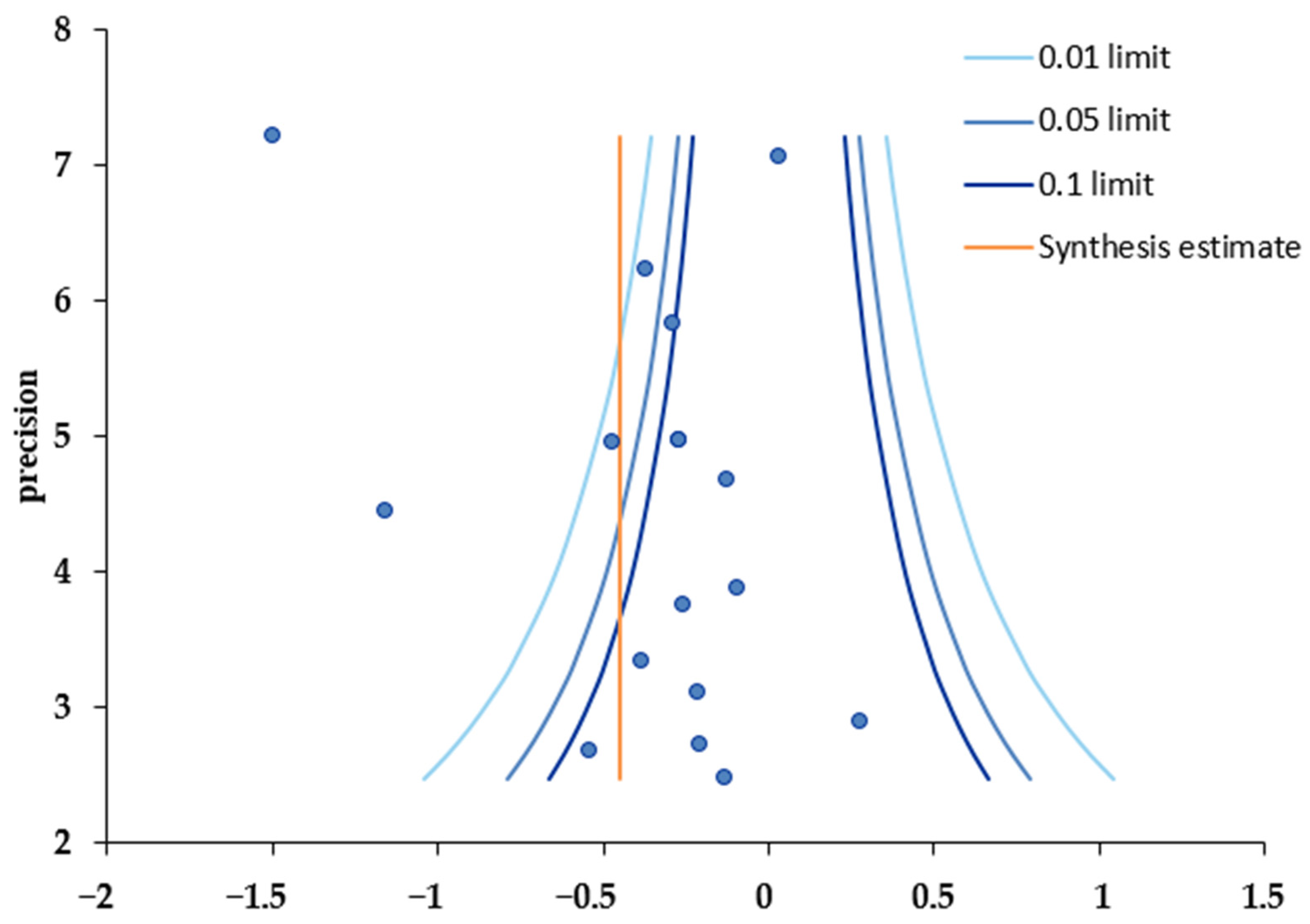
3.6. Publication Bias Analysis
4. Discussion
5. Conclusions and Recommendations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kwon, H.-S. Prevalence and treatment status of diabetes mellitus in Korea. J. Korean Med. Assoc. 2023, 66, 404–407. [Google Scholar] [CrossRef]
- Korean Diabetes Association. Diabetes Fact Sheet in Korea 2020; Korean Diabetes Association: Seoul, Republic of Korea, 2022; pp. 16–29. [Google Scholar]
- Kaptoge, S.; Seshasai, S.R.K.; Sun, L.; Walker, M.; Bolton, T.; Spackman, S.; Ataklte, F.; Willeit, P.; Bell, S.; Burgess, S.; et al. Life expectancy associated with different ages at diagnosis of type 2 diabetes in high-income countries: 23 million person-years of observation. Lancet Diabetes Endocrinol. 2023, 11, 731–742. [Google Scholar] [CrossRef]
- Ghandour, R.; Mikki, N.; Abu Rmeileh, N.M.E.; Jerdén, L.; Norberg, M.; Eriksson, J.W.; Husseini, A. Complications of type 2 diabetes mellitus in Ramallah and al-Bireh: The Palestinian diabetes complications and control study (PDCCS). Prim. Care Diabetes 2018, 12, 547–557. [Google Scholar] [CrossRef] [PubMed]
- Korean Diabetes Association. Available online: https://www.diabetes.or.kr/bbs/?code=guide&category=2023 (accessed on 1 June 2023).
