_Rachiotis.png)
Associations between COVID-19 Pandemic-Related Overtime, Perceived Chronic Stress and Burnout Symptoms in German General Practitioners and Practice Personnel—A Prospective Study

 , and
, and
Abstract
1. Introduction
1.1. Chronic Stress in General Practice
1.2. Burnout in General Practice
1.3. Sources for Chronic Stress and Burnout
1.4. Mental Health Impact of the COVID-19 Pandemic
1.5. The IMPROVEjob Trial
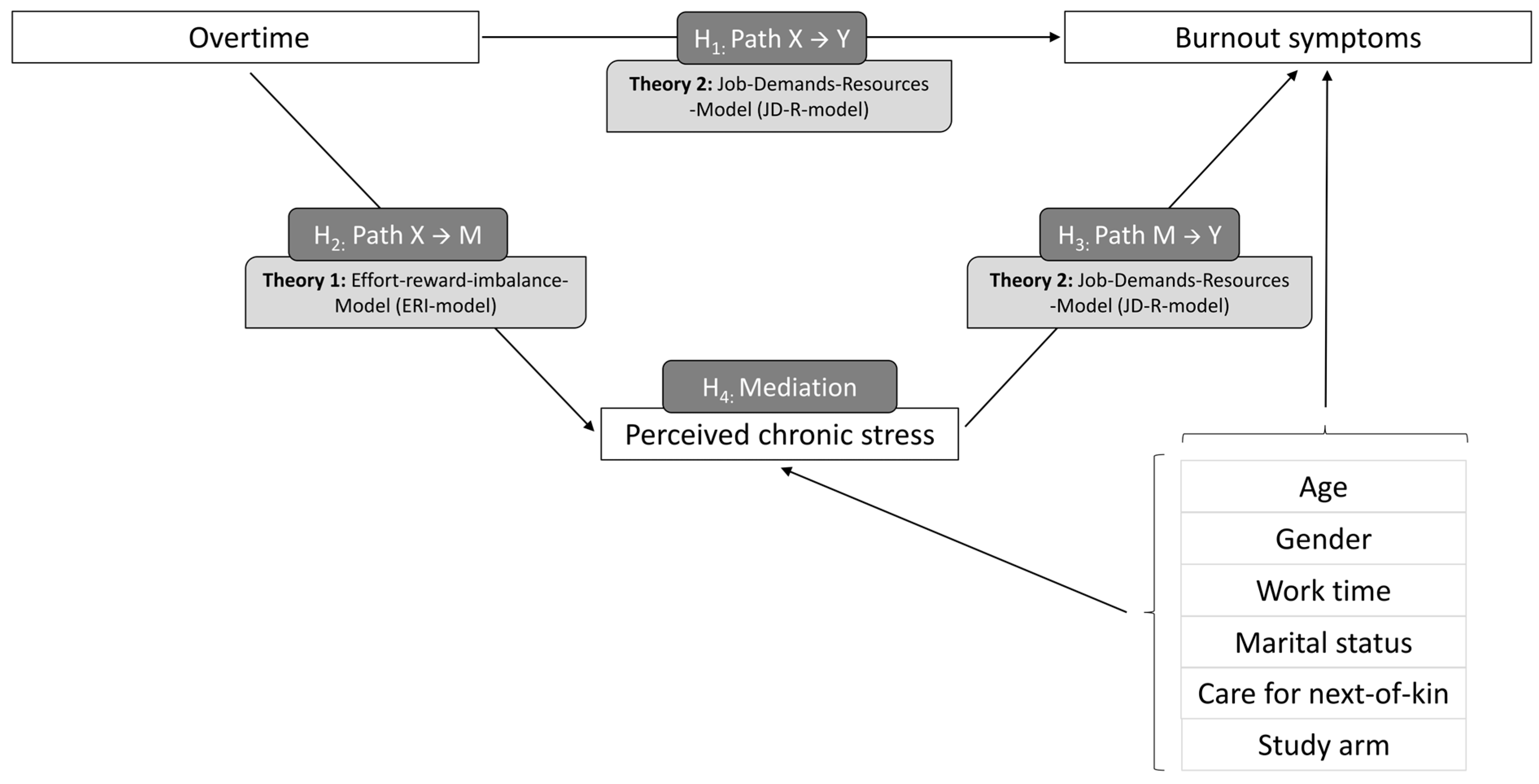
1.6. Theory, Hypothesis, and Research Question
2. Materials and Methods
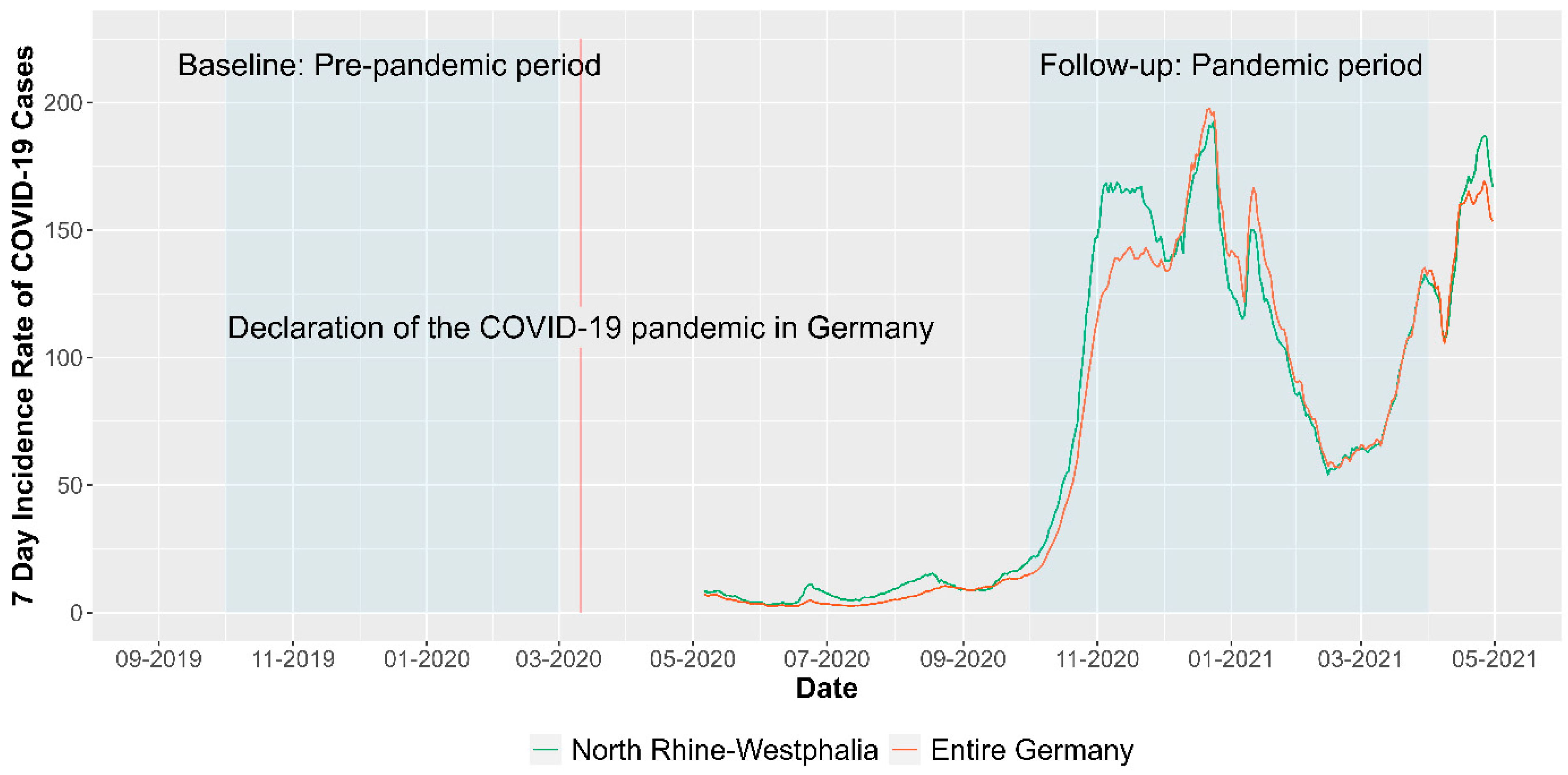
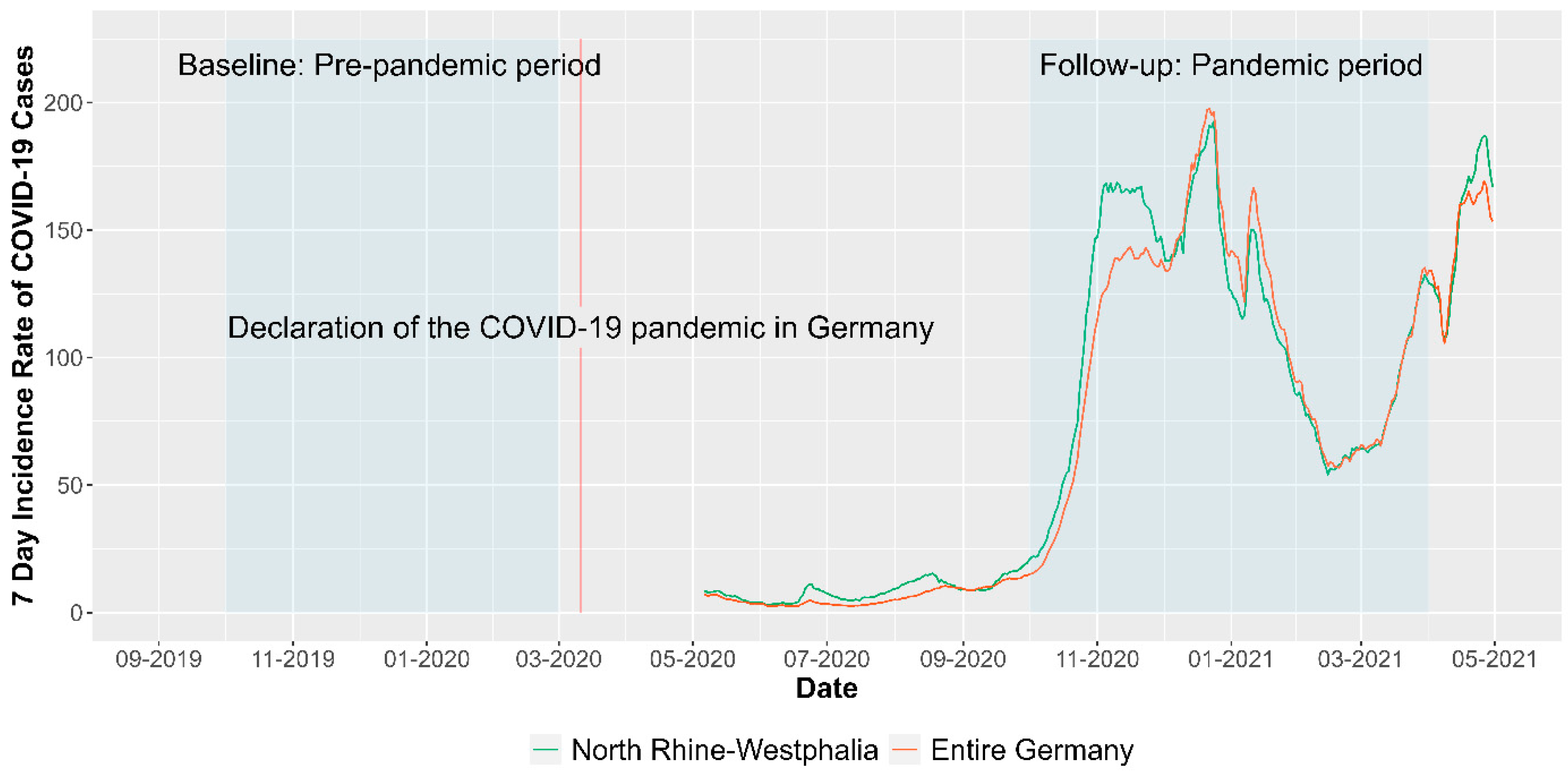
2.1. Study Design and Setting
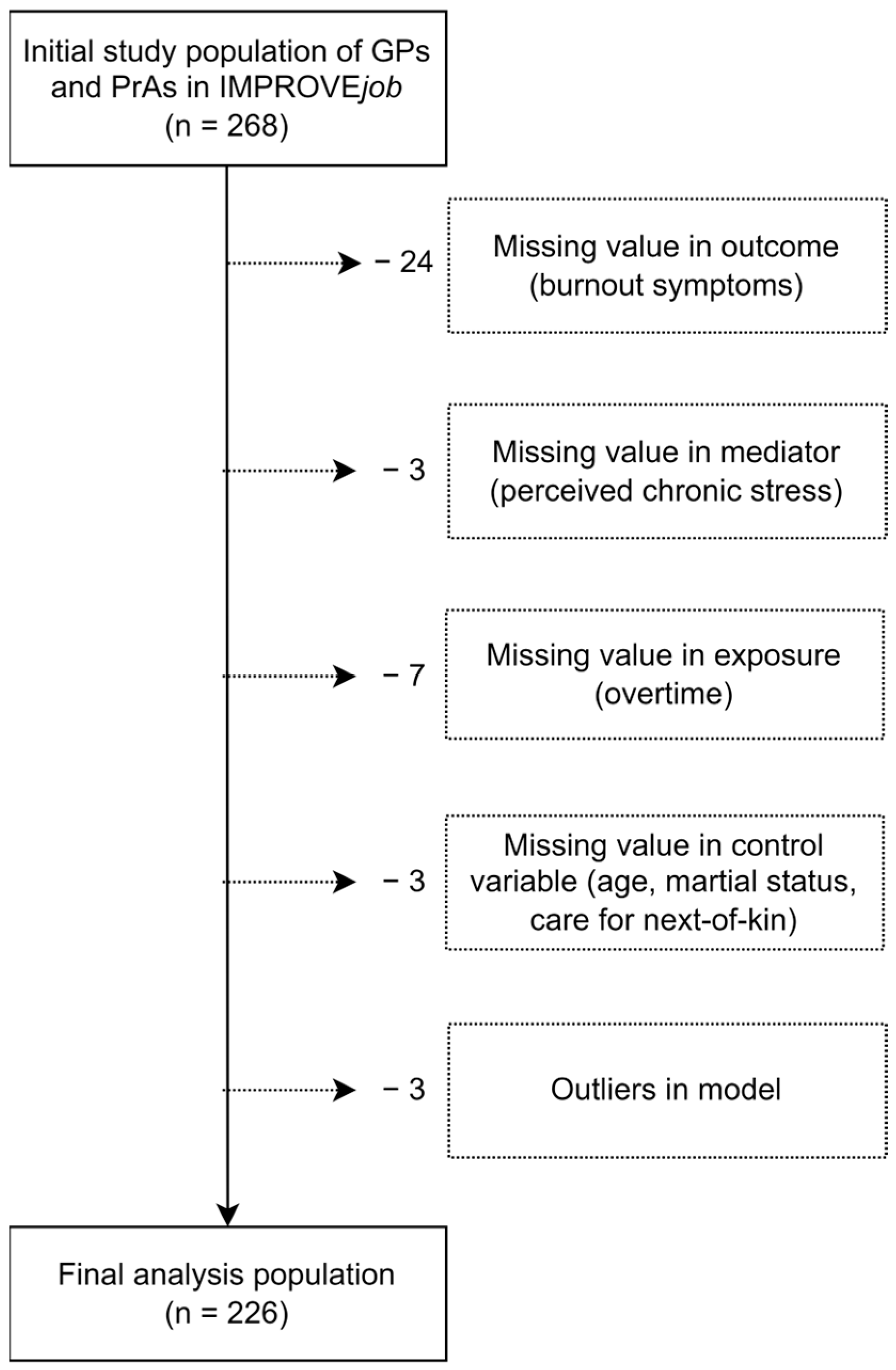
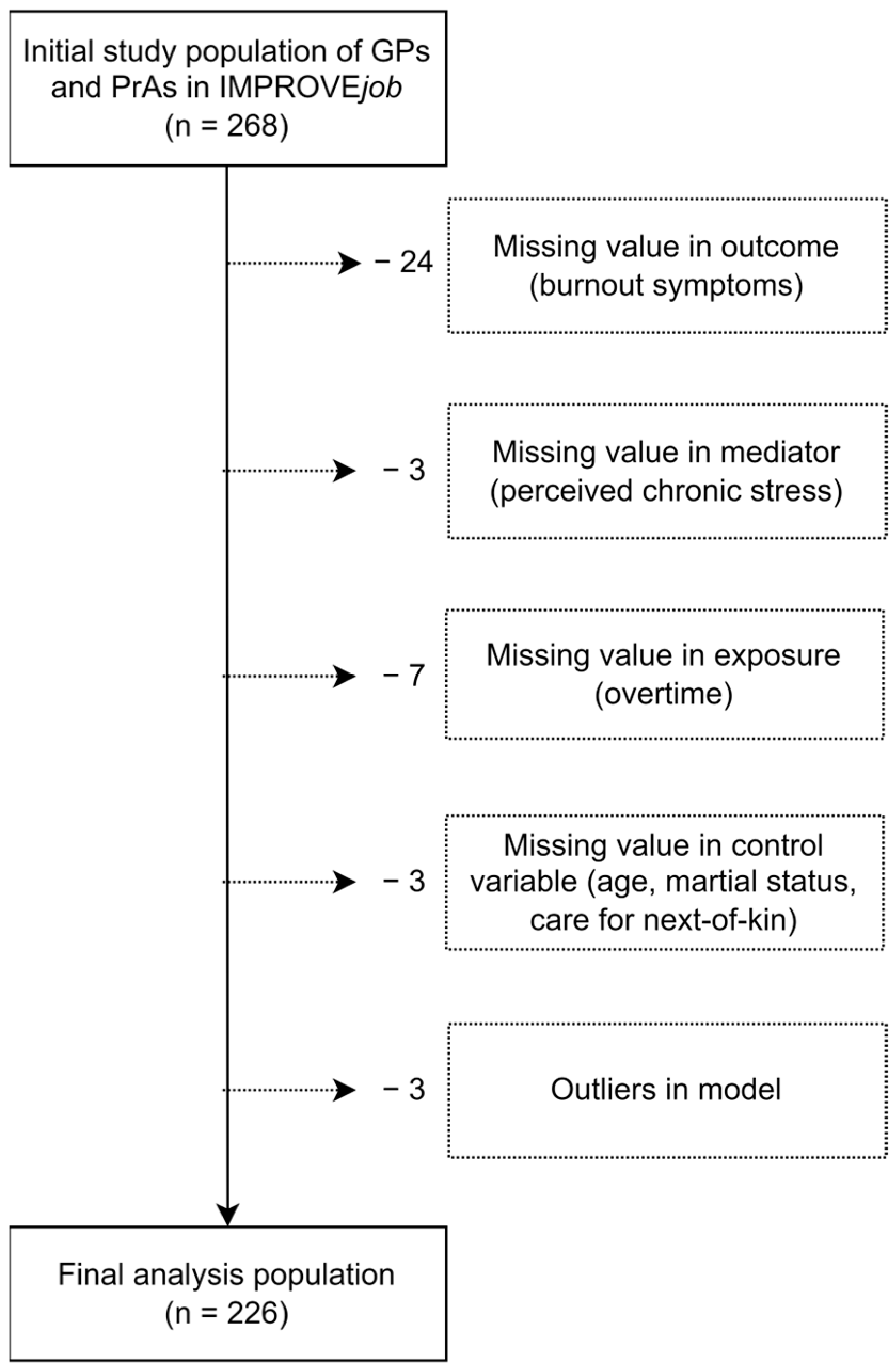
2.2. Recruitment and Analysis Population
2.3. Outcome Variable: Pandemic-Related Changes in Burnout Symptoms
2.4. Independent Variable: Pandemic-Related Changes in Overtime
2.5. Mediator Variable: Pandemic-Related Changes in Perceived Chronic Stress
2.6. Control Variables

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total Sample (n = 226) | ||
|---|---|---|
| Variable | Mean (SD) | t-Test (p-Value) |
| Overtime (BL) | 1.34 (2.16) | |
| Overtime (FU) | 1.42 (2.16) | |
| Overtime (Δ) | 0.08 (2.26) | 0.5 (0.62) |
| TICS-SSCS (BL) | 19.11 (8) | |
| TICS-SSCS (FU) | 18 (8.42) | |
| TICS-SSCS (Δ) | −1.11 (7.04) | −2.36 (0.02) |
| MBI (BL) | 5.56 (1.99) | |
| MBI (FU) | 5.92 (2.02) | |
| MBI (Δ) | 0.36 (1.79) | 3.04 (0.003) |
2.7. Statistical Analysis
3. Results
3.1. Descriptive Results
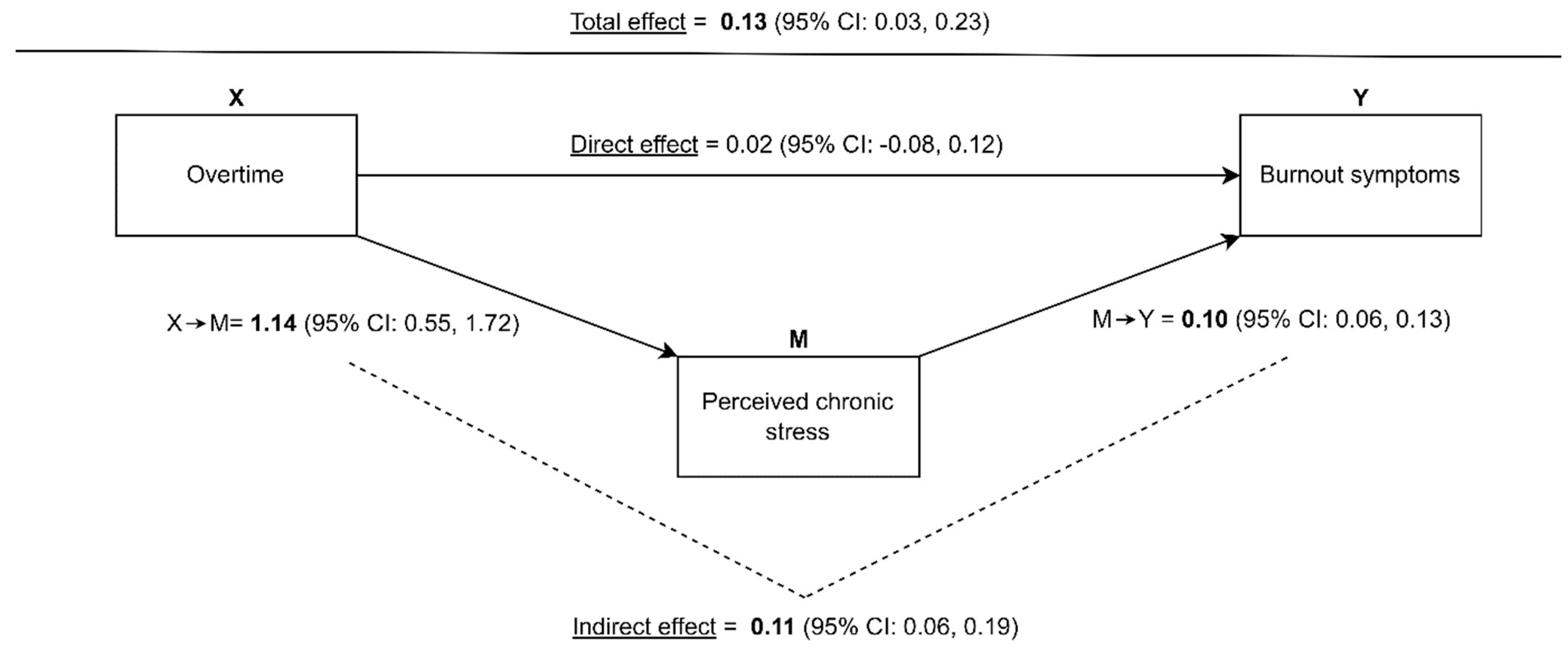
3.2. Mediation Analysis of Pandemic-Related Changes in Overtime, Perceived Chronic Stress and Burnout Symptoms
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vancampfort, D.; Koyanagi, A.; Ward, P.B.; Veronese, N.; Carvalho, A.F.; Solmi, M.; Mugisha, J.; Rosenbaum, S.; De Hert, M.; Stubbs, B. Perceived Stress and Its Relationship With Chronic Medical Conditions and Multimorbidity Among 229,293 Community-Dwelling Adults in 44 Low- and Middle-Income Countries. Am. J. Epidemiology 2017, 186, 979–989. [Google Scholar] [CrossRef]
- Hapke, U.; Maske, U.; Scheidt-Nave, C.; Bode, L.; Schlack, R.; Busch, M. Chronischer Stress bei Erwachsenen in Deutschland. Bundesgesundheitsblatt—Gesundheitsforschung—Gesundheitsschutz 2013, 56, 749–754. [Google Scholar] [CrossRef] [PubMed]
- Hussenoeder, F.S.; Conrad, I.; Pabst, A.; Luppa, M.; Stein, J.; Engel, C.; Zachariae, S.; Zeynalova, S.; Yahiaoui-Doktor, M.; Glaesmer, H.; et al. Different Areas of Chronic Stress and Their Associations with Depression. Int. J. Environ. Res. Public Health 2022, 19, 8773. [Google Scholar] [CrossRef]
- Fishta, A.; Backé, E.-M. Psychosocial stress at work and cardiovascular diseases: An overview of systematic reviews. Int. Arch. Occup. Environ. Health 2015, 88, 997–1014. [Google Scholar] [CrossRef] [PubMed]
