_MD__MPH_PhD.png)
Risks Associated with Quality Care among Hispanic and White Populations—A Cross-Sectional Comparison Study

 ,
,
Abstract
1. Introduction
2. Methods
2.1. Study Design and Setting
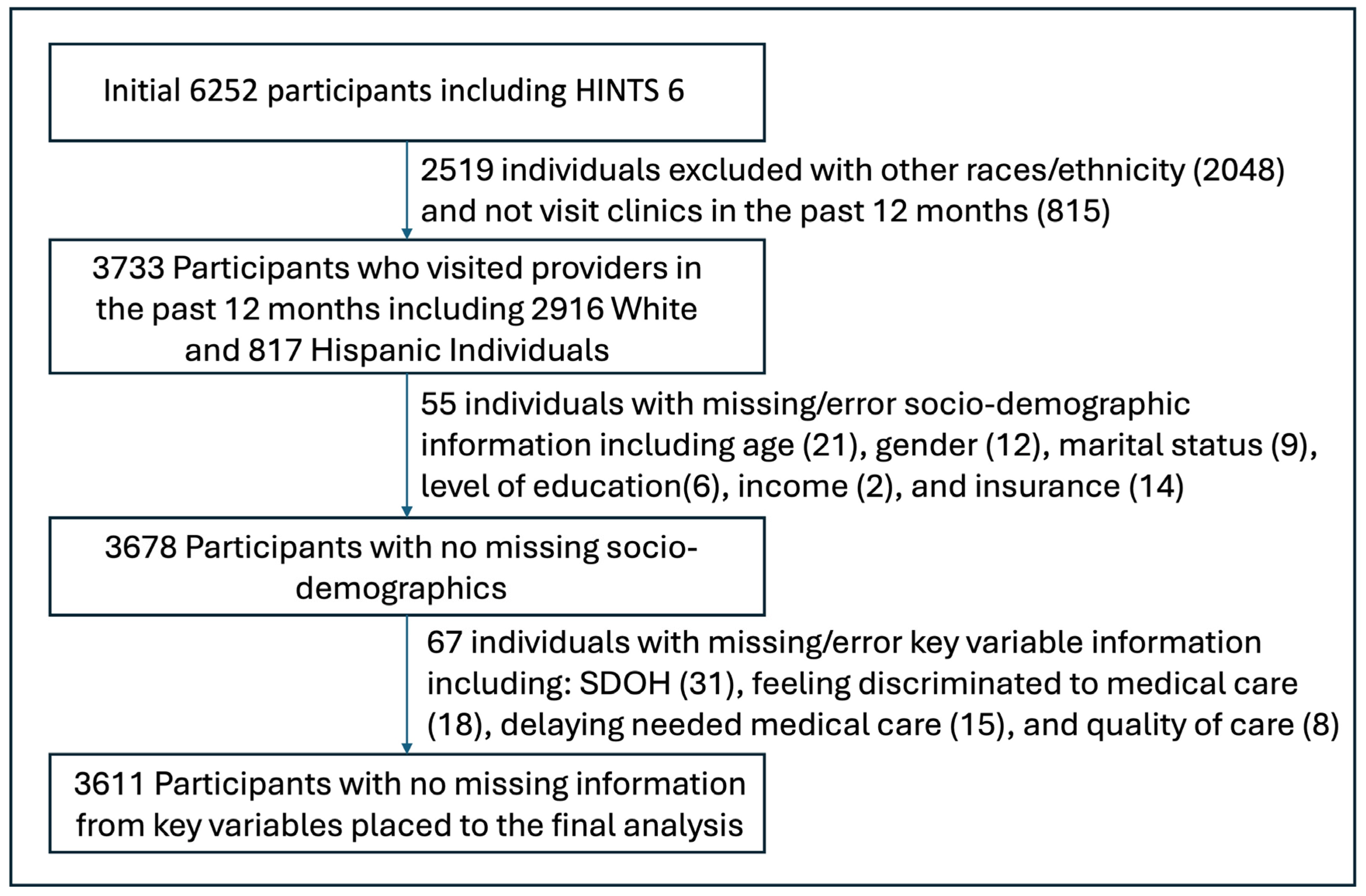
2.2. Inclusion and Exclusion Criteria
2.3. Outcome Measures
2.4. Key Variables
2.5. Other Variables
2.6. Data Analysis
2.7. Reporting Guideline
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
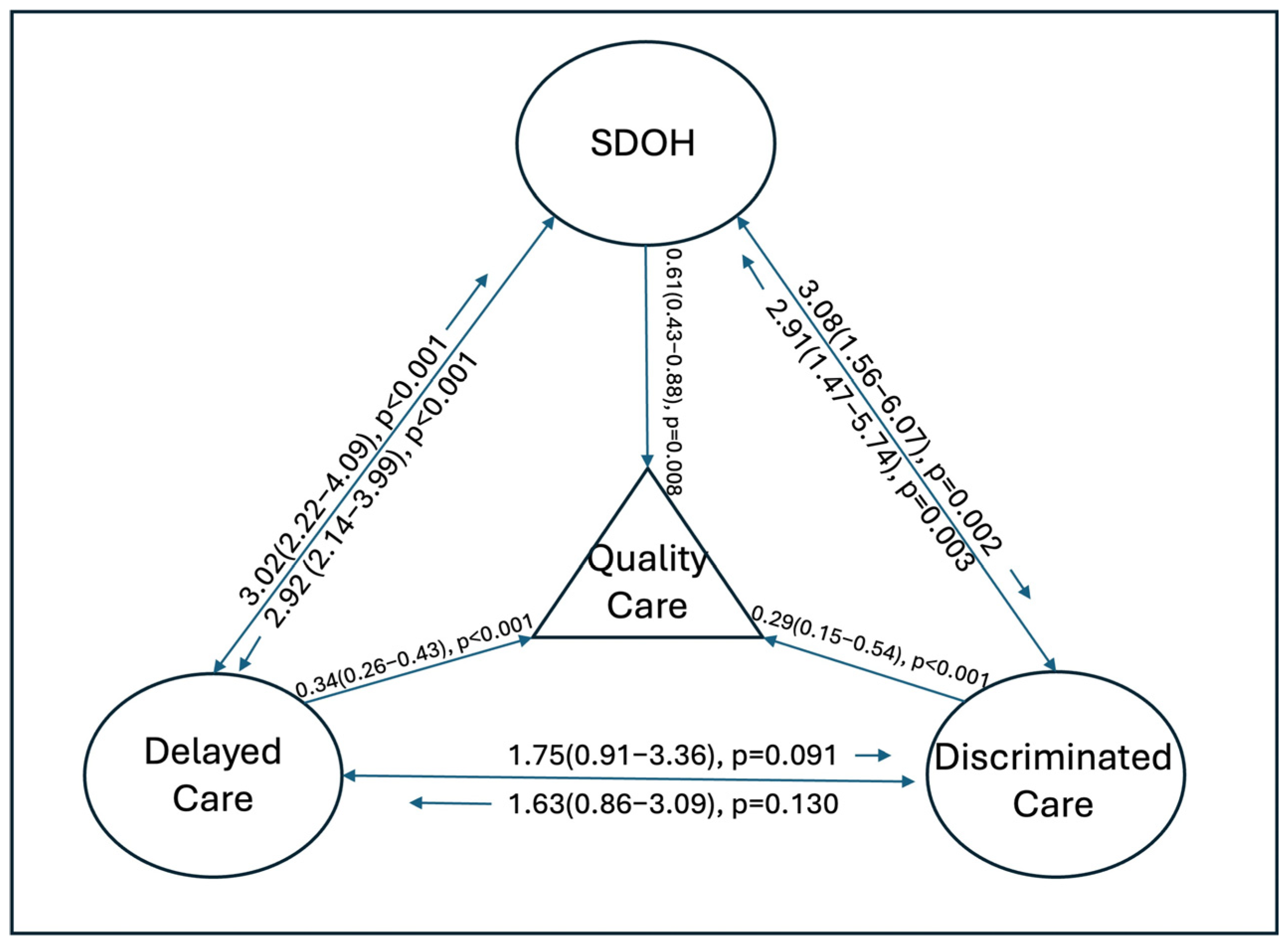
| Quality Care | SDOH | Delayed Care | Discriminated Care | |
|---|---|---|---|---|
| AOR (95% CI), p | AOR (95% CI), p | AOR (95% CI), p | AOR (95% CI), p | |
| Quality care | ||||
| Less optimal (ref) | ||||
| Optimal | 0.61 (0.42–0.88), 0.008 | 0.34 (0.26–0.43), <0.001 | 0.29 (0.16–0.53), <0.001 | |
| SDOH | ||||
| Positive (ref) | ||||
| Negative | 0.61 (0.43–0.88), 0.008 | 2.92 (2.14–3.99), <0.001 | 3.08 (1.56–6.07), 0.002 | |
| Delayed medical care | ||||
| No (ref) | ||||
| Yes | 0.34 (0.26–0.43), <0.001 | 3.02 (2.23–4.09), <0.001 | 1.75 (0.91–3.36), 0.091 | |
| Discriminated care | ||||
| No (ref) | ||||
| Yes | 0.29 (0.15–0.54), <0.001 | 2.91 (1.47–5.74), 0.003 | 1.63 (0.86–3.09), 0.130 | |
| Race/ethnicity | ||||
| White (ref) | ||||
| Hispanic | 0.88 (0.75–1.03), 0.120 | 1.18 (0.96–1.43), 0.107 | 0.89 (0.76–1.04), 0.133 | 2.13 (1.65–2.74), <0.001 |