- International Diabetes Federation. Available online: https://www.idf.org/aboutdiabetes/what-is-diabetes/facts-figures.html (accessed on 1 June 2023).
- Schnell, O.; Alawi, H.; Battelino, T.; Ceriello, A.; Diem, P.; Felton, A.-M.; Grzeszczak, W.; Harno, K.; Kempler, P.; Satman, I.; et al. Self-monitoring of blood glucose in type 2 diabetes: Recent studies. J. Diabetes Sci. Technol. 2013, 7, 478–488. [Google Scholar] [CrossRef]
- Lee, J.H. The occurrence and management of adverse skin events due to continuous glucose monitoring. J. Korean Diabetes 2022, 23, 43–49. [Google Scholar] [CrossRef]
- Boland, E.; Monsod, T.; Delucia, M.; Brandt, C.A.; Fernando, S.; Tamborlane, W.V. Limitations of conventional methods of self-monitoring of blood glucose. Diabetes Care 2001, 24, 1858–1862. [Google Scholar] [CrossRef] [PubMed]
- Bae, S.K. Development of Artificial Skin Phantom for Continuous Glucose Monitoring System. Master’s Thesis, Korea University Graduate School, Seoul, Republic of Korea, 2021. [Google Scholar]
- Rivera-Ávila, D.A.; Esquivel-Lu, A.I.; Salazar-Lozano, C.R.; Jones, K.; Doubova, S.V. The effects of professional continuous glucose monitoring as an adjuvant educational tool for improving glycemic control in patients with type 2 diabetes. BMC Endocr. Disord. 2021, 21, 79. [Google Scholar] [CrossRef] [PubMed]
- Allen, N.A.; Fain, J.A.; Braun, B.; Chipkin, S.R. Continuous glucose monitoring in non–insulin-using individuals with type 2 diabetes: Acceptability, feasibility, and teaching opportunities. Diabetes Technol. Ther. 2009, 11, 151–158. [Google Scholar] [CrossRef]
- Poolsup, N.; Suksomboon, N.; Kyaw, A.M. Systematic Review and meta-analysis of the effectiveness of continuous glucose monitoring (CGM) on glycemic control in diabetes. Diabetol Metab. Syndr. 2013, 5, 39. [Google Scholar] [CrossRef]
- Beck, R.W.; Riddlesworth, T.D.; Ruedy, K.; Ahmann, A.; Haller, S.; Kruger, D.; McGill, J.B.; Polonsky, W.; Price, D.; Aronoff, S.; et al. Continuous glucose monitoring versus usual care in patients with type 2 diabetes receiving multiple daily insulin injections. Ann. Intern. Med. 2017, 167, 365. [Google Scholar] [CrossRef]
- Karter, A.J.; Parker, M.M.; Moffet, H.H.; Gilliam, L.K.; Dlott, R. Association of real-time continuous glucose monitoring with glycemic control and acute metabolic events among patients with insulin-treated diabetes. JAMA 2021, 325, 2273. [Google Scholar] [CrossRef]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. Prisma 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef] [PubMed]
- Bidwell, S.; Jensen, M.F. Using a search protocol to identify sources of information: The COSI model. In Etext on Health Technology Assessment (HTA) Information Resources [Internet]; Topfer, L.A., Auston, I., Eds.; National Library of Medicine: Washington, DC, USA, 2003. Available online: https://www.nlm.nih.gov/archive/20060905/nichsr/ehta/chapter3.html#COSI (accessed on 1 June 2023).