- Lukan, J.; Bolliger, L.; Pauwels, N.S.; Luštrek, M.; De Bacquer, D.; Clays, E. Work environment risk factors causing day-to-day stress in occupational settings: A systematic review. BMC Public Health 2022, 22, 240. [Google Scholar] [CrossRef] [PubMed]
- Viehmann, A.; Kersting, C.; Thielmann, A.; Weltermann, B. Prevalence of chronic stress in general practitioners and practice assistants: Personal, practice and regional characteristics. PLoS ONE 2017, 12, e0176658. [Google Scholar] [CrossRef]
- Beech, J.; Fraser, C.; Gardner, T.; Buzelli, L.; Williamson, S.; Alderwick, H. Stressed and overworked: What the Commonwealth Fund’s 2022 International Health Policy Survey of Primary Care Physicians in 10 Countries means for the UK; The Health Foundation: London, UK, 2023. [Google Scholar]
- Starfield, B.; Shi, L.; Macinko, J. Contribution of Primary Care to Health Systems and Health. Milbank Q. 2005, 83, 457–502. [Google Scholar] [CrossRef]
- Rosta, J.; Bååthe, F.; Aasland, O.G.; Rø, K.I. Changes in work stress among doctors in Norway from 2010 to 2019: A study based on repeated surveys. BMJ Open 2020, 10, e037474. [Google Scholar] [CrossRef]
- Riley, R.; Spiers, J.; Buszewicz, M.; Taylor, A.K.; Thornton, G.; Chew-Graham, C.A. What are the sources of stress and distress for general practitioners working in England? A qualitative study. BMJ Open 2017, 8, e017361. [Google Scholar] [CrossRef]
- Lee, F.J.; Brown, J.B.; Stewart, M. Exploring family physician stress: Helpful strategies. Can. Fam. Physician 2009, 55, 288–289.e6. [Google Scholar]
- McManus, I.; Winder, B.; Gordon, D. The causal links between stress and burnout in a longitudinal study of UK doctors. Lancet 2002, 359, 2089–2090. [Google Scholar] [CrossRef]
- WHO News. Burn-Out An “Occupational Phenomenon”: International Classification of Diseases. 2019. Available online: https://www.who.int/news/item/28-05-2019-burn-out-an-occupational-phenomenon-international-classification-of-diseases (accessed on 5 September 2021).
- Rotenstein, L.S.; Torre, M.; Ramos, M.A.; Rosales, R.C.; Guille, C.; Sen, S.; Mata, D.A. Prevalence of Burnout Among Physicians: A Systematic Review. JAMA 2018, 320, 1131–1150. [Google Scholar] [CrossRef]
- Karuna, C.; Palmer, V.J.; Scott, A.; Gunn, J. Prevalence of burnout among GPs: A systematic review and meta-analysis. Br. J. Gen. Pract. 2022, 72, e316–e324. [Google Scholar] [CrossRef]
- Soler, J.K.; Yaman, H.; Esteva, M.; Dobbs, F.; Asenova, R.S.; Katić, M.; OžVačIć, Z.; Desgranges, J.P.; Moreau, A.; Lionis, C.; et al. Burnout in European family doctors: The EGPRN study. Fam. Pract. 2008, 25, 245–265. [Google Scholar] [CrossRef]
- Degen, L.; Linden, K.; Seifried-Dübon, T.; Werners, B.; Grot, M.; Rind, E.; Pieper, C.; Eilerts, A.-L.; Schroeder, V.; Kasten, S.; et al. Job Satisfaction and Chronic Stress of General Practitioners and Their Teams: Baseline Data of a Cluster-Randomised Trial (IMPROVEjob). Int. J. Environ. Res. Public Health 2021, 18, 9458. [Google Scholar] [CrossRef]