| Insurance coverage | ||||
| No (ref) | ||||
| Yes | 2.03 (1.22–3.37), 0.007 | 0.60 (0.30–1.17), 0.132 | 1.40 (0.75–2.63), 0.288 | 1.55 (0.58–4.16), 0.376 |
| Age | ||||
| 18–34 (ref) | ||||
| 35–49 | 1.39 (0.87–2.20), 0.164 | 0.85 (0.49–1.46), 0.548 | 0.78 (0.53–1.14), 0.190 | 1.13 (0.52–2.48), 0.750 |
| 50–64 | 1.69 (1.04–2.75), 0.034 | 0.64 (0.38–1.08), 0.093 | 0.87 (0.64–1.18), 0.363 | 1.17 (0.49–2.81), 0.715 |
| 65–74 | 1.91 (1.17–3.10), 0.011 | 0.30 (0.16–0.54), <0.001 | 0.59 (0.41–0.84), 0.004 | 1.06 (0.41–2.76), 0.903 |
| 75+ | 1.36 (0.80–2.32), 0.245 | 0.26 (0.12–0.59), 0.002 | 0.45 (0.28–0.72), 0.001 | 0.23 (0.06–0.96), 0.044 |
| Gender | ||||
| Male (ref) | ||||
| Female | 1.03 (0.76–1.40), 0.851 | 1.19 (0.85–1.67), 0.299 | 1.09 (0.88–1.36), 0.427 | 0.77 (0.43–1.39), 0.382 |
| Marital status | ||||
| Single (ref) | ||||
| Married | 1.04 (0.70–1.54), 0.832 | 0.66 (0.46–0.94), 0.024 | 1.09 (0.76–1.54), 0.638 | 1.03 (0.46–2.32), 0.935 |
| Others | 0.85 (0.52–1.41), 0.526 | 1.08 (0.67–1.76), 0.745 | 0.97 (0.64–1.47), 0.896 | 1.05 (0.39–2.80), 0.920 |
| Education | ||||
| Highschool or less (ref) | ||||
| Some college | 1.27 (0.87–1.86), 0.214 | 0.98 (0.62–1.54), 0.915 | 1.68 (1.26–2.23), 0.001 | 1.22 (0.56–2.66), 0.606 |