- Joanna Briggs Institute. Available online: https://jbi.global/critical-appraisal-tools (accessed on 30 June 2023).
- Bax, L.; Yu, L.-M.; Ikeda, N.; Tsuruta, H.; Moons, K.G. Development and validation of MIX: Comprehensive Free Software for meta-analysis of causal research data. BMC Med. Res. Methodol. 2006, 6, 50. [Google Scholar] [CrossRef] [PubMed]
- Shim, S.R.; Kim, S.-J. Intervention meta-analysis: Application and practice using R software. Epidemiol. Health 2019, 41, e2019008. [Google Scholar] [CrossRef] [PubMed]
- Hedges, L.V.; Olkin, I. Statistical Methods for Meta-Analysis; Academic Press: San Diego, CA, USA, 2002. [Google Scholar]
- Higgins, J.P. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Littell, J.H.; Corcoran, J.; Pillai, V.K. Systematic Reviews and Meta-Analysis; Oxford University Press: New York, NY, USA, 2008. [Google Scholar]
- Mavridis, D.; Salanti, G. How to assess publication bias: Funnel Plot, trim-and-fill method and selection models. BMJ Mental Health 2014, 17, 30. [Google Scholar] [CrossRef]
- Ajjan, R.A.; Abougila, K.; Bellary, S.; Collier, A.; Franke, B.; Jude, E.B.; Rayman, G.; Robinson, A.; Singh, B.M. Sensor and software use for the glycaemic management of insulin-treated type 1 and type 2 diabetes patients. Diabetes. Vasc. Dis. Res. 2016, 13, 211–219. [Google Scholar] [CrossRef]
- Blackberry, I.D.; Furler, J.S.; Ginnivan, L.E.; Manski-Nankervis, J.-A.; Jenkins, A.; Cohen, N.; Best, J.D.; Young, D.; Liew, D.; Ward, G.; et al. An exploratory trial of basal and prandial insulin initiation and titration for type 2 diabetes in primary care with adjunct retrospective continuous glucose monitoring: Initiation Study. Diabetes Res. Clin. Pract. 2014, 106, 247–255. [Google Scholar] [CrossRef]
- Cosson, E.; Hamo-Tchatchouang, E.; Dufaitre-Patouraux, L.; Attali, J.-R.; Pariès, J.; Schaepelynck-Bélicar, P. Multicentre, randomised, controlled study of the impact of continuous sub-cutaneous glucose monitoring (GlucoDay®) on glycaemic control in type 1 and type 2 diabetes patients. Diabetes Metab. 2009, 35, 312–318. [Google Scholar] [CrossRef]
- Ehrhardt, N.M.; Chellappa, M.; Walker, M.S.; Fonda, S.J.; Vigersky, R.A. The effect of real-time continuous glucose monitoring on glycemic control in patients with type 2 diabetes mellitus. J. Diabetes Sci. Technol. 2011, 5, 668–675. [Google Scholar] [CrossRef] [PubMed]
- Furler, J.; O’Neal, D.; Speight, J.; Blackberry, I.; Manski-Nankervis, J.-A.; Thuraisingam, S.; de La Rue, K.; Ginnivan, L.; Doyle, R.; Holmes-Truscott, E.; et al. Use of professional-mode flash glucose monitoring, at 3-month intervals, in adults with type 2 diabetes in general practice (GP-osmotic): A Pragmatic, open-label, 12-month, randomised controlled trial. Lancet Diabetes Endocrinol. 2020, 8, 17–26. [Google Scholar] [CrossRef]
- Haak, T.; Hanaire, H.; Ajjan, R.; Hermanns, N.; Riveline, J.-P.; Rayman, G. Flash glucose-sensing technology as a replacement for blood glucose monitoring for the management of insulin-treated type 2 diabetes: A Multicenter, open-label Randomized Controlled Trial. Diabetes Ther. 2016, 8, 55–73. [Google Scholar] [CrossRef] [PubMed]