- Monsalve-Reyes, C.S.; Luis-Costas, C.S.; Gómez-Urquiza, J.L.; Albendín-García, L.; Aguayo, R.; la Fuente, G.A.C.-D. Burnout syndrome and its prevalence in primary care nursing: A systematic review and meta-analysis. BMC Fam. Pract. 2018, 19, 59. [Google Scholar] [CrossRef]
- Bozorgmehr, A.; Thielmann, A.; Weltermann, B. Chronic stress in practice assistants: An analytic approach comparing four machine learning classifiers with a standard logistic regression model. PLoS ONE 2021, 16, e0250842. [Google Scholar] [CrossRef]
- Demerouti, E.; Bakker, A.B.; Nachreiner, F.; Schaufeli, W.B. The job demands-resources model of burnout. Journal of applied psychology 2001, 86, 499. [Google Scholar] [CrossRef]
- Siegrist, J. Adverse health effects of high-effort/low-reward conditions. J. Occup. Health Psychol. 1996, 1, 27–41. [Google Scholar] [CrossRef]
- Goetz, K.; Campbell, S.M.; Steinhaeuser, J.; Broge, B.; Willms, S.; Szecsenyi, J. Evaluation of job satisfaction of practice staff and general practitioners: An exploratory study. BMC Fam. Pract. 2011, 12, 137. [Google Scholar] [CrossRef] [PubMed]
- Tuxford, L.M.; Bradley, G.L. Emotional job demands and emotional exhaustion in teachers. Educ. Psychol. 2013, 35, 1006–1024. [Google Scholar] [CrossRef]
- Burr, H.; Berthelsen, H.; Moncada, S.; Nübling, M.; Dupret, E.; Demiral, Y.; Oudyk, J.; Kristensen, T.S.; Llorens, C.; Navarro, A.; et al. The Third Version of the Copenhagen Psychosocial Questionnaire. Saf. Health Work. 2019, 10, 482–503. [Google Scholar] [CrossRef]
- Le Huu, P.; Bellagamba, G.; Bouhadfane, M.; Villa, A.; Lehucher, M.-P. Meta-analysis of effort–reward imbalance prevalence among physicians. Int. Arch. Occup. Environ. Health 2022, 95, 559–571. [Google Scholar] [CrossRef]
- Kersting, C.; Zimmer, L.; Thielmann, A.; Weltermann, B. Chronic stress, work-related daily challenges and medicolegal investigations: A cross-sectional study among German general practitioners. BMC Fam. Pract. 2019, 20, 143. [Google Scholar] [CrossRef]
- Gardner, R.L.; Cooper, E.; Haskell, J.; A Harris, D.; Poplau, S.; Kroth, P.J.; Linzer, M. Physician stress and burnout: The impact of health information technology. J. Am. Med. Inform. Assoc. 2018, 26, 106–114. [Google Scholar] [CrossRef]
- Shanafelt, T.D.; Boone, S.; Tan, L.; Dyrbye, L.N.; Sotile, W.; Satele, D.; West, C.P.; Sloan, J.; Oreskovich, M.R. Burnout and Satisfaction With Work-Life Balance Among US Physicians Relative to the General US Population. Arch. Intern. Med. 2012, 172, 1377–1385. [Google Scholar] [CrossRef]
- Jefferson, L.; Golder, S.; Heathcote, C.; Avila, A.C.; Dale, V.; Essex, H.; Cornelis, C.v.d.F.; McHugh, E.; Moe-Byrne, T.; Bloor, K. GP wellbeing during the COVID-19 pandemic: A systematic review. Br. J. Gen. Pract. 2022, 72, e325–e333. [Google Scholar] [CrossRef]