| College or above | 1.55 (1.05–1.41), 0.028 | 0.55 (0.34–0.88), 0.014 | 1.80 (1.30–2.48), 0.001 | 1.94 (0.78–4.79), 0.148 |
| Income | ||||
| <$50,000 (ref) | ||||
| $50,000–99,999 | 0.93 (0.66–1.62), 0.693 | 0.42 (0.27–0.64), <0.001 | 1.01 (0.71–1.44), 0.944 | 0.96 (0.38–2.42), 0.935 |
| ≥$100,000 | 1.15 (0.75–1.76), 0.511 | 0.12 (0.06–0.24), <0.001 | 1.07 (0.69–1.65), 0.770 | 1.05 (0.39–2.80), 0.926 |
References
- McCoy, R.G. Reimagining Diabetes Quality Measurement to Advance Quality Care. Popul. Health Manag. 2023, 26, S-9–S-11. [Google Scholar] [CrossRef]
- Kemp, K.; Steele, B.; Ahmed, S.; Fairie, P.; Santana, M. Person-Centred Quality Indicators Are Associated with Unplanned Care Use Following Hospital Discharge. BMJ Open Qual. 2024, 13, e002501. [Google Scholar] [CrossRef] [PubMed]
- Campbell, R.; Ju, A.; King, M.T.; Rutherford, C. Perceived Benefits and Limitations of Using Patient-Reported Outcome Measures in Clinical Practice with Individual Patients: A Systematic Review of Qualitative Studies. Qual. Life Res. 2022, 31, 1597–1620. [Google Scholar] [CrossRef]
- Quality in Healthcare. Agency for Healthcare Research and Quality (US): Rockville, MD, USA. Available online: https://www.ncbi.nlm.nih.gov/books/NBK579353/ (accessed on 9 November 2023).