- Martens, T.; Beck, R.W.; Bailey, R.; Ruedy, K.J.; Calhoun, P.; Peters, A.L.; Pop-Busui, R.; Philis-Tsimikas, A.; Bao, S.; Umpierrez, G.; et al. Effect of continuous glucose monitoring on glycemic control in patients with type 2 diabetes treated with basal insulin. JAMA 2021, 325, 2262–2272. [Google Scholar] [CrossRef] [PubMed]
- Sato, J.; Kanazawa, A.; Ikeda, F.; Shigihara, N.; Kawaguchi, M.; Komiya, K.; Uchida, T.; Ogihara, T.; Mita, T.; Shimizu, T.; et al. Effect of treatment guidance using a retrospective continuous glucose monitoring system on glycaemic control in outpatients with type 2 diabetes mellitus: A randomized controlled trial. J. Int. Med. Res. 2015, 44, 109–121. [Google Scholar] [CrossRef] [PubMed]
- Yoo, H.J.; An, H.G.; Park, S.Y.; Ryu, O.H.; Kim, H.Y.; Seo, J.A.; Hong, E.G.; Shin, D.H.; Kim, Y.H.; Kim, S.G.; et al. Use of a real time continuous glucose monitoring system as a motivational device for poorly controlled type 2 diabetes. Diabetes Res. Clin. Pract. 2008, 82, 73–79. [Google Scholar] [CrossRef] [PubMed]
- Yeoh, E.; Lim, B.K.; Fun, S.; Tong, J.; Yeoh, L.Y.; Sum, C.F.; Subramaniam, T.; Lim, S.C. Efficacy of self-monitoring of blood glucose versus retrospective continuous glucose monitoring in improving glycaemic control in diabetic kidney disease patients. Nephrology 2018, 23, 264–268. [Google Scholar] [CrossRef]
- Ajjan, R.A.; Jackson, N.; Thomson, S.A. Reduction in hba1c using professional flash glucose monitoring in insulin-treated type 2 diabetes patients managed in primary and secondary care settings: A pilot, multicentre, randomised controlled trial. Diabetes Vasc. Dis. Res. 2019, 16, 385–395. [Google Scholar] [CrossRef] [PubMed]
- Wada, E.; Onoue, T.; Kobayashi, T.; Handa, T.; Hayase, A.; Ito, M.; Furukawa, M.; Okuji, T.; Okada, N.; Iwama, S.; et al. Flash glucose monitoring helps achieve better glycemic control than conventional self-monitoring of blood glucose in non-insulin-treated type 2 diabetes: A randomized controlled trial. BMJ Open Diabetes Res. Care 2020, 8, e001115. [Google Scholar] [CrossRef]
- Moon, S.J.; Kim, K.; Lee, W.J.; Lee, M.Y.; Vigersky, R.; Park, C. Efficacy of intermittent short-term use of a real-time continuous glucose monitoring system in non-insulin–treated patients with type 2 diabetes: A randomized controlled trial. Diabetes Obes Metab. 2022, 25, 110–120. [Google Scholar] [CrossRef]
- Price, D.A.; Deng, Q.; Kipnes, M.; Beck, S.E. Episodic real-time CGM use in adults with type 2 diabetes: Results of a pilot randomized controlled trial. Diabetes Ther. 2021, 12, 2089–2099. [Google Scholar] [CrossRef]
- Vigersky, R.A.; Fonda, S.J.; Chellappa, M.; Walker, M.S.; Ehrhardt, N.M. Short- and long-term effects of real-time continuous glucose monitoring in patients with type 2 diabetes. Diabetes Care 2011, 35, 32–38. [Google Scholar] [CrossRef]
- Kim, W.J.; Kim, J.H.; Yoo, H.J.; Son, J.W.; Khang, A.R.; Kwon, S.K.; Kim, J.H.; Kim, T.H.; Ryu, O.H.; Park, K.H.; et al. A position statement of the utilization and support status of continuous glucose monitoring in Korea. J. Korean Diabetes 2021, 22, 225–237. [Google Scholar] [CrossRef]
- Janapala, R.N.; Jayaraj, J.S.; Fathima, N.; Kashif, T.; Usman, N.; Dasari, A.; Jahan, N.; Sachmechi, I. Continuous glucose monitoring versus self-monitoring of blood glucose in type 2 diabetes mellitus: A systematic review with meta-analysis. Cureus 2019, 11, e5634. [Google Scholar] [CrossRef]