- Chutiyami, M.; Cheong, A.M.Y.; Salihu, D.; Bello, U.M.; Ndwiga, D.; Maharaj, R.; Naidoo, K.; Kolo, M.A.; Jacob, P.; Chhina, N.; et al. COVID-19 Pandemic and Overall Mental Health of Healthcare Professionals Globally: A Meta-Review of Systematic Reviews. Front. Psychiatry 2022, 12, 804525. [Google Scholar] [CrossRef] [PubMed]
- Phiri, P.; Ramakrishnan, R.; Rathod, S.; Elliot, K.; Thayanandan, T.; Sandle, N.; Haque, N.; Chau, S.W.; Wong, O.W.; Chan, S.S.; et al. An evaluation of the mental health impact of SARS-CoV-2 on patients, general public and healthcare professionals: A systematic review and meta-analysis. EClinicalMedicine 2021, 34, 100806. [Google Scholar] [CrossRef] [PubMed]
- Moro, M.F.; Calamandrei, G.; Poli, R.; Di Mattei, V.; Perra, A.; Kurotschka, P.K.; Restrepo, A.; Romano, F.; La Torre, G.; Preti, E.; et al. The Impact of the COVID-19 Pandemic on the Mental Health of Healthcare Workers in Italy: Analyzing the Role of Individual and Workplace-Level Factors in the Reopening Phase After Lockdown. Front. Psychiatry 2022, 13, 867080. [Google Scholar] [CrossRef] [PubMed]
- KBV Kassenärztliche Bundesvereinigung. CORONA-REPORT/25.11.2020 2020. Available online: https://www.kbv.de/html/corona-report.php (accessed on 9 September 2023).
- Doleman, G.; De Leo, A.; Bloxsome, D. The impact of pandemics on healthcare providers’ workloads: A scoping review. J. Adv. Nurs. 2023, 79, 4434–4454. [Google Scholar] [CrossRef]
- Mause, L.; Hoffmann, J.; Ohnhäuser, T.; Gunkel, S.; Stöcker, A.; Scholten, N. Work climate in pandemic times: Which burdens do German physicians in primary care report? Fam. Pract. 2021, 39, 46–51. [Google Scholar] [CrossRef]
- Werdecker, L.; Esch, T. Burnout, satisfaction and happiness among German general practitioners (GPs): A cross-sectional survey on health resources and stressors. PLoS ONE 2021, 16, e0253447. [Google Scholar] [CrossRef]
- West, C.P.; Dyrbye, L.N.; Erwin, P.J.; Shanafelt, T.D. Interventions to prevent and reduce physician burnout: A systematic review and meta-analysis. Lancet 2016, 388, 2272–2281. [Google Scholar] [CrossRef]
- Asuero, A.M.; Queraltó, J.M.; Pujol-Ribera, E.; Berenguera, A.; Rodriguez-Blanco, T.; Epstein, R.M. Effectiveness of a Mindfulness Education Program in Primary Health Care Professionals: A Pragmatic Controlled Trial. J. Contin. Educ. Health Prof. 2014, 34, 4–12. [Google Scholar] [CrossRef]
- Council of European Union. Council Directive 89/391/EEC of 12 June 1989 on the introduction of measures to encourage improvements in the safety and health of workers at work, 1989; Council of European Union: Brussel, Belgium, 1989. [Google Scholar]
- Montano, D.; Hoven, H.; Siegrist, J. Effects of organisational-level interventions at work on employees’ health: A systematic review. BMC Public Health. 2014, 14, 135. [Google Scholar] [CrossRef] [PubMed]