- Brach, C.; Borsky, A. How the U.S. Agency for Healthcare Research and Quality Promotes Health Literate Health Care. Stud. Health Technol. Inform. 2020, 269, 313–323. [Google Scholar] [PubMed]
- Mazurenko, O.; Collum, T.; Ferdinand, A.; Menachemi, N. Predictors of Hospital Patient Satisfaction as Measured by Hcahps: A Systematic Review. J. Healthc. Manag. 2017, 62, 272–283. [Google Scholar] [CrossRef] [PubMed]
- Newgard, C.D.; Fu, R.; Heilman, J.; Tanski, M.; Ma, O.J.; Lines, A.; French, L.K. Using Press Ganey Provider Feedback to Improve Patient Satisfaction: A Pilot Randomized Controlled Trial. Acad. Emerg. Med. 2017, 24, 1051–1059. [Google Scholar] [CrossRef] [PubMed]
- Alibrandi, A.; Gitto, L.; Limosani, M.; Mustica, P.F. Patient Satisfaction and Quality of Hospital Care. Eval. Program. Plann. 2023, 97, 102251. [Google Scholar] [CrossRef] [PubMed]
- Al-Rashdan, A.; Watson, L.; Yannitsos, D.; Qi, S.; Grendarova, P.; Barbera, L. Comparison of Patient-Reported Experience of Patients Receiving Radiotherapy Measured by Two Validated Surveys. Curr. Oncol. 2021, 28, 2180–2189. [Google Scholar] [CrossRef]
- Aljarallah, N.A.; Almuqbil, M.; Alshehri, S.; Khormi, A.M.S.; AlReshaidan, R.M.; Alomran, F.H.; Alomar, N.F.; Alshahrani, F.F.; Alshammari, M.S.; Alsanie, W.F.; et al. Satisfaction of Patients with Health Care Services in Tertiary Care Facilities of Riyadh, Saudi Arabia: A Cross-Sectional Approach. Front. Public Health 2022, 10, 1077147. [Google Scholar] [CrossRef]
- Lee, P.Y. Quality Doctor-Patient Communication for Better Patient Satisfaction in Primary Care Practice. Malays. Fam. Physician 2022, 17, 1. [Google Scholar] [CrossRef]
- Leow, H.T.; Liew, S.M. A Cross Sectional Study on Patient Satisfaction and Its Association with Length of Consultation at the University Malaya Medical Centre Primary Care Clinic. Malays. Fam. Physician 2022, 17, 71–80. [Google Scholar] [CrossRef] [PubMed]
- Caraballo, C.; Ndumele, C.D.; Roy, B.; Lu, Y.; Riley, C.; Herrin, J.; Krumholz, H.M. Trends in Racial and Ethnic Disparities in Barriers to Timely Medical Care among Adults in the Us, 1999 to 2018. JAMA Health Forum 2022, 3, e223856. [Google Scholar] [CrossRef] [PubMed]
- Edwards, E.M.; Greenberg, L.T.; Profit, J.; Draper, D.; Helkey, D.; Horbar, J.D. Quality of Care in Us Nicus by Race and Ethnicity. Pediatrics 2021, 148, e2020037622. [Google Scholar] [CrossRef]
- Rei, K.M.; Reddy, V.; Brazdzionis, J.; Siddiqi, J. Determinants and Disparities of Neurosurgery Patients Refusing Inpatient Palliative Care after Provider Recommendation. Cureus 2023, 15, e49925. [Google Scholar] [CrossRef]
- Karram, S.; Sanger, C.; Convery, C.; Brantley, A. Social Determinants of Health among Persons Living with HIV Impact Important Health Outcomes in Michigan. AIDS Behav. 2024, in press. [CrossRef]
- Zhang, J.; Gu, L.L.; Xu, Y.; Zhao, B.B.; Li, D.; Xiao, C. Integrated Medical Care and the Continuous 4c Nursing Model to Improve Nursing Quality and Clinical Treatment of Patients with Acute Stroke: Based on a Retrospective Case-Control Study. Contrast Media Mol. Imaging 2022, 2022, 4810280. [Google Scholar] [CrossRef] [PubMed]
- Spruce, L. Back to Basics: Social Determinants of Health. AORN J. 2019, 110, 60–69. [Google Scholar] [CrossRef]
- Office of Disease Prevention and Health Promotion; U.S. Department of Health and Human Services. Social Determinants of Health. Available online: https://health.gov/healthypeople/priority-areas/social-determinants-health (accessed on 9 November 2023).