- Ida, S.; Kaneko, R.; Murata, K. Utility of real-time and retrospective continuous glucose monitoring in patients with type 2 diabetes mellitus: A meta-analysis of randomized controlled trials. J. Diabetes Res. 2019, 2019, 4684815. [Google Scholar] [CrossRef]
- Edelman, S.V.; Argento, N.B.; Pettus, J.; Hirsch, I.B. Clinical implications of real-time and intermittently scanned continuous glucose monitoring. Diabetes Care 2018, 41, 2265–2274. [Google Scholar] [CrossRef]
- Petrie, J.R.; Peters, A.L.; Bergenstal, R.M.; Holl, R.W.; Fleming, G.A.; Heinemann, L. Improving the clinical value and utility of CGM systems: Issues and recommendations. Diabetes Care 2017, 40, 1614–1621. [Google Scholar] [CrossRef] [PubMed]
- Kim, K. The influencing factors associated with glycemic control among adult diabetes patients. J. Korea Acad.-Ind. Coop. Soc. 2015, 16, 3284–3292. [Google Scholar] [CrossRef]
- Harrabi, I.; Harbi, F.A.; Ghamdi, S.A. Predictors of glycemic control among patients with type 2 diabetes in Najran Armed Forces Hospital: A pilot study. J. Diabetes Mellit. 2014, 04, 141–147. [Google Scholar] [CrossRef]
- Inolopú, J.; Hilario-Huapaya, N.; Tantaleán-Del-Águila, M.A.; Hurtado-Roca, Y.; Ugarte-GilI, C. Interventions for the prevention of risk factors and incidence of type 2 diabetes in the work environment: A systematic review. Rev. Saúde Pública 2019, 53, 101. [Google Scholar] [CrossRef]
- Sequeira, P.A.; Montoya, L.; Ruelas, V.; Xing, D.; Chen, V.; Beck, R.; Peters, A.L. Continuous glucose monitoring pilot in low-income type 1 diabetes patients. Diabetes Technol. Therap. 2013, 15, 855–858. [Google Scholar] [CrossRef] [PubMed]
- PRISMA Transparent Reporting of Systematic Reviews and Meta-Analyses. PRISMA 2020 Checklist. Available online: http://www.prisma-statement.org/ (accessed on 23 January 2024).


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study ID | Author | Year | Country | Center | Fund | Participants | Characteristics of Participants | Type of CGM | Intervention Period (Weeks) | Comparator | Outcome Variables |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Ajjan et al. [25] | 2016 | UK | 9 | Yes | N = 45 (E:30, C:15) | Age ≥ 18 years HbA1c 7.5–12.0% Receiving insulin therapy > 6 months | FreeStyle Navigator (Abbott, Chicago, IL, USA) | 25 | SMBG | CGM data HbA1c Body weight (kg) Blood glucose testing Frequency (tests/day) |
| 2 | Allen et al. [12] | 2008 | US | 2 | Yes | N = 46 (E:21, C:25) | Age > 20 years HbA1c > 7.5% Physical activity ≤2 days/week Not receiving insulin therapy | Minimed (Medtronic, Northridge, CA, USA) | 8 | SMBG | HbA1c Physical activity Self-efficacy BP, BMI |
| 3 | Beck et al. [14] | 2017 | US | 25 | Yes | N = 158 (E:79, C:79) | Age > 25 years HbA1c 7.5–10.0% Receiving insulin therapy > 1 year Stable medication regimen and weight >3 months SMBG ≥ 2/day Estimated glomerular filtration rate > 45 mL/min/1.73 m2 | Dexcom G4 Platinum (Dexcom, San Diego, CA, USA) | 24 | SMBG | HbA1c Hypoglycemia QoL |
| 4 | Blackberry et al. [26] | 2014 | Australia | 22 | Yes | N = 88 (E:46, C:42) | Age 18–80 years HbA1c ≥ 7.5% No previous experience with insulin therapy Stable OHA regimen > prior 3 months SMBG ≥ 2/day | iPro2TM (Medtronic, Northridge, CA, USA) | 24 | SMBG | HbA1c QoL CGM satisfaction 36 Health survey questionnaire version 2 (SF-36 v2) |