- Shiri, R.; Nikunlaakso, R.; Laitinen, J. Effectiveness of Workplace Interventions to Improve Health and Well-Being of Health and Social Service Workers: A Narrative Review of Randomised Controlled Trials. Healthcare 2023, 11, 1792. [Google Scholar] [CrossRef]
- Weltermann, B.M.; Kersting, C.; Pieper, C.; Seifried-Dübon, T.; Dreher, A.; Linden, K.; Rind, E.; Ose, C.; Jöckel, K.-H.; Junne, F.; et al. IMPROVEjob—Participatory intervention to improve job satisfaction of general practice teams: A model for structural and behavioural prevention in small and medium-sized enterprises—A study protocol of a cluster-randomised controlled trial. Trials 2020, 21, 532. [Google Scholar] [CrossRef] [PubMed]
- Degen, L.; Göbel, J.; Minder, K.; Seifried-Dübon, T.; Werners, B.; Grot, M.; Rind, E.; Pieper, C.; Eilerts, A.-L.; Schröder, V.; et al. Leadership program with skills training for general practitioners was highly accepted without improving job satisfaction: The cluster randomized IMPROVEjob study. Sci. Rep. 2022, 12, 17869. [Google Scholar] [CrossRef] [PubMed]
- Robert Koch-Institut. 7-Tage-Inzidenz der COVID-19-Fälle in Deutschland: Zenodo 2023; Robert Koch-Institut: Berlin, Germany, 2023. [Google Scholar]
- Maslach, C.; Jackson, S.E.; Leiter, M.P. Maslach Burnout Inventory. In Evaluating Stress: A Book of Resources; Zalaquett, C.P., Wood, R.J., Eds.; Scarecrow Education: Lanham, MI, USA, 1997. [Google Scholar]
- Kotsopoulos, D.; Bardaki, C.; Papaioannou, T.G. Determinants of Employees’ Personal and Collective Energy Consumption and Conservation at Work. Sustainability 2023, 15, 4913. [Google Scholar] [CrossRef]
- West, C.P.; Dyrbye, L.N.; Sloan, J.A.; Shanafelt, T.D. Single Item Measures of Emotional Exhaustion and Depersonalization Are Useful for Assessing Burnout in Medical Professionals. J. Gen. Intern. Med. 2009, 24, 1318–1321. [Google Scholar] [CrossRef] [PubMed]
- West, C.P.; Dyrbye, L.N.; Satele, D.V.; Sloan, J.A.; Shanafelt, T.D. Concurrent Validity of Single-Item Measures of Emotional Exhaustion and Depersonalization in Burnout Assessment. J. Gen. Intern. Med. 2012, 27, 1445–1452. [Google Scholar] [CrossRef] [PubMed]
- Schulz, P.; Schlotz, W. Trierer Inventar zur Erfassung von chronischem Streß (TICS): Skalenkonstruktion, teststatistische Überprüfung und Validierung der Skala Arbeitsüberlastung. Diagnostica 1999, 45, 8–19. [Google Scholar] [CrossRef]
- Schulz, P.; Schlotz, W.; Becker, P. Trierer Inventar zum Chronischen Stress (TICS) [Trier Inventory for Chronic Stress (TICS)]; Hogrefe: Göttingen, Germany, 2004. [Google Scholar]
- Göbel, J.; Schmidt, M.; Seifried-Dübon, T.; Linden, K.; Degen, L.; Rind, E.; Eilerts, A.-L.; Pieper, C.; Grot, M.; Werners, B.; et al. Higher Work-Privacy Conflict and Lower Job Satisfaction in GP Leaders and Practice Assistants Working Full-Time Compared to Part-Time: Results of the IMPROVEjob Study. Int. J. Environ. Res. Public Health 2022, 19, 2618. [Google Scholar] [CrossRef] [PubMed]