- DeBolt, C.; Harris, D. The Impact of Social Determinants of Health on Gender Disparities within Respiratory Medicine. Clin. Chest Med. 2021, 42, 407–415. [Google Scholar] [CrossRef]
- Research Center. National Overview. Available online: https://www.unitedwayalice.org/in-the-us (accessed on 10 January 2024).
- Okunrintemi, V.; Khera, R.; Spatz, E.S.; Salami, J.A.; Valero-Elizondo, J.; Warraich, H.J.; Virani, S.S.; Blankstein, R.; Blaha, M.J.; Pawlik, T.M.; et al. Association of Income Disparities with Patient-Reported Healthcare Experience. J. Gen. Intern. Med. 2019, 34, 884–892. [Google Scholar] [CrossRef]
- Williams, D.R.; Lawrence, J.A.; Davis, B.A. Racism and Health: Evidence and Needed Research. Annu. Rev. Public Health 2019, 40, 105–125. [Google Scholar] [CrossRef]
- Tai, D.B.G.; Shah, A.; Doubeni, C.A.; Sia, I.G.; Wieland, M.L. The Disproportionate Impact of COVID-19 on Racial and Ethnic Minorities in the United States. Clin. Infect. Dis. 2021, 72, 703–706. [Google Scholar] [CrossRef]
- Meints, S.M.; Cortes, A.; Morais, C.A.; Edwards, R.R. Racial and Ethnic Differences in the Experience and Treatment of Noncancer Pain. Pain Manag. 2019, 9, 317–334. [Google Scholar] [CrossRef]
- Chang, E.; Davis, T.L.; Berkman, N.D. Delayed and Forgone Health Care among Adults with Limited English Proficiency During the Early COVID-19 Pandemic. Med. Care 2023. [CrossRef] [PubMed]
- Martinez Leal, I.; Acquati, C.; Rogova, A.; Chen, T.A.; Connors, S.K.; Agrawal, P.; McNeill, L.H.; Reitzel, L.R. Negotiating Cancer Alone: A Qualitative Study Exploring Care Experiences of Racially and Ethnically Diverse Women Diagnosed with Breast Cancer During COVID-19. J. Health Psychol. 2023, 13591053231214517. [Google Scholar] [CrossRef] [PubMed]
- Arevalo, M.; Pickering, T.A.; Vernon, S.W.; Fujimoto, K.; Peskin, M.F.; Farias, A.J. Racial/Ethnic Disparities in the Association between Patient Care Experiences and Receipt of Initial Surgical Breast Cancer Care: Findings from Seer-Cahps. Breast Cancer Res. Treat. 2023. [Google Scholar] [CrossRef]
- Mannoh, I.; Hussien, M.; Commodore-Mensah, Y.; Michos, E.D. Impact of Social Determinants of Health on Cardiovascular Disease Prevention. Curr. Opin. Cardiol. 2021, 36, 572–579. [Google Scholar] [CrossRef] [PubMed]
- Agbonlahor, O.; DeJarnett, N.; Hart, J.L.; Bhatnagar, A.; McLeish, A.C.; Walker, K.L. Racial/Ethnic Discrimination and Cardiometabolic Diseases: A Systematic Review. J. Racial Ethn. Health Disparities 2023, 1–25. [Google Scholar] [CrossRef] [PubMed]
- Bangerter, L.R.; Griffin, J.; Harden, K.; Rutten, L.J. Health Information-Seeking Behaviors of Family Caregivers: Analysis of the Health Information National Trends Survey. JMIR Aging 2019, 2, e11237. [Google Scholar] [CrossRef]