| 5 | Cosson et al. [27] | 2009 | France | 5 | Yes | N = 25 (E:11, C:14) | Age 40–70 years HbA1c 8.0–10.5% Stable OHA and insulin regimen prior to >3 months SMBG ≥ 4/week No previous experience with CGM | The GlucoDay system (Menarini Diagnostics, Florence, Italy) | 12 | SMBG | HbA1c Glycemic control (Changes in 48 h CGM data) Hypoglycemia |
| 6 | Ehrhardt et al. [28] | 2011 | US | 1 | Yes | N = 100 (E:50, C:50) | Age ≥ 18 years HbA1c 7.0–12.0% Diagnosis ≥ 3 months SMBG 4/day Treated with diet or exercise Not receiving prandial insulin | DexComTM SEVEN (DexCom) | 12 | SMBG | HbA1c Glycemic control Weight BP Stress |
| 7 | Furler et al. [29] | 2020 | Australia | 25 | Yes | N = 299 (E:149, C:150) | Age 18–80 years HbA1c ≥ 7.0% Diagnosis ≥ 1 year Receiving OHA or Insulin therapy | FreeStyle Libre Pro (Abbott) | 52 | SMBG | HbA1c CGM data Distress |
| 8 | Haak et al. [30] | 2016 | European | 26 | Yes | N = 224 (E:149, C:75) | Age ≥ 18 years HbA1c 7.5–12.0% Receiving insulin therapy ≥ 6 months (current regimen ≥ 3M SMBG ≥ 10/week at least 2 months | FreeStyle LibreTM (Abbott) | 24 | SMBG | HbA1c CGM data QoL |
| 9 | Martens et al. [31] | 2021 | US | 15 | Yes | N = 156 (E:105, C:51) | Age ≥ 30 years HbA1c 7.8–11.5% Diagnosis and insulin therapy ≥ 6 months SMBG ≥ 3/week | Dexcom G6 (Dexcom) | 32 | SMBG | HbA1c Height Weight Cholesterol CGM satisfaction |
| 10 | Sato et al. [32] | 2016 | Japan | 1 | Yes | N = 34 (E:17, C:17) | Age > 20 years HbA1c 6.9–11.0% Receiving insulin therapy | iPro® 2 (Medtronic) | 32 | SMBG | HbA1c Diabetes Treatment Satisfaction (DTSQ) |
| 11 | Yoo et al. [33] | 2008 | Korea | 1 | Yes | N = 57 (E:29, C:28) | Age 20–80 years HbA1c 8.0–10.0% Receiving OHA or insulin therapy ≥ 1 year Stable insulin or OHA regimen ≥ prior 2 months Stable OHA or lipid-lowering drugs ≥4 weeks | Guardian RT (Medtronic) | 12 | SMBG | HbA1c FBS, PP2, Lipid profiles, Weight, Waist circumference BMI, Fat consumption Cholesterol intake (g/day) Exercise time (min/week) |
| 12 | Yeoh et al. [34] | 2018 | Singapore | 1 | Yes | N = 30 (E:14, C:16) | Age ≥ 21 years HbA1c > 8% Type 2 diabetes with CKD stage 3 (eGFR 30–60 mL/min per 1.73 m2) Above (pre-dialysis) for >3 months Sustained for >6 months Receiving insulin and/or OHA | iPro device (Medtronic) | 12 | SMBG | HbA1c CGM data |
| 13 | Ajjan et al. [35] | 2019 | England | 22 | No | N = 102 (E:50, C:52) | Age ≥ 18 years HbA1c 7.5%–12.0% Receiving insulin therapy ≥ 6 month | FreeStyle Libre ProTM (Abbott) | 28 | SMBG | HbA1c CGM data Treatment satisfaction (DTSQ) |
| 14 | Wada et al. [36] | 2020 | Japan | 5 | Yes | N = 93 (E:48, C:45) | Age 20–70 years HbA1c 7.5–8.5% | Free Style Libre (Abbott) | 24 | SMBG | HbA1c Weight, BP Diabetes medication change (DTSQ) |
| 15 | Moon et al. [37] | 2022 | Korea | 3 | Yes | N = 30 (E:15, C:15) | Aged 30 to 65 years HbA1c 7.5–10.0% Receiving OHA Treated without insulin ≥ 3 months | Guardian 3 (Medtronic MiniMed, Northridge, CA, USA) | 24 | SMBG | HbA1c CGM data, BP Lipid variables, Weight, Satisfaction K-DMSES, ADS-K, SDSCA-K |