- Horwitz, A.V.; White, H.R.; Howell-White, S. Becoming Married and Mental Health: A Longitudinal Study of a Cohort of Young Adults. J. Marriage Fam. 1996, 58, 895. [Google Scholar] [CrossRef]
- Alves, L.C.d.S.; Monteiro, D.Q.; Bento, S.R.; Hayashi, V.D.; Pelegrini, L.N.d.C.; Vale, F.A.C. Burnout syndrome in informal caregivers of older adults with dementia: A systematic review. Dement. Neuropsychol. 2019, 13, 415–421. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guilford Press: New York, NY, USA, 2013; ISBN 1609182308. [Google Scholar]
- Davidson, R.; MacKinnon, J.G. Estimation and Inference in Econometrics; Oxford University Press: New York, NY, Oxford, 1993; ISBN 9780195060119. [Google Scholar]
- Baron, R.M.; Kenny, D.A. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Pers. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef]
- Feng, J.; Jiang, H.; Shen, X.; Lei, Z.; Li, L.; Zhu, Y.; Zhang, M.; Yang, T.; Meng, X.; Di, H.; et al. Occupational stress and associated factors among general practitioners in China: A national cross-sectional study. BMC Public Health 2022, 22, 1061. [Google Scholar] [CrossRef]
- Núñez-Elvira, A. Trends and determinants of GPs’ work hours in the UK: A quantitative study. BJGP Open 2023, 7. [Google Scholar] [CrossRef]
- Leutgeb, R.; Frankenhauser-Mannuß, J.; Scheuer, M.; Szecsenyi, J.; Goetz, K. Job satisfaction and stressors for working in out-of-hours care—A pilot study with general practitioners in a rural area of Germany. BMC Fam. Pract. 2018, 19, 95. [Google Scholar] [CrossRef]
- Koch, K.; Miksch, A.; Schürmann, C.; Joos, S.; Sawicki, P.T. The German Health Care System in International Comparison. Dtsch. Aerzteblatt Online 2011, 108, 255–261. [Google Scholar] [CrossRef]
- Kramer, V.; Papazova, I.; Thoma, A.; Kunz, M.; Falkai, P.; Schneider-Axmann, T.; Hierundar, A.; Wagner, E.; Hasan, A. Subjective burden and perspectives of German healthcare workers during the COVID-19 pandemic. Eur. Arch. Psychiatry Clin. Neurosci. 2020, 271, 271–281. [Google Scholar] [CrossRef]
- Linzer, M.; Poplau, S.; Babbott, S.; Collins, T.; Guzman-Corrales, L.; Menk, J.; Murphy, M.L.; Ovington, K. Worklife and Wellness in Academic General Internal Medicine: Results from a National Survey. J. Gen. Intern. Med. 2016, 31, 1004–1010. [Google Scholar] [CrossRef]
- Shanafelt, T.D.; West, C.P.; Dyrbye, L.N.; Trockel, M.; Tutty, M.; Wang, H.; Carlasare, L.E.; Sinsky, C. Changes in Burnout and Satisfaction With Work-Life Integration in Physicians During the First 2 Years of the COVID-19 Pandemic. Mayo Clin. Proc. 2022, 97, 2248–2258. [Google Scholar] [CrossRef] [PubMed]
- Sinsky, C.A.; Shanafelt, T.D.; Dyrbye, L.N.; Sabety, A.H.; Carlasare, L.E.; West, C.P. Health Care Expenditures Attributable to Primary Care Physician Overall and Burnout-Related Turnover: A Cross-sectional Analysis. Mayo Clin. Proc. 2022, 97, 693–702. [Google Scholar] [CrossRef] [PubMed]