- Yang, R.; Zeng, K.; Jiang, Y. Prevalence, Factors, and Association of Electronic Communication Use with Patient-Perceived Quality of Care from the 2019 Health Information National Trends Survey 5-Cycle 3: Exploratory Study. J. Med. Internet Res. 2022, 24, e27167. [Google Scholar] [CrossRef]
- Chawla, K.; Kibreab, A.; Scott, V.; Lee, E.L.; Aduli, F.; Brim, H.; Ashktorab, H.; Howell, C.D.; Laiyemo, A.O. Association of Patients’ Perception of Quality of Healthcare Received and Colorectal Cancer Screening Uptake: An Analysis of 2 National Surveys in the USA. Med. Princ. Pract. 2021, 30, 331–338. [Google Scholar] [CrossRef]
- Silveira Bianchim, M.; Crane, E.; Jones, A.; Neukirchinger, B.; Roberts, G.; McLaughlin, L.; Noyes, J. The Implementation, Use and Impact of Patient Reported Outcome Measures in Value-Based Healthcare Programmes: A Scoping Review. PLoS ONE 2023, 18, e0290976. [Google Scholar] [CrossRef]
- Moser, R.P.; Trivedi, N.; Murray, A.; Jensen, R.E.; Willis, G.; Blake, K.D. Patient-Centered Communication (Pcc) Scale: Psychometric Analysis and Validation of a Health Survey Measure. PLoS ONE 2022, 17, e0279725. [Google Scholar] [CrossRef] [PubMed]
- Asan, O.; Yu, Z.; Crotty, B.H. How Clinician-Patient Communication Affects Trust in Health Information Sources: Temporal Trends from a National Cross-Sectional Survey. PLoS ONE 2021, 16, e0247583. [Google Scholar] [CrossRef] [PubMed]
- Powell-Wiley, T.M.; Baumer, Y.; Baah, F.O.; Baez, A.S.; Farmer, N.; Mahlobo, C.T.; Pita, M.A.; Potharaju, K.A.; Tamura, K.; Wallen, G.R. Social Determinants of Cardiovascular Disease. Circ. Res. 2022, 130, 782–799. [Google Scholar] [CrossRef] [PubMed]
- Cockerham, W.C.; Hamby, B.W.; Oates, G.R. The Social Determinants of Chronic Disease. Am. J. Prev. Med. 2017, 52, S5–S12. [Google Scholar] [CrossRef] [PubMed]
- Menza, T.W.; Hixson, L.K.; Lipira, L.; Drach, L. Social Determinants of Health and Care Outcomes among People with Hiv in the United States. Open Forum Infect. Dis. 2021, 8, ofab330. [Google Scholar] [CrossRef] [PubMed]
- Chung, J.; Gendron, T.; Winship, J.; Wood, R.E.; Mansion, N.; Parsons, P.; Demiris, G. Smart Speaker and Ict Use in Relationship with Social Connectedness during the Pandemic: Loneliness and Social Isolation Found in Older Adults in Low-Income Housing. Gerontologist 2023, gnad145. [Google Scholar] [CrossRef] [PubMed]
- Mateen, F.J.; Trápaga Hacker, C. Perceptions of People with Multiple Sclerosis on Social Determinants of Health: Mixed Methods. Mult. Scler. Relat. Disord. 2023, 80, 105089. [Google Scholar] [CrossRef]
- Quickfacts. Available online: https://www.census.gov/quickfacts/fact/table/US/PST045223 (accessed on 7 January 2024).
- 2020 Census Illuminates Racial and Ethnic Composition of the Country. Available online: https://www.census.gov/library/stories/2021/08/improved-race-ethnicity-measures-reveal-united-states-population-much-more-multiracial.html?fbclid=IwAR1xdK8TAwqHZA43L0-U7O6bnzHe1tuL__EXxYCLoXL-tqa99YuT2m697zM (accessed on 7 January 2024).