| 16 | Price et al. [38] | 2021 | US | 8 | Yes | N = 68 (E:45, C:23) | Age ≥ 30 years HbA1c 7.8–10.5% Treated with two or more noninsulin antidiabetic drugs Stable body weight over the past 3 months | Dexcom G6 (Dexcom) | 12 | SMBG | CGM data HbA1c Adverse Events |
| 17 | Vigersky et al. [39] | 2012 | US | 1 | Yes | N = 100 (E:50, C:50) | Age ≥ 18 years HbA1c 7.0–12.0% Diagnosis ≥ 3 months Not receiving prandial insulin SMGB 4/days | DexCom SEVEN (DexCom) | 12 | SMBG | HbA1c Weight BP Stress |
| Joanna Briggs Institute of Critical Appraisal Tools Checklist for Randomized Controlled Trials | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Study ID | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | Total Score |
| 1 | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 8 |
| 2 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 9 |
| 3 | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 8 |
| 4 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 8 |
| 5 | 1 | 1 | 0 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 9 |
| 6 | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 6 |
| 7 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 9 |
| 8 | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 8 |
| 9 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 9 |
| 10 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 9 |
| 11 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 9 |
| 12 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 6 |
| 13 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 8 |
| 14 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 8 |
| 15 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 9 |
| 16 | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 7 |
| 17 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 6 |
| Total | 13 | 12 | 11 | 0 | 1 | 1 | 17 | 17 | 17 | 17 | 0 | 13 | 17 | 8 |
| Characteristics | Subgroup | K | Study ID | N | Overall ES | 95% CI | Z (p) | |
|---|---|---|---|---|---|---|---|---|
| Lower Limit | Upper Limit | |||||||
| Location (country of publication) | US | 6 | 2,3,6,9,16,17 | 627 | −0.29 | −0.45 | −0.13 | −3.57 (<0.001) |
| others | 11 | 1,4,5,7,8,10, 11,12,13,14,15 | 992 | −0.41 | −0.82 | 0.00 | −1.98 (0.048) | |
| Participants | <60 | 7 | 1,2,5,10, 11,12,15 | 265 | −0.22 | −0.46 | 0.03 | −1.74 (0.082) |
| ≥60 | 10 | 3,4,6,7,8,9, 13,14,16,17 | 1354 | −0.46 | −0.81 | −0.11 | −2.56 (0.011) | |
| Study centers | 1 | 5 | 6,10,11,12,17 | 321 | −0.21 | −0.43 | 0.01 | −1.83 (0.067) |
| multiple | 12 | 1,2,3,4,5,7,8, 9,13,14,15,16 | 1298 | −0.45 | −0.78 | −0.12 | −2.65 (0.008) | |
| Intervention | r-CGM | 6 | 1,2,5,8,10,30 | 402 | −0.05 | −0.25 | 0.15 | −0.49 (0.621) |
| rt-CGM | 11 | 3,4,6,7,9,11, 13,14,15,16,17 | 1217 | −0.50 | −0.81 | −0.18 | −3.04 (0.002) | |
| Intervention period (week) | ≤24 | 7 | 2,5,6,11, 12,16,17 | 425 | −0.24 | −0.44 | −0.05 | −2.47 (0.013) |
| >24 | 10 | 1,3,4,7,8,9, 10,13,14,15 | 1194 | −0.45 | −0.84 | −0.07 | −2.30 (0.022) | |
| Quality score | ≤8 | 10 | 1,3,4,6,8,12,13, 14,16,17 | 1004 | −0.31 | −0.52 | −0.10 | −2.94 (0.003) |
| >8 | 7 | 2,5,7,9,10,11,15 | 615 | −0.43 | −0.98 | 0.12 | −1.54 (0.124) | |
| Insulin therapy | Yes | 11 | 1,3,5,7,8,9,10, 11,12,13,14 | 1188 | −0.42 | −0.79 | −0.05 | −2.21 (0.027) |
| No | 6 | 2,4,6,15,16,17 | 431 | −0.25 | −0.44 | −0.05 | −2.51 (0.012) | |