- Shen, X.; Jiang, H.; Xu, H.; Ye, J.; Lv, C.; Lu, Z.; Gan, Y. The global prevalence of turnover intention among general practitioners: A systematic review and meta-analysis. BMC Fam. Pract. 2020, 21, 246. [Google Scholar] [CrossRef] [PubMed]
- Amanullah, S.; Shankar, R.R. The Impact of COVID-19 on Physician Burnout Globally: A Review. Healthcare 2020, 8, 421. [Google Scholar] [CrossRef] [PubMed]
- Macaron, M.M.; Segun-Omosehin, O.A.; Matar, R.H.; Beran, A.; Nakanishi, H.; Than, C.A.; Abulseoud, O.A. A systematic review and meta analysis on burnout in physicians during the COVID-19 pandemic: A hidden healthcare crisis. Front. Psychiatry 2023, 13, 1071397. [Google Scholar] [CrossRef] [PubMed]
- Alarcon, G.; Eschleman, K.J.; Bowling, N.A. Relationships between personality variables and burnout: A meta-analysis. Work. Stress 2009, 23, 244–263. [Google Scholar] [CrossRef]
- Jiménez-Fernández, R.; Corral-Liria, I.; Trevissón-Redondo, B.; Lopez-Lopez, D.; Losa-Iglesias, M.; Becerro-De-Bengoa-Vallejo, R. Burnout, resilience and psychological flexibility in frontline nurses during the acute phase of the COVID-19 pandemic (2020) in Madrid, Spain. J. Nurs. Manag. 2022, 30, 2549–2556. [Google Scholar] [CrossRef]
- M. Blanch, J.; Ochoa, P.; Fernanda Caballero, M. Over Engagement, Protective or Risk Factor of Burnout? In Sustainable Management Practices; Sarfraz, M., Ibrahim Adbullah, M., Rauf, A., Ghulam Meran Shah, S., Eds.; IntechOpen: London, UK, 2019; ISBN 978-1-78985-153-3. [Google Scholar]
- Mangory, K.Y.; Ali, L.Y.; Rø, K.I.; Tyssen, R. Effect of burnout among physicians on observed adverse patient outcomes: A literature review. BMC Health Serv. Res. 2021, 21, 369. [Google Scholar] [CrossRef]
- Han, S.; Shanafelt, T.D.; Sinsky, C.A.; Awad, K.M.; Dyrbye, L.N.; Fiscus, L.C.; Trockel, M.; Goh, J. Estimating the Attributable Cost of Physician Burnout in the United States. Ann. Intern. Med. 2019, 170, 784–790. [Google Scholar] [CrossRef]
- Shanafelt, T.D.; Noseworthy, J.H. Executive Leadership and Physician Well-being. Mayo Clin. Proc. 2016, 92, 129–146. [Google Scholar] [CrossRef]
- Papp, M.; Kőrösi, L.; Sándor, J.; Nagy, C.; Juhász, A.; Ádány, R. Workforce crisis in primary healthcare worldwide: Hungarian example in a longitudinal follow-up study. BMJ Open 2019, 9, e024957. [Google Scholar] [CrossRef]
- Bussche, H.v.D. The future problems of general practice in Germany: Current trends and necessary measures. Bundesgesundheitsblatt—Gesundheitsforschung—Gesundheitsschutz 2019, 62, 1129–1137. [Google Scholar] [CrossRef]
- Wangler, J.; Jansky, M. How can primary care be secured in the long term?—A qualitative study from the perspective of general practitioners in Germany. Eur. J. Gen. Pract. 2023, 29, 2223928. [Google Scholar] [CrossRef]
- Stierli, R.; Rozsnyai, Z.; Felber, R.; Jörg, R.; Kraft, E.; Exadaktylos, A.K.; Streit, S. Primary Care Physician Workforce 2020 to 2025—A cross-sectional study for the Canton of Bern. Swiss Med. Wkly. 2021, 151, w30024. [Google Scholar] [CrossRef] [PubMed]