- Thompson, C. Dietary Health in the Context of Poverty and Uncertainty around the Social Determinants of Health. Proc. Nutr. Soc. 2022, 81, 134–140. [Google Scholar] [CrossRef]
- Yousefi-Rizi, L.; Baek, J.D.; Blumenfeld, N.; Stoskopf, C. Impact of Housing Instability and Social Risk Factors on Food Insecurity among Vulnerable Residents in San Diego County. J. Community Health 2021, 46, 1107–1114. [Google Scholar] [CrossRef]
- Rabbitt, M.P.; Hales, L.J.; Reed-Jones, M.; Coleman-Jensen, A.; USDA Economic Research Service/U.S. Department of Agriculture. Food Security in the U.S.—Key Statistics & Graphics. Available online: https://www.ers.usda.gov/topics/food-nutrition-assistance/food-security-in-the-u-s/key-statistics-graphics/ (accessed on 9 November 2023).
- Shrider, E.A.; Creamer, J.; United States Census Bureau. Poverty in the United States: 2022. Available online: https://www.census.gov/library/publications/2023/demo/p60-280.html?fbclid=IwAR3gXgOxNEj_kh5mpEgRQxht3E_oD62FeVjdG3mP2oCvzTtVEKAgBmlfsFQ#:~:text=The%20official%20poverty%20rate%20in,and%20Table%20A%2D1 (accessed on 9 November 2023).
- Lathrop, B. Moving toward Health Equity by Addressing Social Determinants of Health. Nurs. Women’s Health 2020, 24, 36–44. [Google Scholar] [CrossRef] [PubMed]
- Employment Projections. Available online: https://www.bls.gov/emp/chart-unemployment-earnings-education.htm?fbclid=IwAR3vcU9E8A10H_SN5a-cKuEptGO1l-uyC1JD1HCbDIWydE15QA04JMf4OcU (accessed on 10 January 2024).
- Nutbeam, D.; Lloyd, J.E. Understanding and Responding to Health Literacy as a Social Determinant of Health. Annu. Rev. Public Health 2021, 42, 159–173. [Google Scholar] [CrossRef] [PubMed]
- Mahoney, S.T.; Tawfik-Sexton, D.; Strassle, P.D.; Farrell, T.M.; Duke, M.C. Effects of Education and Health Literacy on Postoperative Hospital Visits in Bariatric Surgery. J. Laparoendosc. Adv. Surg. Tech. A 2018, 28, 1100–1104. [Google Scholar] [CrossRef] [PubMed]
- Zhu, M.; Arinze, N.; de la Vega, P.B.; Alonso, A.; Levin, S.; Farber, A.; King, E.; Kobzeva-Herzog, A.; Chitalia, V.C.; Siracuse, J.J. High Prevalence of Adverse Social Determinants of Health in Dialysis Access Creation Patients in a Safety-Net Setting. Ann. Vasc. Surg. 2024, 100, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Singu, S.; Acharya, A.; Challagundla, K.; Byrareddy, S.N. Impact of Social Determinants of Health on the Emerging COVID-19 Pandemic in the United States. Front. Public Health 2020, 8, 406. [Google Scholar] [CrossRef] [PubMed]
- Zhong, S.; Huisingh-Scheetz, M.; Huang, E.S. Delayed Medical Care and Its Perceived Health Impact among Us Older Adults during the Covid-19 Pandemic. J. Am. Geriatr. Soc. 2022, 70, 1620–1628. [Google Scholar] [CrossRef] [PubMed]
- Findling, M.G.; Blendon, R.J.; Benson, J.M. Delayed Care with Harmful Health Consequences-Reported Experiences from National Surveys during Coronavirus Disease 2019. JAMA Health Forum 2020, 1, e201463. [Google Scholar] [CrossRef]
- Tolentino, D.A.; Ajuwon, A.M. A Cross-Sectional Study on Social Determinants of Mental Health During Covid-19 among Adults in California. J. Adv. Nurs. 2024, 80, 683–691. [Google Scholar] [CrossRef]
- Dibble, K.E.; Deng, Z.; Connor, A.E. Differences in Survivorship Care Experiences among Older Breast Cancer Survivors by Clinical Cancer Characteristics, Race/Ethnicity, and Socioeconomic Factors: A Seer-Cahps Study. Breast Cancer Res. Treat. 2023, 199, 565–582. [Google Scholar] [CrossRef]