| Covariate (Ref.) | Estimate | SE | Z | p |
|---|---|---|---|---|
| Location (country of publication; Ref.: others) US | 0.26 | 0.11 | 2.49 | 0.013 |
| Participants (Ref.: <60) ≥ 60 | −0.28 | 0.14 | −2.06 | 0.039 |
| Study centers (Ref.: multicenter) one | 0.31 | 0.13 | 2.47 | 0.013 |
| Intervention (Ref.: r-CGM) rt-CGM | −0.53 | 0.12 | −4.45 | <0.001 |
| Intervention period (Ref.: week > 24) ≤ 24 | 0.29 | 0.12 | 2.49 | 0.013 |
| Quality assessment (Ref.: >8) ≤ 8 | −0.45 | 0.11 | −4.15 | <0.001 |
| Receiving insulin therapy (Ref.: not receiving) | −0.29 | 0.12 | −2.49 | 0.013 |
| Variables | Number of Studies | N | Hedge’s G | 95% CI | Z (p) | I2 (%) | |
|---|---|---|---|---|---|---|---|
| Lower Limit | Upper Limit | ||||||
| Weight | 6 (1,3,6,9,11,17) | 593 | −0.52 | −1.22 | 0.18 | −1.46 (0.145) | 93.7 |
| BMI | 4 (2,9,11,17) | 330 | −0.04 | −0.27 | 0.20 | −0.30 (0.764) | 10.1 |
| Glucose | 6 (3,5,8,9,10,13) | 688 | −0.14 | −0.40 | 0.11 | −1.12 (0.263) | 56.3 |
| SBP | 4 (2,6,9,17) | 374 | −0.12 | −0.34 | 0.10 | −1.09 (0.274) | 4.8 |
| DBP | 4 (2,6,9,17) | 341 | 0.07 | −0.15 | 0.29 | 0.63 (0.527) | 0 |
| TIR | 10 (3,4,5,7,8,9,10,13,15,16) | 1110 | 0.31 | −0.14 | 0.75 | 1.35 (0.177) | 91.3 |
| Hyperglycemia | 10 (1,3,4,5,8,9,10,13,15,16) | 908 | −0.20 | −0.49 | 0.09 | −1.35 (0.178) | 74.6 |
| Hypoglycemia | 10 (1,3,4,5,8,9,10,13,15,16) | 898 | −0.19 | −0.52 | 0.13 | −1.16 (0.246) | 79.7 |
| HDL-cholesterol | 2 (9,11) | 194 | −0.33 | −0.68 | 0.03 | −1.78 (0.075) | 25.9 |
| Distress | 3 (3,7,17) | 510 | −0.08 | −0.36 | 0.20 | −0.56 (0.574) | 57.8 |
| QoL | 3 (3,4,8) | 462 | −1.29 | −3.87 | 1.29 | −0.98 (0.326) | 99.2 |
| Satisfaction | 3 (8,10,13) | 359 | 2.77 | −1.18 | 6.72 | 1.38 (0.169) | 99.2 |
| Publication Bias Test | Coefficient | SE | 95% CI | Z | p | ||
|---|---|---|---|---|---|---|---|
| Lower Limit | Upper Limit | ||||||
| Egger’s regression test | intercept | 2.23 | 1.83 | −1.35 | 5.81 | 1.22 | 0.222 |
| slope | −0.90 | 0.39 | −1.67 | −0.14 | −2.31 | 0.021 | |
| tau-b | ties | Z | p | ||||
| Begg’s test | standard | −0.05 | 4 | −0.29 | 0.771 | ||
| corrected | −0.04 | 4 | −0.25 | 0.805 | |||
| Hedge’s | 95% CI | ||||||
| Lower Limit | Upper Limit | ||||||
| Trim and fill | original | −0.36 | −0.62 | −0.10 | |||
| corrected | −0.58 | −0.83 | −0.33 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kong, S.-Y.; Cho, M.-K. Effects of Continuous Glucose Monitoring on Glycemic Control in Type 2 Diabetes: A Systematic Review and Meta-Analysis. Healthcare 2024, 12, 571. https://doi.org/10.3390/healthcare12050571
Kong S-Y, Cho M-K. Effects of Continuous Glucose Monitoring on Glycemic Control in Type 2 Diabetes: A Systematic Review and Meta-Analysis. Healthcare. 2024; 12(5):571. https://doi.org/10.3390/healthcare12050571
Chicago/Turabian StyleKong, Seung-Yeon, and Mi-Kyoung Cho. 2024. "Effects of Continuous Glucose Monitoring on Glycemic Control in Type 2 Diabetes: A Systematic Review and Meta-Analysis" Healthcare 12, no. 5: 571. https://doi.org/10.3390/healthcare12050571
APA StyleKong, S.-Y., & Cho, M.-K. (2024). Effects of Continuous Glucose Monitoring on Glycemic Control in Type 2 Diabetes: A Systematic Review and Meta-Analysis. Healthcare, 12(5), 571. https://doi.org/10.3390/healthcare12050571