- Le Floch, B.; Bastiaens, H.; Le Reste, J.Y.; Lingner, H.; Hoffman, R.; Czachowski, S.; Assenova, R.; Koskela, T.H.; Klemenc-Ketis, Z.; Nabbe, P.; et al. Which positive factors give general practitioners job satisfaction and make general practice a rewarding career? A European multicentric qualitative research by the European general practice research network. BMC Fam. Pract. 2019, 20, 96. [Google Scholar] [CrossRef] [PubMed]
- Van Ham, I.; Verhoeven, A.A.H.; Groenier, K.H.; Groothoff, J.W.; De Haan, J. Job satisfaction among general practitioners: A systematic literature review. Eur. J. Gen. Pract. 2006, 12, 174–180. [Google Scholar] [CrossRef] [PubMed]


| Total Sample (n = 226) | |
|---|---|
| Variable | |
| Female, n (%) | 196 (86.7) |
| Age in years, mean (SD) | 45 (12) |
| General practice assistants, n (%) | 158 (69.9) |
| Working full-time, n (%) | 123 (54.4) |
| Living in a relationship/married, n (%) | 183 (81.0) |
| Care for next-of-kin, n (%) | 48 (21.2) |
| Control group, n (%) | 119 (52.7) |
| Total Sample (n = 226) | GPs (n = 68) | PrAs (n = 158) | ||||
|---|---|---|---|---|---|---|
| Coefficient | 95% CI | Coefficient | 95% CI | Coefficient | 95% CI | |
| Total Effect | 0.13 | 0.03, 0.23 | 0.05 | −0.16, 0.26 | 0.34 | 0.12, 0.57 |
| Direct Effect | 0.02 | −0.08, 0.12 | −0.03 | −0.29, 0.23 | 0.17 | −0.05, 0.38 |
| Indirect Effect | 0.11 | 0.06, 0.19 | 0.08 | 0.01, 0.17 | 0.17 | 0.08, 0.29 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Küppers, L.; Göbel, J.; Aretz, B.; Rieger, M.A.; Weltermann, B. Associations between COVID-19 Pandemic-Related Overtime, Perceived Chronic Stress and Burnout Symptoms in German General Practitioners and Practice Personnel—A Prospective Study. Healthcare 2024, 12, 479. https://doi.org/10.3390/healthcare12040479
Küppers L, Göbel J, Aretz B, Rieger MA, Weltermann B. Associations between COVID-19 Pandemic-Related Overtime, Perceived Chronic Stress and Burnout Symptoms in German General Practitioners and Practice Personnel—A Prospective Study. Healthcare. 2024; 12(4):479. https://doi.org/10.3390/healthcare12040479
Chicago/Turabian StyleKüppers, Lucas, Julian Göbel, Benjamin Aretz, Monika A. Rieger, and Birgitta Weltermann. 2024. "Associations between COVID-19 Pandemic-Related Overtime, Perceived Chronic Stress and Burnout Symptoms in German General Practitioners and Practice Personnel—A Prospective Study" Healthcare 12, no. 4: 479. https://doi.org/10.3390/healthcare12040479
APA StyleKüppers, L., Göbel, J., Aretz, B., Rieger, M. A., & Weltermann, B. (2024). Associations between COVID-19 Pandemic-Related Overtime, Perceived Chronic Stress and Burnout Symptoms in German General Practitioners and Practice Personnel—A Prospective Study. Healthcare, 12(4), 479. https://doi.org/10.3390/healthcare12040479