- Farias, A.J.; Ochoa, C.Y.; Toledo, G.; Bang, S.I.; Hamilton, A.S.; Du, X.L. Racial/Ethnic Differences in Patient Experiences with Health Care in Association with Earlier Stage at Breast Cancer Diagnosis: Findings from the Seer-Cahps Data. Cancer Causes Control 2020, 31, 13–23. [Google Scholar] [CrossRef]
- Nguyen, K.H.; Wilson, I.B.; Wallack, A.R.; Trivedi, A.N. Racial and Ethnic Disparities in Patient Experience of Care among Nonelderly Medicaid Managed Care Enrollees. Health Aff. 2022, 41, 256–264. [Google Scholar] [CrossRef] [PubMed]
| White | Hispanic | p-Value | |
|---|---|---|---|
| Number of participants—N (Wt%) | 2833 (81.73) | 778 (18.27) | |
| Age—N (Wt%) | <0.001 | ||
| 18–34 | 313 (19.67) | 184 (35.89) | |
| 35–49 | 495 (22.89) | 194 (28.14) | |
| 50–64 | 816 (30.46) | 208 (22.84) | |
| 65–74 | 713 (15.92) | 126 (8.87) | |
| 75+ | 496 (11.06) | 66 (4.26) | |
| Gender | 0.1965 | ||
| Male | 1149 (47.74) | 274 (44.29) | |
| Female | 1684 (52.26) | 504 (55.71) | |
| Marital Status | 0.0004 | ||
| Single | 397 (24.18) | 155 (33.07) | |
| Married | 1629 (62.67) | 424 (55.85) | |
| Others | 807 (13.15) | 199 (11.07) | |
| Level of Education | <0.0001 | ||
| High school or below | 751 (32.16) | 332 (51.65) | |
| Some college | 558 (30.40) | 162 (26.42) | |
| Bachelor’s degree or above | 1524 (37.44) | 284 (21.93) | |
| Income levels | <0.0001 | ||
| <USD 50,000 | 969 (30.33) | 411 (45.35) | |
| USD 50,000–99,999 | 909 (32.14) | 214 (33.11) | |
| ≥USD 100,000 | 955 (37.53) | 153 (21.55) | |
| Insurance | <0.0001 | ||
| Yes | 2727 (95.15) | 672 (84.36) | |
| No | 106 (4.85) | 106 (15.64) |
| Optimal Quality Care | Less Optimal Quality Care | p-Value | |
|---|---|---|---|
| Race/ethnicity—N (Wt%) | 0.0001 | ||
| White | 2136 (74.19) | 697 (25.81) | |
| Hispanic | 477 (60.00) | 301 (40.00) | |
| Patient-centered communication—N (Wt%) | <0.0001 | ||
| Positive | 1611 (61.64) | 173 (15.55) | |
| Negative | 1002 (38.36) | 825 (84.45) | |
| SDOHs—N (Wt%) | <0.0001 | ||
| Negative | 404 (52.39) | 317 (47.61) | |
| Positive | 2209 (76.67) | 681 (23.33) | |
| Having unfair or discriminated care—N (Wt%) | <0.0001 | ||
| Yes | 56 (33.34) | 92 (66.66) | |
| No | 2557 (73.04) | 906 (26.96) | |
| Delaying or not receiving medical care needed—N (Wt%) | <0.0001 | ||
| Yes | 617 (54.04) | 494 (45.96) | |
| No | 1996 (79.61) | 504 (20.39) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tzeng, C.-F.T.; Swoboda, T.; Huggins, C.; D’Etienne, J.; Wang, H. Risks Associated with Quality Care among Hispanic and White Populations—A Cross-Sectional Comparison Study. Healthcare 2024, 12, 250. https://doi.org/10.3390/healthcare12020250
Tzeng C-FT, Swoboda T, Huggins C, D’Etienne J, Wang H. Risks Associated with Quality Care among Hispanic and White Populations—A Cross-Sectional Comparison Study. Healthcare. 2024; 12(2):250. https://doi.org/10.3390/healthcare12020250
Chicago/Turabian StyleTzeng, Ching-Fang Tiffany, Thomas Swoboda, Charles Huggins, James D’Etienne, and Hao Wang. 2024. "Risks Associated with Quality Care among Hispanic and White Populations—A Cross-Sectional Comparison Study" Healthcare 12, no. 2: 250. https://doi.org/10.3390/healthcare12020250
APA StyleTzeng, C.-F. T., Swoboda, T., Huggins, C., D’Etienne, J., & Wang, H. (2024). Risks Associated with Quality Care among Hispanic and White Populations—A Cross-Sectional Comparison Study. Healthcare, 12(2), 250. https://doi.org/10.3390/healthcare12020250